
Levodopa-Carbidopa Intestinal Gel in Advanced Parkinson’s Disease: Observations and Dilemmas after 10 Years of Real-Life Experience

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- What are the upper limits of conventional dopaminergic medication, especially LD doses (maximum daily dose or dosage intervals), without compromising patient/relative compliance, or how are these influenced by access to various add-on therapies or device-aided therapies?
- How long is it advisable to “insist” on available combination therapy options and what doses should be used in case of these treatments (the concept of “optimized medication”); also, in what way are these treatment options influenced by access (or lack of) to different device-aided therapy options?
- How can the severity and profile of various motor and non-motor complications be accurately assessed and what is their real impact on quality of life?
- How can one recognize the time when motor complications can no longer be controlled or ameliorated with standard oral/transdermal therapy (the concept of “medically refractory motor complications”)?
- What is the best time to start LCIG so that the benefits are maximized (predictability of clinical response and long-term safety)?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloemd, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tambasco, N.; Romoli, M.; Calabresi, P. Levodopa in Parkinson’s Disease: Current Status and Future Developments. Curr. Neuropharmacol. 2017, 16, 1239–1252. [Google Scholar] [CrossRef] [PubMed]
- Warren Olanow, C.; Kieburtz, K.; Rascol, O.; Poewe, W.; Schapira, A.H.; Emre, M.; Nissinen, H.; Leinonen, M.; Stocchi, F. Factors Predictive of the Development of Levodopa-Induced Dyskinesia and Wearing-off in Parkinson’s Disease. Mov. Disord. 2013, 28, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Ahlskog, J.E.; Muenter, M.D. Frequency of Levodopa-Related Dyskinesias and Motor Fluctuations as Estimated from the Cumulative Literature. Mov. Disord. 2001, 16, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Poewe, W.; Chaudhuri, K.R.; Jech, R.; Pickut, B.; Pirtošek, Z.; Szasz, J.; Valldeoriola, F.; Winkler, C.; Bergmann, L.; et al. Levodopa-Carbidopa Intestinal Gel in Advanced Parkinson’s: Final Results of the GLORIA Registry. Park. Relat. Disord. 