Nasal Administration and Plasma Pharmacokinetics of Parathyroid Hormone Peptide PTH 1-34 for the Treatment of Osteoporosis



Abstract
:1. Introduction
2. Materials
3. Methods
3.1. Preparation of Nasal Formulations for Clinical Study
3.2. Preparation of Nasal Formulations for Ovine Study
3.3. Healthy Human Volunteer Pharmacokinetic/Gamma Scintigraphy Study
3.3.1. Pharmacokinetics
- Cmax
- Tmax
- Terminal half-life (t1/2)
- AUC to 2 h (AUC0–2h)
- AUC to last measured time point (AUClast) and corresponding Frel for nasal formulation
3.3.2. Gamma Scintigraphy
3.3.3. Ovine Study
4. Results
4.1. Clinical Study
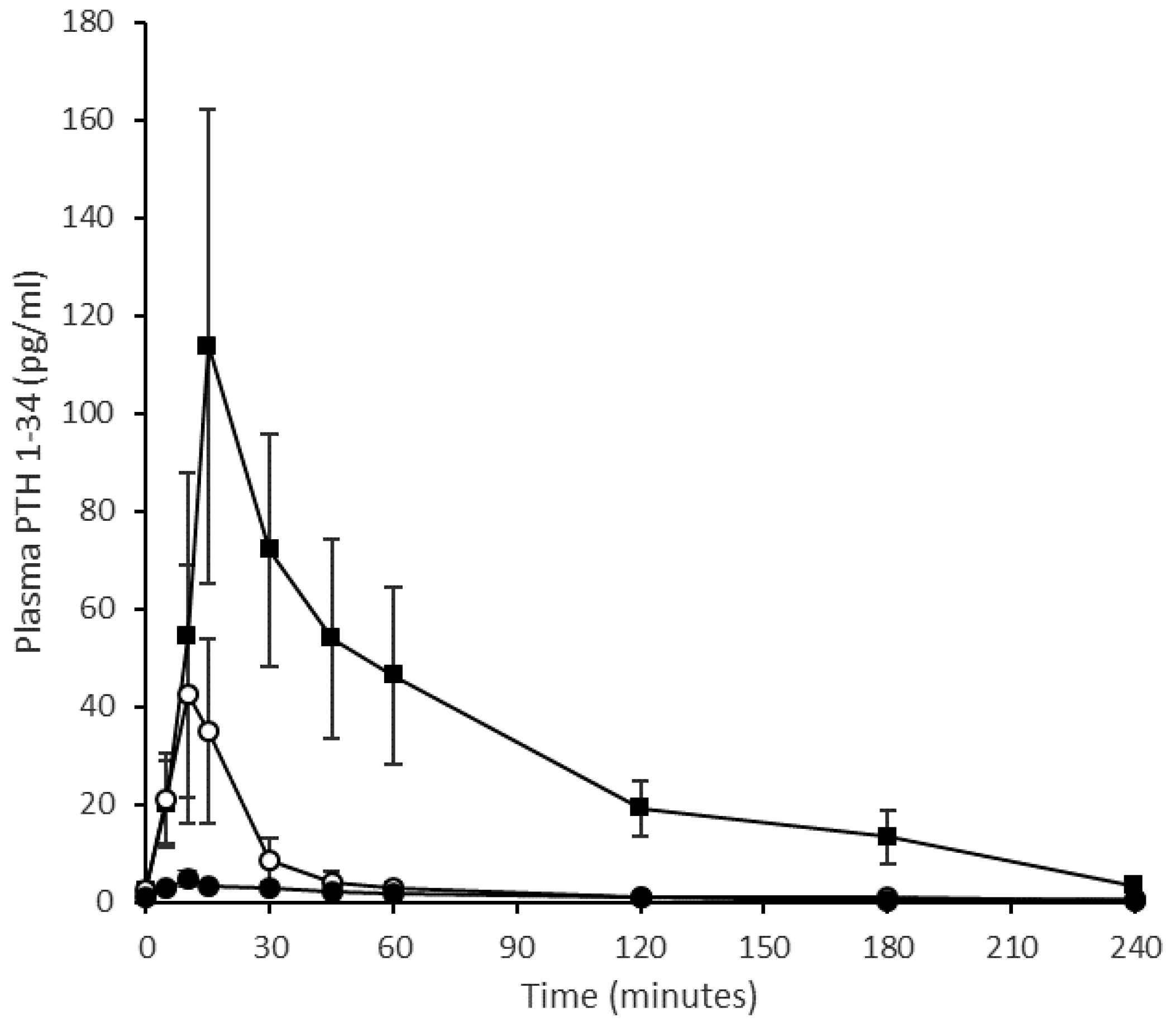
4.1.1. Pharmacokinetics
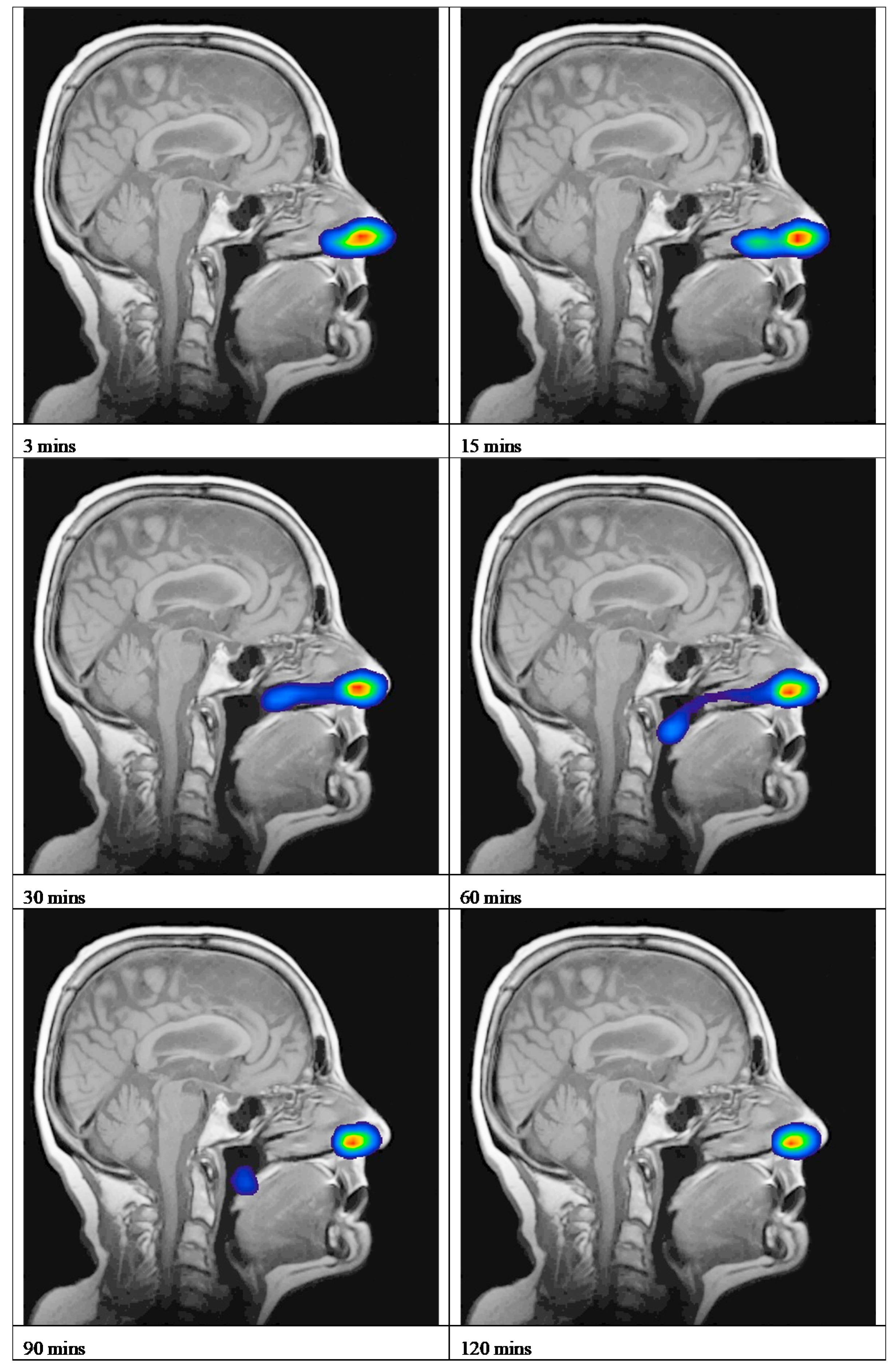
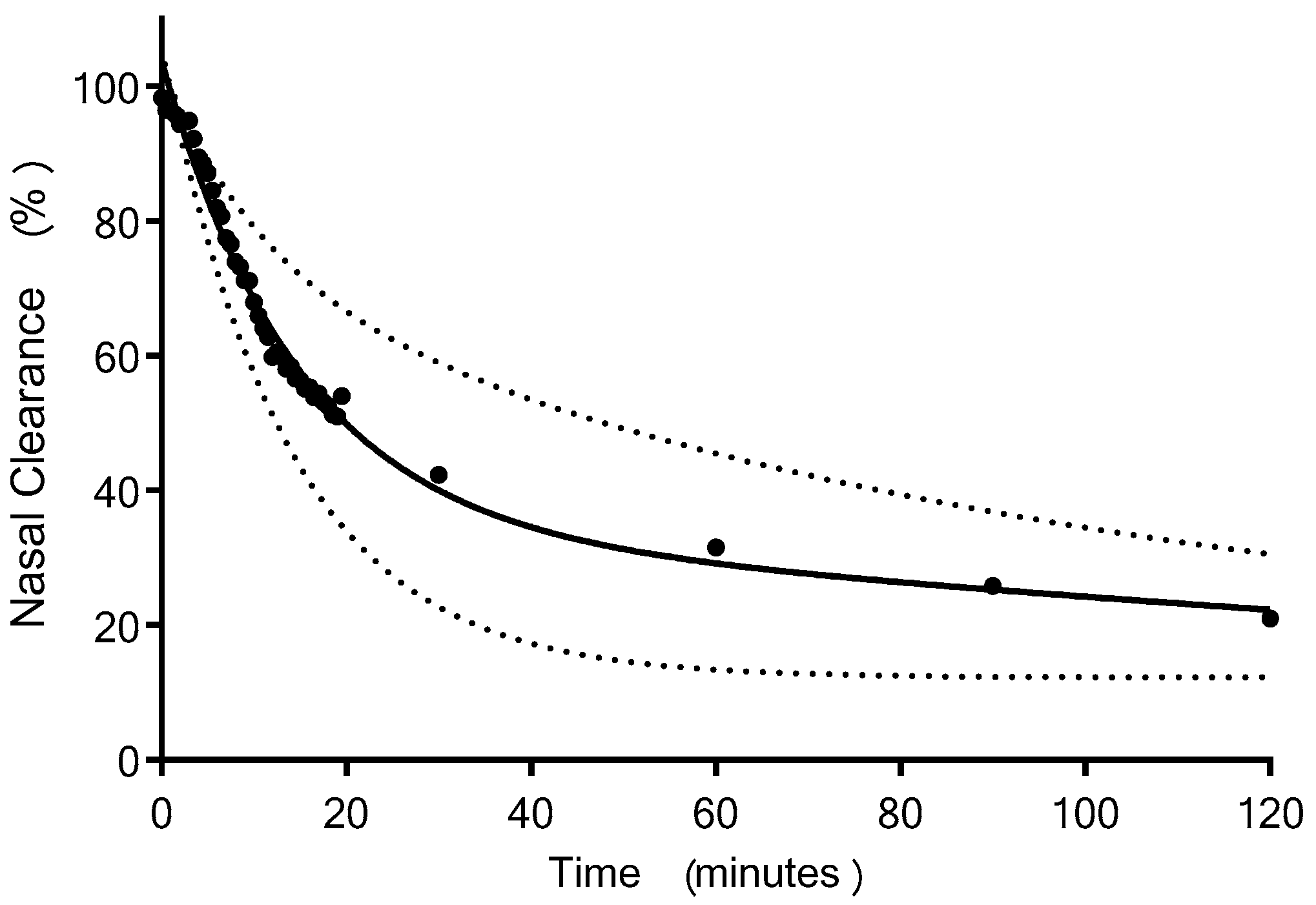
4.1.2. Gamma Scintigraphy
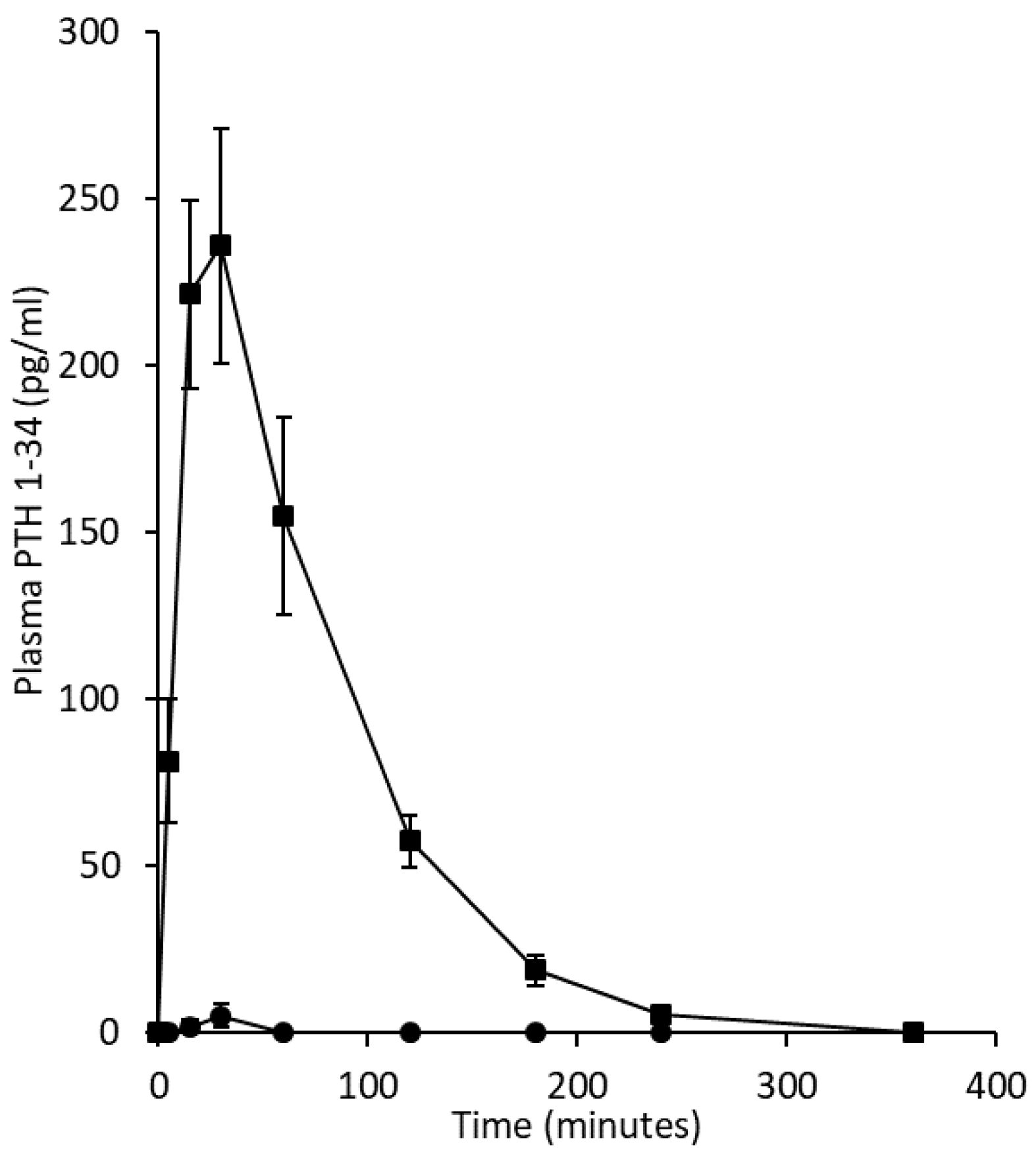
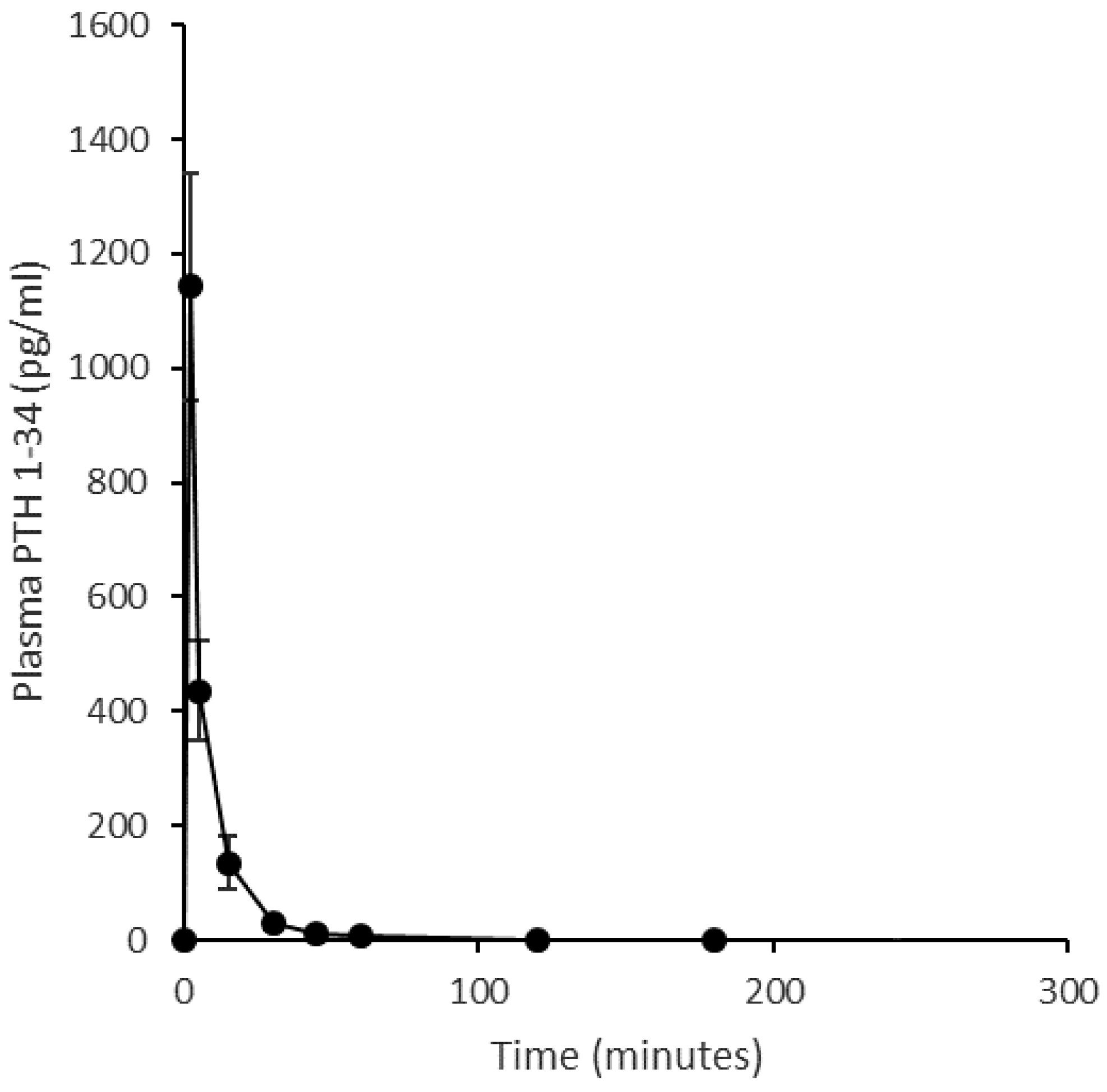
4.1.3. Ovine Study
