
Mutations in the Reverse Transcriptase and Protease Genes of Human Immunodeficiency Virus-1 from Antiretroviral Naïve and Treated Pediatric Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection
2.2. Laboratory Measurements
2.3. Drug Resistance Profiling

{kind=link}
{kind=link}
{kind=link}
| Primer | Orientation | HXB2 Position | Sequence |
|---|---|---|---|
| Reverse Transcriptase | |||
| RT1 | Forward | 2551–2572 | 5ʹ-TTCCCATTAGTCCTATTGAAACTGT -3ʹ |
| RT2 | Reverse | 3292–3313 | 5ʹ-TCATTGACAGTCCAGCTATCCTTT T -3ʹ |
| RT3 | Forward | 2705–2725 | 5ʹ-GCCTGAAAATCCATATAACAC TCC -3ʹ |
| RT4 | Reverse | 3219–3237 | 5ʹ-CCATCCAAAGAAATGGAGGTTC -3ʹ |
| Protease | |||
| PR1 | Forward | 2082–2109 | 5ʹ-TAATTTTTTAGGGAAGATCTGGCCCTTC-3ʹ |
| PR2 | Reverse | 2734–2703 | 5ʹ-GCAAATACTGGAGTTGTATGGATTTTCAGG-3ʹ |
| PR3 | Forward | 2136–2162 | 5ʹ-TCAGAGCAGACCAGAGCCAACAGCCCC-3ʹ |
| PR4 | Reverse | 2650–2621 | 5ʹ-AATGCTTTTATTTTTTTCTTCTGTCAATGGC-3ʹ |

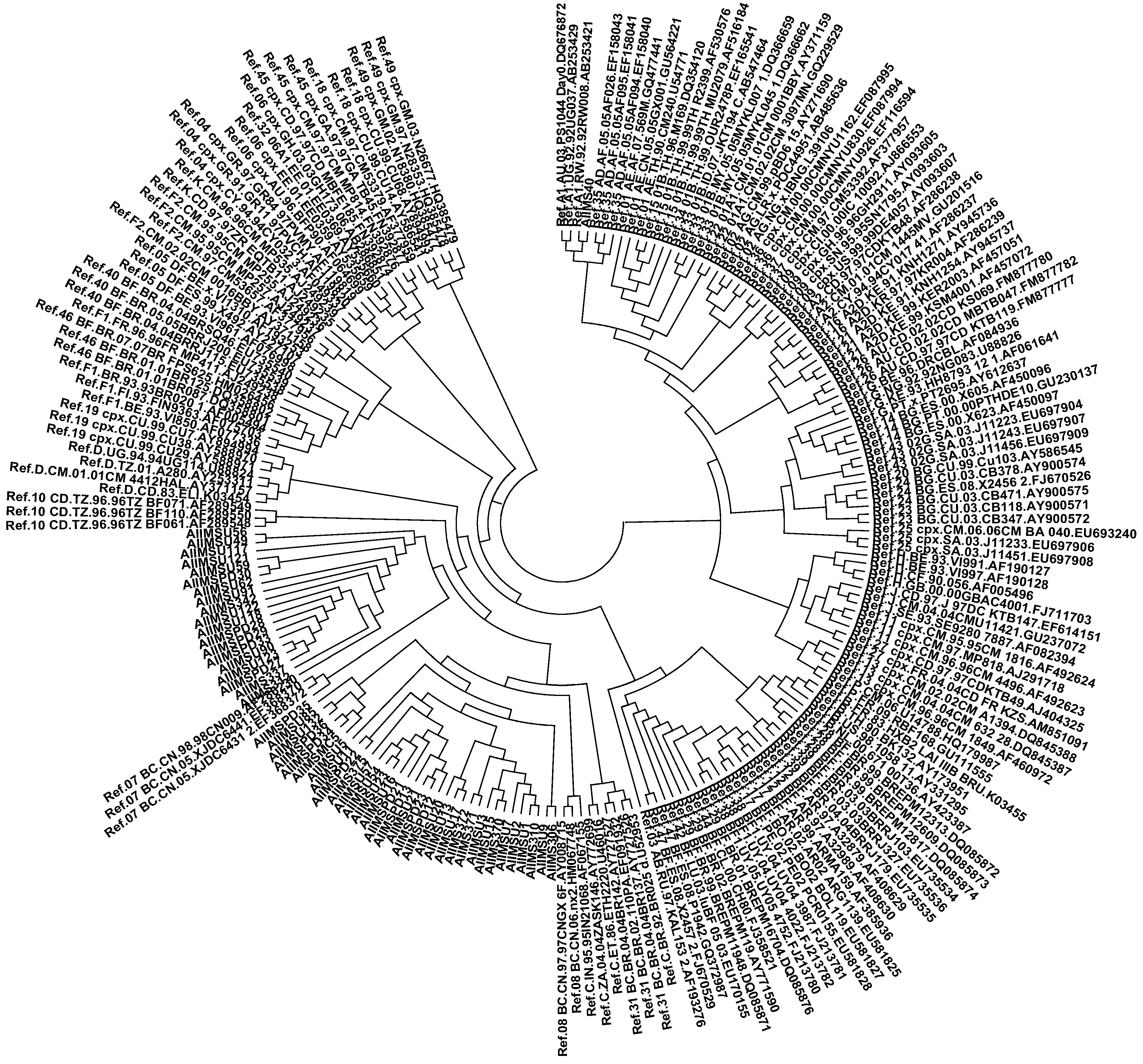
2.4. Viral Subtyping and Phylogenetic Analysis
2.5 Statistical Analysis
3. Results
3.1. Patient Characteristics
| Parameter | Naïve (n = 70) | Treated (n = 70) | p-Value |
|---|---|---|---|
| Age (Y), median (range) | 8 (2–16) | 10 (2–17) | 0.06 |
| Sex | 0.55 | ||
| Boys | 52 | 56 | |
| Girls | 18 | 14 | |
| CD4 count | 645 | 769 | 0.66 |
| cells/µL, median (range) | (17–2285) | (6–2269) | |
| Viral load | 38,900 | 1780 | 0.02 |
| RNA copies/mL, median (range) | (5190–228,000) | (47–38,200) |
3.2. Determination of Viral Subtype


| Patient ID | CD4 Count (Cells/µL) | Viral Load (RNA Copies/mL) | Subtype | T/N # | Major Drug Resistance Mutations | Minor Drug Resistance Mutations | Other Mutations * | Drug Regimen ** | Duration of Treatment | |
|---|---|---|---|---|---|---|---|---|---|---|
| Reverse Transcriptase | NRTI | NNRTI | ||||||||
| AIIMSU30 | 627 | <47 | B | T | D67E | L74Y | W88R, K102Q, L109Q, S162C, R206X, Q207X | NVP,LAM,STA | 2 Years 8 months | |
| AIIMSU35 | 837 | 1620 | C | T | M184V | K103N | W88C, K101Q, D121H, K122E, I135L, K173A, Q174R, D177E, I178L, E194A, G196E, T200A, Q207E | NVP,LAM,STA | 4 Years 1 month | |
| AIIMSU48 | 569 | NA | B | T | F227L | R206X, Q207X, L228X, M230E | LAM,STA,EFV | 4 Years | ||
| AIIMSU52 | 288 | NA | C | T | D67G | K65E | D121H, K122E, K173A, Q174R, D177E, T200A, Q207E, R211K | NVP,LAM,STA | 4 months | |