2017, 45, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juhász, A.; Aschermann, Z.; Ács, P.; Janszky, J.; Kovács, M.; Makkos, A.; Harmat, M.; Tényi, D.; Karádi, K.; Komoly, S.; et al. Levodopa/Carbidopa Intestinal Gel Can Improve Both Motor and Non-Motor Experiences of Daily Living in Parkinson’s Disease: An Open-Label Study. Park. Relat. Disord. 2017, 37, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Băjenaru, O.; Ene, A.; Popescu, B.O.; Szász, J.A.; Sabău, M.; Mureşan, D.F.; Perju-Dumbrava, L.; Popescu, C.D.; Constantinescu, A.; Buraga, I.; et al. The Effect of Levodopa-Carbidopa Intestinal Gel Infusion Long-Term Therapy on Motor Complications in Advanced Parkinson’s Disease: A Multicenter Romanian Experience. J Neural Transm. 2016, 123, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Antonini, A.; Pahwa, R.; Odin, P.; Henriksen, T.; Soileau, M.J.; Rodriguez-Cruz, R.; Isaacson, S.H.; Merola, A.; Lindvall, S.; Domingos, J.; et al. Psychometric Properties of Clinical Indicators for Identification and Management of Advanced Parkinson’s Disease: Real-World Evidence From G7 Countries. Neurol. Ther. 2022, 11, 303–318. [Google Scholar] [CrossRef]
- Szász, J.A.; Constantin, V.A.; Orbán-Kis, K.; Rácz, A.; Arianabancu, L.; Georgescu, D.; Szederjesi, J.; Mihály, I.; Fárr, A.M.; Kelemen, K.; et al. Profile of Patients with Advanced Parkinson’s Disease Suitable for Device-Aided Therapies: Restrospective Data of a Large Cohort of Romanian Patients. Neuropsychiatr. Dis. Treat. 2019, 15, 3187–3195. [Google Scholar] [CrossRef] [Green Version]
- Szász, J.A.; Szatmári, S.; Constantin, V.; Mihály, I.; Rácz, A.; Frigy, A.; Nagy, E.; Kelemen, K.; Forró, T.; Almásy, E.; et al. Decision-Making and Duration to Accept Device-Aided Therapy in Advanced Parkinson’s Disease. Retrospective Data from an Eastern European Center with High Patient Turnover [Döntési Szempontok És Az Eszközös Terápia Elfogadásához Szükséges Idő Előrehaladott. Orv. Hetil. 2021, 162, 839–847. (In Hungarian) [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic Review of Levodopa Dose Equivalency Reporting in Parkinson’s Disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H.; Jenner, P. Etiology and Pathogenesis of Parkinson’s Disease. Mov. Disord. 2011, 26, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E.; Frigy, A.; Szász, J.; Horváth, E. Neuroinflammation and Microglia/Macrophage Phenotype Modulate the Molecular Background of Post-Stroke Depression: A Literature Review. Exp. Ther. Med. 2020, 20, 2510–2523. [Google Scholar] [CrossRef] [PubMed]