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baron, R.; Hesse, E. Update on Bone Anabolics in Osteoporosis Treatment: Rationale, Current Status, and Perspectives. J. Clin. Endocrinol. Metab. 2012, 97, 311–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhiman, P.; Andersen, S.; Vestergaard, P.; Masud, T.; Qureshi, N. Does bone mineral density improve the predictive accuracy of fracture risk assessment? A prospective cohort study in Northern Denmark. BMJ Open 2018, 8, 018898. [Google Scholar] [CrossRef] [PubMed]
- Moppett, I.K.; Wiles, M.D.; Moran, C.G.; Sahota, O. The Nottingham Hip Fracture Score as a predictor of early discharge following fractured neck of femur. Age Ageing 2012, 41, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, M.J.; Moran, C.G.; Moppett, I.K. Development and validation of a preoperative scoring system to predict 30 day mortality in patients undergoing hip fracture surgery. Br. J. Anaesth. 2008, 101, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunning, T.; Dickinson, R.; Fagan, E.; Inman, D.; Johansen, A.; Judge, A.; Hannaford, J.; Liddicoat, M.; Wakeman, R. National Hip Fracture Database (NHFD) Annual Report 2018; Royal College of Physicians: London, UK, 2017. [Google Scholar]
- Modi, A.; Sajjan, S.; Insinga, R.; Weaver, J.; Lewiecki, E.M.; Harris, S.T. Frequency of discontinuation of injectable osteoporosis therapies in US patients over 2 years. Osteoporos. Int. 2017, 28, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.C.; Chang, C.H.C.; Lim, L.C.; Brnabic, A.J.M.; Tsauo, J.Y.; Burge, R.; Hsiao, F.Y.; Jin, L.; Gurbuz, S.; Yang, R.S. Association between teriparatide treatment persistence and adherence, and fracture incidence in Taiwan: Analysis using the National Health Insurance Research Database. Osteoporos. Int. 2016, 27, 2855–2865. [Google Scholar] [CrossRef] [PubMed]
- Fraenkel, L.; Gulanski, B.; Wittink, D. Patient treatment preferences for osteoporosis. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2006, 55, 729–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brayden, D.J.; Bzik, V.A.; Lewis, A.L.; Illum, L. CriticalSorb promotes permeation of flux markers across isolated rat intestinal mucosae and Caco-2 monolayers. Pharm. Res. 2012, 29, 2543–2554. [Google Scholar] [CrossRef] [PubMed]
