Recent Advances in the Design of Topical Ophthalmic Delivery Systems in the Treatment of Ocular Surface Inflammation and Their Biopharmaceutical Evaluation

Abstract
:1. Introduction
2. NSAIDs, SAIDs, and Immunosuppressive Agents
2.1. Chemical Family
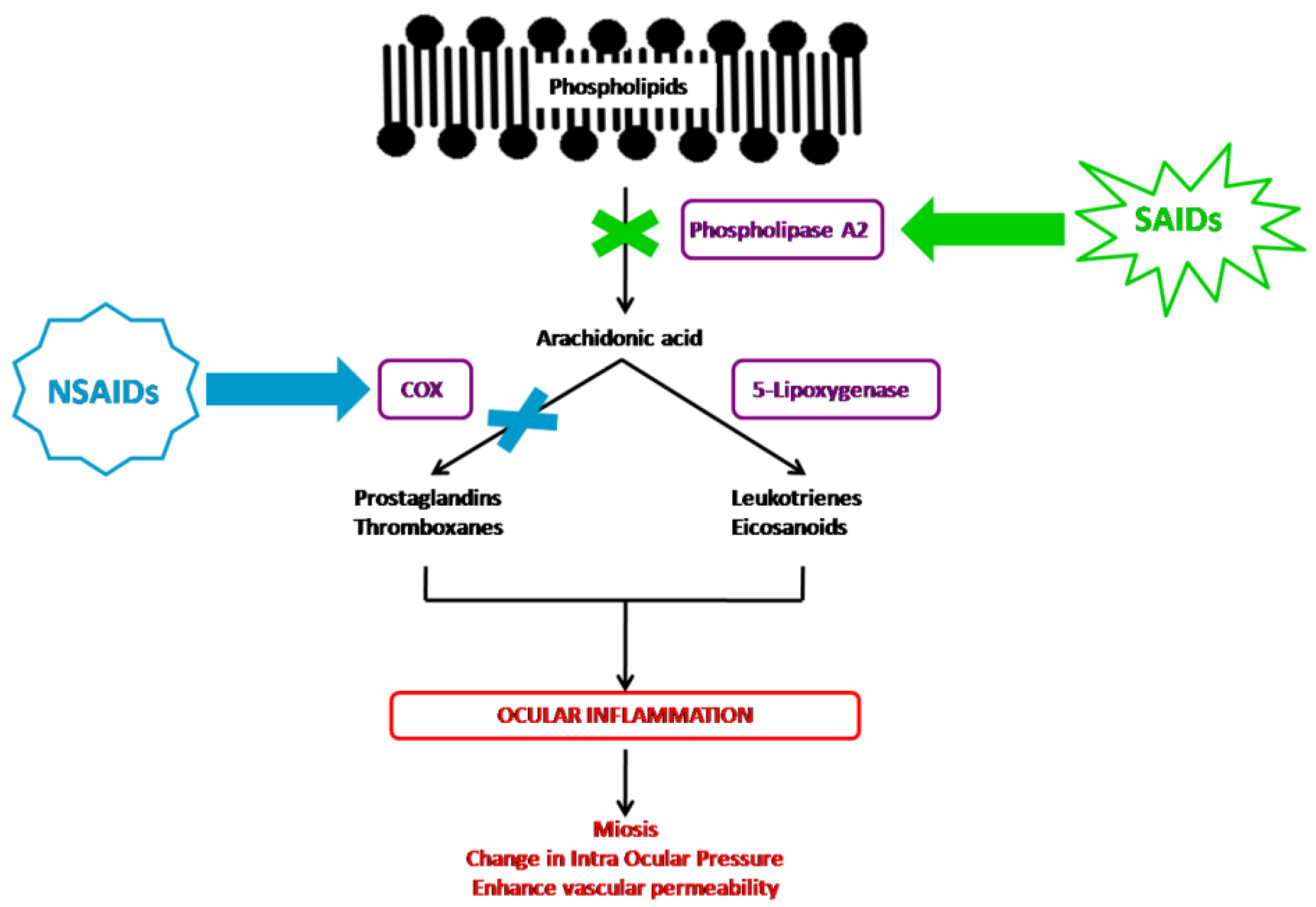
2.2. Mechanism of Action
2.3. Sites of Action/Therapeutic Uses
2.4. Side Effects
3. Formulation for Topical Ophthalmic Drug Delivery Systems
3.1. Conventional Formulation
3.1.1. Ointments
3.1.2. Eye Drops
Solutions
Suspensions
3.1.3. Gels
3.1.4. Emulsions
3.1.5. Use of Penetration Enhancers
3.2. Original Formulations
3.2.1. Contact Lens
3.2.2. Ophthalmic Insert
3.2.3. Micro and Nanocarriers for Ocular Drug Delivery
3.2.4. Combined Strategies
4. Current Biopharmaceutical Attributes of Topical Ophthalmic Formulations
4.1. Sterility Tests and Physicochemical Attributes
4.1.1. Sterility Tests
- -
- Fluid thioglycolate medium with resazurin, used for the growth of aerobic and anaerobic bacteria incubated at 30–35 °C; and
- -
- Soy-bean casein digest medium, used for the growth of aerobic bacteria and fungi incubated at 20–25 °C.
4.1.2. Clarity Examinations
4.1.3. Osmolality and PH
4.1.4. Rheological Characterization
4.1.5. Mucoadhesion Tests
4.1.6. Characterization of the Particle Size and Morphology
4.1.7. Zeta Potential Measurement
4.1.8. Drug and Preservative Contents
4.1.9. Stability Study
4.1.10. In Vitro Drug Release Study
4.2. Biological Evaluations
4.2.1. Toxicity and Biocompatibility Tests
In Vitro Tests
Ex Vivo Tests
In Vivo Tests
In Silico Tests
4.2.2. Pharmacokinetic Studies
Ex Vivo Transcorneal Permeation Studies
In Vivo Tests
4.2.3. Efficacy Testing
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahuja, M.; Dhake, A.S.; Sharma, S.K.; Majumdar, D.K. Topical ocular delivery of NSAIDs. AAPS J. 2008, 10, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Behar-Cohen, F. Towards an Optimized Use of Ocular Corticosteroids: EURETINA Award Lecture 2017. Ophthalmologica 2018, 240, 111–119. [Google Scholar] [CrossRef]
- Schalnus, R. Topical nonsteroidal anti-inflammatory therapy in ophthalmology. Ophthalmologica 2003, 217, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.J.; Schutte, S.M.; Abel, S.R. Comparing the Efficacy of Ophthalmic NSAIDs in Common Indications: A Literature Review to Support Cost-effective Prescribing. Ann. Pharm. 2015, 49, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Suresh, P.K.; Sah, A.K. Patent perspectives for corticosteroids based ophthalmic therapeutics. Recent Pat. Drug Deliv. 2014, 8, 206–223. [Google Scholar] [CrossRef] [PubMed]
- Lallemand, F.; Schmitt, M.; Bourges, J.-L.; Gurny, R.; Benita, S.; Garrigue, J.-S. Cyclosporine A delivery to the eye: A comprehensive review of academic and industrial efforts. Eur. J. Pharm. Biopharm. 2017, 117, 14–28. [Google Scholar] [CrossRef]
- Deveney, T.; Asbell, P.A. Patient and physician perspectives on the use of cyclosporine ophthalmic emulsion 0.05% for the management of chronic dry eye. Clin. Ophthalmol. 2018, 12, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Kompella, U.B.; Kadam, R.S.; Lee, V.H.L. Recent advances in ophthalmic drug delivery. Delivery 2010, 1, 435–456. [Google Scholar] [CrossRef] [Green Version]
- Gause, S.; Hsu, K.-H.; Shafor, C.; Dixon, P.; Powell, K.C.; Chauhan, A. Mechanistic modeling of ophthalmic drug delivery to the anterior chamber by eye drops and contact lenses. Adv. Colloid Interface Sci. 2016, 233, 139–154. [Google Scholar] [CrossRef] [Green Version]
- Koç, F.E.; Senel, M. Solubility enhancement of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) using polypolypropylene oxide core PAMAM dendrimers. Int. J. Pharm. 2013, 451, 18–22. [Google Scholar] [CrossRef]
- Moya-Ortega, M.D.; Messner, M.; Jansook, P.; Nielsen, T.T.; Wintgens, V.; Larsen, K.L.; Amiel, C.; Sigurdsson, H.H.; Loftsson, T. Drug loading in cyclodextrin polymers: Dexamethasone model drug. J. Incl. Phenom. Macrocycl. Chem. 2011, 69, 377–382. [Google Scholar] [CrossRef]
- Lallemand, F.; Perottet, P.; Felt-Baeyens, O.; Kloeti, W.; Philippoz, F.; Marfurt, J.; Besseghir, K.; Gurny, R. A water-soluble prodrug of cyclosporine A for ocular application: A stability study. Eur. J. Pharm. Sci. 2005, 26, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, R.S.; Braga-Mele, R.; Donaldson, K.; Emerick, G.; Henderson, B.; Kahook, M.; Mamalis, N.; Miller, K.M.; Realini, T.; Shorstein, N.H.; et al. Cataract surgery and nonsteroidal antiinflammatory drugs. J. Cataract Refract. Surg. 2016, 42, 1368–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, R.K.; Melton, R. Unleash the power of corticosteroids. Rev. Optom. 2016, 26–32. [Google Scholar]
- Sheppard, J.D.; Comstock, T.L.; Cavet, M.E. Impact of the Topical Ophthalmic Corticosteroid Loteprednol Etabonate on Intraocular Pressure. Adv. Ther. 2016, 33, 532–552. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.L.; Gilger, B.C.; Robinson, M.R. Novel approaches to ocular drug delivery. Curr. Opin. Mol. 2004, 6, 195–205. [Google Scholar]
- Ke, T.L.; Graff, G.; Spellman, J.M.; Yanni, J.M. Nepafenac, a unique nonsteroidal prodrug with potential utility in the treatment of trauma-induced ocular inflammation: II. In vitro bioactivation and permeation of external ocular barriers. Inflammation 2000, 24, 371–384. [Google Scholar] [CrossRef]
- Lindstrom, R.; Kim, T. Ocular permeation and inhibition of retinal inflammation: An examination of data and expert opinion on the clinical utility of nepafenac. Curr. Med. Res. Opin. 2006, 22, 397–404. [Google Scholar] [CrossRef]
- Lallemand, F.; Felt-Baeyens, O.; Rudaz, S.; Hamel, A.R.; Hubler, F.; Wenger, R.; Mutter, M.; Besseghir, K.; Gurny, R. Conversion of cyclosporine A prodrugs in human tears vs rabbits tears. Eur. J. Pharm. Biopharm. 2005, 59, 51–56. [Google Scholar] [CrossRef]
- Lallemand, F.; Varesio, E.; Felt-Baeyens, O.; Bossy, L.; Hopfgartner, G.; Gurny, R. Biological conversion of a water-soluble prodrug of cyclosporine A. Eur. J. Pharm. Biopharm. 2007, 67, 555–561. [Google Scholar] [CrossRef]
- Lallemand, F.; Furrer, P.; Felt-Baeyens, O.; Gex-Fabry, M.; Dumont, J.-M.; Besseghir, K.; Gurny, R. A novel water-soluble cyclosporine A prodrug: Ocular tolerance and in vivo kinetics. Int. J. Pharm. 2005, 295, 7–14. [Google Scholar] [CrossRef]
- Bourges, J.L.; Lallemand, F.; Agla, E.; Besseghir, K.; Dumont, J.M.; BenEzra, D.; Gurny, R.; Behar-Cohen, F. Evaluation of a topical cyclosporine A prodrug on corneal graft rejection in rats. Mol. Vis. 2006, 12, 1461–1466. [Google Scholar] [PubMed]
- Rodriguez-Aller, M.; Kaufmann, B.; Guillarme, D.; Stella, C.; Furrer, P.; Rudaz, S.; El Zaoui, I.; Valamanesh, F.; Di Tommaso, C.; Behar-Cohen, F.; et al. In vivo characterisation of a novel water-soluble Cyclosporine A prodrug for the treatment of dry eye disease. Eur. J. Pharm. Biopharm. 2012, 80, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Aller, M.; Guillarme, D.; El Sanharawi, M.; Behar-Cohen, F.; Veuthey, J.-L.; Gurny, R. In vivo distribution and ex vivo permeation of cyclosporine A prodrug aqueous formulations for ocular application. J. Control Rel. 2013, 170, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Rupenthal, I.D. Modern approaches to the ocular delivery of cyclosporine A. Drug Discov. Today 2016, 21, 977–988. [Google Scholar] [CrossRef]
- Taskar, P.; Tatke, A.; Majumdar, S. Advances in the use of prodrugs for drug delivery to the eye. Exp. Opin. Drug Deliv. 2017, 14, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D. Ocular Drug Delivery: Present Innovations and Future Challenges. J. Pharm. Exp. 2019, 370, 602–624. [Google Scholar] [CrossRef]
- Lobo, A.-M.; Sobrin, L.; Papaliodis, G.N. Drug Delivery Options for the Treatment of Ocular Inflammation. Semin. Ophthalmol. 2010, 25, 283–288. [Google Scholar] [CrossRef]
- Janagam, D.R.; Wu, L.; Lowe, T.L. Nanoparticles for drug delivery to the anterior segment of the eye. Adv. Drug Deliv. Rev. 2017, 122, 31–64. [Google Scholar] [CrossRef]
- Lalu, L.; Tambe, V.; Pradhan, D.; Nayak, K.; Bagchi, S.; Maheshwari, R.; Kalia, K.; Tekade, R.K. Novel nanosystems for the treatment of ocular inflammation: Current paradigms and future research directions. J. Control Release 2017, 268, 19–39. [Google Scholar] [CrossRef]
- Cholkar, K.; Patel, S.P.; Vadlapudi, A.D.; Mitra, A.K. Novel strategies for anterior segment ocular drug delivery. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2013, 29, 106–123. [Google Scholar] [CrossRef] [Green Version]
- Kwatra, G.; Mukhopadhyay, S. Topical Corticosteroids: Pharmacology. In A Treatise on Topical Corticosteroids in Dermatology; Lahiri, K., Ed.; Springer Singapore: Singapore, 2018; pp. 11–22. ISBN 978-981-10-4608-7. [Google Scholar]
- Einhorn, M. Similarities between Corticosteroids. Sci. J. Lander Coll. Arts Sci. 2014, 7, 38–45. [Google Scholar]
- Comstock, T.L.; Decory, H.H. Advances in corticosteroid therapy for ocular inflammation: Loteprednol etabonate. Int. J. Inflam. 2012, 2012, 789623. [Google Scholar] [CrossRef] [PubMed]
- Koay, P. The emerging roles of topical non-steroidal anti-inflammatory agents in ophthalmology. Br. J. Ophthalmol. 1996, 80, 480–485. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.M. Clinical pharmacokinetics of tiaprofenic acid and its enantiomers. Clin. Pharm. 1996, 31, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Roth, S.H. Rationale for using nabumetone and clinical experience. Drugs 2000, 59, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Cremonesi, G.; Cavalieri, L. Efficacy and safety of morniflumate for the treatment of symptoms associated with soft tissue inflammation. J. Int. Med. Res. 2015, 43, 290–302. [Google Scholar] [CrossRef] [Green Version]
- Raguenes-Nicol, C.; Russo-Marie, F.; Domage, G.; Diab, N.; Solito, E.; Dray, F.; Mace, J.L.; Streichenberger, G. Anti-inflammatory mechanism of alminoprofen: Action on the phospholipid metabolism pathway. Biochem. Pharm. 1999, 57, 433–443. [Google Scholar] [CrossRef]
- Kowalski, M.L.; Makowska, J.S. Seven Steps to the Diagnosis of NSAIDs Hypersensitivity: How to Apply a New Classification in Real Practice? Allergy Asthma Immunol. Res. 2015, 7, 312. [Google Scholar] [CrossRef] [Green Version]
- Rhen, T.; Cidlowski, J.A. Antiinflammatory Action of Glucocorticoids—New Mechanisms for Old Drugs. N. Eng. J. Med. 2005, 1611–1723. [Google Scholar] [CrossRef] [Green Version]
- Campbell, W.; Haluska, P. Lipid Derived Autocoids. In Goodman and Gilman’s the Pharmacological Basisi of Therapeutics, 9th ed.; Hardman, J.G., Limbird, L.E., Eds.; Chapter 26; Mc Graw-Hill: New York, NY, USA, 1990. [Google Scholar]
- Gaynes, B.I.; Fiscella, R. Topical nonsteroidal anti-inflammatory drugs for ophthalmic use: A safety review. Drug Saf. 2002, 25, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Hulin, A. Today in molecular mechanisms of immunosuppressive drugs actions: Roles of pharmacist. Ann. Pharm. Fr. 2008, 66, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Kronke, M.; Leonard, W.J.; Depper, J.M.; Arya, S.K.; Wong-Staal, F.; Gallo, R.C.; Waldmann, T.A.; Greene, W.C. Cyclosporin A inhibits T-cell growth factor gene expression at the level of mRNA transcription. Proc. Natl. Acad. Sci. USA 1984, 81, 5214–5218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klahr, S.; Ishidoya, S.; Morrissey, J. Role of angiotensin II in the tubulointerstitial fibrosis of obstructive nephropathy. Am. J. Kidney Dis. 1995, 26, 141–146. [Google Scholar] [CrossRef]
- Kiefer, F.; Tibbles, L.A.; Anafi, M.; Janssen, A.; Zanke, B.W.; Lassam, N.; Pawson, T.; Woodgett, J.R.; Iscove, N.N. HPK1, a hematopoietic protein kinase activating the SAPK/JNK pathway. EMBO J. 1996, 15, 7013–7025. [Google Scholar] [CrossRef]
- Granelli-Piperno, A. In situ hybridization for interleukin 2 and interleukin 2 receptor mRNA in T cells activated in the presence or absence of cyclosporin A. J. Exp. Med. 1988, 168, 1649–1658. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, L.A.; Clipstone, N.A.; Ho, S.N.; Northrop, J.P.; Crabtree, G.R. Rapid shuttling of NF-AT in discrimination of Ca2+ signals and immunosuppression. Nature 1996, 383, 837–840. [Google Scholar] [CrossRef]
- Molkentin, J.D.; Lu, J.-R.; Antos, C.L.; Markham, B.; Richardson, J.; Robbins, J.; Grant, S.R.; Olson, E.N. A Calcineurin-Dependent Transcriptional Pathway for Cardiac Hypertrophy. Cell 1998, 93, 215–228. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.; Wairkar, S. Recent advances in cyclosporine drug delivery: Challenges and opportunities. Drug Deliv. Transl. Res. 2019, 9, 1067–1081. [Google Scholar] [CrossRef]
- Rodríguez Villanueva, J.; Rodríguez Villanueva, L.; Guzmán Navarro, M. Pharmaceutical technology can turn a traditional drug, dexamethasone into a first-line ocular medicine. A global perspective and future trends. Int. J. Pharm. 2017, 516, 342–351. [Google Scholar] [CrossRef]
