
Sustained-Release Microspheres of Rivoceranib for the Treatment of Subfoveal Choroidal Neovascularization

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation and Characterization of Rivoceranib Microspheres
2.3. Differential Scanning Calorimetric (DSC) and Fourier-Transform Infrared (FTIR) Spectral Studies
2.4. Drug Release Profiles of PLGA/Rivoceranib Microspheres
2.5. Animals
2.6. Mouse Model of Laser-Induced Choroidal Neovascularization (CNV)
2.7. Quantification of Laser-Induced CNV
2.8. Statistical Analysis
3. Results
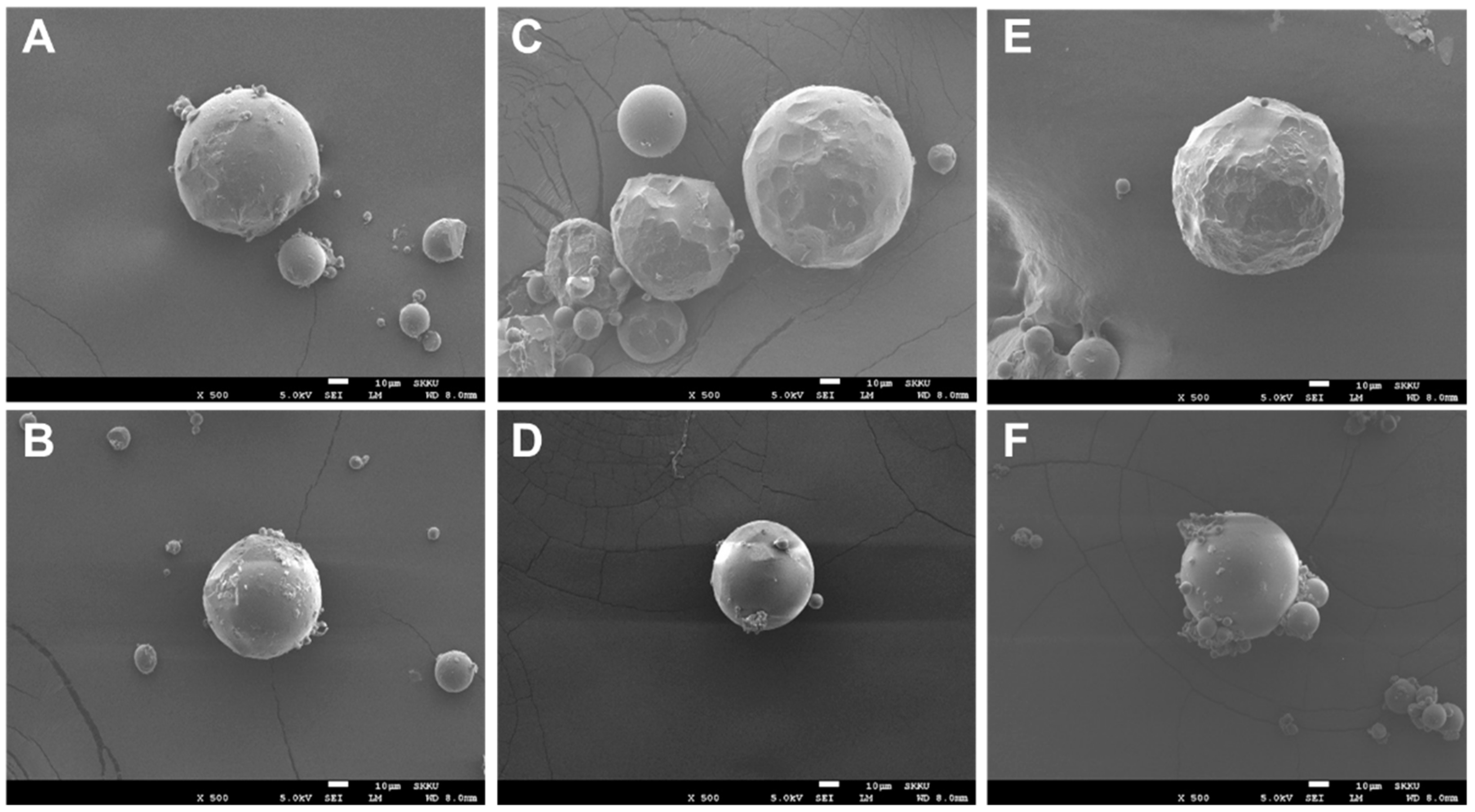
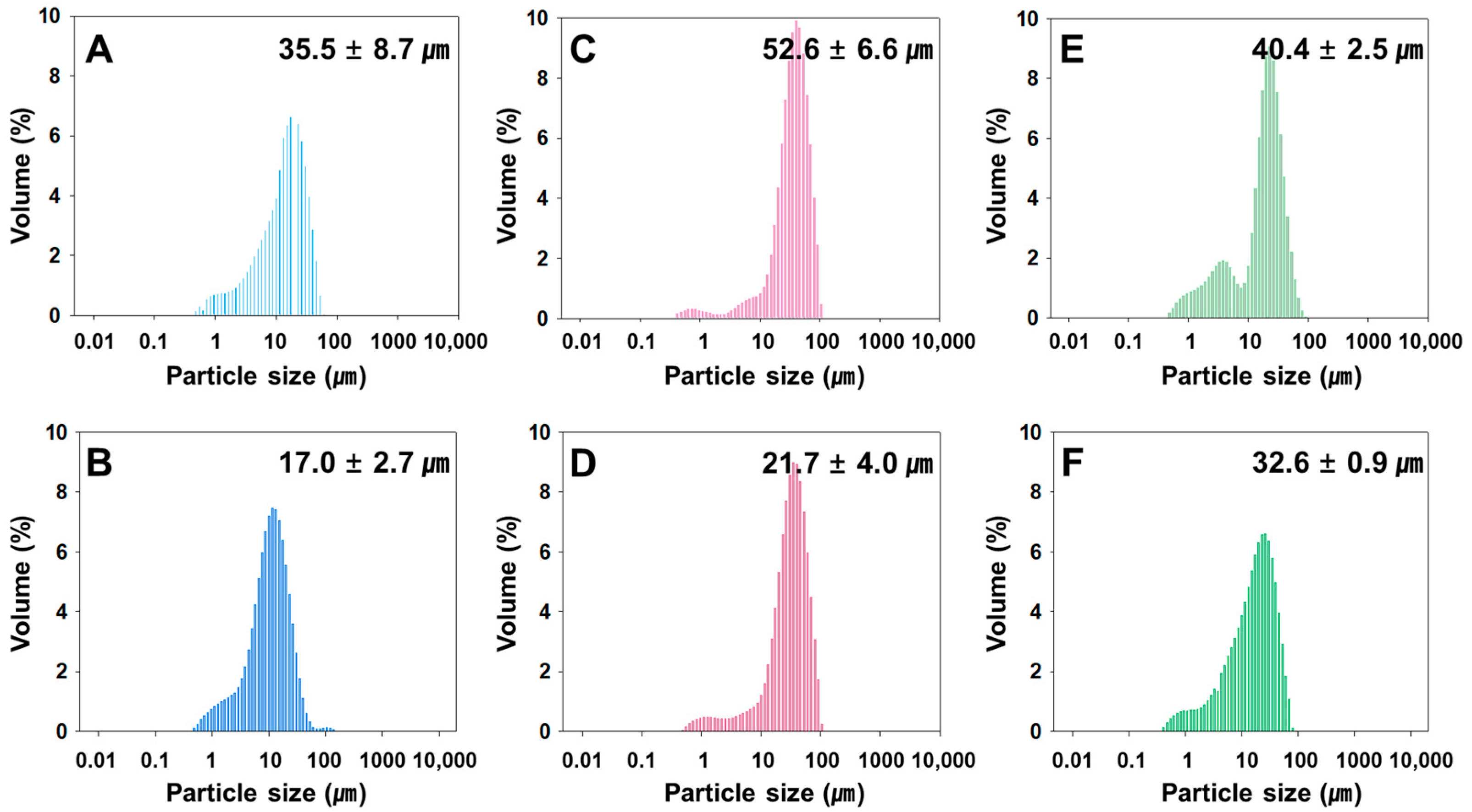
3.1. Preparation and Characterization of Rivoceranib Microspheres
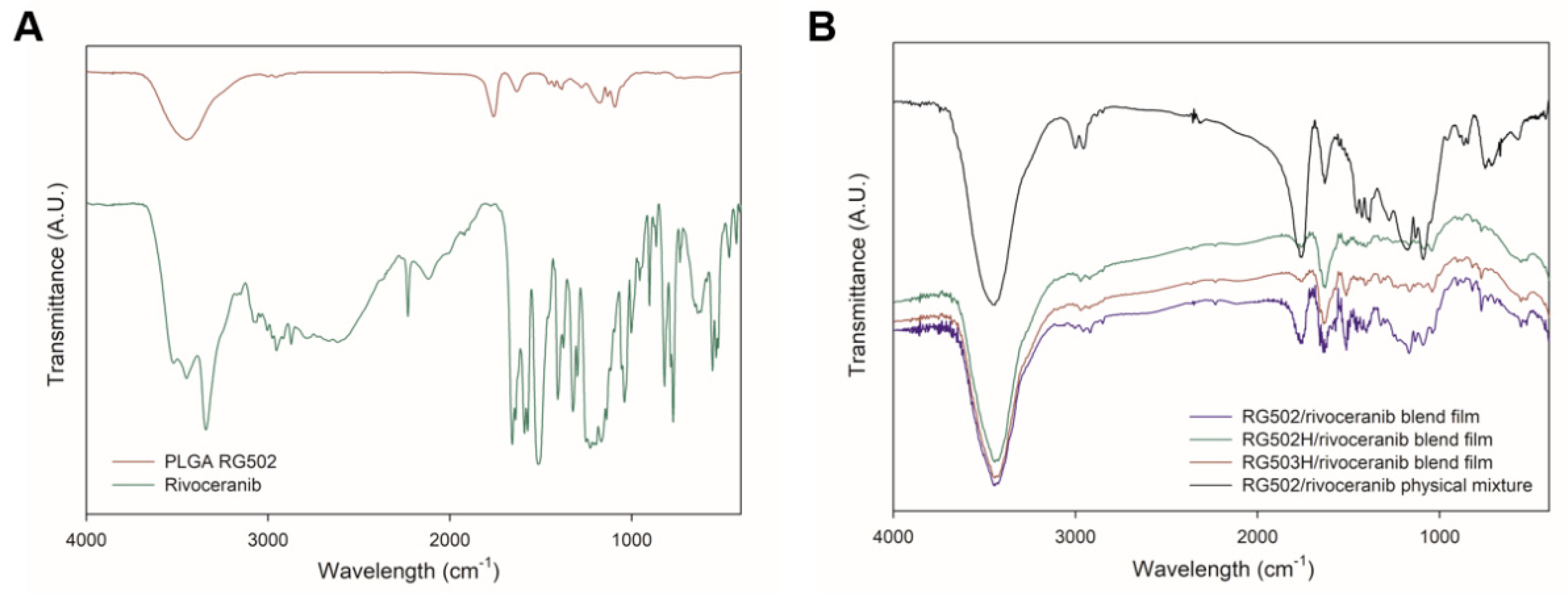
3.2. Polymer–Drug Interactions
3.3. Sustained Drug Release Profiles of Rivoceranib Microspheres
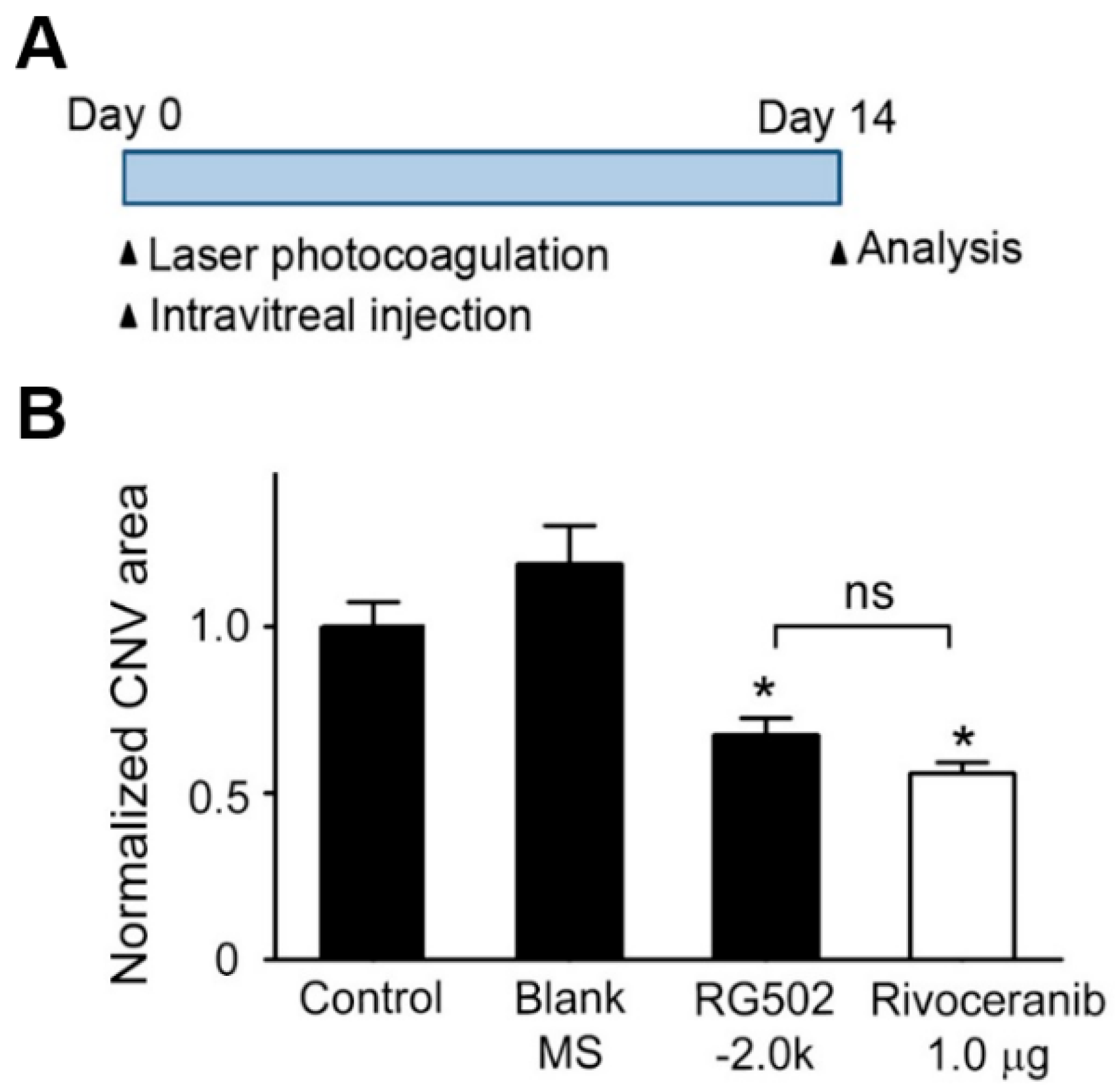
3.4. Suppression of CNV Formation in Mice by Intravitreal Administration of Rivoceranib Microspheres
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Klaver, C.C.; Wolfs, R.C.; Vingerling, J.R.; Hofman, A.; de Jong, P.T. Age-specific prevalence and causes of blindness and visual impairment in an older population: The rotterdam study. Arch. Ophthalmol. 1998, 116, 653–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleckenstein, M.; Keenan, T.D.; Guymer, R.H.; Chakravarthy, U.; Schmitz-Valckenberg, S.; Klaver, C.C.; Wong, W.T.; Chew, E.Y. Age-related macular degeneration. Nat. Rev. Dis. Primers 2021, 7, 31. [Google Scholar] [CrossRef]