- Illum, L. Nasal drug delivery—Recent developments and future prospects. J. Control. Release 2012, 161, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Illum, L.; Jordan, F.; Lewis, A.L. CriticalSorb (TM): A novel efficient nasal delivery system for human growth hormone based on Solutol HS15. J. Control. Release 2012, 162, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, J.; Lupo, N.; Bernkop-Schnurch, A. Advanced formulations for intranasal delivery of biologics. Int. J. Pharm. 2018, 553, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Maggio, E.T. Intravail™: Highly effective intranasal delivery of peptide and protein drugs AU-Maggio. Expert Opin. Drug Deliv. 2006, 3, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.J.; Jordan, F.; King, G.; Lewis, A.L.; Illum, L.; Masud, T.; Perkins, A.C.; Pearson, R.G. In vitro and preclinical assessment of an intranasal spray formulation of parathyroid hormone PTH 1-34 for the treatment of osteoporosis. Int. J. Pharm. 2018, 535, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Shubber, S.; Vllasaliu, D.; Rauch, C.; Jordan, F.; Illum, L.; Stolnik, S. Mechanism of Mucosal Permeability Enhancement of CriticalSorb (R) (Solutol (R) HS15) Investigated In Vitro in Cell Cultures. Pharm. Res. 2015, 32, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Soane, R.J.; Frier, M.; Perkins, A.C.; Jones, N.S.; Davis, S.S.; Illum, L. Evaluation of the clearance characteristics of bioadhesive systems in humans. Int. J. Pharm. 1999, 178, 55–65. [Google Scholar] [CrossRef]
- Illum, L. Nasal delivery. The use of animal models to predict performance in man. J. Drug Target. 1996, 3, 427–442. [Google Scholar] [CrossRef]
- Lewis, A.L.; Jordan, F.; Patel, T.; Jeffery, K.; King, G.; Savage, M.; Shalet, S.; Illum, L. Intranasal Human Growth Hormone (hGH) Induces IGF-1 Levels Comparable With Subcutaneous Injection With Lower Systemic Exposure to hGH in Healthy Volunteers. J. Clin. Endocrinol. Metab. 2015, 100, 4364–4371. [Google Scholar] [CrossRef]