- Fel, A.; Aslangul, E.; Le Jeunne, C. Eye and corticosteroid’s use. Presse Med. 2012, 41, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, E.B.; Farah, M.E.; Bottós, J.M.; Bom Aggio, F. Nonsteroidal Anti-Inflammatory Drugs in the Treatment of Retinal Diseases. Dev. Ophthalmol. 2016, 55, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Sall, K.; Stevenson, O.D.; Mundorf, T.K.; Reis, B.L. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease11Reprint requests to: Linda Lewis, 575 Anton Blvd, Suite 900, Costa Mesa, CA 92626. Ophthalmology 2000, 107, 631–639. [Google Scholar] [CrossRef]
- Iwamoto, S.; Koga, T.; Ohba, M.; Okuno, T.; Koike, M.; Murakami, A.; Matsuda, A.; Yokomizo, T. Non-steroidal anti-inflammatory drug delays corneal wound healing by reducing production of 12-hydroxyheptadecatrienoic acid, a ligand for leukotriene B4 receptor 2. Sci. Rep. 2017, 7, 13267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nebbioso, M.; Alisi, L.; Giovannetti, F.; Armentano, M.; Lambiase, A. Eye drop emulsion containing 0.1% cyclosporin (1 mg/mL) for the treatment of severe vernal keratoconjunctivitis: An evidence-based review and place in therapy. OPTH 2019, 13, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Ding, S. Recent developments in ophthalmic drug delivery. PSTT 1998, 1, 328–335. [Google Scholar] [CrossRef]
- Sasaki, H.; Yamamura, K.; Nishida, K.; Nakamura, J.; Ichikawa, M. Delivery of drugs to the eye by topical application. Prog. Retin. Eye Res. 1996, 15, 583–620. [Google Scholar] [CrossRef]
- Ali, Y.; Lehmussaari, K. Industrial perspective in ocular drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1258–1268. [Google Scholar] [CrossRef]
- Hui, H.W.; Robinson, J.R. Effect of particle dissolution rate on ocular drug bioavailability. J. Pharm. Sci. 1986, 75, 280–287. [Google Scholar] [CrossRef]
- Yellepeddi, V.K.; Palakurthi, S. Recent Advances in Topical Ocular Drug Delivery. J. Ocul. Pharm. 2016, 32, 67–82. [Google Scholar] [CrossRef]
- Gaynes, B.I.; Onyekwuluje, A. Topical ophthalmic NSAIDs: A discussion with focus on nepafenac ophthalmic suspension. Clin. Ophthalmol. 2008, 2, 355–368. [Google Scholar] [CrossRef] [Green Version]
- Scoper, S.V.; Kabat, A.G.; Owen, G.R.; Stroman, D.W.; Kabra, B.P.; Faulkner, R.; Kulshreshtha, A.K.; Rusk, C.; Bell, B.; Jamison, T.; et al. Ocular distribution, bactericidal activity and settling characteristics of TobraDex ST ophthalmic suspension compared with TobraDex ophthalmic suspension. Advance 2008, 25, 77–88. [Google Scholar] [CrossRef]
- Nanjundswami, N.G.; Dasankoppa, F.S.; Sholapur, H.N. A Review on Hydrogels and Its Use in In Situ Ocular Drug Delivery. Indian J. Nov. Drug Deliv. 2009, 1, 11–17. [Google Scholar]
- Kirchhof, S.; Gregoritza, M.; Messmann, V.; Hammer, N.; Goepferich, A.M.; Brandl, F.P. Diels-Alder hydrogels with enhanced stability: First step toward controlled release of bevacizumab. Eur. J. Pharm. Biopharm. 2015, 96, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Gan, L.; Wang, J.; Jiang, M.; Bartlett, H.; Ouyang, D.; Eperjesi, F.; Liu, J.; Gan, Y. Recent advances in topical ophthalmic drug delivery with lipid-based nanocarriers. Drug Discov. Today 2013, 18, 290–297. [Google Scholar] [CrossRef]
- Stringer, W.; Bryant, R. Dose uniformity of topical corticosteroid preparations: Difluprednate ophthalmic emulsion 0.05% versus branded and generic prednisolone acetate ophthalmic suspension 1%. Clin. Ophthalmol. 2010, 4, 1119–1124. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, M.; Yasueda, S.; Isowaki, A.; Yamamoto, M.; Kimura, M.; Inada, K.; Ohtori, A. Formulation of an ophthalmic lipid emulsion containing an anti-inflammatory steroidal drug, difluprednate. Int. J. Pharm. 2005, 301, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Ames, P.; Galor, A. Cyclosporine ophthalmic emulsions for the treatment of dry eye: A review of the clinical evidence. Clin. Investig. (Lond.) 2015, 5, 267–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, T.; Dutot, M.; Christon, R.; Beaudeux, J.-L.; Martin, C.; Warnet, J.-M.; Rat, P. Benefits and side effects of different vegetable oil vectors on apoptosis, oxidative stress, and P2X7 cell death receptor activation. Investig. Ophthalmol. Vis. Sci. 2007, 48, 5000–5006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Human Medicine European Public Assessment Report: IKERVIS; European Medicines Agency: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Lallemand, B.; Ouedraogo, M.; Wauthoz, N.; Lamkami, T.; Mathieu, V.; Jabin, I.; Amighi, K.; Kiss, R.; Dubois, J.; Goole, J. Synthesis and plasma pharmacokinetics in CD-1 mice of a 18β-glycyrrhetinic acid derivative displaying anti-cancer activity: Pharmacokinetics of a GA derivative. J. Pharm. Pharmacol. 2013, 65, 402–410. [Google Scholar] [CrossRef]
- Lallemand, F.; Daull, P.; Benita, S.; Buggage, R.; Garrigue, J.-S. Successfully Improving Ocular Drug Delivery Using the Cationic Nanoemulsion, Novasorb. J. Drug Deliv. 2012, 2012, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, Y.I. A comparative review of Haute Autorité de Santé and National Institute for Health and Care Excellence health technology assessments of Ikervis® to treat severe keratitis in adult patients with dry eye disease which has not improved despite treatment with tear substitutes. J. Mark. Access Health Policy 2017, 5, 1336043. [Google Scholar] [CrossRef] [PubMed]
- Morrison, P.W.J.; Khutoryanskiy, V.V. Enhancement in corneal permeability of riboflavin using calcium sequestering compounds. Int. J. Pharm. 2014, 472, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moiseev, R.V.; Morrison, P.W.J.; Steele, F.; Khutoryanskiy, V.V. Penetration Enhancers in Ocular Drug Delivery. Pharmaceutics 2019, 11, 321. [Google Scholar] [CrossRef] [Green Version]
- Morrison, P.W.J.; Connon, C.J.; Khutoryanskiy, V.V. Cyclodextrin-mediated enhancement of riboflavin solubility and corneal permeability. Mol. Pharm. 2013, 10, 756–762. [Google Scholar] [CrossRef]
- Edsman, K.; Hägerström, H. Pharmaceutical applications of mucoadhesion for the non-oral routes. J. Pharm. Pharm. 2005, 57, 3–22. [Google Scholar] [CrossRef]
- Sampath Kumar, K.; Bhowmik, D.; Harish, G.; Duraivel, S.; Pragathi Kumar, B. Ocular Inserts: A Novel Controlled Drug Delivery System. Pharma Innov. J. 2012, 1, 1–16. [Google Scholar]
- Addo, R.T. Ocular Drug Delivery: Advances, Challenges and Applications; Springer: Berlin, Germany, 2016; ISBN 978-3-319-47691-9. [Google Scholar]
- Jervis, L.P. A Summary of Recent Advances in Ocular Inserts and Implants. J. Bioequivalence Bioavailab. 2017, 9, 320–323. [Google Scholar] [CrossRef]
- Souto, E.B.; Dias-Ferreira, J.; López-Machado, A.; Ettcheto, M.; Cano, A.; Camins Espuny, A.; Espina, M.; Garcia, M.L.; Sánchez-López, E. Advanced Formulation Approaches for Ocular Drug Delivery: State-Of-The-Art and Recent Patents. Pharmaceutics 2019, 11, 460. [Google Scholar] [CrossRef] [Green Version]
- Nagarwal, R.C.; Kant, S.; Singh, P.N.; Maiti, P.; Pandit, J.K. Polymeric nanoparticulate system: A potential approach for ocular drug delivery. J. Control Release 2009, 136, 2–13. [Google Scholar] [CrossRef]
- Araújo, J.; Gonzalez, E.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Nanomedicines for ocular NSAIDs: Safety on drug delivery. Nanomedicine 2009, 5, 394–401. [Google Scholar] [CrossRef]
- Lakhani, P.; Patil, A.; Majumdar, S. Recent advances in topical nano drug-delivery systems for the anterior ocular segment. Delivery 2018, 9, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Mandal, A.; Bisht, R.; Rupenthal, I.D.; Mitra, A.K. Polymeric micelles for ocular drug delivery: From structural frameworks to recent preclinical studies. J. Control Release 2017, 248, 96–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansook, P.; Pichayakorn, W.; Muankaew, C.; Loftsson, T. Cyclodextrin–poloxamer aggregates as nanocarriers in eye drop formulations: Dexamethasone and amphotericin B. Drug Dev. Ind. Pharm. 2016, 42, 1446–1454. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Yu, Y.; Chaurasiya, B.; Li, X.; Xu, Y.; Webster, T.; Tu, J.; Sun, R. Stability, safety, and transcorneal mechanistic studies of ophthalmic lyophilized cyclosporine-loaded polymeric micelles. Int. J. Nanomed. 2018, 13, 8281–8296. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Chen, D.; Li, Y.; Yang, W.; Tu, J.; Shen, Y. Improving the topical ocular pharmacokinetics of lyophilized cyclosporine A-loaded micelles: Formulation, in vitro and in vivo studies. Drug Deliv. 2018, 25, 888–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Pizarro, R.; Silva-Abreu, M.; Calpena, A.C.; Egea, M.A.; Espina, M.; García, M.L. Development of fluorometholone-loaded PLGA nanoparticles for treatment of inflammatory disorders of anterior and posterior segments of the eye. Int. J. Pharm. 2018, 547, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Baba, K.; Tanaka, Y.; Kubota, A.; Kasai, H.; Yokokura, S.; Nakanishi, H.; Nishida, K. A method for enhancing the ocular penetration of eye drops using nanoparticles of hydrolyzable dye. J. Control Release 2011, 153, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Y.; Yang, J.; Zhang, H.; Gan, L. Cationized hyaluronic acid coated spanlastics for cyclosporine A ocular delivery: Prolonged ocular retention, enhanced corneal permeation and improved tear production. Int. J. Pharm. 2019, 565, 133–142. [Google Scholar] [CrossRef]
- Gupta, A.K.; Madan, S.; Majumdar, D.K.; Maitra, A. Ketorolac entrapped in polymeric micelles: Preparation, characterisation and ocular anti-inflammatory studies. Int. J. Pharm. 2000, 209, 1–14. [Google Scholar] [CrossRef]
- Asasutjarit, R.; Theerachayanan, T.; Kewsuwan, P.; Veeranodha, S.; Fuongfuchat, A.; Ritthidej, G.C. Development and Evaluation of Diclofenac Sodium Loaded-N-Trimethyl Chitosan Nanoparticles for Ophthalmic Use. AAPS Pharmscitech. 2015, 16, 1013–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Fuente, M.; Raviña, M.; Paolicelli, P.; Sanchez, A.; Seijo, B.; Alonso, M.J. Chitosan-based nanostructures: A delivery platform for ocular therapeutics. Adv. Drug Deliv. Rev. 2010, 62, 100–117. [Google Scholar] [CrossRef] [PubMed]
- Badawi, A.A.; El-Laithy, H.M.; El Qidra, R.K.; El Mofty, H.; El dally, M. Chitosan based nanocarriers for indomethacin ocular delivery. Arch. Pharm. Res. 2008, 31, 1040–1049. [Google Scholar] [CrossRef]
- Akhter, S.; Anwar, M.; Siddiqui, M.A.; Ahmad, I.; Ahmad, J.; Ahmad, M.Z.; Bhatnagar, A.; Ahmad, F.J. Improving the topical ocular pharmacokinetics of an immunosuppressant agent with mucoadhesive nanoemulsions: Formulation development, in-vitro and in-vivo studies. Colloids Surf. B Biointerfaces 2016, 148, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Price, F.W. Efficacy of topical cyclosporine 0.05% for prevention of cornea transplant rejection episodes. Ophthalmology 2006, 113, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Katara, R.; Sachdeva, S.; Majumdar, D.K. Design, characterization, and evaluation of aceclofenac-loaded Eudragit RS 100 nanoparticulate system for ocular delivery. Pharm. Dev. Technol. 2019, 24, 368–379. [Google Scholar] [CrossRef]
- Katara, R.; Majumdar, D.K. Eudragit RL 100-based nanoparticulate system of aceclofenac for ocular delivery. Colloids Surf. B Biointerfaces 2013, 103, 455–462. [Google Scholar] [CrossRef]
- Li, Y.-J.; Luo, L.-J.; Harroun, S.G.; Wei, S.-C.; Unnikrishnan, B.; Chang, H.-T.; Huang, Y.-F.; Lai, J.-Y.; Huang, C.-C. Synergistically dual-functional nano eye-drops for simultaneous anti-inflammatory and anti-oxidative treatment of dry eye disease. Nanoscale 2019, 11, 5580–5594. [Google Scholar] [CrossRef]
- Tsukamoto, T.; Hironaka, K.; Fujisawa, T.; Yamaguchi, D.; Tahara, K.; Tozuka, Y.; Takeuchi, H. Preparation of bromfenac-loaded liposomes modified with chitosan for ophthalmic drug delivery and evaluation of physicochemical properties and drug release profile. Asian J. Pharm. Sci. 2013, 8, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.K.; Sahoo, P.K.; Majumdar, D.K.; Panda, A.K. Topical ocular delivery of a COX-II inhibitor via biodegradable nanoparticles. Nanotechnol. Rev. 2016, 5. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Egea, M.A.; Cano, A.; Espina, M.; Calpena, A.C.; Ettcheto, M.; Camins, A.; Souto, E.B.; Silva, A.M.; García, M.L. PEGylated PLGA nanospheres optimized by design of experiments for ocular administration of dexibuprofen-in vitro, ex vivo and in vivo characterization. Colloids Surf. B Biointerfaces 2016, 145, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Shi, S.; Zhang, Z.; Luo, Z.; Yu, J.; Liang, R.; Li, X.; Chen, H. Chitosan grafted methoxy poly(ethylene glycol)-poly(ε-caprolactone) nanosuspension for ocular delivery of hydrophobic diclofenac. Sci. Rep. 2015, 5, 11337. [Google Scholar] [CrossRef] [Green Version]
- Cao, F.; Wang, Y.; Ping, Q.; Liao, Z. Zn-Al-NO(3)-layered double hydroxides with intercalated diclofenac for ocular delivery. Int. J. Pharm. 2011, 404, 250–256. [Google Scholar] [CrossRef]