| AIIMSU56 | 698 | 27,500 | C | T | M184V | K103N | K73X, I135T, D177E, I178L, T200A, Q207E, R211K, F214L, L228F, M230D | NVP,LAM,STA | 6 Years | |
| AIIMSU58 | 979 | 5570 | B | N | K65E | K66E, R72E, L228F, M230N | ||||
| AIIMSU63 | 1528 | 34,200 | C | N | L74I | R72K, D76X, D121Y, K122E, D123E, K173A, R206X, Q207X, L228X, M230G | ||||
| AIIMSU76 | 1459 | 1459 | C | T | F77L | D76N, E79G, D121H, K122E, I135R, K173A, T200A, Q207E, R211K | NEV,LAM,ZDV | 1 Year | ||
| AIIMSU85 | 1027 | NA | C | N | L74Y | I63M, K64Q, T69X, R72K, K73i, I94K, D121Y, K122E, I135T, S162A, K173A, Q197K, T200A, R206X, Q207X, P226X, L228F | ||||
| AIIMSPD04 | 150 | 9480 | C | N | K219Q | P55S, V60I, D121Y, K122E, S162A, K173A, D177E, T200A, Q207A, R211K, F214X, D218R, H221S | ||||
| AIIMSPD05 | NA | <47 | C | N | V106A | L109P, K122A, D123S, K173A, D177E, I178L, T200A, Q207X | ||||
| AIIMSPD11 | 1222 | 39,000 | C | N | D67N | K101E, G190A | V60I, D121Y, K122E, I135K, S162A, K173A, D177E, T200A, Q207E, F214X | |||
| AIIMSPD12 | 225 | 585,000 | C | N | V179D | V60I, W88C, D121H, K122E, I135R, K173A, Q174R, D177E, T200A, I202V, Q207E | ||||
| AIIMSPD13 | 723 | NA | B | N | F227L | K73X, D121H, K122E, S162T, L228F | ||||
| AIIMSPD16 | NA | NA | B | N | V179F | D86H, G93 *, H96L, V106X, T107E, V118L, L120F, D121Q, D123Y, T128P, P133Q, I142M, Q145H, Q151R, E169Q, F171L, R206X, Q207X, W212R, P226A, Y232S, E233P, H235S, D237G | ||||
| Protease | ||||||||||
| AIIMS306 | 1284 | 13,100 | C | N | L10V | T12S, G16E, L19I, M36I, N37S, R41K, H69K, L89M, I93L | ||||
| AIIMSU40 | 225 | 24,000 | A | T | L10I | I13V, E35D, M36I, N37E, R41K, R57K, H69K, L89M | NVP,LAM,STA | 1 Year | ||
| AIIMSU59 | 1944 | NA | B | T | I84T | E34Q, L63P | NVP,LAM,STA | 2 Years 1 month | ||
| AIIMSU91 | 358 | 5190 | B | N | L76T | L63P, K70N, G73N, V75P, V77I, T80P | ||||
| AIIMSPD27 | 679 | NA | B | N | I84R | L63P, R87K, L97R | ||||
