M Mode Ultrasound and Tissue Doppler Imaging to Assess Diaphragm Feature in Late Onset Pompe Disease


1
Intensive Care Unit and Home Mechanical Ventilation Unit, Raymond Poincaré Hospital, APHP, 92380 Garches, France
2
Cardiology Unit, Paris Saclay University, Raymond Poincaré Hospital, APHP, 92380 Garches, France
*
Author to whom correspondence should be addressed.
Neurol. Int. 2020, 12(3), 55-58; https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint12030012
Submission received: 20 January 2020
/
Accepted: 10 February 2020
/
Published: 13 November 2020
{kind=link}
{kind=link}
Abstract
:Late-onset Pompe disease (LOPD) is an autosomal recessive lysosomal storage disease. Clinical features include skeletal muscle deficiency and diaphragm weakness. Clinical management relies on supportive treatment and mechanical ventilation in patients with chronic respiratory failure. M mode ultrasound and sniff tissue Doppler imaging can be used to assess and follow diaphragm function.
1. Introduction
Late-onset Pompe disease (LOPD) is an autosomal recessive lysosomal storage disease. This disease is related to a defect in the activity of the glycogen degrading lysosomal enzyme, the alpha 1–4 glucosidase enzyme (GAA), causing glycogen accumulation and muscle weakness [1]. Clinical features include skeletal muscle deficiency and diaphragm weakness. Clinical management relies on supportive treatment that includes enzyme replacement therapy and mechanical ventilation. Respiratory muscle monitoring is essential in this disease, since respiratory insufficiency and sleep disordered breathing are frequent in patients with LOPD and an important cause of morbidity [2,3]. Diaphragm, the main inspiratory muscle, has a crucial role in breathing during sleep. Diaphragm weakness is often associated with sleep-disordered breathing. Recently, ultrasound has been used to assess diaphragm weakness in LOPD [4]. Here, using M mode ultrasound and tissue Doppler imaging (TDI) [5], we report diaphragm weakness attested by a paradoxical motion during a sniff test in a patient with LOPD. The study was performed in compliance with the ethical principles formulated in the declaration of Helsinki and was approved by the French regulatory board (CNIL, commission nationale de l’informatique et des libertés). Informed consent was obtained from the patient for this case report.