- Li, N.; Zhuang, C.; Wang, M.; Sun, X.; Nie, S.; Pan, W. Liposome coated with low molecular weight chitosan and its potential use in ocular drug delivery. Int. J. Pharm. 2009, 379, 131–138. [Google Scholar] [CrossRef]
- Li, X.; Zhang, Z.; Li, J.; Sun, S.; Weng, Y.; Chen, H. Diclofenac/biodegradable polymer micelles for ocular applications. Nanoscale 2012, 4, 4667–4673. [Google Scholar] [CrossRef]
- Agnihotri, S.M.; Vavia, P.R. Diclofenac-loaded biopolymeric nanosuspensions for ophthalmic application. Nanomedicine 2009, 5, 90–95. [Google Scholar] [CrossRef]
- Attama, A.A.; Reichl, S.; Müller-Goymann, C.C. Diclofenac sodium delivery to the eye: In Vitro evaluation of novel solid lipid nanoparticle formulation using human cornea construct. Int. J. Pharm. 2008, 355, 307–313. [Google Scholar] [CrossRef]
- Han, S.; Shen, J.; Gan, Y.; Geng, H.; Zhang, X.; Zhu, C.; Gan, L. Novel vehicle based on cubosomes for ophthalmic delivery of flurbiprofen with low irritancy and high bioavailability. Acta Pharm. Sin. 2010, 31, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Pan, H.; Li, P.; Wang, H.; Wang, X.; Pan, W.; Yuan, Y. The potential use of novel chitosan-coated deformable liposomes in an ocular drug delivery system. Colloids Surf. B Biointerfaces 2016, 143, 455–462. [Google Scholar] [CrossRef]
- Vega, E.; Gamisans, F.; García, M.L.; Chauvet, A.; Lacoulonche, F.; Egea, M.A. PLGA nanospheres for the ocular delivery of flurbiprofen: Drug release and interactions. J. Pharm. Sci. 2008, 97, 5306–5317. [Google Scholar] [CrossRef]
- Pignatello, R.; Bucolo, C.; Spedalieri, G.; Maltese, A.; Puglisi, G. Flurbiprofen-loaded acrylate polymer nanosuspensions for ophthalmic application. Biomaterials 2002, 23, 3247–3255. [Google Scholar] [CrossRef]
- Vega, E.; Egea, M.A.; Valls, O.; Espina, M.; García, M.L. Flurbiprofen loaded biodegradable nanoparticles for ophtalmic administration. J. Pharm. Sci. 2006, 95, 2393–2405. [Google Scholar] [CrossRef] [PubMed]
- Gamisans, F.; Lacoulonche, F.; Chauvet, A.; Espina, M.; García, M.L.; Egea, M.A. Flurbiprofen-loaded nanospheres: Analysis of the matrix structure by thermal methods. Int. J. Pharm. 1999, 179, 37–48. [Google Scholar] [CrossRef]
- Lacoulonche, F.; Gamisans, F.; Chauvet, A.; García, M.L.; Espina, M.; Egea, M.A. Stability and in vitro drug release of flurbiprofen-loaded poly-epsilon-caprolactone nanospheres. Drug Dev. Ind. Pharm. 1999, 25, 983–993. [Google Scholar] [CrossRef]
- Valls, R.; Vega, E.; Garcia, M.L.; Egea, M.A.; Valls, J.O. Transcorneal permeation in a corneal device of non-steroidal anti-inflammatory drugs in drug delivery systems. Open Med. Chem. J. 2008, 2, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Araújo, J.; Vega, E.; Lopes, C.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Effect of polymer viscosity on physicochemical properties and ocular tolerance of FB-loaded PLGA nanospheres. Colloids Surf. B Biointerfaces 2009, 72, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ramos Yacasi, G.R.; García López, M.L.; Espina García, M.; Parra Coca, A.; Calpena Campmany, A.C. Influence of freeze-drying and γ-irradiation in preclinical studies of flurbiprofen polymeric nanoparticles for ocular delivery using d-(+)-trehalose and polyethylene glycol. Int. J. Nanomed. 2016, 11, 4093–4106. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Mira, E.; Egea, M.A.; Souto, E.B.; Calpena, A.C.; García, M.L. Optimizing flurbiprofen-loaded NLC by central composite factorial design for ocular delivery. Nanotechnology 2011, 22, 045101. [Google Scholar] [CrossRef]
- Shen, J.; Gan, L.; Zhu, C.; Zhang, X.; Dong, Y.; Jiang, M.; Zhu, J.; Gan, Y. Novel NSAIDs ophthalmic formulation: Flurbiprofen axetil emulsion with low irritancy and improved anti-inflammation effect. Int. J. Pharm. 2011, 412, 115–122. [Google Scholar] [CrossRef]
- Gai, X.; Cheng, L.; Li, T.; Liu, D.; Wang, Y.; Wang, T.; Pan, W.; Yang, X. In vitro and In vivo Studies on a Novel Bioadhesive Colloidal System: Cationic Liposomes of Ibuprofen. AAPS Pharmscitech 2018, 19, 700–709. [Google Scholar] [CrossRef]
- Dong, Y.; Dong, P.; Huang, D.; Mei, L.; Xia, Y.; Wang, Z.; Pan, X.; Li, G.; Wu, C. Fabrication and characterization of silk fibroin-coated liposomes for ocular drug delivery. Eur. J. Pharm. Biopharm. 2015, 91, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Nie, S.; Kong, J.; Li, N.; Ju, C.; Pan, W. A controlled-release ocular delivery system for ibuprofen based on nanostructured lipid carriers. Int. J. Pharm. 2008, 363, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Bucolo, C.; Maltese, A.; Puglisi, G.; Pignatello, R. Enhanced ocular anti-inflammatory activity of ibuprofen carried by an Eudragit RS100 nanoparticle suspension. Ophthalmic. Res. 2002, 34, 319–323. [Google Scholar] [CrossRef]
- Pignatello, R.; Bucolo, C.; Ferrara, P.; Maltese, A.; Puleo, A.; Puglisi, G. Eudragit RS100 nanosuspensions for the ophthalmic controlled delivery of ibuprofen. Eur. J. Pharm. Sci. 2002, 16, 53–61. [Google Scholar] [CrossRef]
- Nagai, N.; Ito, Y.; Okamoto, N.; Shimomura, Y. A nanoparticle formulation reduces the corneal toxicity of indomethacin eye drops and enhances its corneal permeability. Toxicology 2014, 319, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Calvo, P.; Alonso, M.J.; Vila-Jato, J.L.; Robinson, J.R. Improved ocular bioavailability of indomethacin by novel ocular drug carriers. J. Pharm. Pharm. 1996, 48, 1147–1152. [Google Scholar] [CrossRef]
- Calvo, P.; Vila-Jato, J.L.; Alonso, M.J. Evaluation of cationic polymer-coated nanocapsules as ocular drug carriers. Int. J. Pharm. 1997, 153, 41–50. [Google Scholar] [CrossRef]
- Hippalgaonkar, K.; Adelli, G.R.; Hippalgaonkar, K.; Repka, M.A.; Majumdar, S. Indomethacin-loaded solid lipid nanoparticles for ocular delivery: Development, characterization, and in vitro evaluation. J. Ocul. Pharm. 2013, 29, 216–228. [Google Scholar] [CrossRef] [Green Version]
- Aşık, M.D.; Uğurlu, N.; Yülek, F.; Tuncer, S.; Türk, M.; Denkbaş, E.B. Ketorolac Tromethamine Loaded Chitosan Nanoparticles as a Nanotherapeutic System for Ocular Diseases. Hacet. J. Biol. Chem. 2013, 41, 81–86. [Google Scholar]
- Fathalla, Z.M.A.; Khaled, K.A.; Hussein, A.K.; Alany, R.G.; Vangala, A. Formulation and corneal permeation of ketorolac tromethamine-loaded chitosan nanoparticles. Drug Dev. Ind. Pharm. 2016, 42, 514–524. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Reddy, J.; Sekhar, C. Formulation development and characterization of naproxen sodium-loaded mucoadhesive microspheres. J. Pharm. Sci. Res. 2012, 4, 1709–1715. [Google Scholar]
- Javadzadeh, Y.; Ahadi, F.; Davaran, S.; Mohammadi, G.; Sabzevari, A.; Adibkia, K. Preparation and physicochemical characterization of naproxen-PLGA nanoparticles. Colloids Surf. B Biointerfaces 2010, 81, 498–502. [Google Scholar] [CrossRef]
- Lorenzo-Veiga, B.; Sigurdsson, H.H.; Loftsson, T. Nepafenac-Loaded Cyclodextrin/Polymer Nanoaggregates: A New Approach to Eye Drop Formulation. Materals 2019, 12, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, Z.; Muratomi, N.; Huang, W.; Huang, L.; Ren, J.; Yang, J.; Persaud, Y.; Loloi, J.; Mallangada, N.; Kung, P.; et al. The ocular pharmacokinetics and biodistribution of phospho-sulindac (OXT-328) formulated in nanoparticles: Enhanced and targeted tissue drug delivery. Int. J. Pharm. 2019, 557, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Giunchedi, P.; Chetoni, P.; Conte, U.; Saettone, M.F. Albumin Microspheres for Ocular Delivery of Piroxicam. Pharm. Pharmacol. Commun. 2000, 6, 149–153. [Google Scholar] [CrossRef]
- Adibkia, K.; Siahi Shadbad, M.R.; Nokhodchi, A.; Javadzedeh, A.; Barzegar-Jalali, M.; Barar, J.; Mohammadi, G.; Omidi, Y. Piroxicam nanoparticles for ocular delivery: Physicochemical characterization and implementation in endotoxin-induced uveitis. J. Drug Target. 2007, 15, 407–416. [Google Scholar] [CrossRef]
- Gan, L.; Han, S.; Shen, J.; Zhu, J.; Zhu, C.; Zhang, X.; Gan, Y. Self-assembled liquid crystalline nanoparticles as a novel ophthalmic delivery system for dexamethasone: Improving preocular retention and ocular bioavailability. Int. J. Pharm. 2010, 396, 179–187. [Google Scholar] [CrossRef]
- Kesavan, K.; Kant, S.; Singh, P.N.; Pandit, J.K. Mucoadhesive chitosan-coated cationic microemulsion of dexamethasone for ocular delivery: In Vitro and In Vivo evaluation. Curr. Eye Res. 2013, 38, 342–352. [Google Scholar] [CrossRef]
- Nagai, N.; Nakazawa, Y.; Ito, Y.; Kanai, K.; Okamoto, N.; Shimomura, Y. A Nanoparticle-Based Ophthalmic Formulation of Dexamethasone Enhances Corneal Permeability of the Drug and Prolongs Its Corneal Residence Time. Biol. Pharm. Bull. 2017, 40, 1055–1062. [Google Scholar] [CrossRef] [Green Version]
- Moya-Ortega, M.D.; Alves, T.F.G.; Alvarez-Lorenzo, C.; Concheiro, A.; Stefánsson, E.; Thorsteinsdóttir, M.; Loftsson, T. Dexamethasone eye drops containing γ-cyclodextrin-based nanogels. Int. J. Pharm. 2013, 441, 507–515. [Google Scholar] [CrossRef]
- Jamard, M.; Hoare, T.; Sheardown, H. Nanogels of methylcellulose hydrophobized with N-tert-butylacrylamide for ocular drug delivery. Drug Deliv. Transl. Res. 2016, 6, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Garapati, C.; Chowdhury, P.; Gupta, H.; Nesamony, J.; Nauli, S.; Boddu, S.H.S. Development and evaluation of dexamethasone nanomicelles with potential for treating posterior uveitis after topical application. J. Ocul. Pharm. 2015, 31, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Balzus, B.; Sahle, F.F.; Hönzke, S.; Gerecke, C.; Schumacher, F.; Hedtrich, S.; Kleuser, B.; Bodmeier, R. Formulation and ex vivo evaluation of polymeric nanoparticles for controlled delivery of corticosteroids to the skin and the corneal epithelium. Eur. J. Pharm. Biopharm. 2017, 115, 122–130. [Google Scholar] [CrossRef]
- Kassem, M.A.; Abdel Rahman, A.A.; Ghorab, M.M.; Ahmed, M.B.; Khalil, R.M. Nanosuspension as an ophthalmic delivery system for certain glucocorticoid drugs. Int. J. Pharm. 2007, 340, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, S.; Vavia, P.R.; Trotta, F.; Cavalli, R. Nanosponges encapsulating dexamethasone for ocular delivery: Formulation design, physicochemical characterization, safety and corneal permeability assessment. J. Biomed. Nanotechnol. 2013, 9, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Ban, J.; Zhang, Y.; Huang, X.; Deng, G.; Hou, D.; Chen, Y.; Lu, Z. Corneal permeation properties of a charged lipid nanoparticle carrier containing dexamethasone. Int. J. Nanomed. 2017, 12, 1329–1339. [Google Scholar] [CrossRef] [Green Version]
- Loftsson, T.; Hreinsdóttir, D.; Stefánsson, E. Cyclodextrin microparticles for drug delivery to the posterior segment of the eye: Aqueous dexamethasone eye drops. J. Pharm. Pharm. 2007, 59, 629–635. [Google Scholar] [CrossRef]
- Kalam, M.A. The potential application of hyaluronic acid coated chitosan nanoparticles in ocular delivery of dexamethasone. Int. J. Biol. Macromol. 2016, 89, 559–568. [Google Scholar] [CrossRef]
- Kalam, M.A. Development of chitosan nanoparticles coated with hyaluronic acid for topical ocular delivery of dexamethasone. Int. J. Biol. Macromol. 2016, 89, 127–136. [Google Scholar] [CrossRef]
- Fabiano, A.; Chetoni, P.; Zambito, Y. Mucoadhesive nano-sized supramolecular assemblies for improved pre-corneal drug residence time. Drug Dev. Ind. Pharm. 2015, 41, 2069–2076. [Google Scholar] [CrossRef]
- Vafaei, S.Y.; Dinarvand, R.; Esmaeili, M.; Mahjub, R.; Toliyat, T. Controlled-release drug delivery system based on fluocinolone acetonide-cyclodextrin inclusion complex incorporated in multivesicular liposomes. Pharm. Dev. Technol. 2015, 20, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.H.; Mahmoud, A.A.; Kamel, R. A Novel Method for Preparing Surface-Modified Fluocinolone Acetonide Loaded PLGA Nanoparticles for Ocular Use: In Vitro and In Vivo Evaluations. AAPS Pharmscitech 2016, 17, 1159–1172. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, A.K.; Maincent, P.; Thouvenot, P.; Kreuter, J. Hydrocortisone delivery to healthy and inflamed eyes using a micellar polysorbate 80 solution or albumin nanoparticles. Int. J. Pharm. 1994, 110, 211–222. [Google Scholar] [CrossRef]
- Vandervoort, J.; Ludwig, A. Preparation and evaluation of drug-loaded gelatin nanoparticles for topical ophthalmic use. Eur J. Pharm. Biopharm. 2004, 57, 251–261. [Google Scholar] [CrossRef]
- Nasr, F.H.; Khoee, S. Design, characterization and in vitro evaluation of novel shell crosslinked poly(butylene adipate)-co-N-succinyl chitosan nanogels containing loteprednol etabonate: A new system for therapeutic effect enhancement via controlled drug delivery. Eur. J. Med. Chem. 2015, 102, 132–142. [Google Scholar] [CrossRef]
- Sah, A.K.; Suresh, P.K.; Verma, V.K. PLGA nanoparticles for ocular delivery of loteprednol etabonate: A corneal penetration study. Artif. Cells Nanomed. Biotechnol. 2017, 45, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adibkia, K.; Omidi, Y.; Siahi, M.R.; Javadzadeh, A.R.; Barzegar-Jalali, M.; Barar, J.; Maleki, N.; Mohammadi, G.; Nokhodchi, A. Inhibition of endotoxin-induced uveitis by methylprednisolone acetate nanosuspension in rabbits. J. Ocul. Pharm. 2007, 23, 421–432. [Google Scholar] [CrossRef]