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Resino, S.; Bellon, J.M.; Resino, R.; Navarro, M.L.; Ramos, J.T.; de José, M.I.; Mellado, M.J.; Fernandez, M.A. Extensive implementation of highly active antiretroviral therapy shows great effect on survival and surrogate markers in vertically HIV-infected children. Clin. Infect. Dis. 2004, 38, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Fassinou, P.; Elenga, N.; Rouet, F.; Laguide, R.; Kouakoussui, K.A.; Timite, M.; Blanche, S.; Msellati, P. Highly active antiretroviral therapies among hiv-1-infected children in Abidjan, Cote d’Ivoire. AIDS 2004, 18, 1905–1913. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.A.; Keiser, O.; Technau, K.; Eley, B.; Rabie, H.; van Cutsem, G.; Giddy, J.; Wood, R.; Boulle, A.; Egger, M.; et al. Outcomes of the south african national antiretroviral treatment programme for children: The iedea southern africa collaboration. South Afr. Med. J. 2009, 99, 730–737. [Google Scholar]
- Wamalwa, D.C.; Farquhar, C.; Obimbo, E.M.; Selig, S.; Mbori-Ngacha, D.A.; Richardson, B.A.; Overbaugh, J.; Emery, S.; Wariua, G.; Gichuhi, C.; et al. Early response to highly active antiretroviral therapy in HIV-1-infected kenyan children. J. Acquir. Immune Defic. Syndr. 2007, 45, 311–317. [Google Scholar]
- Mugyenyi, P.; Walker, A.S.; Hakim, J.; Munderi, P.; Gibb, D.M.; Kityo, C.; Reid, A.; Grosskurth, H.; Darbyshire, J.H.; Ssali, F.; et al. Routine vs. clinically driven laboratory monitoring of HIV antiretroviral therapy in africa (dart): A randomised non-inferiority trial. Lancet 2009, 375, 123–131. [Google Scholar]
- Barry, O.; Powell, J.; Renner, L.; Bonney, E.Y.; Prin, M.; Ampofo, W.; Kusah, J.; Goka, B.; Sagoe, K.W.; Shabanova, V.; et al. Effectiveness of first-line antiretroviral therapy and correlates of longitudinal changes in cd4 and viral load among HIV-infected children in ghana. BMC Infect. Dis. 2013, 13, e476. [Google Scholar] [CrossRef]
- Brindeiro, P.C.A.; Brindeiro, R.M.; Mortensen, C.U.; Hertogs, K.; de Vroey, V.; Rubini, N.P.M.; Sion, F.S.; de Sá, C.A.M.; Machado, D.M.; Succi, R.C.M.; et al. Testing genotypic and phenotypic resistance in human immunodeficiency virus type 1 isolates of clade b and other clades from children failing antiretroviral therapy. J. Clin. Microbiol. 2002, 40, 4512–4519. [Google Scholar] [CrossRef]
- Machado, E.S.; Lambert, J.S.; Watson, D.C.; Afonso, A.O.; da Cunha, S.M.; Nogueira, S.A.; Caride, E.; Oliveira, R.H.; Sill, A.M.; DeVico, A.; et al. Genotypic resistance and HIV-1 subtype in brazilian children on dual and triple combination therapy. J. Clin. Virol. 2004, 30, 24–31. [Google Scholar] [CrossRef]