2. Case Report
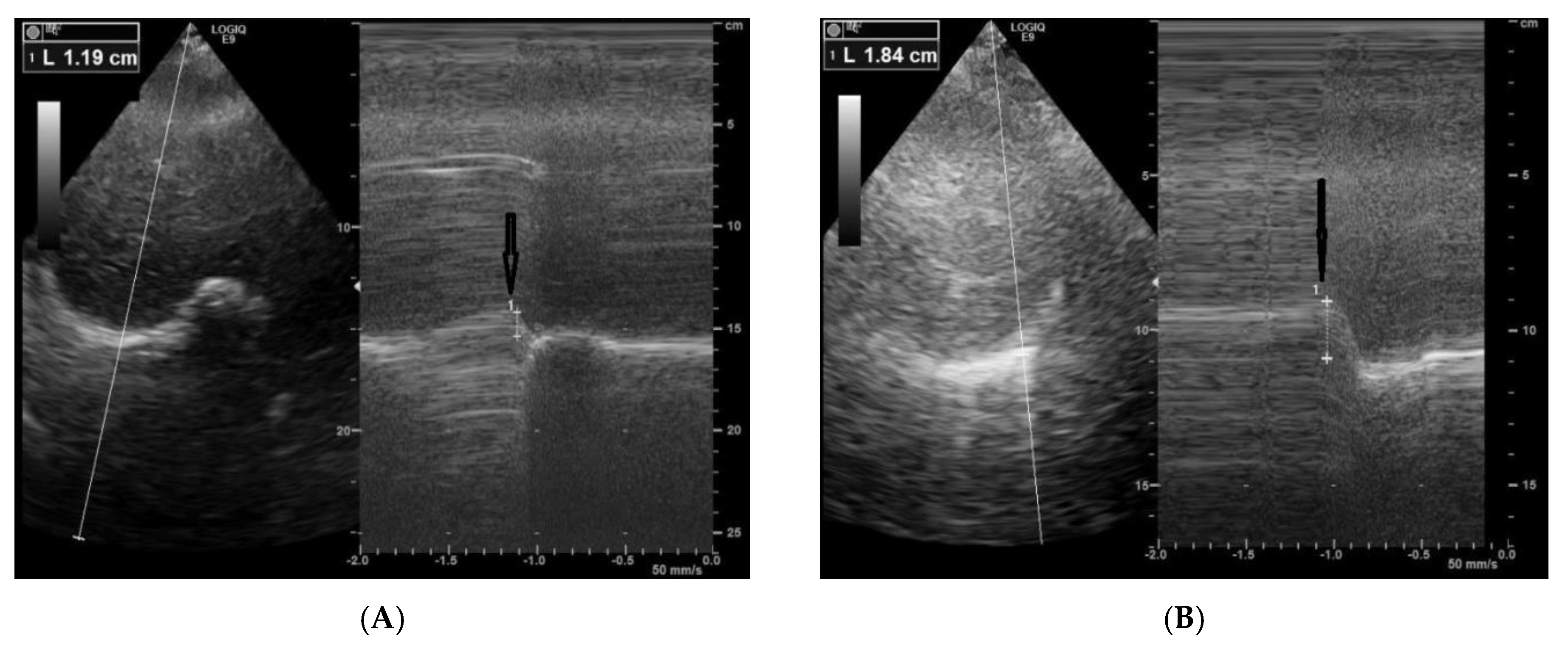
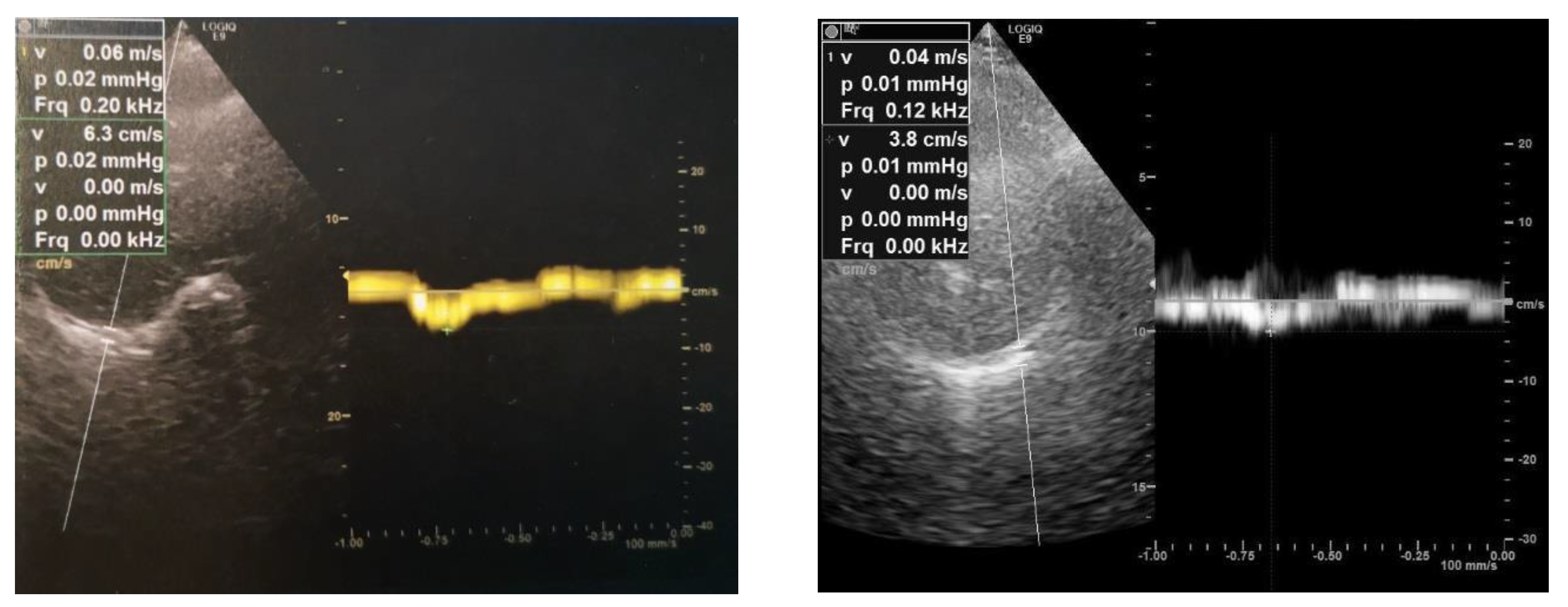
A 64-year-old female patient was referred to our unit for a cardiorespiratory evaluation because of dyspnea and orthopnea. She was treated with enzyme replacement therapy for 10 years because of LOPD. She had limb girdle weakness with waddling gait. The Walton score was 3. The other clinical parameters were as follows: body mass index at 26 kg/m2, systolic blood pressure at 109 mmHg, diastolic blood pressure at 65 mmHg, and diurnal oxygen transcutaneous saturation at 100%. Doppler Echocardiography showed a normal left ventricular ejection fraction (61%) with normal cardiac loading and subnormal systolic arterial pulmonary pressure (41 mmHg). We performed a diaphragm exploration using ultrasound in the same exam. From the subcostal view, we assessed the diaphragm motion using TM mode in rest and during a sniff maneuver, as previously described [5]. We found a paradoxical diaphragm motion during a sniff maneuver of both the right (−11 mm) and the left hemi diaphragm (−18 mm), with M mode (Figure 1). Using tissue Doppler imaging, we also found a negative and reduced peak velocity of diaphragm during the sniff maneuver, measured on the right hemi diaphragm (−6 cm/s) and on the left hemi diaphragm (−4 cm/s) (Figure 2). Diaphragm weakness was confirmed by the decrease in maximal inspiratory pressure (22 cm H2O), the decrease in sniff inspiratory pressure (29 cm H2O) and the drop in the predicted value of respiratory forced vital capacity (VC) from upright to supine position (from 43% to 27%). In the meantime, with transcutaneous capnometry, the patient disclosed nocturnal hypoventilation attested by an increase in the transcutaneous PCO2 (82% of the registration time with PCO2 > 50 mmHg) and a decrease in transcutaneous PO2 (39% of time with PO2 < 90%). Non-invasive nocturnal ventilation was introduced to manage the respiratory failure.
3. Discussions