- Silva, R.O.; da Costa, B.L.; da Silva, F.R.; da Silva, C.N.; de Paiva, M.B.; Dourado, L.F.N.; Malachias, Â.; de Souza Araújo, A.A.; Nunes, P.S.; Silva-Cunha, A. Treatment for chemical burning using liquid crystalline nanoparticles as an ophthalmic delivery system for pirfenidone. Int. J. Pharm. 2019, 568, 118466. [Google Scholar] [CrossRef]
- Qu, X.; Khutoryanskiy, V.V.; Stewart, A.; Rahman, S.; Papahadjopoulos-Sternberg, B.; Dufes, C.; McCarthy, D.; Wilson, C.G.; Lyons, R.; Carter, K.C.; et al. Carbohydrate-based micelle clusters which enhance hydrophobic drug bioavailability by up to 1 order of magnitude. Biomacromolecules 2006, 7, 3452–3459. [Google Scholar] [CrossRef]
- Katzer, T.; Chaves, P.; Bernardi, A.; Pohlmann, A.; Guterres, S.S.; Ruver Beck, R.C. Prednisolone-loaded nanocapsules as ocular drug delivery system: Development, in vitro drug release and eye toxicity. J. Microencapsul. 2014, 31, 519–528. [Google Scholar] [CrossRef]
- Elbialy, N.S.; Abdol-Azim, B.M.; Shafaa, M.W.; El Shazly, L.H.; El Shazly, A.H.; Khalil, W.A. Enhancement of the ocular therapeutic effect of prednisolone acetate by liposomal entrapment. J. Biomed. Nanotechnol. 2013, 9, 2105–2116. [Google Scholar] [CrossRef] [PubMed]
- Gaafar, P.M.E.; Abdallah, O.Y.; Farid, R.M.; Abdelkader, H. Preparation, characterization and evaluation of novel elastic nano-sized niosomes (ethoniosomes) for ocular delivery of prednisolone. J. Liposome Res. 2014, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.K.; El-Leithy, I.S.; Makky, A.A. Mucoadhesive nanoparticles as carrier systems for prolonged ocular delivery of gatifloxacin/prednisolone bitherapy. Mol. Pharm. 2010, 7, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.; Li, Q.; Sun, Y.; Guo, J.; Zhao, Q.; Yin, X.; Wei, H.; Wu, S.; Bi, H. Evaluation of controlled-release triamcinolone acetonide-loaded mPEG-PLGA nanoparticles in treating experimental autoimmune uveitis. Nanotechnology 2019, 30, 165702. [Google Scholar] [CrossRef]
- Mahaling, B.; Srinivasarao, D.A.; Raghu, G.; Kasam, R.K.; Bhanuprakash Reddy, G.; Katti, D.S. A non-invasive nanoparticle mediated delivery of triamcinolone acetonide ameliorates diabetic retinopathy in rats. Nanoscale 2018, 10, 16485–16498. [Google Scholar] [CrossRef]
- Sabzevari, A.; Adibkia, K.; Hashemi, H.; Hedayatfar, A.; Mohsenzadeh, N.; Atyabi, F.; Ghahremani, M.H.; Dinarvand, R. Polymeric triamcinolone acetonide nanoparticles as a new alternative in the treatment of uveitis: In Vitro and In Vivo studies. Eur. J. Pharm. Biopharm. 2013, 84, 63–71. [Google Scholar] [CrossRef]
- Guengerich, F.P. Intersection of the Roles of Cytochrome P450 Enzymes with Xenobiotic and Endogenous Substrates: Relevance to Toxicity and Drug Interactions. Chem. Res. Toxicol. 2017, 30, 2–12. [Google Scholar] [CrossRef]
- Gupta, H.; Jain, S.; Mathur, R.; Mishra, P.; Mishra, A.K.; Velpandian, T. Sustained ocular drug delivery from a temperature and pH triggered novel in situ gel system. Drug Deliv. 2007, 14, 507–515. [Google Scholar] [CrossRef]
- Patravale, V.B.; Date, A.A.; Kulkarni, R.M. Nanosuspensions: A promising drug delivery strategy. J. Pharm. Pharm. 2004, 56, 827–840. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.M.; Abd-Elgawad, A.-E.H.; Soliman, O.A.-E.; Jablonski, M.M. Stability and Ocular Pharmacokinetics of Celecoxib-Loaded Nanoparticles Topical Ophthalmic Formulations. J. Pharm. Sci. 2016, 105, 3691–3701. [Google Scholar] [CrossRef]
- Gupta, H.; Aqil, M.; Khar, R.K.; Ali, A.; Bhatnagar, A.; Mittal, G. Nanoparticles laden in situ gel for sustained ocular drug delivery. J. Pharm. Bioallied. Sci. 2013, 5, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Abd-Elgawad, A.-E.H.; Soliman, O.A.-E.; Jablonski, M.M. Nanoparticle-based topical ophthalmic formulations for sustained celecoxib release. J. Pharm. Sci. 2013, 102, 1036–1053. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Abd-Elgawad, A.-E.H.; Soliman, O.A.-E.; Jablonski, M.M. Natural bioadhesive biodegradable nanoparticles-based topical ophthalmic formulations for sustained celecoxib release: In Vitro study. J. Pharm. Technol. Drug Res. 2013, 2, 7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; He, Z.; Liang, R.; Ma, Y.; Huang, W.; Jiang, R.; Shi, S.; Chen, H.; Li, X. Fabrication of a Micellar Supramolecular Hydrogel for Ocular Drug Delivery. Biomacromolecules 2016, 17, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Mira, E.; Nikolić, S.; Calpena, A.C.; Egea, M.A.; Souto, E.B.; García, M.L. Improved and safe transcorneal delivery of flurbiprofen by NLC and NLC-based hydrogels. J. Pharm. Sci. 2012, 101, 707–725. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.; Lobão, P.; Frigerio, C.; Fonseca, J.; Silva, R.; Sousa Lobo, J.M.; Amaral, M.H. Preparation, characterization and biocompatibility studies of thermoresponsive eyedrops based on the combination of nanostructured lipid carriers (NLC) and the polymer Pluronic F-127 for controlled delivery of ibuprofen. Pharm. Dev. Technol. 2017, 22, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Morsi, N.; Ghorab, D.; Refai, H.; Teba, H. Ketoroloac tromethamine loaded nanodispersion incorporated into thermosensitive in situ gel for prolonged ocular delivery. Int. J. Pharm. 2016, 506, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zu, D.; Chen, J.; Peng, J.; Liu, Y.; Zhang, H.; Li, S.; Pan, W. Bovine serum albumin–meloxicam nanoaggregates laden contact lenses for ophthalmic drug delivery in treatment of postcataract endophthalmitis. Int. J. Pharm. 2014, 475, 25–34. [Google Scholar] [CrossRef]
- Paulsamy, M.; Ponnusamy, C.; Palanisami, M.; Nackeeran, G.; Paramasivam, S.; Sugumaran, A.; Kandasamy, R.; Natesan, S.; Palanichamy, R. Nepafenac loaded silica nanoparticles dispersed in-situ gel systems: Development and characterization. Int. J. Biol. Macromol. 2018, 110, 336–345. [Google Scholar] [CrossRef]
- Giunchedi, P.; Conte, U.; Chetoni, P.; Saettone, M.F. Pectin microspheres as ophthalmic carriers for piroxicam: Evaluation in vitro and in vivo in albino rabbits. Eur. J. Pharm. Sci. 1999, 9, 1–7. [Google Scholar] [CrossRef]
- Abrego, G.; Alvarado, H.; Souto, E.B.; Guevara, B.; Bellowa, L.H.; Parra, A.; Calpena, A.; Garcia, M.L. Biopharmaceutical profile of pranoprofen-loaded PLGA nanoparticles containing hydrogels for ocular administration. Eur. J. Pharm. Biopharm. 2015, 95, 261–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, Y.; Ban, J.; Mo, Z.; Zhang, Y.; An, P.; Liu, L.; Xie, Q.; Du, Y.; Xie, B.; Zhan, X.; et al. A potential nanoparticle-loaded in situ gel for enhanced and sustained ophthalmic delivery of dexamethasone. Nanotechnology 2018, 29, 425101. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.; Ban, J.; Zhang, Y.; Du, Y.; Wen, Y.; Huang, X.; Xie, Q.; Shen, L.; Zhang, S.; Deng, H.; et al. Nanostructured lipid carriers-based thermosensitive eye drops for enhanced, sustained delivery of dexamethasone. Nanomedicine 2018, 13, 1239–1253. [Google Scholar] [CrossRef] [PubMed]
- Pramanik, A.; Sahoo, R.N.; Nanda, A.; Mohapatra, R.; Singh, R.; Mallick, S. Ocular Permeation and Sustained Anti-inflammatory Activity of Dexamethasone from Kaolin Nanodispersion Hydrogel System. Curr. Eye Res. 2018, 43, 828–838. [Google Scholar] [CrossRef]
- Gonzalez-Pizarro, R.; Carvajal-Vidal, P.; Halbault Bellowa, L.; Calpena, A.C.; Espina, M.; García, M.L. In-situ forming gels containing fluorometholone-loaded polymeric nanoparticles for ocular inflammatory conditions. Colloids Surf. B Biointerfaces 2019, 175, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Nakrani, H.; Raval, M.; Sheth, N. Development of loteprednol etabonate-loaded cationic nanoemulsified in-situ ophthalmic gel for sustained delivery and enhanced ocular bioavailability. Drug Deliv. 2016, 23, 3712–3723. [Google Scholar] [CrossRef] [Green Version]
- Hanafy, A.F.; Abdalla, A.M.; Guda, T.K.; Gabr, K.E.; Royall, P.G.; Alqurshi, A. Ocular anti-inflammatory activity of prednisolone acetate loaded chitosan-deoxycholate self-assembled nanoparticles. Int J. Nanomed. 2019, 14, 3679–3689. [Google Scholar] [CrossRef] [Green Version]
- Baranowski, P.; Karolewicz, B.; Gajda, M.; Pluta, J. Ophthalmic Drug Dosage Forms: Characterisation and Research Methods. Sci. World J. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Chédru-Legros, V.; Fines-Guyon, M.; Chérel, A.; Perdriel, A.; Albessard, F.; Debruyne, D.; Mouriaux, F. [Fortified antibiotic (vancomycin, amikacin and ceftazidime) eye drop stability assessment at -20 degrees C]. J. Fr. Ophtalmol. 2007, 30, 807–813. [Google Scholar] [CrossRef]
- Zhu, H.; Chauhan, A. Effect of viscosity on tear drainage and ocular residence time. Optom. Vis. Sci. 2008, 85, 715–725. [Google Scholar] [CrossRef]
- Graça, A.; Gonçalves, L.M.; Raposo, S.; Ribeiro, H.M.; Marto, J. Useful In Vitro Techniques to Evaluate the Mucoadhesive Properties of Hyaluronic Acid-Based Ocular Delivery Systems. Pharmaceutics 2018, 10, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaiyasan, W.; Praputbut, S.; Kompella, U.B.; Srinivas, S.P.; Tiyaboonchai, W. Penetration of mucoadhesive chitosan-dextran sulfate nanoparticles into the porcine cornea. Colloids Surf. B Biointerfaces 2017, 149, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Gèze, A.; Choisnard, L.; Putaux, J.-L.; Wouessidjewe, D. Colloidal systems made of biotransesterified α, β and γ cyclodextrins grafted with C10 alkyl chains. Mater. Sci. Eng. C 2009, 29, 458–462. [Google Scholar] [CrossRef]
- Gèze, A.; Putaux, J.-L.; Choisnard, L.; Jéhan, P.; Wouessidjewe, D. Long-term shelf stability of amphiphilic β-cyclodextrin nanosphere suspensions monitored by dynamic light scattering and cryo-transmission electron microscopy. J. Microencapsul. 2004, 21, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Cho, D.; Lee, S.; Frey, M.W. Characterizing zeta potential of functional nanofibers in a microfluidic device. J. Colloid Interface Sci. 2012, 372, 252–260. [Google Scholar] [CrossRef]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. International Conference on Harmonisation—Validation of Analytical Procedures: Text and Methodology Q2(R1); ICH: Brussels, Belgium, 2005. [Google Scholar]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. International Conference on Harmonisation—Stability Testing of NEW Drug Substances and Products Q1A (R2); ICH: Brussels, Belgium, 2003. [Google Scholar]
- Duan, Y.; Cai, X.; Du, H.; Zhai, G. Novel in situ gel systems based on P123/TPGS mixed micelles and gellan gum for ophthalmic delivery of curcumin. Colloids Surf. B Biointerfaces 2015, 128, 322–330. [Google Scholar] [CrossRef]
- Huhtala, A.; Pohjonen, T.; Salminen, L.; Salminen, A.; Kaarniranta, K.; Uusitalo, H. In vitro biocompatibility of degradable biopolymers in cell line cultures from various ocular tissues: Extraction studies. J. Mater. Sci. Mater. Med. 2008, 19, 645–649. [Google Scholar] [CrossRef]
- OECD. Guideline for the Testing of Chemicals—Short Time Exposure In VITRO Test Method; Organisation for Economic Co-operation and Development: Paris, France, 2018; p. 19. [Google Scholar]
- Grimaudo, M.A.; Pescina, S.; Padula, C.; Santi, P.; Concheiro, A.; Alvarez-Lorenzo, C.; Nicoli, S. Topical application of polymeric nanomicelles in ophthalmology: A review on research efforts for the noninvasive delivery of ocular therapeutics. Expert Opin. Drug Deliv. 2019, 16, 397–413. [Google Scholar] [CrossRef]
- OECD. Guidance Documenton an Integrated Approach on Testing and Assessment (IATA) for Serious Eye Damage and Eye Irritation; Organisation for Economic Co-operation and Development: Paris, France, 2017; p. 90. [Google Scholar]
- Agarwal, P.; Rupenthal, I.D. In vitro and ex vivo corneal penetration and absorption models. Drug Deliv. Transl. Res. 2016, 6, 634–647. [Google Scholar] [CrossRef]
- Draize, J.; Woodard, G.; Calvery, H. Metods for the study of irritation and toxicity of substances applied topically to the skin and mucous membranes. J. Pharm. Exp. Ther. 1944, 82, 377–390. [Google Scholar]
- OECD. Guideline for the Testing of Chemicals—Acute Eye Irritation/Corrosion; Organisation for Economic Co-operation and Development: Paris, France, 2012; p. 19. [Google Scholar]
- Barile, F.A. Validating and troubleshooting ocular in vitro toxicology tests. J. Pharm. Toxicol. Methods 2010, 61, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.L.; Ahearne, M.; Hopkinson, A. An overview of current techniques for ocular toxicity testing. Toxicology 2015, 327, 32–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jester, J.V.; Li, L.; Molai, A.; Maurer, J.K. Extent of initial corneal injury as a basis for alternative eye irritation tests. Toxicol. Vitr. 2001, 15, 115–130. [Google Scholar] [CrossRef]
- NRC. Principles and Procedures for Evaluating the Toxicity of Household Substances; National Academy of Sciences Publication: Washington, DC, USA, 1977.