- Satterwhite, J.; Heathman, M.; Miller, P.D.; Marin, F.; Glass, E.V.; Dobnig, H. Pharmacokinetics of Teriparatide (rhPTH 1–34) and Calcium Pharmacodynamics in Postmenopausal Women with Osteoporosis. Calcif. Tissue Int. 2010, 87, 485–492. [Google Scholar] [CrossRef]
- Joint Formulary Committee. British National Formulary, 72th ed.; BMJ Group and Pharmaceutical Press: London, UK, 2018. [Google Scholar]
- Takacs, I.; Jokai, E.; Kovats, D.E.; Aradi, I. The first biosimilar approved for the treatment of osteoporosis: Results of a comparative pharmacokinetic/pharmacodynamic study. Osteoporos. Int. 2019, 30, 675–683. [Google Scholar] [CrossRef]
- Basu, P.; Joglekar, G.; Rai, S.; Suresh, P.; Vernon, J. Analysis of Manufacturing Costs in Pharmaceutical Companies. J. Pharm. Innov. 2008, 3, 30–40. [Google Scholar] [CrossRef]
- Eli_Lilly. Highlights of Prescribing Information; AbbVie Inc.: North Chicago, IL, USA, 2014; Available online: https://pi.lilly.com/us/forteo-pi.pf (accessed on 20 November 2018).
