
Cytokine Response to SARS-CoV-2 Infection in Children

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Statistical Analysis
3. Results
3.1. Patients: Clinical and Laboratory Features
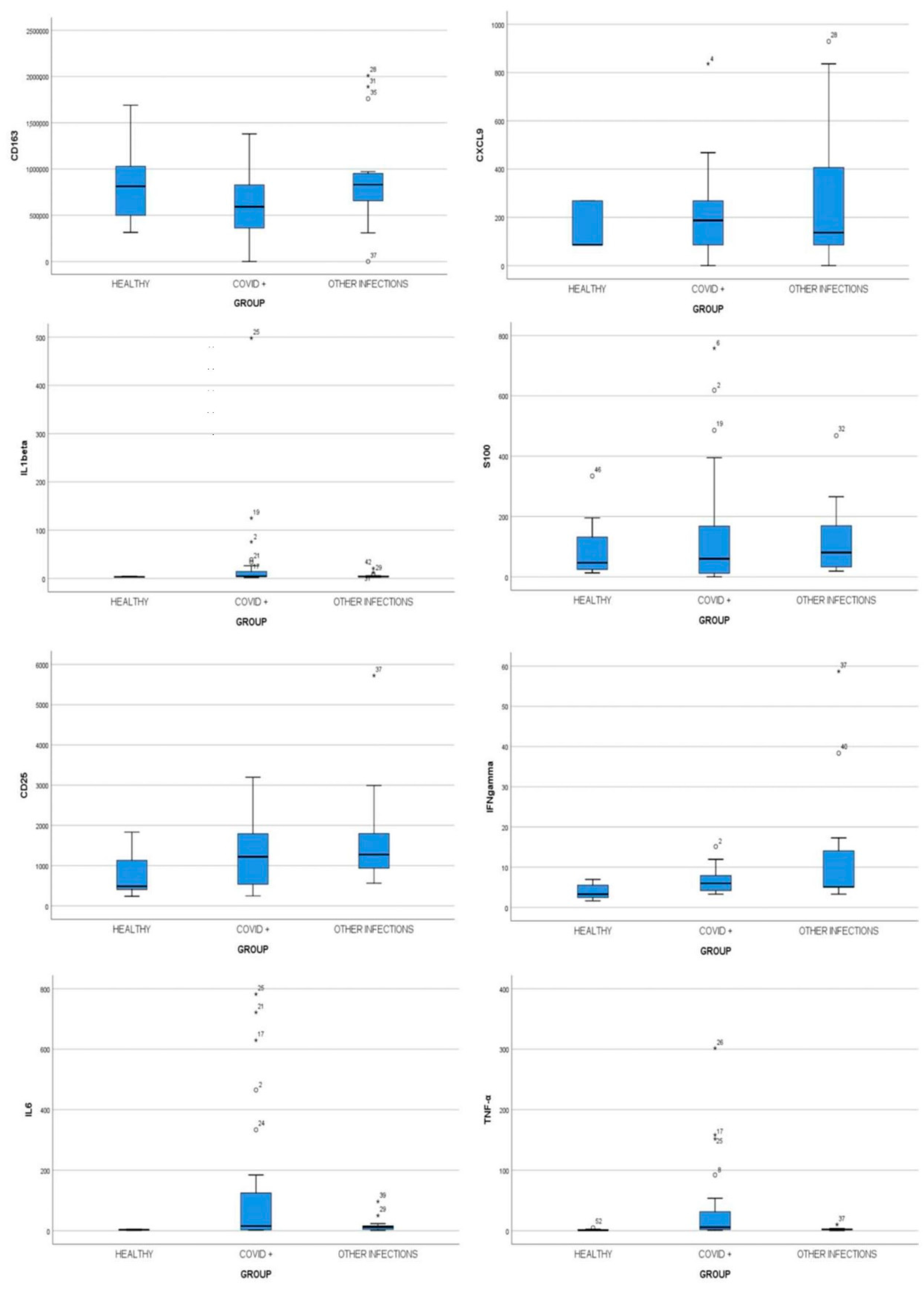
3.2. Cytokine Screening
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Curatola, A.; Lazzareschi, I.; Bersani, G.; Covino, M.; Gatto, A.; Chiaretti, A. Impact of COVID-19 outbreak in acute bronchiolitis: Lesson from a tertiary Italian Emergency Department. Pediatr. Pulmonol. 2021, 56, 2484–2488. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Palmieri, L.; Agazio, E.; Andrianou, X.; Barbariol, P.; Bella, A.; Benelli, E.; Bertinato, L.; Bocci, M.; Boros, S.; Calcagnini, G.; et al. Characteristics of COVID-19 patients dying in Italy report based on available data on March 20, 2020. Epicentro 2020. Available online: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-analysis-of-deaths (accessed on 15 March 2021).