- Dave, V.; Paliwal, S.; Yadav, S.; Sharma, S. Effect of in vitro Transcorneal Approach of Aceclofenac Eye Drops through Excised Goat, Sheep, and Buffalo Corneas. Sci. World J. 2015, 2015, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luaces-Rodríguez, A.; Touriño-Peralba, R.; Alonso-Rodríguez, I.; García-Otero, X.; González-Barcia, M.; Rodríguez-Ares, M.T.; Martínez-Pérez, L.; Aguiar, P.; Gómez-Lado, N.; Silva-Rodríguez, J.; et al. Preclinical characterization and clinical evaluation of tacrolimus eye drops. Eur. J. Pharm. Sci. 2018, 120, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Méndez, R.; Yilmaz, T.; Cordero-Coma, M. Moving forward in uveitis therapy: Preclinical to phase II clinical trial drug development. Expert. Opin. Investig. Drugs 2016, 25, 195–214. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DCI | NSAID/ SAID | Chemical Classes | Routes of Administration |
|---|---|---|---|
| Aceclofenac | NSAID | Aryl-acetic acid derivatives | Per os |
| Alminoprofen | NSAID | Propionic acid derivatives | Per os |
| Betamethasone | SAID | Per os, inj and topical ophthalmic | |
| Bromfenac | NSAID | Aryl-acetic acid derivatives | Topical ophthalmic |
| Celecoxib | NSAID | Selective cylooxygenase -2 inhibitors | Per os |
| Deflazacort | SAID | Per os | |
| Dexamethasone (base and phosphate sodium) | SAID | Per os, inj and topical ophthalmic | |
| Dexketoprofen | NSAID | Propionic acid derivatives | Inj |
| Diclofenac | NSAID | Aryl-acetic acid derivatives | Per os and topical ophthalmic |
| Difluprednate | SAID | Topical ophthalmic | |
| Etodolac | NSAID | Indole and indene derivatives | Per os |
| Etoricoxib | NSAID | Selective cylooxygenase -2 inhibitors | Per os |
| Fluorometholone (base and acetate) | SAID | Topical ophthalmic | |
| Flurbiprofen | NSAID | Propionic acid derivatives | Topical ophthalmic |
| Hydrocortisone | SAID | Per os, inj and topical ophthalmic | |
| Ibuprofen | NSAID | Propionic acid derivatives | Per os and inj |
| Indomethacin | NSAID | Indole and indene derivatives | Per os, inj and topical ophthalmic |
| Ketoprofen | NSAID | Propionic acid derivatives | Per os and inj |
| Ketorolac tromethamine | NSAID | Aryl-acetic acid derivatives | Per os, inj and topical ophthalmic |
| Loteprednoletobonate | SAID | Topical ophthalmic | |
| Meclofenamate sodium | NSAID | Fenamic acid derivatives | Per os |
| Mefenamicacid | NSAID | Fenamic acid derivatives | Per os |
| Meloxicam | NSAID | Enolic acid derivatives | Per os and inj |
| Methylprednisolone | SAID | Per os and inj | |
| Nabumetone | NSAID | Non acidic derivatives | Per os |
| Naproxen | NSAID | Propionic acid derivatives | Per os |
| Nepafenac | NSAID | Aryl-acetic acid derivatives | Topical ophthalmic |
| Niflumic acid | NSAID | Fenamic acid derivatives | Per os |
| Oxaprozin | NSAID | Propionic acid derivatives | Per os |
| Parecoxib | NSAID | Selective cylooxygenase -2 inhibitors | Inj |
| Piroxicam | NSAID | Enolic acid derivatives | Per os and inj |
| Prednisolone (Acetate and Sodium Phosphate) | SAID | Per os, inj and topical ophthalmic | |
| Prednisone | SAID | Per os | |
| Salicylic Acid | NSAID | Salicylic acid derivatives | Per os and topical ophthalmic |
| Sulindac | NSAID | Indole and indene derivatives | Per os |
| Tenoxicam | NSAID | Enolic acid derivatives | Per os |
| Tiaprofen | NSAID | Propionic acid derivatives | Per os |
| Tolmetin | NSAID | Aryl-acetic acid derivatives | Per os |
| Triamcinolone | SAID | Inj and topical ophthalmic |
| DCI | NSAID/SAID | Product Names in USA, EU and France |
|---|---|---|
| Bromfenac | NSAID | BROMSITE EQ®, PROLENSA EQ®, YELLOX® |
| Ciclosporin A | CsA | CEQUA®, IKERVIS®, RESTASIS®, RESTASIS® MULTIDOSE, VERKAZIA® |
| Dexamethasone (Base or Sodium Phosphate) | SAID | CHIBRO CADRON®, DEXAFREE®, DEXASPORIN®, DEXTENZA®, FRAKIDEX®, MAXIDEX®, MAXIDROL®, MAXITROL®, STERDEX®, TOBRADEX® |
| Diclofenac | NSAID | VOLTAREN®, VOLTAREN®OPHTA, VOLTAREN®OPHTABAK |
| Difluprednate | SAID | DUREZOL® |
| Fluorometholone (Acetate or Base) | SAID | FLUCON®, FML®, FML FORTE® FLAREX® |
| Flurbiprofen | NSAID | OCUFEN® |
| Hydrocortisone | SOFTACORT® | |
| Indomethacin | NSAID | INDOCOLLYRE®, INDOBIOTIC® |
| Ketorolac tromethamine | NSAID | ACULAR®, ACULAR LS®, ACUVAIL®, |
| Loteprednol etabonate | SAID | ALREX®, INVELTYS®, LOTEMAX®, LOTEMAX SM®, ZYLET® |
| Nepafenac | NSAID | ILEVRO®, NEVANAC® |
| Prednisolone (Acetate or Sodium Phosphate) | SAID | BLEPHAMIDE®, BLEPHAMIDE S.O.P®,OMNIPRED®, PRED FORTE®, PRED MILD |
| Salicylicacid | NSAID | ANTALYRE®, CIELLA® |
| Triamcinolone | SAID | CIDERMEX® |
| Indications | Commonly Used Drugs | ||
|---|---|---|---|
| Management of post-operative inflammation | Diclofenac, ketorolac, SAIDs [1,53] | ||
| Prevention of intra-operative miosis | Flurbiprofen, ketorolac [54] | ||
| Anterior segment | Conjunctiva | Treatment of allergic conjunctivitis | Ketorolac, SAIDs [1,53] |
| Treatment of blepharoconjunctivitis | SAIDs [53] | ||
| Treatment of corneo-conjunctival burn | SAIDs [53] | ||
| Increase tear production in patients with keratoconjunctivitis sicca associated with dry eye syndrome | Ciclosporin [55] | ||
| Cornea | Prevention of corneal graft rejection | Dexamethasone [52,53] | |
| Control of pain after refractive surgery | Diclofenac, ketorolac [1] | ||
| Treatment of immune keratitis | SAIDs [53] | ||
| Treatment of bacterial keratitis | SAIDs [53] | ||
| Trade Name and Presentation | Active Substance | Excipients | Pharmaceutical Form | Marketed In | Year of Authorization |
|---|---|---|---|---|---|
| Alrex 0.2% | Loteprednol etabonate | Benzalkonium chloride, | suspension/drops | USA | 1998 |
| Multidose bottle 2.5, 5 and 10 mL | Edetate disodium, glycerin, povidone, purified water, tyloxapol, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Dexafree 0.1% | Dexamethasone phosphate | solution/drops | Fr | 2006 | |
| Single use vial 0.4 mL | Edetate disodium, sodium phosphate dibasic, sodium chloride, water for injection | ||||
| Dexamethasone Sodium Phosphate EQ 0.1% Phosphate | Dexamethasone phosphate | Sodium bisulfite, phenylethyl alcohol, benzalkonium chloride, | solution/drops | USA | 1996 |
| Multidose bottle 5 mL | Sodium citrate, sodium borate, creatinine, polysorbate 80, edetate disodium dihydrate, purified water, hydrochloric acid | ||||
| Dextenza 0.4MG | Dexamethasone | intracanalicular insert | USA | 2018 | |
| Single dose | 4-arm polyethylene glycol (PEG) N-hydroxysuccinimidyl glutarate (20 K), trilysine acetate, N-hydroxysuccinimide-fluorescein, sodium phosphate dibasic, sodium phosphate monobasic, water for injection | ||||
| DUREZOL 0.05% | Difluprednate | Sorbic acid, | emulsion | USA | 2008 |
| 2.5 mL in 5 mL multidose bottle 5 mL in 5 mL multidose bottle | Boric acid, castor oil, glycerin, polysorbate 80, purified water, sodium acetate, sodium EDTA, sodium hydroxide to adjust the pH | ||||
| FLAREX 0.1% | Fluorometholone acetate | Benzalkonium chloride, | suspension/drops | USA | 1986 |
| 5 mL in 8 mL multidose bottle 10 mL in 10 mL multidose bottle 15 mL in 15 mL multidose bottle | Sodium chloride, monobasic sodium phosphate, edetate disodium, hydroxyethyl cellulose, tyloxapol, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | ||||
| FLUCON 0.1% | Fluorometholone | Benzalkonium chloride, | suspension/drops | Fr | 1980 |
| Multidose bottle 3 mL | Monobasic sodium phosphate, dibasic sodium phosphate, polysorbate 80, sodium chloride, edetate disodium, polyvinyl alcohol, hydroxypropylmethylcellulose, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| FML 0.1% | Fluorometholone | Phenylmercuric acetate, | ointment | USA | 1985 |
| 3.5 g tube | Mineral oil, petrolatum alcohol, lanolin alcohol, white petrolatum | ||||
| FML 0.1% | Fluorometholone | Benzalkonium chloride, | suspension/drops | USA | 1972 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle 15 mL in 15 mL multidose bottle | Edetate disodium, polysorbate 80, polyvinyl alcohol, purified water, sodium chloride, sodium phosphate dibasic, sodium phosphate monobasic, sodium hydroxide | ||||
| FML FORTE 0.25% | Fluorometholone | Benzalkonium chloride, | suspension/drops | USA | 1986 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle 15 mL in 15 mL multidose bottle | Edetate disodium, polysorbate 80, polyvinyl alcohol, purified water, sodium chloride, sodium phosphate dibasic, sodium phosphate monobasic, sodium hydroxide | ||||
| Inveltys 1% | Loteprednol etabonate | suspension/drops | USA | 2018 | |
| 2.8 mL in 5 mL multidose bottle | Glycerin, sodium citrate dihydrate, poloxamer 407, sodium chloride, edetate disodium dihydrate, citric acid | ||||
| Lotemax 0.5% | Loteprednol etabonate | gel | USA | 2012 | |
| 5 g in 10 mL multidose bottle | Boric acid, edetate disodium, glycerin, polycarbophil, propylene glycol, sodium chloride, tyloxapol, water for injection, sodium hydroxide to adjust to the pH | ||||
| Lotemax 0.5% | Loteprednol etabonate | Benzalkonium chloride, | suspension/drops | USA | 1998 |
| Multidose bottle 2.5, 5, 10 and 15 mL | Edetate disodium, glycerin, povidone, purified water, tyloxapol, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Lotemax 0.5% | Loteprednol etabonate | ointment | USA | 2011 | |
| 3.5 g tube | Mineral oil, white petrolatum, | ||||
| Lotemax 0.5% | Loteprednol etabonate | gel | USA | 2012 | |
| 5 g in 10 mL multidose bottle | Boric acid, edetate disodium, glycerin, polycarbophil, propylene glycol, sodium chloride, tyloxapol, water for injection, sodium hydroxide to adjust to the pH | ||||
| Lotemax Sm 0.38% | Loteprednol etabonate | Benzalkonium chloride, | gel | USA | 2019 |
| 5 g in 10 mL multidose bottle | Boric acid, edetate disodium dihydrate, glycerin, hypromellose, poloxamer, polycarbophil, propylene glycol, sodium chloride, water for injection, | ||||
| Loteprednol Etabonate 0.5% | Loteprednol etabonate | Benzalkonium chloride, | suspension/drops | USA | 2019 |
| Multidose bottle 5, 10 and 15 mL | Edetate disodium, glycerin, povidone, purified water, hydrochloric acid and/or sodium hydroxide to adjust the pH, tyloxapol | ||||
| Maxidex 0.1% | Dexamethasone | Benzalkonium chloride, | suspension/drops | Fr | 1992 |
| Multidose bottle 3 mL | Sodium phosphate monobasic, polysorbate 80, edetate disodium, sodium chloride, methylhydroxypropylcellulose, citric acid, purified water | ||||
| Maxidex 0.1% | Dexamethasone | Benzalkonium chloride, | suspension/drops | USA | 1962 |
| Multidose bottle 5 mL | Hypromellose, sodium chloride, dibasic sodium phosphate, polysorbate 80, edetate disodium, citric acid and/or sodium hydroxide to adjust the pH, purified water | ||||
| Omnipred 1% | Prednisolone acetate | Benzalkonium chloride, | suspension/drops | USA | 1973 |
| Multidose bottle 5 and 10 mL | Hypromellose, dibasic sodium phosphate, polysorbate 80, edetate disodium, glycerin, citric acid and/or sodium hydroxide to adjust the pH, purified water | ||||
| Pred Forte 1% | Prednisolone acetate | Benzalkonium chloride, | suspension/drops | USA | 1973 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle 15 mL in 15 mL multidose bottle | Boric acid, edetate disodium, hypromellose, polysorbate 80, purified water, sodium bisulfite, sodium chloride, sodium citrate | ||||
| PRED MILD 0.12% | Prednisolone acetate | Benzalkonium chloride, | suspension/drops | USA | 1972 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle | Boric acid, edetate disodium, hypromellose, polysorbate 80, purified water, sodium bisulfite, sodium chloride, sodium citrate | ||||
| Prednisolone Sodium Phosphate EQ 0.9% | Prednisolone sodium phosphate | Benzalkonium chloride, | solution/drops | USA | 1994 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle 15 mL in 15 mL multidose bottle | Hypromellose, monobasic sodium phosphate, dibasic sodium phosphate, sodium chloride, edetate disodium dihydrate, purified water, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Softacort 0.335% | Hydrocortisone | solution/drops | Fr | 2017 | |
| Single use vial 0.4 mL | Sodium phosphate dibasic, monobasic sodium phosphate, edetate disodium, hydrochloric acid to adjust the pH, water for injection, |
| Trade Name and Presentation | Active Substance | Excipients | Pharmaceutical Form | Marketed In | Year of Authorization |
|---|---|---|---|---|---|
| Acular 0.5% | Ketorolac trometamol | Benzalkonium chloride, | solution/drops | Fr | 1991 |
| Multidose bottle 5 mL | Sodium chloride, edetate disodium, octoxynol 40, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | ||||
| Acular 0.5% | Ketorolac tromethamine | Benzalkonium chloride, | solution/drops | USA | 1992 |
| Multidose bottle 5 and 10 mL | Edetate disodium, octoxynol 40, purified water, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Acular LS 0.4% | Ketorolac tromethamine | Benzalkonium chloride, | solution/drops | USA | 2003 |
| Multidose bottle 5 and 10 mL | Edetate disodium, octoxynol 40, purified water, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Acuvail 0.45% | Ketorolac tromethamine | solution/drops | USA | 2009 | |
| Single use vial 0.4 mL | Carboxymethylcellulose, sodium chloride, sodium citrate, purified water, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Antalyre 0.1% | Salicylic acid | solution/drops | Fr | 2004 | |
| Single use vial 0.4 mL | Borax, boric acid, sodium chloride, purified water | ||||
| Bromfenac Sodium EQ 0.09% Acid | Bromfenac sodium | Benzalkonium chloride, | solution/drops | USA | 2014 |
| 1.7 mL in 6 mL multidose bottle | Boric acid, edetate disodium, polysorbate 80, povidone (K30), purified water, sodium borate, sodium sulfite anhydrous, sodium hydroxide to adjust the pH | ||||
| Bromsite EQ 0.075% Acid | Bromfenac sodium | Benzalkonium chloride, | solution/drops | USA | 2016 |
| 5 mL in 7.5 mL multidose bottle | Boric acid, sodium borate, citric acid anhydrous, sodium citrate dihydrate, poloxamer 407, polycarbophil, sodium chloride, edetate disodium, sodium hydroxide, water for injection | ||||
| Ciella 0.1% | Salicylic acid | solution | Fr | 2004 | |
| Multidose bottle 5 mL | Borax, sodium chloride, boric acid, rose-flavored water, purified water | ||||
| Diclofenac Sodium 0.1% | Diclofenac sodium | solution/drops | USA | 2008 | |
| Multidose bottle 2.5 and 5 mL | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | ||||
| Diclofenac Sodium 0.1% | Diclofenac sodium | solution/drops | USA | 2015 | |
| Multidose bottle 5 mL | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | ||||