- Pirtošek, Z.; Bajenaru, O.; Kovács, N.; Milanov, I.; Relja, M.; Skorvanek, M. Update on the Management of Parkinson’s Disease for General Neurologists. Park. Dis. 2020, 2020, 9131474. [Google Scholar] [CrossRef]
- Grétarsdóttir, H.M.; Widman, E.; Johansson, A.; Nyholm, D. Personalized Medicine Approach in Treating Parkinson’s Disease, Using Oral Administration of Levodopa/Carbidopa Microtablets in Clinical Practice. J. Pers. Med. 2021, 11, 720. [Google Scholar] [CrossRef]
- Adamiak-Giera, U.; Jawień, W.; Pierzchlińska, A.; Białecka, M.; Kobierski, J.D.; Janus, T.; Gawrońska-Szklarz, B. Pharmacokinetics of Levodopa and 3-o-Methyldopa in Parkinsonian Patients Treated with Levodopa and Ropinirole and in Patients with Motor Complications. Pharmaceutics 2021, 13, 1395. [Google Scholar] [CrossRef]
- Silva, S.; Almeida, A.J.; Vale, N. Importance of Nanoparticles for the Delivery of Antiparkinsonian Drugs. Pharmaceutics 2021, 13, 508. [Google Scholar] [CrossRef]
- Fabbri, M.; Ferreira, J.J.; Lees, A.; Stocchi, F.; Poewe, W.; Tolosa, E.; Rascol, O. Opicapone for the Treatment of Parkinson’s Disease: A Review of a New Licensed Medicine. Mov. Disord. 2018, 33, 1528–1539. [Google Scholar] [CrossRef]
- Borgohain, R.; Szasz, J.; Stanzione, P.; Meshram, C.; Bhatt, M.; Chirilineau, D.; Stocchi, F.; Lucini, V.; Giuliani, R.; Forrest, E.; et al. Randomized Trial of Safinamide Add-on to Levodopa in Parkinson’s Disease with Motor Fluctuations. Mov. Disord. 2014, 29, 229–237. [Google Scholar] [CrossRef]
- Borgohain, R.; Szasz, J.; Stanzione, P.; Meshram, C.; Bhatt, M.H.; Chirilineau, D.; Stocchi, F.; Lucini, V.; Giuliani, R.; Forrest, E.; et al. Two-Year, Randomized, Controlled Study of Safinamide as Add-on to Levodopa in Mid to Late Parkinson’s Disease. Mov. Disord. 2014, 29, 1273–1280. [Google Scholar] [CrossRef]
- Rosca, E.C.; Tudor, R.; Cornea, A.; Simu, M. Parkinson’s Disease in Romania: A Scoping Review. Brain Sci. 2021, 11, 709. [Google Scholar] [CrossRef] [PubMed]
- Szasz, J.A.; Jianu, D.C.; Simu, M.A.; Constantin, V.A.; Dulamea, A.O.; Onuk, K.; Popescu, D.; Vasile, M.T.; Popescu, B.O.; Fasano, A.; et al. Characterizing Advanced Parkinson’s Disease: Romanian Subanalysis from the OBSERVE-PD Study. Park. Dis. 2021, 2021, 6635618. [Google Scholar] [CrossRef] [PubMed]