- Bird, A.C.; Bressler, N.M.; Bressler, S.B.; Chisholm, I.H.; Coscas, G.; Davis, M.D.; de Jong, P.T.; Klaver, C.C.; Klein, B.E.; Klein, R.; et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The international arm epidemiological study group. Surv. Ophthalmol. 1995, 39, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Holz, F.G.; Wolfensberger, T.J.; Piguet, B.; Gross-Jendroska, M.; Wells, J.A.; Minassian, D.C.; Chisholm, I.H.; Bird, A.C. Bilateral macular drusen in age-related macular degeneration. Prognosis and risk factors. Ophthalmology 1994, 101, 1522–1528. [Google Scholar] [CrossRef]
- Soubrane, G.; Bressler, N.M. Treatment of subfoveal choroidal neovascularisation in age related macular degeneration: Focus on clinical application of verteporfin photodynamic therapy. Br. J. Ophthalmol. 2001, 85, 483–495. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, N.; Gerber, H.P.; LeCouter, J. The biology of vegf and its receptors. Nat. Med. 2003, 9, 669–676. [Google Scholar] [CrossRef]
- van Wijngaarden, P.; Coster, D.J.; Williams, K.A. Inhibitors of ocular neovascularization: Promises and potential problems. JAMA 2005, 293, 1509–1513. [Google Scholar] [CrossRef] [PubMed]
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandal, A.; Pal, D.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Mitra, A.K. Ocular delivery of proteins and peptides: Challenges and novel formulation approaches. Adv. Drug Deliv. Rev. 2018, 126, 67–95. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, V.M.; Chan, C.C. The role of anti-inflammatory agents in age-related macular degeneration (amd) treatment. Eye 2011, 25, 127–139. [Google Scholar] [CrossRef]