We report this case, in which bedside diaphragm evaluation by ultrasound suggested diaphragm weakness with nocturnal hypoventilation as the cause of dyspnea and orthopnea, in a patient with LOPD. In LOPD, clinically relevant diaphragm weakness may develop even in patients with little peripheral muscular impairment, causing nocturnal hypoventilation, supine dyspnea aggravation, daytime hypercapnia, fatigue and excessive daytime sleepiness [3]. Diaphragm weakness is often associated with limb girdle weakness [6]. NIV has been shown to normalize gas exchange and improve respiratory status and symptoms in this context [1,7]. Respiratory involvement in LOPD can be subtle and it is essential to monitor patients with repeated respiratory function tests, measuring vital capacity, maximal inspiratory pressure, and maximal expiratory pressure. The disease can affect not only the diaphragm, but also the upper airways and the other respiratory muscles [1]. Classically, the drop in the VC from upright to supine is an indirect marker of diaphragmatic weakness [8]. To assess the inspiratory muscle strength, sniff inspiratory nasal pressure and maximal inspiratory mouth pressure can be used. Sniff maneuver coupled with ultrasound can be used to selectively assess diaphragm function [5,9]. Regular respiratory function monitoring is crucial in LOPD. In fact, LOPD patients with a supine VC < 60% of predicted value frequently have sleep-disordered breathing, and nocturnal hypoventilation is frequent when VC is below 40% [10]. M mode ultrasound and Tissue Doppler imaging may be applied in patients with LOPD to assess and monitor the diaphragm function, with the advantage of being applicable at the bedside, without the need for lung function facilities. In this case report, the paradoxical motion and the negative velocity of the diaphragm during the sniff manoeuver gave the necessary clues to further investigate respiratory function, allowing the depiction of the presence of nocturnal hypoventilation. This finding highlights the potential application of ultrasound to monitor diaphragm in LOPD. Current guidelines recommend introducing noninvasive ventilation in patients with LOPD relying on the values of blood gas exchange, MIP, FCV and sleep studies. Future studies will be necessary to assess the additive value of diaphragm ultrasound in this field.
4. Conclusions
In LOPD, bedside ultrasound may be used to screen for diaphragmatic dysfunction. In the presence of a diaphragm paradoxical motion or a negative TDI velocity during a sniff maneuver, nocturnal transcutaneous capnometry should be performed.