- Machado, D.M.; Fernandes, S.C.U.; Succi, R.C.L.D.M.; Freire, W.S.; Pannuti, C.U.S.R.; Gouveia, A.D.B.; Levi, J.E.; Diaz, R.S. Analysis of HIV- type 1 protease and reverse transcriptase in brazilian children failing highly active antiretroviral therapy (haart). Revista Do Instituto De Medicina Tropical De São Paulo 2005, 47, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dutta Choudhury, S.; Chaudhury, A.K.; Kalra, R.; Andrabi, R.; Wig, N.; Biswas, A.; Bala, M.; Luthra, K. Antiretroviral drug resistance mutations in the reverse transcriptase gene of HIV-1 isolates from northern indian patients: A follow-up study. Arch. Virol. 2010, 155, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Vartanian, J.P. HIV1 reverse transcriptase: An out-of-the-ordinary enzyme. Bull. l’Inst. Pasteur 1998, 96, 49–63. [Google Scholar] [CrossRef]
- Mullen, J.; Leech, S.; O’Shea, S.; Chrystie, I.L.; Du Mont, G.; Ball, C.; Sharland, M.; Cottam, F.; Zuckerman, M.; Rice, P.; et al. Antiretroviral drug resistance among HIV-1 infected children failing treatment. J. Med. Virol. 2002, 68, 299–304. [Google Scholar] [CrossRef]
- Rates of mother-to-child transmission of HiV-1 in africa, america, and europe: Results from 13 perinatal studies. The working group on mother-to-child transmission of HIV. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1995, 8, 506–510.
- Sehgal, S.; Pasricha, N.; Singh, S. High rate of mutation k103n causing resistance to nevirapine in indian children with acquired immunodeficiency syndrome. Indian J. Med. Microbiol. 2008, 26, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Soundararajan, L.; Karunaianandham, R.; Jauvin, V.; Schrive, M.H.; Ramachandran, R.; Narayanan, P.R.; Fleury, H.J.; Swaminathan, S. Characterization of hiv-1 isolates from antiretroviral drug-naive children in southern india. AIDS Res. Hum. Retrovir. 2007, 23, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Naco Guidelines for HIV Care and Treatment in Infants and Children. November 2006. Available online: http://www.Whoindia.Org/link-files/hiv-aids_naco_guidelines_on_art_for_paediatric_hiv_aids.Pdf (accessed on 25 November 2014).
- Stanford University. HIV Drug Resistance database. Available online: http://hivdb.Stanford.Edu (accessed on 14 November 2014).