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; et al. Ophthalmic drug delivery systems for the treatment of retinal diseases: Basic research to clinical applications. Investig. Ophth. Vis. Sci. 2010, 51, 5403–5420. [Google Scholar] [CrossRef]
- Haller, J.A.; Bandello, F.; Belfort, R.; Blumenkranz, M.S.; Gillies, M.; Heier, J.; Loewenstein, A.; Yoon, Y.H.; Jiao, J.; Li, X.Y.; et al. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion. Ophthalmology 2011, 118, 2453–2460. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Brown, D.M.; Pearson, A.; Chen, S.; Boyer, D.; Ruiz-Moreno, J.; Garretson, B.; Gupta, A.; Hariprasad, S.M.; Bailey, C.; et al. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology 2012, 119, 2125–2132. [Google Scholar] [CrossRef]
- Herrero-Vanrell, R.; Bravo-Osuna, I.; Andres-Guerrero, V.; Vicario-de-la-Torre, M.; Molina-Martinez, I.T. The potential of using. Biodegradable microspheres in retinal diseases and other intraocular pathologies. Prog. Retin. Eye Res. 2014, 42, 27–43. [Google Scholar] [CrossRef]
- Prajapati, V.D.; Jani, G.K.; Kapadia, J.R. Current knowledge on biodegradable microspheres in drug delivery. Expert Opin. Drug Del. 2015, 12, 1283–1299. [Google Scholar] [CrossRef] [PubMed]
- Saishin, Y.; Silva, R.L.; Saishin, Y.; Callahan, K.; Schoch, C.; Ahlheim, M.; Lai, H.; Kane, F.; Brazzell, R.K.; Bodmer, D.; et al. Periocular injection of microspheres containing pkc412 inhibits choroidal neovascularization in a porcine model. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4989–4993. [Google Scholar] [CrossRef]
- Mietzner, R.; Kade, C.; Froemel, F.; Pauly, D.; Stamer, W.D.; Ohlmann, A.; Wegener, J.; Fuchshofer, R.; Breunig, M. Fasudil loaded plga microspheres as potential intravitreal depot formulation for glaucoma therapy. Pharmaceutics 2020, 12, 706. [Google Scholar] [CrossRef]