- Santos-Garcia, D.; Fernández Pajarín, G.; Oropesa-Ruiz, J.M.; Escamilla Sevilla, F.; Rahim López, R.R.A.; Muñoz Enríquez, J.G. Opicapone Improves Global Non-Motor Symptoms Burden in Parkinson’s Disease: An Open-Label Prospective Study. Brain Sci. 2022, 12, 383. [Google Scholar] [CrossRef] [PubMed]
- Kiss, T.; Katona, G.; Mérai, L.; Janovák, L.; Deák, Á.; Kozma, G.; Kónya, Z.; Ambrus, R. Development of a Hydrophobicity-Controlled Delivery System Containing Levodopa Methyl Ester Hydrochloride Loaded into a Mesoporous Silica. Pharmaceutics 2021, 13, 1039. [Google Scholar] [CrossRef]
- Szász, J.A.; Szatmári, S.; Constantin, V.; Mihály, I.; Rácz, A.; Török, I.; Nagy, E.; Kelemen, K.; Forró, T.; Baróti, B.; et al. The Importance of Evaluation of Gastrointestinal Symptoms in Advanced Parkinson’s Disease [A Gastrointestinalis Panaszok Felmérésének Jelentősége Előrehaladott Parkinson-Kórban]. Orv. Hetil. 2020, 161, 1681–1687. (In Hungarian) [Google Scholar] [CrossRef]
- Patel, A.B.; Jimenez-Shahed, J. Profile of Inhaled Levodopa and Its Potential in the Treatment of Parkinson’s Disease: Evidence to Date. Neuropsychiatr. Dis. Treat. 2018, 14, 2955–2964. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castrillo, J.C.; Martínez-Martín, P.; Burgos, Á.; Arroyo, G.; García, N.; Luquín, M.R.; Arbelo, J.M. Prevalence of Advanced Parkinson’s Disease in Patients Treated in the Hospitals of the Spanish National Healthcare System: The PARADISE Study. Brain Sci. 2021, 11, 1557. [Google Scholar] [CrossRef]
- Fasano, A.; Fung, V.S.C.; Lopiano, L.; Elibol, B.; Smolentseva, I.G.; Seppi, K.; Takáts, A.; Onuk, K.; Parra, J.C.; Bergmann, L.; et al. Characterizing Advanced Parkinson’s Disease: OBSERVE-PD Observational Study Results of 2615 Patients. BMC Neurol. 2019, 19, 50. [Google Scholar] [CrossRef] [Green Version]
- Pedrosa, D.J.; Gandor, F.; Jost, W.H.; Arlt, C.; Onuk, K.; Timmermann, L. Characterization of Advanced Parkinson ’ s Disease in Germany: Results of the Non - Interventional OBSERVE - PD Study. Neurol. Res. Pract. 2022, 4, 9. [Google Scholar] [CrossRef]
- Takáts, A.; Aschermann, Z.; Vécsei, L.; Klivényi, P.; Dézsi, L.; Zádori, D.; Valikovics, A.; Varannai, L.; Onuk, K.; Kinczel, B.; et al. Advanced Parkinson’s Disease Characteristics in Clinical Practice: Results from the Observe-Pd Study and Sub-Analysis of the Hungarian Data. Ideggyogy. Sz. 2020, 73, 261–268. [Google Scholar] [CrossRef]