- Tamura, K.; Dudley, J.; Nei, M.; Kumar, S. Mega4: Molecular evolutionary genetics analysis (mega) software version 4.0. Mol. Biol. Evol. 2007, 24, 1596–1599. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.S.; Andrabi, R.; Kumar, R.; Kabra, S.K.; Lodha, R.; Vajpayee, M.; Luthra, K. Binding antibody responses to the immunogenic regions of viral envelope in hiv-1-infected indian children. Viral Immunol. 2011, 24, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Das, M.; Chu, P.L.; Santos, G.M.; Scheer, S.; Vittinghoff, E.; McFarland, W.; Colfax, G.N. Decreases in community viral load are accompanied by reductions in new hiv infections in san francisco. PLoS One 2010, 5, e11068. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.S.; Lima, V.D.; Barrios, R.; Yip, B.; Wood, E.; Kerr, T.; Shannon, K.; Harrigan, P.R.; Hogg, R.S.; Daly, P.; et al. Association of highly active antiretroviral therapy coverage, population viral load, and yearly new hiv diagnoses in british columbia, canada: A population-based study. Lancet 2010, 376, 532–539. [Google Scholar] [CrossRef]
- Keller, M.; Lu, Y.; Lalonde, R.G.; Klein, M.B. Impact of HIV-1 viral subtype on CD4+ T-cell decline and clinical outcomes in antiretroviral naive patients receiving universal healthcare. AIDS 2009, 23, 731–737. [Google Scholar] [PubMed]
- Neogi, U.; Bontell, I.; Shet, A.; de Costa, A.; Gupta, S.; Diwan, V.; Laishram, R.S.; Wanchu, A.; Ranga, U.; Banerjea, A.C.; et al. Molecular epidemiology of hiv-1 subtypes in india: Origin and evolutionary history of the predominant subtype c. PLoS One 2012, 7, e39819. [Google Scholar] [CrossRef]
- Neogi, U.; Sood, V.; Ronsard, L.; Singh, J.; Lata, S.; Ramachandran, V.G.; Das, S.; Wanchu, A.; Banerjea, A.C. Genetic architecture of hiv-1 genes circulating in north india & their functional implications. Indian J. Med. Res. 2011, 134, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Delaugerre, C.; Chaix, M.-L.; Blanche, S.; Warszawski, J.; Cornet, D.; Dollfus, C.; Schneider, V.; Burgard, M.; Faye, A.; Mandelbrot, L.; et al. Perinatal acquisition of drug-resistant hiv-1 infection: Mechanisms and long-term outcome. Retrovirology 2009, 6, e85. [Google Scholar] [CrossRef] [Green Version]
- Verweel, G.; van Rossum, A.M.; Hartwig, N.G.; Wolfs, T.F.; Scherpbier, H.J.; de Groot, R. Treatment with highly active antiretroviral therapy in human immunodeficiency virus type 1-infected children is associated with a sustained effect on growth. Pediatrics 2002, 109, e25. [Google Scholar] [CrossRef] [PubMed]
- Soh, C.H.; Oleske, J.M.; Brady, M.T.; Spector, S.A.; Borkowsky, W.; Burchett, S.K.; Foca, M.D.; Handelsman, E.; Jimenez, E.; Dankner, W.M.; et al. Long-term effects of protease-inhibitor-based combination therapy on cd4 t-cell recovery in hiv-1-infected children and adolescents. Lancet 2003, 362, 2045–2051. [Google Scholar] [CrossRef]
- Kandathil, A.J.; Kannangai, R.; Abraham, O.C.; Sudarsanam, T.D.; Pulimood, S.A.; Sridharan, G. Genotypic resistance profile of hiv-1 protease gene: A preliminary report from vellore, south india. Indian J. Med. Microbiol. 2008, 26, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Schapiro, J.M.; Brenner, B.G.; Wainberg, M.A. The influence of protease inhibitor resistance profiles on selection of hiv therapy in treatment-naive patients. Antivir. Ther. 2004, 9, 301–314. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bure, D.; Makhdoomi, M.A.; Lodha, R.; Prakash, S.S.; Kumar, R.; Parray, H.A.; Singh, R.; Kabra, S.K.; Luthra, K. Mutations in the Reverse Transcriptase and Protease Genes of Human Immunodeficiency Virus-1 from Antiretroviral Naïve and Treated Pediatric Patients. Viruses 2015, 7, 590-603. https://0-doi-org.brum.beds.ac.uk/10.3390/v7020590
Bure D, Makhdoomi MA, Lodha R, Prakash SS, Kumar R, Parray HA, Singh R, Kabra SK, Luthra K. Mutations in the Reverse Transcriptase and Protease Genes of Human Immunodeficiency Virus-1 from Antiretroviral Naïve and Treated Pediatric Patients. Viruses. 2015; 7(2):590-603. https://0-doi-org.brum.beds.ac.uk/10.3390/v7020590
Chicago/Turabian StyleBure, Dinesh, Muzamil A. Makhdoomi, Rakesh Lodha, Somi Sankaran Prakash, Rajesh Kumar, Hilal A. Parray, Ravinder Singh, Sushil K. Kabra, and Kalpana Luthra. 2015. "Mutations in the Reverse Transcriptase and Protease Genes of Human Immunodeficiency Virus-1 from Antiretroviral Naïve and Treated Pediatric Patients" Viruses 7, no. 2: 590-603. https://0-doi-org.brum.beds.ac.uk/10.3390/v7020590