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Yuan, J.; Liu, Y.; Fu, T.; Yu, X.; Zhang, Z.-J. Novel Coronavirus Infection in Hospitalized Infants Under 1 Year of Age in China. JAMA 2020, 323, 1313. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Shao, J.; Guo, Y.; Peng, X.; Li, Z.; Hu, D. Clinical and CT features in pediatric patients with COVID-19 infecton: Different points from adults. Pediatr. Pulmonol. 2020, 55, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatto, A.; Rivetti, S.; Capossela, L.; Pata, D.; Covino, M.; Chiaretti, A. Utility of a pediatric observation unit for the management of children admitted to the emergency department. Ital. J. Pediatr. 2021, 47, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, P.; Curtis, N. Coronavirus infections in children including COVID-19: An overview of the Epidemiology, Clinical Features, Diagnosis, Treatment and Prevention Options in Children. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef]
- Salem, C.B. Acute respiratory distress syndrome. N. Engl. J. Med. 2017, 377, 1904. [Google Scholar]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Ozsurekci, Y.; Aykac, K.; Er, A.G.; Halacli, B.; Arasli, M.; Oygar, P.D.; Gürlevik, S.; Yayla, B.C.C.; Karakaya, J.; Alp, A.; et al. Predictive value of cytokine/chemokine responses for the disease severity and management in children and adult cases with COVID-19. J. Med Virol. 2021, 93, 2828–2837. [Google Scholar] [CrossRef]
- Soraya, G.V.; Ulhaq, Z.S. Interleukin-6 levels in children developing SARS-CoV-2 infection. Pediatr. Neonatol. 2020, 61, 253–254. [Google Scholar] [CrossRef]
- Parri, N.; Magistà, A.M.; Marchetti, F.; Cantoni, B.; Arrighini, A.; Romanengo, M.; Felici, E.; Urbino, A.; Da Dalt, L.; Verdoni, L.; et al. Characteristic of COVID-19 infection in pediatric patients: Early findings from two Italian Pediatric Research Networks. Eur. J. Nucl. Med. Mol. Imaging 2020, 179, 1315–1323. [Google Scholar]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2. Arthritis Rheumatol. 2021, 73, e13–e29. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Sforzi, I.; Trapani, S.; Biban, P.; Silvagni, D.; Villa, G.; Tibaldi, J.; Bertacca, L.; Felici, E.; Perricone, G.; et al. Characteristics and risk factors for SARS-CoV-2 in children tested in the early phase of the pandemic: A cross-sectional study, Italy, 23 February to 24 May 2020. Euro Surveill. 2021, 26, 2001248. [Google Scholar] [CrossRef] [PubMed]
- Fara, A.; Mitrev, Z.; Rosalia, R.A.; Assas, B.M. Cytokine storm and COVID-19: A chronicle of pro-inflammatory cytokines. Open Biol. 2020, 10, 200160. [Google Scholar] [CrossRef] [PubMed]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- Qian, G.; Zhang, Y.; Xu, Y.; Hu, W.; Hall, I.P.; Yue, J.; Lu, H.; Ruan, L.; Ye, M.; Mei, J. Reduced inflammatory responses to SARS-CoV-2 infection in children presenting to hospital with COVID-19 in China. E Clin. Med. 2021, 34, 100831. [Google Scholar]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. Chinese Pediatric Novel Coronavirus Study Team. SARS-CoV-2 infection in children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [Green Version]