- Szász, J.A.; Szatmári, S.; Constantin, V.; Mihály, I.; Rácz, A.; Domokos, L.C.; Vajda, T.; Orbán-Kis, K. Characteristics of Levodopa Treatment in Advanced Parkinson’s Disease in the Experiences of the Neurology Clinics of Târgu Mures, Romania [Az Orális Levodopakezelés Jellegzetességei Előrehaladott Parkinson-Kórban a Marosvásárhelyi Neurológiai Klinikák Tap. Orv. Hetil. 2019, 160, 662–669. (In Hungarian) [Google Scholar] [CrossRef] [PubMed]
- Odin, P.; Ray Chaudhuri, K.; Slevin, J.T.; Volkmann, J.; Dietrichs, E.; Martinez-Martin, P.; Krauss, J.K.; Henriksen, T.; Katzenschlager, R.; Antonini, A.; et al. Collective Physician Perspectives on Non-Oral Medication Approaches for the Management of Clinically Relevant Unresolved Issues in Parkinson’s Disease: Consensus from an International Survey and Discussion Program. Park. Relat. Disord. 2015, 21, 1133–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luquin, M.R.; Kulisevsky, J.; Martinez-Martin, P.; Mir, P.; Tolosa, E.S. Consensus on the Definition of Advanced Parkinson’s Disease: A Neurologists-Based Delphi Study (CEPA Study). Park. Dis. 2017, 2017, 4047392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini, A.; Stoessl, A.J.; Kleinman, L.S.; Skalicky, A.M.; Marshall, T.S.; Sail, K.R.; Onuk, K.; Odin, P.L.A. Developing Consensus among Movement Disorder Specialists on Clinical Indicators for Identification and Management of Advanced Parkinson’s Disease: A Multi-Country Delphi-Panel Approach. Curr. Med. Res. Opin. 2018, 34, 2063–2073. [Google Scholar] [CrossRef] [PubMed]
- Szász, J.A.; Szatmári, S.; Constantin, V.A.; Mihály, I.; Török, Á.; Frigy, A.; Metz, E.J.; Kelemen, K.; Szász, R.M.; Forró, T.; et al. Ten-Year Trends of the Characteristics in Patients with Advanced Parkinson’s Disease at the Time of Intestinal Gel Therapy Introduction [Az Intestinalis Gél Bevezetésekor Rögzített Jellemzők Tíz Éves Tendenciái Előrehaladott Parkinson-Kóros Betegeknél]. Orv. Hetil. 2022, in press. (In Hungarian) [Google Scholar] [CrossRef]
- Fasano, A.; Gurevich, T.; Jech, R.; Kovács, N.; Svenningsson, P.; Szász, J.; Parra, J.C.; Bergmann, L.; Johnson, A.; Sanchez-Soliño, O.; et al. Concomitant Medication Usage with Levodopa-Carbidopa Intestinal Gel: Results from the COSMOS Study. Mov. Disord. 2021, 36, 1853–1862. [Google Scholar] [CrossRef]