- Carrasquillo, K.G.; Ricker, J.A.; Rigas, I.K.; Miller, J.W.; Gragoudas, E.S.; Adamis, A.P. Controlled delivery of the anti-vegf aptamer eye001 with poly(lactic-co-glycolic)acid microspheres. Investig. Ophthalmol. Vis. Sci. 2003, 44, 290–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, A.K.; Dimberg, A.; Kreuger, J.; Claesson-Welsh, L. Vegf receptor signalling-in control of vascular function. Nat. Rev. Mol. Cell Biol. 2006, 7, 359–371. [Google Scholar] [CrossRef]
- Kang, H.; Ho, A.L.; Muzaffar, J.; Bowles, D.W.; Kim, S.B.; Ahn, M.J.; Hanna, G.J.; Worden, F.P.; Yun, T.; Norton, S.; et al. A phase ii open-label, multicenter, study to evaluate the efficacy and safety of rivoceranib in subjects with recurrent or metastatic adenoid cystic carcinoma. J. Clin. Oncol. 2020, 38, TPS6597. [Google Scholar] [CrossRef]
- Jeong, J.H.; Nguyen, H.K.; Lee, J.E.; Suh, W. Therapeutic effect of apatinib-loaded nanoparticles on diabetes-induced retinal vascular leakage. Int. J. Nanomed. 2016, 11, 3101–3109. [Google Scholar]
- Lee, J.E.; Kim, K.L.; Kim, D.; Yeo, Y.; Han, H.; Kim, M.G.; Kim, S.H.; Kim, H.; Jeong, J.H.; Suh, W. A patinib-loaded nanoparticles suppress vascular endothelial growth factor-induced angiogenesis and experimental corneal neovascularization. Int. J. Nanomed. 2017, 12, 4813–4822. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Goindi, S.; Saini, B.; Bansal, G. Thermal characterization and compatibility studies of itraconazole and excipients for development of solid lipid nanoparticles. J. Therm. Anal. Calorim. 2014, 115, 2375–2383. [Google Scholar] [CrossRef]