| Diclofenac Sodium 0.1% | Diclofenac sodium | solution/drops | USA | 2007 | |
| Multidose bottle 5 mL | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | ||||
| Diclofenac Sodium 0.1% | Diclofenac sodium | solution/drops | USA | 2008 | |
| Multidose bottle 5 mL | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | ||||
| Diclofenac Sodium 0.1% | Diclofenac sodium | solution/drops | USA | 2008 | |
| Multidose bottle 5 mL | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | ||||
| Flurbiprofen Sodium 0.03% | Flurbiprofen sodium | Thimerosal, | solution/drops | USA | 1995 |
| Multidose bottle 2.5 mL | Citric acid, edetate disodium, polyvinyl alcohol, potassium chloride, purified water, sodium chloride, sodium citrate, hydrochloric acid and/or sodium hydroxide to adjust the pH | ||||
| Ilevro 0.3% | Nepafenac | Benzalkonium chloride, | suspension/drops | USA | 2012 |
| 1.7 mL in 4 mL multidose bottle | Boric acid, propylene glycol, carbomer 974P, sodium chloride, guar gum, carboxymethylcellulose sodium, edetate disodium, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | ||||
| Indocollyre 0.1% | Indomethacin | Thimerosal, | solution/drops | Fr | 1996 |
| Multidose bottle 5 mL | Arginine, hydroxypropylbetadex, hydrochloric acid, purified water | ||||
| Indocollyre 0.1% | Indomethacin | solution/drops | Fr | 1997 | |
| Single use vial 0.35 mL | Arginine, hydroxypropylbetadex, hydrochloric acid, purified water | ||||
| Ketorolac Tromethamine 0.4% | Ketorolac tromethamine | solution/drops | USA | 2009 | |
| NA | |||||
| Ketorolac Tromethamine 0.4% | Ketorolac tromethamine | solution/drops | USA | 2009 | |
| NA | |||||
| Ketorolac Tromethamine 0.4% | Ketorolac tromethamine | solution/drops | USA | 2009 | |
| NA | |||||
| Ketorolac Tromethamine 0.4% | Ketorolac tromethamine | solution/drops | USA | 2018 | |
| NA | |||||
| Ketorolac Tromethamine 0.5% | Benzalkonium chloride, | solution/drops | USA | 2009 | |
| 5 mL in 11 mL multidose bottle 10 mL in 11 mL multidose bottle | Nepafenac Ketorolac tromethamine | Edetate disodium, octoxynol 40, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH, water for injection | suspension/drops solution/drops | USA USA | 2012 2009 |
| KETOROLAC TROMETHAMINE 0.5% | Benzalkonium chloride, | ||||
| Multidose bottle 5 and 10 mL | Indomethacin Ketorolac tromethamine | Edetate disodium, octoxynol 40, purified water, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH | solution/drops solution/drops | Fr USA | 1996 2009 |
| Ketorolac Tromethamine 0.5% | Benzalkonium chloride, | ||||
| Multidose bottle 3, 5 and 10 mL | Indomethacin Ketorolac tromethamine | Edetate disodium, octoxynol 40, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | solution/drops solution/drops | Fr USA | 1997 2009 |
| Ketorolac Tromethamine 0.5% | Benzalkonium chloride, | ||||
| 3 mL in 5 mL multidose bottle 5 mL in 5 mL multidose bottle 10 mL in 10 mL multidose bottle | Ketorolac tromethamine Nepafenac | Edetate disodium, octoxynol 40, water for injection, sodium chloride, hydrochloric acid and/or sodium hydroxide to adjust the pH | solution/drops suspension/drops | USA EU | 2009 2007 |
| Nevanac 0.1% | Benzalkonium chloride, | ||||
| Multidose bottle 3 mL | Ketorolac tromethamine Nepafenac | Boric acid, propylene glycol, carbomer 974P, sodium chloride, guar gum, carboxymethylcellulose sodium, edetate disodium, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | solution/drops suspension/drops | USA USA | 2009 2005 |
| Nevanac 0.1% | Benzalkonium chloride, | ||||
| 3 mL in 4 mL multidose bottle | Ketorolac tromethamine Flurbiprofen sodium | Boric acid, propylene glycol, carbomer 974P, sodium chloride, tyloxapol, edetate disodium, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | solution/drops solution/drops | USA Fr | 2009 1991 |
| Ocufen 0.03% | |||||
| Single use vial 0.4 mL | Ketorolac tromethamine Flurbiprofen sodium | Polyvinyl alcohol, sodium chloride, sodium citrate, potassium chloride, citric acid, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | solution/drops solution/drops | USA USA | 2018 1986 |
| Ocufen 0.03% | Thimerosal, | ||||
| 2.5 mL in 5 mL multidose bottle | Ketorolac tromethamine Bromfenac sodium | Citric acid, edetate disodium, polyvinyl alcohol, potassium chloride, purified water, sodium chloride, sodium citrate, hydrochloric acid and/or sodium hydroxide to adjust the pH | solution/drops solution/drops | USA USA | 2009 2013 |
| Prolensa EQ 0.07% Acid | Benzalkonium chloride, | ||||
| 1.6 mL in 7.5 mL multidose bottle 13 mL in 7.5 mL multidose bottle | Ketorolac tromethamine Diclofenac sodium | Boric acid, edetate disodium, povidone, sodium borate, sodium sulfite, tyloxapol, sodium hydroxide, water for injection | solution/drops solution/drops | USA USA | 2009 1991 |
| Voltaren 0.1% | |||||
| Multidose bottle 5 mL | Ketorolac tromethamine Diclofenac sodium | Polyoxyl 35 castor oil, boric acid, tromethamine, sorbic acid, edetate disodium, purified water | solution/drops solution/drops | USA Fr | 2009 1995 |
| Voltarenophta 0.1% | |||||
| Single use vial 0.3 mL | Ketorolac tromethamine Diclofenac sodium | Cremophor EL, tromethamine, boric acid, water for injection | solution/drops solution/drops | USA Fr | 2009 2005 |
| Voltarenophtabak 0.1% | |||||
| Multidose bottle 10 mL | Nepafenac Bromfenac | Cremophor EL, tromethamine, boric acid, water for injection | suspension/drops solution/drops | EU EU | 2007 2011 |
| Yellox 0.09% | Benzalkonium chloride, | ||||
| Multidose bottle 5 mL | Nepafenac Bromfenac sodium | Boric acid, borax, sodium sulphite anhydrous (E221), tyloxapol, povidone, edetate disodium, water for injections, sodium hydroxide to adjust the pH | suspension/drops solution/drops | USA Fr | 2005 2011 |
| Yellox 0.09% | Benzalkonium chloride, | ||||
| Multidose bottle 5 mL | Flurbiprofen sodium | Boric acid, borax, sodium sulphite anhydrous (E221), tyloxapol, povidone, edetate disodium, water for injections, sodium hydroxide to adjust the pH | solution/drops | Fr | 1991 |
| Trade Name AND Presentation | Active Substance | SAID/ NSAID | Excipients | Pharmaceutical Form | Marketed In | Year of Authorization |
|---|---|---|---|---|---|---|
| Bacitracin-Neomycin-Polymyxin W/ Hydrocortisone Acetate 400 UNITS/GM;1%;EQ 3.5MG BASE/Gm;10,000 Units/GM | Hydrocortisone acetate, Bacitracin zinc, Neomycin sulfate, Polymyxin B sulfate | SAID | ointment | USA | 1981 | |
| - | ||||||
| Blephamide 0.2%; 10% | Prednisolone acetate, Sulfacetamide sodium | SAID | Benzalkonium chloride, | suspension/ drops | USA | 1961 |
| 5 mL in 10 mL multidose bottle 10 mL in 15 mL multidose bottle | Edetate disodium, polysorbate 80, polyvinyl alcohol, potassium phosphate monobasic, purified water, sodium phosphate dibasic, sodium thiosulfate, hydrochloric acid and/or sodium hydroxide to adjust the pH | |||||
| Blephamide S.O.P. 0.2%; 10% | Prednisolone acetate, Sulfacetamide sodium | SAID | Phenylmercuric acetate, | ointment | USA | 1986 |
| 3.5 g multidose tube | Mineral oil, petrolatum alcohol, lanolin alcohol, white petrolatum | |||||
| Chibro Cadron 0.1%; 3 500 UNITS/ML | Dexamethasone sodium phosphate, Neomycin sulfate | SAID | Benzododecinium bromide, | solution/drops | Fr | 1992 |
| Multidose bottle 5 mL | Sodium citrate, polysorbate 80, hydroxyethylcellulose, sodium hydroxide, sodium chloride, purified water, sodium citrate dihydrate | |||||
| Cidermex 0.1%; 3 500 UNITS/GM | Triamcinolone, Neomycin sulfate | SAID | ointment | Fr | 1991 | |
| 3 g multidose tube | Mineral oil, white petrolatum | |||||
| Dexasporin 0.1%; EQ 3.5MG BASE/ML; 10 000 UNITS/ML | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | suspension/ drops | USA | 1995 | |
| - | ||||||
| Frakidex 0.1%; 6 300 UNITS/ML | Dexamethasone sodium phosphate, Framycetine sulfate | SAID | Benzalkonium chloride, | solution/drops | Fr | 1997 |
| Multidose bottle 5 mL | sodium citrate, polysorbate 80, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Frakidex 0.1%; 3 150 UNITS/GM | Dexamethasone sodium phosphate, Framycetine sulfate | SAID | ointment | Fr | 1998 | |
| 5 g multidose tube | Mineral oil, white petrolatum | |||||
| Indobiotic 0.1%; 3 000 UNITS/ML | Indomethacin, Gentamicin sulfate | NSAID | solution/drops | Fr | 2000 | |
| Single use vial 0.35 mL | Hydroxypropylbetadex, arginine, hydrochloric acid, purified water | |||||
| Maxidrol 0.1%; 3500 UNITS/ML; 6 000 UNITS/ML | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | Benzalkonium chloride, | suspension/drops | Fr | 1991 |
| Multidose bottle 3 mL | Methylhydroxypropylcellulose, sodium chloride, polysorbate 20, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Maxidrol 0.1%; 3500 UNITS/GM; 6 000 UNITS/GM | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | Methylparaben, propylparaben, | ointment | Fr | 1997 |
| 3.5 g multidose tube | Lanolin, white petrolatum | |||||
| Maxitrol 0.1%; EQ 3.5MG BASE/ML; 10 000 UNITS/ML | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | Benzalkonium chloride, | suspension/ drops | USA | 1963 |
| 5 mL in 8 mL multidose bottle | Hypromellose, sodium chloride, polysorbate 80, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Maxitrol 0.1%; EQ 3.5MG BASE/GM; 10 000 UNITS/GM | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | Methylparaben, propylparaben, | ointment | USA | 1963 |
| 3.5 g multidose tube | White petrolatum, anhydrous liquid lanolin | |||||
| Maxitrol 0.1%; EQ 3.5MG BASE/ML; 10 000 UNITS/ML | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | suspension/ drops | USA | 1984 | |
| - | ||||||
| Neomycin AND Polymyxin B Sulfates AND Dexamethasone 0.1%; EQ 3.5MG BASE/GM; 10 000 UNITS/GM | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | Methylparaben, propylparaben, | ointment | USA | 1994 |
| 3.5 g multidose tube | White petrolatum, lanolin, mineral oil | |||||
| Neomycin AND Polymyxin B Sulfates AND Dexamethasone 0.1%; EQ 3.5MG Base/GM; 10 000 UNITS/GM | Dexamethasone, Neomycin sulfate, Polymyxin B sulfate | SAID | ointment | USA | 1989 | |
| - | ||||||
| Neomycin AND Polymyxin B Sulfates AND Hydrocortisone 1%; EQ 3.5MG BASE/ML; 10 000 UNITS/ML | Hydrocortisone, Neomycin sulfate, Polymyxin B sulfate | SAID | Potassium metabisulfite, | suspension/ drops | USA | 1988 |
| Multidose bottle 10 mL | Glycerin, propylene glycol, hydrochloric acid, water for injection | |||||
| Neomycin AND Polymyxin B Sulfates, Bacitracin ZINC AND Hydrocortisone 400 UNITS/GM; 1%; EQ 3.5MG BASE/GM; 10 000 UNITS/GM | Hydrocortisone acetate, Bacitracin zinc, Neomycin sulfate, Polymyxin B sulfate | SAID | ointment | USA | 1995 | |
| 3.5 g multidose tube | Mineral oil, white petrolatum | |||||
| Neomycin AND Polymyxin B Sulfates, Bacitracin Zinc AND Hydrocortisone 400 UNITS/GM; 1%; EQ 3.5MG BASE/GM; 10 000 UNITS/GM | Hydrocortisone acetate, Bacitracin zinc, Polymyxin B sulfate Neomycin sulfate, | SAID | ointment | USA | 2012 | |
| 3.5 g multidose tube | ||||||
| Pred-G EQ 0.3%; 0.6% | Prednisolone acetate, Gentamicin sulfate | SAID | Chlorobutanol, | ointment | USA | 1989 |
| 3.5 g multidose tube | Mineral oil, petrolatum, lanolin alcohol, white petrolatum | |||||
| Pred-G EQ 0.3%; 1% | Prednisolone acetate, Gentamicin sulfate | SAID | Benzalkonium chloride, | suspension/ drops | USA | 1988 |
| 5 ml in 10 mL multidose bottle 10 ml in 15 mL multidose bottle | Edetate disodium, hypromellose, polyvinyl alcohol, polysorbate 80, purified water, sodium chloride, sodium citrate dihydrate, hydrochloric acid and/or sodium hydroxide to adjust the pH | |||||
| Sterdex | Dexamethasone, Axytetracycline | SAID | ointment | Fr | 1997 | |
| Single dose vial | Mineral oil, white petrolatum | |||||
| Tobradex 0.1%; 0.3% | Dexamethasone, Tobramycin | SAID | Benzalkonium chloride, | suspension/ drops | USA | 1988 |
| 10 ml in 15 mL multidose bottle | Tyloxapol, edetate disodium, sodium chloride, hydroxyethyl cellulose, sodium sulfate, sulfuric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Tobradex 0.1%; 0.3% | Dexamethasone, Tobramycin | SAID | Chlorobutanol, | ointment | USA | 1988 |
| 3.5 g multidose tube | Mineral oil, white petrolatum | |||||
| Tobradex ST 0.05%; 0.3% | Dexamethasone, Tobramycin | SAID | Benzalkonium chloride, | suspension/ drops | USA | 2009 |
| Multidose bottle 2.5, 5 and 10 mL | Xanthan gum, tyloxapol, edetate disodium, sodium chloride, propylene glycol, sodium sulfate, hydrochloric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Tobradex 0.1%; 0.3% | Dexamethasone, Tobramycin | SAID | Benzalkonium chloride, | suspension/ drops | Fr | 1997 |
| Multidose bottle 5 mL | Edetate disodium, sodium chloride, sodium sulfate, tyloxapol, hydroxyethylcellulose, sulfuric acid and/or sodium hydroxide to adjust the pH, purified water | |||||
| Tobramycin AND Dexamethasone 0.1%; 0.3% | Dexamethasone, Tobramycin | SAID | Benzalkonium chloride, | suspension/ drops | USA | 1991 |
| Multidose bottle 2.5 and 5 mL | Sodium sulfate, sodium chloride, hydroxyethylcellulose, tyloxapol, edetate disodium, purified water, sulfuric acid and/or sodium hydroxide to adjust the pH | |||||
| Zylet 0.5%; 0.3% | Loteprednol etabonate, Tobramycin | SAID | Benzalkonium chloride, | suspension/ drops | USA | 2004 |
| 5 mL in 7.5 mL multidose bottle 10 mL in 10 mL bottle | Edetate disodium, glycerin, povidone, purified water, tyloxapol, sulfuric acid and/or sodium hydroxide to adjust the pH | |||||
| Prednisolone Sodium Phosphate EQ 0.23%; Sulfacetamide Sodium 10% | Prednisolone sodium phosphate, Sulfacetamide sodium | SAID | solution/drops | USA | 1993 | |
| - | ||||||
| Prednisolone Sodium Phosphate EQ 0.23%; Sulfacetamide Sodium 10% | Prednisolone sodium phosphate, Sulfacetamide sodium | SAID | Thimerosal, | solution/drops | USA | 1995 |
| Multidose bottle 5 and 10 mL | Poloxamer 407, boric acid, edetate disodium, purified water, hydrochloric acid and/or sodium hydroxide to adjust the pH |
| Trade Name AND Presentation | Excipients | Pharmaceutical Form | Marketed In | Year of Authorization |
|---|---|---|---|---|
| Cequa 0.09% | solution/drops | USA | 2018 | |
| Single use vial 0.25 mL | Polyoxyl-35 castor oil, octoxynol 40, polyvinylpyrrolidone, sodium phosphate monobasic, sodium phosphate dibasic, hydrochloric acid and/or sodium hydroxide to adjust the pH, water for injection | |||
| Ikervis 1 mg/mL | emulsion | EU, Fr | 2015 | |
| Single use vial 0.3 mL | Medium-chain triglycerides, cetalkonium chloride, glycerol, tyloxapol, poloxamer 407, sodium hydroxide to adjust the pH, water for injection | |||