- Gandor, F.; Kübler, D.; Ebersbach, G.; Kühn, A.; Müller, J.; Klostermann, F.; Th, M.; Lipp, A. TEMP-Therapy Escalation in M. Parkinson-A German Regional Multicenter Survey. Austin J. Clin. Neurol. 2021, 8, 1154. [Google Scholar]
- Malek, N.; Grosset, D.G. Medication Adherence in Patients with Parkinson’s Disease. CNS Drugs 2014, 29, 47–53. [Google Scholar] [CrossRef]
- Szász, J.A.; Constantin, V.A.; Orbán-Kis, K.; Bancu, L.A.; Ciorba, M.; Mihály, I.; Nagy, E.E.; Szász, R.M.; Kelemen, K.; Simu, M.A.; et al. Management Challenges of Severe, Complex Dyskinesia. Data from a Large Cohort of Patients Treated with Levodopa-Carbidopa Intestinal Gel for Advanced Parkinson’s Disease. Brain Sci. 2021, 11, 826. [Google Scholar] [CrossRef]
- Ezat, B.; Pihlstrøm, L.; Aasly, J.; Tysnes, O.-B.; Egge, A.; Dietrichs, E. Use of Advanced Therapies for Parkinson’s Disease in Norway. Tidsskr. Nor. Laegeforen. 2017, 137, 619–623. [Google Scholar] [CrossRef]
- Lökk, J. Lack of Information and Access to Advanced Treatment for Parkinson’s Disease Patients. J. Multidiscip. Healthc. 2011, 4, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olanow, C.W.; Kieburtz, K.; Odin, P.; Espay, A.J.; Standaert, D.G.; Fernandez, H.H.; Vanagunas, A.; Othman, A.A.; Widnell, K.L.; Robieson, W.Z.; et al. Continuous Intrajejunal Infusion of Levodopa-Carbidopa Intestinal Gel for Patients with Advanced Parkinson’s Disease: A Randomised, Controlled, Double-Blind, Double-Dummy Study. Lancet Neurol. 2014, 13, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.D.; Bao, Y.; Liu, G.J. Comparison between Levodopa-Carbidopa Intestinal Gel Infusion and Subthalamic Nucleus Deep-Brain Stimulation for Advanced Parkinson’s Disease: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simu, M.A.; Jianu, D.C.; Dulamea, A.O.; Constantin, V.A.; Popescu, D.; Parra, J.C.; Szász, J.A. Advanced Parkinson’s Disease Treatment Simplification and Long-Term Outcomes with Levodopa Carbidopa Intestinal Gel: COSMOS Romanian Subanalysis. Brain Sci. 2021, 11, 1566. [Google Scholar] [CrossRef]
- Zadikoff, C.; Poewe, W.; Boyd, J.T.; Bergmann, L.; Ijacu, H.; Kukreja, P.; Robieson, W.Z.; Benesh, J.; Antonini, A. Safety of Levodopa-Carbidopa Intestinal Gel Treatment in Patients with Advanced Parkinson’s Disease Receiving ≥2000 Mg Daily Dose of Levodopa. Park. Dis. 2020, 2020, 9716317. [Google Scholar] [CrossRef]