- Haemmerle, S.P.; Mindeholm, L.; Launonen, A.; Kiese, B.; Loeffler, R.; Harfst, E.; Azria, M.; Arnold, M.; John, M.R. The single dose pharmacokinetic profile of a novel oral human parathyroid hormone formulation in healthy postmenopausal women. Bone 2012, 50, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Forssmann, W.-G.; Tillmann, H.-C.; Hock, D.; Forssmann, K.; Bernasconi, C.; Forssmann, U.; Richter, R.; Hocher, B.; Pfuetzner, A. Pharmacokinetic and Pharmacodynamic Characteristics of Subcutaneously Applied PTH-1-37. Kidney Blood Press. Res. 2016, 41, 507–518. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, K.; Andersen, J.R.; Riis, B.J.; Mehta, N.; Tavakkol, R.; Alexandersen, P.; Byrjalsen, I.; Valter, I.; Nedergaard, B.S.; Teglbjaerg, C.S.; et al. Evaluation of the efficacy, safety and pharmacokinetic profile of oral recombinant human parathyroid hormone rhPTH(1-31)NH2 in postmenopausal women with osteoporosis. Bone 2013, 53, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Shi, S.; Wu, J.; Li, Z.; Zhou, X.; Zeng, F. Safety, Tolerability, Pharmacokinetics and Pharmacodynamics of Recombinant Human Parathyroid Hormone after Single- and Multiple-Dose Subcutaneous Administration in Healthy Chinese Volunteers. Basic Clin. Pharmacol. Toxicol. 2012, 110, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Shiraki, M.; Hagino, H.; Iinuma, H.; Nakamura, T. Daily nasal spray of hPTH(1–34) for 3 months increases bone mass in osteoporotic subjects: A pilot study. Osteoporos. Int. 2006, 17, 1532–1538. [Google Scholar] [CrossRef] [PubMed]
- Brandt, G.C.; Spann, B.M.; Sileno, A.P.; Costantino, H.R.; Li, C.; Quay, S.C. Teriparatide nasal spray: Pharmacokinetics and safety versus subcutaneous teriparatide in healthy volunteers. Calcif. Tissue Int. 2006, 78, S45. [Google Scholar]
- Djupesland, P.G. Nasal drug delivery devices: Characteristics and performance in a clinical perspective—A review. Drug Deliv. Transl. Res. 2013, 3, 42–62. [Google Scholar] [CrossRef] [PubMed]
- McInnes, F.J.; O’Mahony, B.; Lindsay, B.; Band, J.; Wilson, C.G.; Hodges, L.A.; Stevens, H.N.E. Nasal residence of insulin containing lyophilised nasal insert formulations, using gamma scintigraphy. Eur. J. Pharm. Sci. 2007, 31, 25–31. [Google Scholar] [CrossRef]
- Takala, A.; Kaasalainen, V.; Seppala, T.; Kalso, E.; Olkkola, K.T. Pharmacokinetic comparison of intravenous and intranasal administration of oxycodone. Acta Anaesthesiol. Scand. 1997, 41, 309–312. [Google Scholar] [CrossRef]
- Djupesland, P.G.; Skretting, A. Nasal Deposition and Clearance in Man: Comparison of a Bidirectional Powder Device and a Traditional Liquid Spray Pump. J. Aerosol Med. Pulm. Drug Deliv. 2012, 25, 280–289. [Google Scholar] [CrossRef] [Green Version]
- Charlton, S.; Jones, N.S.; Davis, S.S.; Illum, L. Distribution and clearance of bioadhesive formulations from the olfactory region in man: Effect of polymer type and nasal delivery device. Eur. J. Pharm. Sci. 2007, 30, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghananeem, A.; Sandefer, E.; Doll, W.; C Page, R.; Chang, Y.; A Digenis, G. Gamma scintigraphy for testing bioequivalence: A case study on two cromolyn sodium nasal spray preparations. Int. J. Pharm. 2008, 357, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Soane, R.J.; Hinchcliffe, M.; Davis, S.S.; Illum, L. Clearance characteristics of chitosan based formulations in the sheep nasal cavity. Int. J. Pharm. 2001, 217, 183–191. [Google Scholar] [CrossRef]
- Masud, T.; Pearson, R.G. Nasally and sc Administered Teriparatide in Healthy Volunteers (NINTTO). Available online: https://clinicaltrials.gov/ct2/show/NCT01913834 (accessed on 5 June 2019).