- Mao, B.; Liu, Y.; Chai, Y.-H.; Jin, X.-Y.; Lu, H.-W.; Yang, J.-W.; Gao, X.-W.; Song, X.-L.; Bao, H.; Wang, A.; et al. Assessing risk factors for SARS-CoV-2 infection in patients presenting with symptoms in Shanghai, China: A multicentre, observational cohort study. Lancet Dig. Health 2020, 2, e323–e330. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; François, B.; Sève, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Correction to: Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensiv. Care Med. 2020, 46, 1294–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Moratto, D.; Giacomelli, M.; Chiarini, M.; Savarè, L.; Saccani, B.; Motta, M.; Timpano, S.; Poli, P.; Paghera, S.; Imberti, L.; et al. Immune response in children with COVID-19 is characterized by lower levels of T-cell activation than infected adults. Eur. J. Immunol. 2020, 50, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Aceti, A.; Margarucci, L.M.; Scaramucci, E.; Orsini, M.; Salerno, G.; Di Sante, G.; Gianfranceschi, G.; Di Liddo, R.; Valeriani, F.; Ria, F.; et al. Serum S100B protein as a marker of severity in Covid-19 patients. Sci. Rep. 2020, 10, 1–8. [Google Scholar]



{kind=link}
{kind=link}
| Group 1 (n = 27) | Group 2 (n = 16) | Group 3 (n = 9) | p-Value | |
|---|---|---|---|---|
| Gender (M) | 16 (17.1%) | 7 (25.0%) | 5 (17.9%) | 0.567 |
| Contact with COVID-19 positive | 17 (63.0%) | 1 (6.3%) | 0 (0.0%) | 0.000 |
| Cardiopathy | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Immune deficiency | 1 (3.7%) | 2 (12.5%) | 0 (0.0%) | 0.570 |
| Tachycardia | 2 (7.4%) | 2 (12.5%) | 0 (0.0%) | 0.640 |
| Tachypnea | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Fever | 19 (70.4%) | 16 (100.0%) | 0 (0.0%) | 0.000 |
| Cough | 7 (25.9%) | 5 (31.3%) | 1 (11.1%) | 0.570 |
| Rinitis | 4 (14.8%) | 0 (0.0%) | 0 (0.0%) | 0.280 |
| Dyspnea | 1 (3.7%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Respiratory symptoms | 8 (29.6%) | 5 (31.3%) | 1 (11.1%) | 0.588 |
| Rash | 2 (28.6%) | 4 (57.1%) | 1 (14.3%) | 0.292 |
| Muscle aches | 6 (22.2%) | 4 (25.0%) | 2 (22.2%) | 1.000 |
| Chest pain | 3 (11.1%) | 0 (0.0%) | 1 (11.1%) | 0.377 |
| Abdominal Pain | 4 (14.8%) | 6 (37.5%) | 1 (11.1%) | 0.232 |
| Vomit | 2 (7.4%) | 2 (12.5%) | 1 (11.1%) | 0.838 |
| Diarrhea | 3 (11.1%) | 2 (12.5%) | 0 (0.0%) | 0.692 |
| Gastrointestinal symptoms | 6 (22.2%) | 7 (43.8%) | 1 (11.1%) | 0.172 |
| Headache | 2 (7.4%) | 2 (12.5%) | 1 (11.1%) | 0.838 |
| Asthenia | 8 (29.6%) | 7 (43.8%) | 3 (33.3%) | 0.684 |
| Seizures | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Ageusia | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Anosmia | 2 (7.4%) | 0 (0.0%) | 0 (0.0%) | 0.674 |
| Neurological symptoms | 11 (40.7%) | 8 (50.0%) | 4 (44.4%) | 0.929 |