Author Contributions
P.M. and A.F. conceived and wrote the manuscript. A.O. analyzed the results and added substantial scientific modifications. A.F. drafted the final version. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mellies, U.; Lofaso, F. Pompe disease: A neuromuscular disease with respiratory muscle involvement. Respir. Med. 2009, 103, 477–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boentert, M.; Dräger, B.; Glatz, C.; Young, P. Sleep-Disordered Breathing and Effects of Noninvasive Ventilation in Patients with Late-Onset Pompe Disease. J. Clin. Sleep Med. 2016, 12, 1623–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boentert, M.; Karabul, N.; Wenninger, S.; Stubbe-Dräger, B.; Mengel, E.; Schoser, B.; Young, P. Sleep-related symptoms and sleep-disordered breathing in adult Pompe disease. Eur. J. Neurol. 2015, 22, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Spiesshoefer, J.; Henke, C.; Kabitz, H.J.; Brix, T.; Görlich, D.; Herkenrath, S.; Randerath, W.; Young, P.; Boentert, M. The nature of respiratory muscle weakness in patients with late-onset Pompe disease. Neuromuscul. Disord. 2019, 29, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Fayssoil, A.; Nguyen, L.S.; Ogna, A.; Stojkovic, T.; Meng, P.; Mompoint, D.; Carlier, R.; Prigent, H.; Clair, B.; Behin, A.; et al. Diaphragm sniff ultrasound: Normal values, relationship with sniff nasal pressure and accuracy for predicting respiratory involvement in patients with neuromuscular disorders. PLoS ONE 2019, 14, e0214288. [Google Scholar] [CrossRef] [PubMed]
- Van der Beek, N.A.M.E.; van Capelle, C.I.; van der Velden-van Etten, K.I.; Hop, W.C.J.; van den Berg, B.; Reuser, A.J.J.; van Doorn, P.A.; van der Ploeg, A.T.; Stam, H. Rate of progression and predictive factors for pulmonary outcome in children and adults with Pompe disease. Mol. Genet. Metab. 2011, 104, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Mellies, U.; Stehling, F.; Dohna-Schwake, C.; Ragette, R.; Teschler, H.; Voit, T. Respiratory failure in Pompe disease: Treatment with noninvasive ventilation. Neurology 2005, 64, 1465–1467. [Google Scholar] [CrossRef] [PubMed]
- Fromageot, C.; Lofaso, F.; Annane, D.; Falaize, L.; Lejaille, M.; Clair, B.; Gajdos, P.; Raphaël, J.C. Supine fall in lung volumes in the assessment of diaphragmatic weakness in neuromuscular disorders. Arch. Phys. Med. Rehabil. 2001, 82, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Iandelli, I.; Gorini, M.; Misuri, G.; Gigliotti, F.; Rosi, E.; Duranti, R.; Scano, G. Assessing inspiratory muscle strength in patients with neurologic and neuromuscular diseases: Comparative evaluation of two noninvasive techniques. Chest 2001, 119, 1108–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishnani, P.S.; Steiner, R.D.; Bali, D.; Berger, K.; Byrne, B.J.; Case, L.E.; Crowley, J.F.; Downs, S.; Howell, R.R.; Kravitz, R.M.; et al. Pompe disease diagnosis and management guideline. Genet. Med. 2006, 8, 267–288. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
(A) (−11 mm) and (B) (−18 mm) hemi diaphragm paradoxical displacement using M mode ultrasound during a sniff maneuver in patient with LOPD.
Figure 1.
(A) (−11 mm) and (B) (−18 mm) hemi diaphragm paradoxical displacement using M mode ultrasound during a sniff maneuver in patient with LOPD.

Figure 2.
Diaphragm right peak negative velocity (−6 cm/s) and left peak negative velocity (−4 cm/s) using tissue Doppler imaging coupled to a sniff maneuver in patient with LOPD.
Figure 2.
Diaphragm right peak negative velocity (−6 cm/s) and left peak negative velocity (−4 cm/s) using tissue Doppler imaging coupled to a sniff maneuver in patient with LOPD.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Meng, P.; Ogna, A.; Fayssoil, A. M Mode Ultrasound and Tissue Doppler Imaging to Assess Diaphragm Feature in Late Onset Pompe Disease. Neurol. Int. 2020, 12, 55-58. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint12030012
AMA Style
Meng P, Ogna A, Fayssoil A. M Mode Ultrasound and Tissue Doppler Imaging to Assess Diaphragm Feature in Late Onset Pompe Disease. Neurology International. 2020; 12(3):55-58. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint12030012
Chicago/Turabian StyleMeng, Paris, Adam Ogna, and Abdallah Fayssoil. 2020. "M Mode Ultrasound and Tissue Doppler Imaging to Assess Diaphragm Feature in Late Onset Pompe Disease" Neurology International 12, no. 3: 55-58. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint12030012