- Ioannidis, J.P.A. Extrapolating from Animals to Humans. Sci. Transl. Med. 2012, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.H. The meaning of translational research and why it matters. JAMA J. Am. Med. Assoc. 2008, 299, 211–213. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Route | Nominal PTH Concentration (μg/mL) | Dose Volume (mL) | Dose Weight (mg) | Nominal PTH Dose (µg) |
|---|---|---|---|---|---|
| Solution # | intranasal | 1000 | 0.2 † | not applicable | 200 |
| Powder | intranasal | 10 ** | not applicable | 20 † (13 ± 1.5) § | 200 (130 ± 15) § |
| Solution * | subcutaneous | 40 | 0.5 | not applicable | 20 |
| Solution * | Intravenous | 40 | 0.5 ‡ | not applicable | 20 |
| Subcutaneous Injection (20 μg Teriparatide) * | Intranasal Spray (90 μg PTH 1-34) ‡ | |
|---|---|---|
| Cmax (pg/mL) | 252.5 | 5.2 |
| tmax (min) | 21.4 | 8.6 |
| t½ (min) | 64.8 | NC |
| AUC0–2h (pg·min/mL) | 17,381.9 | 242.3 |
| AUC0–last (pg·min/mL) | 20,725.6 | 242.3 |
| Intranasal Liquid (200 μg) | Intranasal Powder (200 μg 1) | Subcutaneous Injection (20 μg) | Intravenous Injection (20 μg) | |
|---|---|---|---|---|
| Cmax (pg/mL) | 47 ± 21 | 8 ± 3 | 121 ± 47 | 1142 ± 198 2 |
| Tmax (min) | 10 ± 2.0 (10) | 11 ± 6.6 (8) | 12 ± 1.5 (10) | 2 ± 0 (2) |
| t1/2 (min) | 109 ± 43.7 (77) | 96 ± 29.8 (71) | 54 ± 8.7 (47) | 75 ± 18.1 (78) |
| AUC0-last (pg·min/mL) | 1094 ± 410 | 317 ± 49 | 7197 ± 2204 | 10,660 ± 1888 |
| AUCINF (pg·min/mL) | 1222 ± 370 | 442 ± 41 | 7460 ± 2220 | 10,799 ± 1900 3 |
| Frel (%) 4 | 1.4 ± 0.31 | 1.0 ± 0.12 | 100 | 155.8 ± 24.0 |
| Fab (%) 5 | 1.1 ± 0.26 | 0.7 ± 0.03 | 77.0 ± 13.71 | 100 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearson, R.G.; Masud, T.; Blackshaw, E.; Naylor, A.; Hinchcliffe, M.; Jeffery, K.; Jordan, F.; Shabir-Ahmed, A.; King, G.; Lewis, A.L.; et al. Nasal Administration and Plasma Pharmacokinetics of Parathyroid Hormone Peptide PTH 1-34 for the Treatment of Osteoporosis. Pharmaceutics 2019, 11, 265. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics11060265
Pearson RG, Masud T, Blackshaw E, Naylor A, Hinchcliffe M, Jeffery K, Jordan F, Shabir-Ahmed A, King G, Lewis AL, et al. Nasal Administration and Plasma Pharmacokinetics of Parathyroid Hormone Peptide PTH 1-34 for the Treatment of Osteoporosis. Pharmaceutics. 2019; 11(6):265. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics11060265
Chicago/Turabian StylePearson, Richard G., Tahir Masud, Elaine Blackshaw, Andrew Naylor, Michael Hinchcliffe, Kirk Jeffery, Faron Jordan, Anjumn Shabir-Ahmed, Gareth King, Andrew L. Lewis, and et al. 2019. "Nasal Administration and Plasma Pharmacokinetics of Parathyroid Hormone Peptide PTH 1-34 for the Treatment of Osteoporosis" Pharmaceutics 11, no. 6: 265. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics11060265