- Slevin, J.T.; Fernandez, H.H.; Zadikoff, C.; Hall, C.; Eaton, S.; Dubow, J.; Chatamra, K.; Benesh, J. Long-Term Safety and Maintenance of Efficacy of Levodopa-Carbidopa Intestinal Gel: An Open-Label Extension of the Double-Blind Pivotal Study in Advanced Parkinson’s Disease Patients. J. Park. Dis. 2015, 5, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Constantin, V.A.; Szász, J.A.; Orbán-Kis, K.; Rosca, E.C.; Popovici, M.; Cornea, A.; Bancu, L.A.; Ciorba, M.; Mihály, I.; Nagy, E.; et al. Levodopa-Carbidopa Intestinal Gel Infusion Therapy Discontinuation: A Ten-Year Retrospective Analysis of 204 Treated Patients. Neuropsychiatr. Dis. Treat. 2020, 16, 1835–1844. [Google Scholar] [CrossRef]
- Szász, J.A.; Orbán-Kis, K.; Constantin, V.A.; Péter, C.; Bíró, I.; Mihály, I.; Szegedi, K.; Balla, A.; Szatmári, S. Therapeutic Strategies in the Early Stages of Parkinson’s Disease: A Cross-Sectional Evaluation of 15 Years’ Experience with a Large Cohort of Romanian Patients. Neuropsychiatr. Dis. Treat. 2019, 15, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Szász, J.; Constantin, V.; Fazakas, P.; Blényesi, E.; Grieb, L.; Balla, A.; Sárig, M.; Szegedi, K.; Bartha, E.; Sz, S. The Role of Selective Monoamine Oxidase B Inhibitors in the Therapeutic Strategy of Parkinson’s Disease in the Neurology Clinics of Tirgu Mures County Emergency Clinical Hospital [A Szelektív Monoaminoxidáz-B-Gátlók Helye a Parkinson-Kór Kezelési Stratégi. Orv. Hetil. 2017, 158, 2023–2028. (In Hungarian) [Google Scholar] [CrossRef]
- Szász, J.A.; Constantin, V.; Mihály, I.; Biró, I.; Péter, C.; Orbán-Kis, K.; Szatmári, S. Dopamine Agonists in Parkinson’s Disease Therapy-15 Years of Experience of the Neurological Clinics from Tirgu Mures. A Cross-Sectional Study [A Dopaminagonisták Jelentősége a Parkinson-Kór Kezelésében a Marosvásárhelyi Ideggyógyászati Klinikák 15 Éves. Ideggyogy. Sz. 2019, 72, 187–193. (In Hungarian) [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Motor Complications | n% | Duration (Hours, Mean ± SD) |
|---|---|---|
| off periods | 150 (100%) | 4.73 ± 1.08 |
| peak dose dyskinesia | 95 (63.3%) | 2.96 ± 0.84 |
| diphasic dyskinesia | 44 (29.33%) | 3 ± 0.82 |
| early morning akinesia | 132 (88%) | |
| delayed on | 90 (60%) | |
| no on | 35 (23.33%) | |
| sudden off | 58 (38.67%) | |
| freezing | 81 (54%) |