| Lymphadenopathy | 3 (11.1%) | 3 (18.8%) | 0 (0.0%) | 0.448 |
| Pharyngodynia | 4 (14.8%) | 5 (31.3%) | 0 (0.0%) | 0.140 |
| Conjunctivitis | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Asymptomatic | 4 (14.8%) | 0 (0.0%) | 4 (44.4%) | 0.120 |
| Hospitalization | 16 (59.3%) | 10 (62.5%) | 2 (22.2%) | 0.131 |
| Cytokine | Asymptomatic (n = 4) | Mild (n = 18) | Moderate (n = 4) | Severe (n = 1) | p-Value |
|---|---|---|---|---|---|
| CD163 (pg/mL) | 477937.53 ± 233631.34 | 630800.59 ± 367831.35 | 612994.86 ± 516348.23 | 704946.15 | 0.893 |
| CXCL9 (pg/mL) | 204.70 (86.16–340.34) | 208.48 (0.00–836.24) | 93.72 (0.00–187.44) | 0.00 | 0.246 |
| IL-1β (pg/mL) | 10.17 (3.69–497.80) | 4.21 (1.86–124.93) | 3.34 (2.34–75.62) | 4.39 | 0.511 |
| S100 (pg/mL) | 153.75 (80.73–304.62 ) | 44.05 (0.00–757.85) | 0.00 (0.00–618.56) | 60.03 | 0.254 |
| CD25 (pg/mL) | 1052.83 (245.49–1507.56) | 1372.44 (276.29–3195.35) | 768.19 (452.14–3128.03) | 2505.33 | 0.458 |
| IFN-γ (pg/mL) | 4.17 (3.28–7.91) | 5.99 (4.16–11.95) | 5.59 (3.28–15.12) | 5.99 | 0.639 |
| IL-6 (pg/mL) | 169.65 (3.35–781.95) | 15.30 (1.39–721.59) | 9.82 (1.70–465.22) | 63.25 | 0.736 |
| TNF-α (pg/mL) | 23.75 (2.51–158.30) | 4.72 (0.57–301.59) | 3.90 (1.44–15.96) | 6.42 | 0.781 |
| Cytokine | Group 1 (n = 27) | Group 2 (n = 16) | Group 3 (n = 9) | p-Value |
|---|---|---|---|---|
| CD163 (pg/mL) | 608262.46 ± 358962.97 | 922327.12 ± 541792.5 | 805893.37 ± 434707.79 | 0.074 |
| CXCL9 (pg/mL) | 187.44 (86.16–277.76) | 136.8 (86.16–406.25) | 86.16 (86.16–268.57) | 0.705 |
| IL-1β (pg/mL) | 4.39 (3.17–15.5) | 3.86 (3.25–5.19) | 3.00 (2.50–4.21) | 0.057 |
| S100 (pg/mL) | 60.03 (10.05–169.41) | 80.70 (31.77–172.99) | 46.77 (13.1–195.59) | 0.663 |
| CD25 (pg/mL) | 1219.55 (532.17–1802.42) | 1274.53 (928.01–1926.75) | 484.53 (370.07–1132.12) | 0.039 |
| IFN-γ (pg/mL) | 5.06 (4.16–7.91) | 5.99 (5.06–14.58) | 3.28 (2.05–5.76) | 0.044 |
| IL-6 (pg/mL) | 15.3 (2.67–131.7) | 12.29 (4.46–17.27) | 3.01 (1.50–4.41) | 0.014 |
| TNF-α (pg/mL) | 5.67 (1.84–40.18) | 2.38 (1.31–2.93) | 0.81 (0.81–2.11) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curatola, A.; Chiaretti, A.; Ferretti, S.; Bersani, G.; Lucchetti, D.; Capossela, L.; Sgambato, A.; Gatto, A. Cytokine Response to SARS-CoV-2 Infection in Children. Viruses 2021, 13, 1868. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091868
Curatola A, Chiaretti A, Ferretti S, Bersani G, Lucchetti D, Capossela L, Sgambato A, Gatto A. Cytokine Response to SARS-CoV-2 Infection in Children. Viruses. 2021; 13(9):1868. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091868
Chicago/Turabian StyleCuratola, Antonietta, Antonio Chiaretti, Serena Ferretti, Giulia Bersani, Donatella Lucchetti, Lavinia Capossela, Alessandro Sgambato, and Antonio Gatto. 2021. "Cytokine Response to SARS-CoV-2 Infection in Children" Viruses 13, no. 9: 1868. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091868