| Restasis 0.05% | emulsion | USA | 2002 | |
| Single use vial 0.4 mL | Glycerin, castor oil, polysorbate 80, carbomer 1342, sodium hydroxide to adjust the pH, purified water | |||
| Restasis 0.05% | emulsion | USA | 2016 | |
| 5.5 mL in 10 mL multidose bottle | Glycerin, castor oil, polysorbate 80, carbomer copolymer A, sodium hydroxide to adjust the pH, purified water | |||
| Verkazia 1mg/mL | emulsion | EU | 2018 | |
| Single use vial 0.3 mL | Medium-chain triglycerides, cetalkonium chloride, glycerol, tyloxapol, poloxamer 407, sodium hydroxide to adjust the pH, water for injection |
| Drug | System | Main Components | Key Results | Ref. |
|---|---|---|---|---|
| Aceclofenac | Nanoparticles | EUDRAGIT®RS 100, Polysorbate 80, mannitol, water | High entrapment efficiency (>90%) Sustained drug release in vitro 2-fold higher transcorneal permeation ex vivo as compared with aceclofenac solution Higher anti-inflammatory activity in vivo than marketed formulation | [100] |
| EUDRAGIT®RL 100, Polysorbate 80, mannitol, water | High entrapment efficiency (>95%) 2-fold higher transcorneal permeation ex vivo as compared with aceclofenac solution Higher anti-inflammatory activity in vivo than marketed formulation | [101] | ||
| Amfenac | Nanoparticles | Catechin, HAuCl4, tris acetate buffer, water | No irritation effect in vivo and no cytotoxic effect in vitro Higher efficiency in DED treatment in vivo than marketed formulation of ciclosporin A | [102] |
| Bromfenac Sodium | Liposomes | L-α-distearoylphosphatidylcholine, dicetylphosphate, cholesterol, acetate salt solution, Hank’s balanced salt solution, 2-morpholinoethanesulfonic acid monohydrate, chitosan, water | Good entrapment efficiency (>75%) Sustained drug release without burst effect in vitro | [103] |
| Celecoxib | Nanoparticles | Poly-ε-caprolactone, poloxamer 188, Sorenson’s phosphate buffer, water | High entrapment efficiency (>89%) Sustained drug release without burst effect in vitro ≈ 2-fold higher corneal permeation ex vivo Higher anti-inflammatory activity in vivo than marketed formulation | [104] |
| Solid lipid nanoparticles | Lipid glyceryl monostearate, PVA, polysorbate 80, poloxamer 188, Sorenson’s phosphate buffer, water | Entrapment efficiency (65 < X < 94%) Sustained drug release with burst effect in vitro ≈ 2-fold higher corneal permeation ex vivo Higher anti-inflammatory activity in vivo than marketed formulation | [104] | |
| Dexibuprofen | Nanoparticles | PLGA-PEG 5%, PVA, water | No irritant effect in vitro and in vivo High entrapment efficiency (>85%) Sustained drug release up to 12 h in vitro and ex vivo Sustained anti-inflammatory activity in vivo | [105] |
| Diclofenac | Nanoparticles | Methoxy poly(ethylene glycol)-poly(ε-caprolactone)-chitosan copolymer, sodium chloride, water | No cytotoxic effect in vitro no irritation effect in vivo High entrapment efficiency (>95%) Sustained drug release up to 8 h in vitro ≈1.4-fold higher corneal penetration ex vivo than marketed formulation 2.3-fold higher concentration in aqueous humor in vivo than marketed formulation | [106] |
| NaOH, Zn(NO3)2 6H2O, Al(NO3)3 9H2O, PVP K30, trichlorobutanol, water | No irritation effect in vivo High corneal penetration ex vivo High apparent permeability coefficient and prolonged precorneal retention time in vivo | [107] | ||
| Diclofenac Sodium | Liposomes | Phosphatidylcholine, cholesterol, phosphatidylserine low molecular weight chitosan and sodium chloride, water | No irritation effect in vivo High entrapment efficiency (>95%) ≈2-fold higher corneal penetration at 6 h ex vivo than diclofenac solution | [108] |
| Micelles | Methoxypoly(ethylene glycol)-poly(ε-caprolactone), water | No irritation effect in vivo Good entrapment efficiency (>70%) Sustained drug release in vitro up to 24 h 17-fold higher corneal penetration ex vivo 3-fold higher concentration in aqueous humor in vivo 2-fold higher bioavailability in vivo | [109] | |
| Diclofenac Sodium | Nanoparticles | N-trimethyl chitosan, phosphate buffer, polysorbate 80, sodium tripolyphosphate, water | No irritating effect in vitro and in vivo Entrapment efficiency >70% Sustained drug release in vitro ≈2-fold higher concentration in aqueous humor in vivo at 1 h | [95] |
| Nanoparticles | PLGA, poly[Lac(Glc-Leu)], polysorbate 80, benzalkonium chloride, mannitol, water | No irritants effect in vivo Sustained drug release in vitro up to 14 h | [110] | |
| Solid lipid nanoparticles | PHOSPHOLIPON 90G®, goat fat, polysorbate 80, sorbitol, thimerosal, water | High entrapment efficiency (≈90%) Sustained drug release in vitro Higher corneal permeation flux | [111] | |
| Flurbiprofen | Cubosomes | Glyceryl monooleate, poloxamer 407, glycerol, water | No irritation effect in vivo High entrapment efficiency (>98%) Sustained drug release without burst effect in vitro 2.5- and 2-fold higher apparent permeability ex vivo 2-fold higher aqueous humor concentration in vivo at 3 h | [112] |
| Liposomes | Chitosan, egg phosphatidylcholine, cholesterol, SOLUTOL®HS-15, HCl, water | No irritation effect in vivo High encapsulation efficiency (>90%) 4.59-, 3.56- and 2.36-fold higher apparent permeability ex vivo 4.11- and 2.19-fold higher prolonged retention time in vivo | [113] | |
| Nanoemulsion | PLGA, poloxamer 188, water | High entrapment efficiency (>85%) Sustained drug release in vitro ≈1.7-fold increase corneal permeation ex vivo than marketed formulation | [114] | |
| Nanoparticles | EUDRAGIT®RS 100 and RL 100, polysorbate 80, phosphate buffer, benzalkonium chloride, water | No irritation effect in vivo High entrapment efficiency (>85%) Sustained drug release without burst effect Higher concentration in aqueous humor than with marketed formulation | [115] | |
| PLGA, poloxamer 188, PVA, water | No irritation effect in vivo Good entrapment efficiency (>75%) Sustained drug release in vitro Higher anti-inflammatory activity in vivo than marketed formulation | [116] | ||
| Poly-ε-caprolactone, poloxamer 188, water | Entrapment capacity (>75%) Sustained drug release in vitro | [117,118] | ||
| PLGA or poly-ε-caprolactone, water | Good entrapment efficiency (>85%) ≈ 3.9- and 7.6-fold increase corneal permeation ex vivo | [119] | ||
| PLGA, poloxamer 188, water | No irritation effect in vitro High entrapment efficiency (>90%) Sustained drug release in vitro | [120] | ||
| Poly-ε-caprolactone, poloxamer 188, trehalose or PEG3350, water | No irritating effect in vitro and in vivo Good entrapment efficiency (>85%) Sustained drug release in vitro Enhance corneal permeation ex vivo Higher anti-inflammatory activity in vivo | [121] | ||
| Solid lipid nanoparticles | Stearic acid, MIGLYOL® 812, castor oil, polysorbate 80, water | No irritation effect in vivo Good entrapment efficiency (>75%) Sustained drug release without burst effect in vitro | [122] | |
| Flurbiprofen Axetil | Nanoemulsion | Castor oil, polysorbate 80, glycerin, carbomer 974P, sodium acetate, boric acid, sorbic acid, water | High entrapment efficiency (>98%) Better ocular biocompatibility than marketed formulation Higher anti-inflammatory activity in vivo than marketed formulation | [123] |
| Ibuprofen | Liposomes | Soybean phospholipids, cholesterol, octadecylamine, water | 72.9 % entrapment efficiency 1.64-fold higher corneal permeation ex vivo at 6 h 1.53-fold higher aqueous humor concentration in vivo | [124] |
| Liposomes | Cotton-like silk fibroin, phosphate buffer, purified soybean lecithin, cholesterol, stearylamine, water | No cytotoxic effect in vitro Entrapment efficacy (59 < X < 86%) Sustained release in vitro and sustained corneal permeation ex vivo | [125] | |
| Solid lipid nanoparticles | Polyoxyl-35 castor oil, COMPRITOL® 888 ATO, Gelucire 44/14 or TRANSCUTOL® P or stearylamine, MIGLYOL® 812, water | High entrapment efficiency (>90%) 4.19-fold higher corneal apparent permeability ex vivo 3.99-fold increase of aqueous humor drug concentration in vivo | [126] | |
| Ibuprofen Sodium Salt | Nanoparticles | EUDRAGIT®RS 100, polysorbate 80, water | Higher anti-inflammatory activity in vivo than marketed formulation ≈ 1,5-fold higher aqueous humor concentration in vivo than with ibuprofen solution | [127] |
| Nanoparticles | EUDRAGIT® RS 100, polysorbate 80, benzalkonium chloride, water | Good ocular tolerability High entrapment efficiency (>90%) Sustained drug release Higher aqueous humor concentration in vivo | [128] | |
| Indomethacin | Microparticles/ Nanoparticles | Zirconia beads and Bead Smash 12, benzalkonium chloride, mannitol or methylcellulose, HPβCD, sodium chloride, water | Better ocular tolerance than marketed formulation in vitro ≈ 6-fold higher corneal penetration in vitro ≈ 10-fold higher corneal penetration in vivo | [129] |
| Nanoemulsion/ Nanoparticles | NC: Poly-ε-caprolactone, lecithin, MIGLYOL® 840, poloxamer 188, water NE: Lecithin, MIGLYOL® 840, poloxamer 188, water NP: Poloxamer 188, water | Good tolerance in vivo High entrapment efficiency (>89%) Sustained drug release 4–5-fold higher corneal penetration ex vivo than marketed formulation | [130] | |
| Nanoemulsion/Nanoparticles | NP: Chitosan with tripolyphosphate, acid acetic, water NE: Chitosan, lecithin soya, MIGLYOL® 840 and Poloxamer 188 or PVA or polysorbate 80, sorbitol, benzalkonium chloride, water | Good entrapment efficiency (>75%) Sustained release in vitro 30-fold higher corneal concentration in vivo at 1 h with NE than with solution 13-fold higher aqueous humor in vivo at 6 h post instillation with NE than with solution | [97] | |
| Nanoparticles | Poly-ε-caprolactone, lecithin, MIGLYOL® 840, poloxamer 188, poly-l-lysin or chitosan, water | Good tolerance in vivo High entrapment efficiency (>90%) Rapid release in vitro 4-6 and 4-7-fold higher corneal and aqueous humor concentrations in vivo after 30 and 60 minS post-instillation than marketed formulation | [131] | |
| Solid lipid nanoparticles | COMPRITOL® 888 ATO, poloxamer 188 and/or polysorbate 80, glycerin, NaOH or HCl, water | Entrapment efficiency (>70%) 3 – 4.5-fold higher corneal permeability ex vivo than marketed formulation | [132] | |
| Ketorolac Tromethamine | Micelles | Copolymer of N-isopropylacrylamide, vinyl pyrrolidone and acrylic acid crosslinked with N,N′-methylene bis-acrylamide, water | 30% entrapment efficiency Sustained release in vitro 2-fold higher corneal permeation ex vivo Higher anti-inflammatory activity up to 3 h and PMN migration in vivo | [94] |
| Nanoparticles | Chitosan, acetic acid, NaOH, tripolyphosphate, water | Entrapment efficiency (34 < X < 41%) Sustained drug release | [133] | |
| Chitosan, acetic acid, tripolyphosphate, NaOH, water | Entrapment efficiency (5 < X < 75%) Sustained release in vitro up to 6 h 3.77-fold lower permeation parameters lower than solution ex vivo | [134] | ||
| Naproxen | Microparticles | Sodium alginate, carbomer 974P, hydroxypropyl methylcellulose, paraffin, calcium chloride, water | Good entrapment efficiency (63 < X < 76%) Sustained release in vitro without burst effect | [135] |
| Nanoparticles | PLGA, PVA, water | High entrapment efficiency (>80%) Sustained drug release in vivo without burst effect in vitro | [136] | |
| Nepanefac | Nanoaggregates | PVP, PVA, carboxymethylcellulose, hydroxypropylmethylcellulose, methyl cellulose, tyloxapol, γCD, HPβCD, EDTA, benzalkonium chloride, sodium chloride, water | Good entrapment efficiency (>60%) | [137] |
| Phospho-Sulindac | Nanoparticles | Methoxy poly(ethylene glycol)-poly(lactide), sodium cholate, water, phosphate buffer | Entrapment efficacy 46.4% Sustained drug release in vitro up to 24 h | [138] |
| Piroxicam | Microparticles | Albumin, sodium chloride or sorbitol, water | High entrapment efficiency (>99%) Sustained release in vitro 1.8-fold higher bioavailability in vivo than marketed formulation | [139] |
| Nanoparticles | EUDRAGIT®RS 100, hydroxypropyl methylcellulose, PVA, sodium chloride, water | Sustained release in vitro Great anti-inflammatory activity in vivo up to 12 h but no difference compared with microsuspension | [140] |
| Drug | System | Main Components | Key Results | Ref. |
|---|---|---|---|---|
| Dexamethasone | Cubosomes | Monoolein, poloxamer 407, glycerol, water | Good tolerance in vitro High entrapment efficiency (>95%) 4.5 - 3.5-fold higher apparent permeability in vitro 1.8 fold increase the concentration in aqueous humor in vivo | [141] |
| Microemulsion | Isopropyl myristate, polysorbate 80, propylene glycol, chitosan, acetate buffer, water | No irritation effect in vivo High entrapment efficiency (>95%) Sustained drug release with burst effect in vitro Higher anti-inflammatory activity in vivo than marketed formulation | [142] | |
| Microparticles/Nanoparticles | Zirconia beads and Bead Smash 12,methylcellulose, propyl p-hydroxybenzoate, methyl p-hydroxybenzoate, water | No cytotoxic effect in vitro ≈ 5.1-fold higher corneal penetration of nanoparticles than marketed formulation in vivo | [143] | |
| Nanogels suspension | HPγCD, γCD nanogels, EDTA, benzalkonium chloride, hydroxypropylmethylcellulose, sodium chloride, pH adjuster, water | No irritation effect in vitro and in vivo Sustained drug release without burst effect ≈ 80-fold increase concentration in tear fluid at 6 h in vivo 3-fold increase concentration in aqueous humor in vivo, 2 h after instillation | [144] | |
| N-tert-butylacrylamide, methylcellulose, nitric acid, cerium ammonium nitrate, water | No cytotoxic effect in vitro High entrapment encapsulation efficiency (>95%) Sustained drug release without burst effect | [145] | ||
| Nanomicelles | Polyoxyl-40-stearate, polysorbate 80, water | No irritation effect in vivo Sustained drug release in vitro | [146] | |
| Nanoparticles | Ethyl cellulose or EUDRAGIT® RS or ethyl cellulose/EUDRAGIT® RS, PVA, water | No toxicity, except for ethylcellulose particles Entrapment efficiency (12 < X < 87%) Sustained drug release without burst release | [147] | |
| Propylene glycol, phosphate buffer, EDTA, poloxamer 188, hydroxyethylcellulose, benzalkonium chloride, water | Higher intensity of drug action Higher extent of drug absorption | [148] | ||
| γCD, HPγCD, poloxamer 407, benzalkonium chloride, EDTA, sodium chloride, water | 15-fold higher concentration than marketed formulation | [88] | ||
| Nanosponges | βCD nanosponge, water | No irritation or toxic effect ex vivo Entrapment efficiency (3 < X < 10%) Sustained drug release without burst effect ≈2-fold higher corneal permeability ex vivo | [149] | |