- Mohamed, A.I.; Abd-Motagaly, A.M.; Ahmed, O.A.; Amin, S.; Ali, A.I. Investigation of drug-polymer compatibility using chemometric-assisted uv-spectrophotometry. Pharmaceutics 2017, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Botha, S.A.; Lotter, A.P. Compatibility study between naproxen and tablet excipients using differential scanning calorimetry. Drug Dev. Ind. Pharm. 1990, 16, 673–683. [Google Scholar] [CrossRef]
- Qiao, M.X.; Chen, D.W.; Ma, X.C.; Liu, Y.J. Injectable biodegradable temperature-responsive plga-peg-plga copolymers: Synthesis and effect of copolymer composition on the drug release from the copolymer-based hydrogels. Int. J. Pharm. 2005, 294, 103–112. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, X.; Li, B.; Hou, Y.; Yang, J.; Yi, L. Development of a novel morphological paclitaxel-loaded plga microspheres for effective cancer therapy: In vitro and in vivo evaluations. Drug Deliv. 2018, 25, 166–177. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Palazzo, A.; Hennink, W.E.; Kok, R.J. Effect of particle size on drug loading and release kinetics of gefitinib-loaded plga microspheres. Mol. Pharm. 2017, 14, 459–467. [Google Scholar] [CrossRef]
- Gong, Y.; Li, J.; Sun, Y.; Fu, Z.; Liu, C.H.; Evans, L.; Tian, K.; Saba, N.; Fredrick, T.; Morss, P.; et al. Optimization of an image-guided laser-induced choroidal neovascularization model in mice. PLoS ONE 2015, 10, e0132643. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.L.; Suh, W. Apatinib, an inhibitor of vascular endothelial growth factor receptor 2, suppresses pathologic ocular neovascularization in mice. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3592–3599. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Polymer Molecular Weight (Mw) a | Polymer end Group | Emulsification Rate (rpm) | Drug Loading Content (%) | Encapsulation Efficiency (%) |
|---|---|---|---|---|---|
| 502−1.5k | 7000–17,000 | Hydroxyl | 1500 | 7.94 | 79.4 |
| 502−2.0k | 7000–17,000 | Hydroxyl | 2000 | 7.38 | 73.8 |
| 502H−1.5k | 7000–17,000 | Carboxyl | 1500 | 8.25 | 82.5 |
| 502H−2.0k | 7000–17,000 | Carboxyl | 2000 | 7.89 | 78.9 |
| 503H−1.5k | 24,000–38,000 | Carboxyl | 1500 | 7.80 | 78.0 |
| 503H−2.0k | 24,000–38,000 | Carboxyl | 2000 | 8.77 | 87.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.S.; Lee, M.S.; Jeong, H.; Lim, S.Y.; Kim, D.; Kim, D.; Jung, J.; Lyu, S.; Cho, H.J.; Kim, D.M.; et al. Sustained-Release Microspheres of Rivoceranib for the Treatment of Subfoveal Choroidal Neovascularization. Pharmaceutics 2021, 13, 1548. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13101548
Kim ES, Lee MS, Jeong H, Lim SY, Kim D, Kim D, Jung J, Lyu S, Cho HJ, Kim DM, et al. Sustained-Release Microspheres of Rivoceranib for the Treatment of Subfoveal Choroidal Neovascularization. Pharmaceutics. 2021; 13(10):1548. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13101548
Chicago/Turabian StyleKim, E Seul, Min Sang Lee, Hayoung Jeong, Su Yeon Lim, Doha Kim, Dahwun Kim, Jaeback Jung, Siyan Lyu, Hee Joo Cho, Dong Min Kim, and et al. 2021. "Sustained-Release Microspheres of Rivoceranib for the Treatment of Subfoveal Choroidal Neovascularization" Pharmaceutics 13, no. 10: 1548. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13101548