| Add-on Therapy | n% | Dose (mg/Day, Mean ± SD) |
|---|---|---|
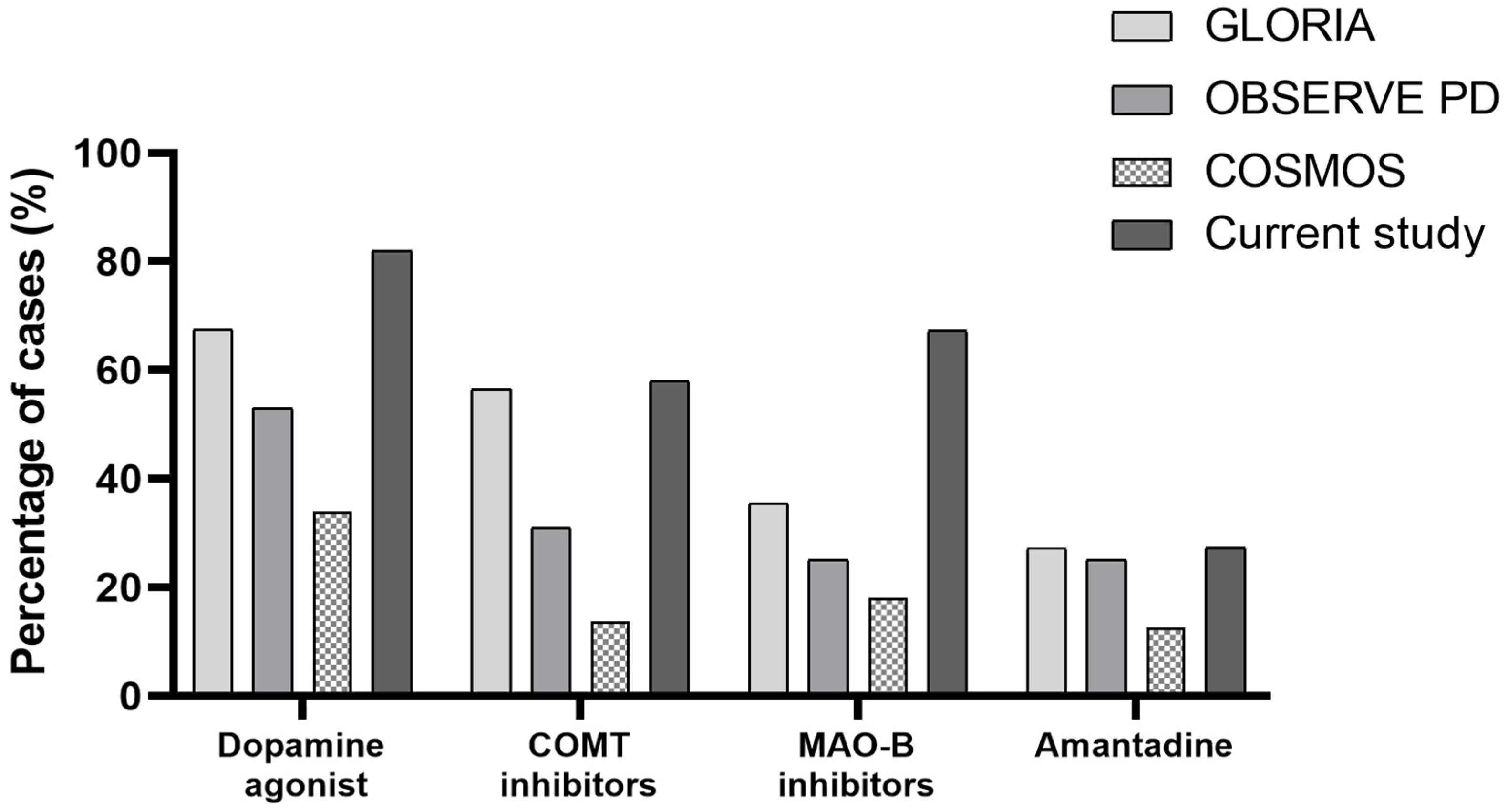
| Dopamin agonist | 123 (82%) | |
| Pramipexol | 42 | 2.25 ± 0.60 |
| Ropinirol | 33 | 13.45 ± 4.98 |
| Rotigotine | 51 | 8.16 ± 2.93 |
| MAO-Bi (n,%) | 101 (67.33%) | |
| COMTi (n,%) | 87 (58%) | |
| Amantadine (n,%) | 41 (27.33%) |
| Before PEG-J | After PEG-J | |
|---|---|---|
| N = 150 | N = 150 | |
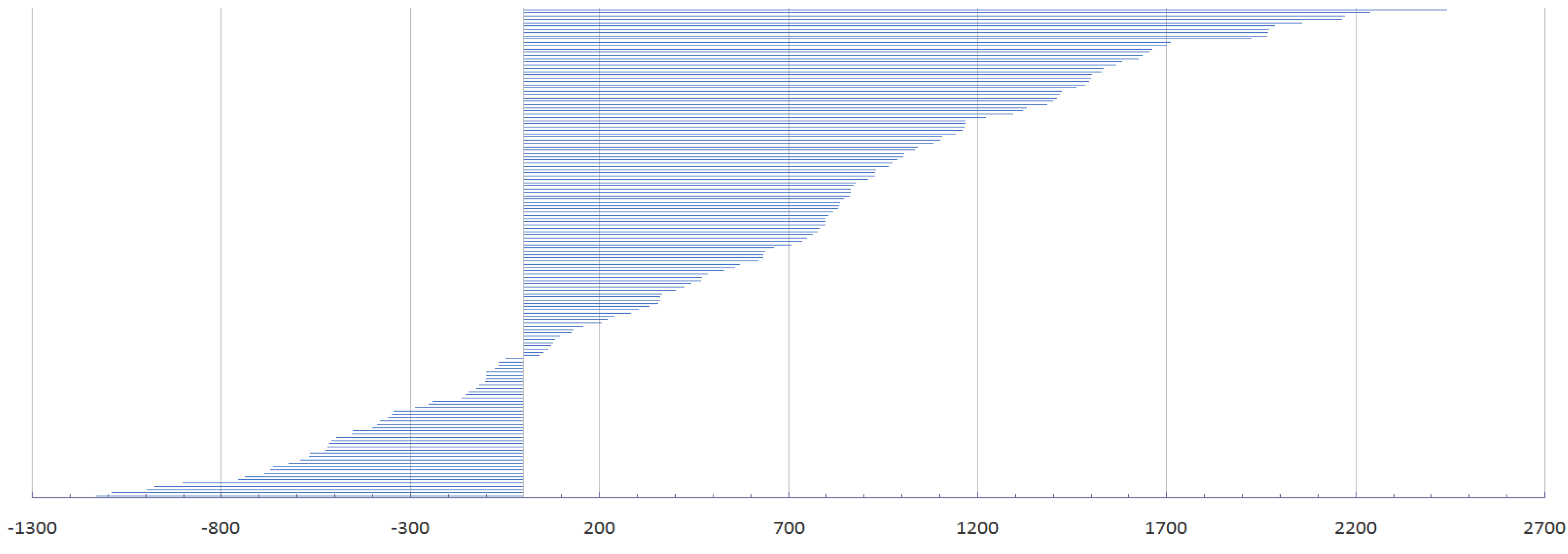
| LD /LCIG dose (mean ± SD) | 854.16 ± 258.15 mg | 1877 ± 769 mg |
| Hoehn and Yahr scale (Mean ± SD) | ||
| on state | 3.23 ± 0.42 | 2.96 ± 0.2 |
| off state | 4.39 ± 0.50 | 3.82 ± 0.4 |
| PGI-I (mean ± SD) | -- | 1.7 ± 0.55 |
| Very much improved (n) | 52 | |
| Much improved (n) | 91 | |
| Minimally improved (n) | 7 | |
| No change (n) | 0 | |
| Minimally worse (n) | 0 |
| Characteristics of LCIG Administration | |
|---|---|
| Titration days (mean ± SD) | 6 ± 1 days |
| LCIG calculated (mean ± SD) | 1309 ± 321 mg |
| LCIG real (mean ± SD) | 1877 ± 769 mg |
| LCIG infusion administration | |
| Mean ± SD | 19.8 ± 3.6 h/day |
| median | 18 h/day |
| duration of LCIG administration (hrs/day) | n |
| 16 h | 53 |
| 18 h | 35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szász, J.A.; Constantin, V.A.; Orbán-Kis, K.; Bancu, L.A.; Bataga, S.M.; Ciorba, M.; Nagy, E.; Neagoe, M.R.; Mihály, I.; Szász, R.M.; et al. Levodopa-Carbidopa Intestinal Gel in Advanced Parkinson’s Disease: Observations and Dilemmas after 10 Years of Real-Life Experience. Pharmaceutics 2022, 14, 1115. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061115
Szász JA, Constantin VA, Orbán-Kis K, Bancu LA, Bataga SM, Ciorba M, Nagy E, Neagoe MR, Mihály I, Szász RM, et al. Levodopa-Carbidopa Intestinal Gel in Advanced Parkinson’s Disease: Observations and Dilemmas after 10 Years of Real-Life Experience. Pharmaceutics. 2022; 14(6):1115. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061115
Chicago/Turabian StyleSzász, József Attila, Viorelia Adelina Constantin, Károly Orbán-Kis, Ligia Ariana Bancu, Simona Maria Bataga, Marius Ciorba, Előd Nagy, Mircea Radu Neagoe, István Mihály, Róbert Máté Szász, and et al. 2022. "Levodopa-Carbidopa Intestinal Gel in Advanced Parkinson’s Disease: Observations and Dilemmas after 10 Years of Real-Life Experience" Pharmaceutics 14, no. 6: 1115. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061115