| Solid lipid nanoparticles | Soy lecithin, soybean oil, glycerol, poloxamer 188+/-chitosan, water | No irritation effect in vivo Entrapment efficiency (30 < X < 70%) Sustained drug release in vitro 4.69-fold higher concentration in aqueous humor from L/NPs with chitosan than aqueous solution in vivo | [150] | |
| Dexamethasone Sodium Phosphate | Microparticles | RMβCD or γCD, benzalkonium chloride, EDTA, sodium chloride, hydroxypropylmethylcellulose, water | No irritation effect in vivo 3-8-fold higher concentration in aqueous humor 2 h after instillation in vivo than marketed formulation | [151] |
| Nanoparticles | Chitosan, sodium tripolyphosphate, acid acetic, phosphate buffer, hyaluronic acid, water | No irritation effect in vivo Entrapment efficiency (58 < X < 73%) Sustained drug release in vitro Prolonged precorneal retention in vivo ≈ 8-fold increase the aqueous concentration at 6 h in vivo | [152,153] | |
| Quaternary ammonium-chitosan conjugate or its thiolated derivative, acid hyaluronic, phosphate buffer, water | No irritation effect in vivo Entrapment efficiency (18 < X < 35%) Sustained drug release in vitro Sustained residence time in tear fluid in vivo | [154] | ||
| Fluocinolone Acetonide | Liposomes | α-, β and HPβCD, water, dextrose, glucose, phosphatidyl choline, triolein, cholesterol, L-lysine, phosphate buffer, water | Entrapment efficiency (7 < X < 52%) Sustained release in vitro up to 180h for FA-HPβCD complex | [155] |
| Nanoparticles | PLGA P 5002 or 7502, poloxamer 407, phosphate buffer, chitosan HCl, water | No irritation effect in vivo Entrapment efficiency (> 50%) Sustained drug release in vitro ≈ 2.5-fold higher concentration in tear sample in vivo at 1h | [156] | |
| Fluoro-Metholone | Nanoparticles | PLGA, poloxamer188, water | No irritation effect in vitro and in vivo High entrapment efficiency (>99%) Sustained drug release in vitro ≈2.2-fold higher increase corneal permeation ex vivo than marketed formulation Higher anti-inflammatory activity in vivo at 30 mins than marketed formulation | [91] |
| Hydrocortisone | Micelles/Nanoparticles | Albumin, glutaraldehyde, sodium metabisulfite, glucose, polysorbate 80, phosphate buffer, water | Entrapment efficiency (16 < X < 70%) Sustained corneal permeation ex vivo Neither higher AUC values nor prolonged release in vivo | [157] |
| Nanoparticles | Propylene glycol, isotonic phosphate buffer, EDTA, hydroxyethylcellulose, benzalkonium chloride, poloxamer 188, water | Higher intensity of drug action Higher extent of drug absorption | [148] | |
| Gelatin A or B, water, HCl or NaOH, sodium metabisulfite, HPβCD, glutaraldehyde, water | Entrapment efficiency (35 < X < 45%) Sustained drug release in vitro closed to zero order, 30% in 200 min | [158] | ||
| Loteprednol Etabonate | Nanogels suspension | N-boc ethylenediamine, polysorbate 60, chitosan, succinic anhydride, 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide, N-hydroxysuccinimide, phosphate buffer, water | No cytotoxic effect in vitro Good entrapment efficiency (67 < X < 70%) Sustained release in vitro | [159] |
| Nanoparticles | PLGA, PVA, water | Good entrapment efficiency (>70%) Improve ex vivo transcorneal penetration | [160] | |
| Methyl-Prednisolone Acetate | Nanoparticles | EUDRAGIT®RS 100, PVA, sodium chloride, hydroxypropylmethylcellulose, water | No irritation effect in vivo Sustained release in vitro Higher anti-inflammatory activity up to 36 h in vivo | [161] |
| Pirfenidone | Nanoparticles | Monoolein, poloxamer P 407, oleic acid, NaOH, glycerin, water | No irritation effect in vitro Entrapment efficiency (6 < X < 36%) Sustained release in vitro Reduction in ocular lesions associated with a reduction of inflammatory cells in vivo | [162] |
| Prednisolone | Micelles | Quaternary ammonium palmitoyl gycol chitosan, poloxamer 407, water | 45% entrapment efficiency 10-fold aqueous humor concentration in vivo | [163] |
| Nanoparticles | Poly-ε-caprolactone or EUDRAGIT® RS100, castor oil and mineral oil, sorbitan monostrearate, polysorbate 80, water | No irritation effect in vitro, no cytotoxic effect in vitro Entrapment efficiency (45 < X < 52%) Sustained release in vitro | [164] | |
| Propylene glycol, phosphate buffer, EDTA, hydroxyethylcellulose, benzalkonium chloride, poloxamer 188, water | Higher intensity of drug action Higher extent of drug absorption | [148] | ||
| Prednisolone Acetate | Liposomes | 1,2-dipalmitoyl-sn-glycerol-3-phosphocholine, cholesterol, stearylamine, water | High entrapment efficiency (78 < X < 90%) Sustained release in vitro 1.2 – 2.8-fold lower apparent corneal permeability ex vivo than solution ≈ 3 – 5-fold higher aqueous humor concentration at 3 h in vivo than solution Higher anti-inflammatory activity in vivo with positively charged unilamelar liposome | [165] |
| Prednisolone Acetate or Phosphate | Ethoniosomes | SPAN® 60, cholesterol, phosphate buffer, water | No irritation effect in vivo Entrapment efficiency >85% for prednisolone acetate and 25 < X < 46% for Prednisolone phosphate Sustained release in vitro Higher corneal permeation than marketed formulation Lower bioavailability than marketed formulation Quicker anti-inflammatory activity than marketed formulation | [166] |
| Prednisolone Gatifloxacine | Nanoparticles | EUDRAGIT®RS 100, RL 100, hyaluronic acid, benzalkonium chloride, EDTA, water | Good entrapment efficiency (>60%) Sustained release in vitro 5.23-fold higher and sustained concentration in aqueous humor in vivo than marketed formulation | [167] |
| Triamcinolone Acetonide | Nanoparticles | Methoxypoly(ethylene glycol)-poly(dl-lactic-co-glycolic acid),PVA, water | No cytotoxic effect in vitro 77% entrapment efficiency Sustained release maintained for 45 days in vitro anti-inflammatory activity in vivo | [168] |
| Poly-ε-caprolactone, poloxamer 188, water | No cytotoxic effect in vitro 60% encapsulation efficiency Sustained release in vitro anti-inflammatory activity in vivo | [169] | ||
| PLGA, PVA, water | Poor entrapment efficiency (12 < X < 32%) Sustained release in vitro Similar anti-inflammatory activity in vivo than intravitreal injection | [170] |
| Drug | System | Main Components | Key Results | Ref. |
|---|---|---|---|---|
| Celecoxib | Nanoparticles in gel | Lecithin, poloxamer 188, PVA, poly-ε-caprolactone or PLA or PLGA, trehalose, hydroxypropylmethylcellulose or methylcellulose, phosphate buffer, benzalkonium chloride, water | No cytotoxic effect in vitro Good entrapment efficiency (>79%) Sustained drug release without burst effect in vitro | [176] |
| Celecoxib | Nanoparticles in gel | Chitosan or sodium alginate, poly-ε-caprolactone or PLA or PLGA, lecithin, PVA, poloxamer 188, trehalose, hydroxypropylmethylcellulose or methylcellulose, phosphate buffer, benzalkonium chloride, water | ≈ 5-fold higher concentration in aqueous humor in vivo 4.8–29.7-fold higher bioavailability in vivo than marketed formulation | [174] |
| Celecoxib | Nanoparticles in gel | Chitosan or poly-ε-caprolactone, sodium alginate, lecithin, PVA or poloxamer 188, acetic solution, trehalose, hydroxypropylmethylcellulose or methylcellulose, benzalkonium chloride, water | No cytotoxic effects in vitro Entrapment efficiency (>75%) Sustained drug release without burst effect in vitro | [177] |
| Diclofenac | Micelles in gel | Methoxypoly(ethylene glycol)-poly-ε-caprolactone copolymer,αCD, water | Low cytotoxic effects in vitro No irritant effects in vivo Sustained drug release in vitro up to 216 h, 2.37-fold higher concentration in aqueous humor in vivo 1h after instillation compared to micelles | [178] |
| Flurbiprofen | Solid lipid nanoparticles in gel | COMPRITOL® 888 ATO, saturated fatty acid of C18, Gelificante PFC carbomer, MIGLYOL® 812, castor oil, Polysorbate 80, glycerol, NaOH, water | No irritation effects in vivo Good entrapment efficiency (>70%) Sustained release without burst effect in vitro, Higher corneal permeation ex vivo | [179] |
| Ibuprofen | Solid lipid nanoparticles in-situ forming gel | COMPRITOL® 888 ATO, MIGLYOL® 812, cetyltrimethylammonium bromide, Polysorbate 80, poloxamer 407, water | No cytotoxic in vitro High entrapment efficiency (>90%) Sustained release in vitro | [180] |
| Ketorolac Tromethamine | Nanoparticles in-situ forming gel | EUDRAGIT®RL 100, poloxamer 407, hydroxypropylmethylcellulose, citrate-phosphate buffer, PVA, water | No irritation effect in vivo Entrapment efficiency (51 < X < 92%) ≈ 3-fold higher corneal permeation ex vivo ≈ 4-fold higher concentration in aqueous humor in vivo at 4 h | [181] |
| Meloxicam | Nanoaggregates in contact lens | Bovine serum albumin, polysorbate 80, NaOH, HCl, 2-HEMA monomer, tetraethylene glycol dimethacrylate, ethylene glycol, sodium metabisulfite, ammonium persulfate, water | No irritation effect in vivo Sustained drug release without burst effect in vitro Reduce corneal penetration ex vivo | [182] |
| Nepanefac | Nanoparticles in-situ forming gel | Tetraethyl orthosilicate, cetyltrimethyl ammonium bromide, ammonia, polysorbate 80, poloxamer 407, Pluronic F67 or chitosan, water | No cytotoxic effect in vitro High entrapment capacity (>98%) Sustained drug release in vitro 3.68-fold higher corneal permeation ex vivo | [183] |
| Piroxicam | Microparticles /Microparticles in gel | Pectine, polyacrylate gel, water | Entrapment efficiency (41 < X < 46%) ≈ 5–6-fold higher residence time in vivo ≈ fold increase bioavailability in aqueous humor in vivo than marketed formulation | [184] |
| Pranoprofen | Nanoparticles in gel | PLGA, PVA, carbomer 934P, glycerol, glycerin or azone, water | No irritation effects in vitro and in vivo High entrapment efficiency (>80%) Sustained release in vitro Greater anti-inflammatory effect in the cornea in vivo than marketed formulation | [185] |
| Drug | System | Main Components | Key Results | Ref. |
|---|---|---|---|---|
| Dexamethasone | Nanoparticles in-situ forming gel | Poloxamer 188, poloxamer 407, water | No irritation effects in vivo Sustained drug release in vitro 2.56-fold higher corneal permeation ex vivo ≈3-fold higher concentration in aqueous humor in vivo | [186] |
| Dexamethasone | Solid lipid nanoparticles in gel | Soybean oil, glycerol, poloxamer 188, poloxamer 407, water | No irritation effects in vivo Entrapment efficiency >50% Sustained drug release 2.56-fold increase corneal permeability ex vitro ≈3-fold higher concentration in aqueous humor in vivo at 6h after instillation than marketed formulation | [187] |
| Dexamethasone Acetate | Nanoparticles in film hydrogel | Kaolin, hydroxypropyl methylcellulose 5 and 15000cps, triethanolamine, water | Poor entrapment efficiency (8.89–9.8%) Controlled drug releases in vitro up to 6h without burst effect Kaolin extends the corneal permeation up to 6h ex vivo Sustained anti-inflammatory activity in vivo | [188] |
| Fluorometholone | Nanoparticles in-situ forming gel | PLGA, poloxamer 407, sodium alginate, sodium carboxymethylcellulose, benzalkonium chloride, water | No irritation effect in vitro and in vivo Sustained drug release in vitro Higher corneal residence time than marketed formulation in vivo 2–3-fold higher concentration in aqueous humor than marketed formulation in vivo Greater capacity in decreasing OII than marketed formulation in vivo | [189] |
| Loteprednol Etabonate | Nanoemulsion in-situ forming gel | Propylene glycol monocaprylate, poloxamer 407, poloxamer 188, benzalkonium chloride, artificial tear fluid, acetate buffer, cetalkonium chloride, glycerin, water | Zero-order drug release kinetics No irritation in vitro High entrapment efficiency (>95%) 2.54-fold higher bioavailability compared to marketed formulation in vivo | [190] |
| Prednisolone Acetate | Nanoparticles in gel | Acetic acid, PVA, sodium deoxycholate, methylparaben, propylparaben, hydroxypropylmethylcellulose, water | Entrapment efficiency (35 < X < 60%) Sustained drug release in vitro Greater anti-inflammatory effects in vivo than marketed formulation | [191] |
| Maximal Number of Particles | Diameter | |||
|---|---|---|---|---|
| ≥10 µm | ≥25 µm | ≥50 µm | ≥90 µm | |
| According to <798> USP | 50 per mL | 5 per mL | 2 per mL | |
| According to EP 10th | 20 per 10 µg of solid active substance | 2 per 10 µg of solid active substance | None per 10 µg of solid active substance | |
| Cell Viability | UN GHS Classification | Applicability | |
|---|---|---|---|
| At 5% | At 0.05% | ||
| >70% | >70% | No category | No serious damage nor eye irritation effect |
| ≤70% | >70% | No prediction can be made | No prediction can be made, eventual eye irritation |
| ≤70% | ≤70% | Category I | Serious eye damage |
| Items | Primary Cell Cultures | Immortalized Cell Line | Reconstructed Tissue Culture |
|---|---|---|---|
| Obtention | From rabbit’s corneal tissue or human corneal epithelial cells by excising the tissue and allowing it to adhere | By maintaining the harvested cells in suitable growth medium and transfecting them with a viral vector to induce cell division | From bovine or human corneal tissue construct |
| Advantages | Relatively cheap and easy | Good correlation with excised rabbit cornea | Morphology similar to excised cornea More accurate way to mimic the cornea |
| Disadvantages | Are not a true representation of the whole cornea | Exhibit abnormal gene expression and/or biological function |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazet, R.; Yaméogo, J.B.G.; Wouessidjewe, D.; Choisnard, L.; Gèze, A. Recent Advances in the Design of Topical Ophthalmic Delivery Systems in the Treatment of Ocular Surface Inflammation and Their Biopharmaceutical Evaluation. Pharmaceutics 2020, 12, 570. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics12060570
Mazet R, Yaméogo JBG, Wouessidjewe D, Choisnard L, Gèze A. Recent Advances in the Design of Topical Ophthalmic Delivery Systems in the Treatment of Ocular Surface Inflammation and Their Biopharmaceutical Evaluation. Pharmaceutics. 2020; 12(6):570. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics12060570
Chicago/Turabian StyleMazet, Roseline, Josias B. G. Yaméogo, Denis Wouessidjewe, Luc Choisnard, and Annabelle Gèze. 2020. "Recent Advances in the Design of Topical Ophthalmic Delivery Systems in the Treatment of Ocular Surface Inflammation and Their Biopharmaceutical Evaluation" Pharmaceutics 12, no. 6: 570. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics12060570