Impacts of Music Intervention on Dementia: A Review Using Meta-Narrative Method and Agenda for Future Research


Abstract
:
1. Introduction
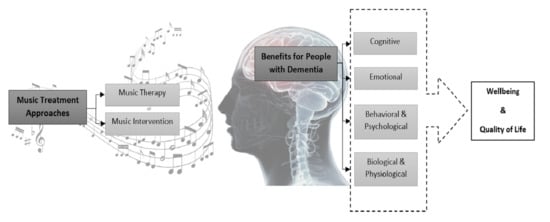
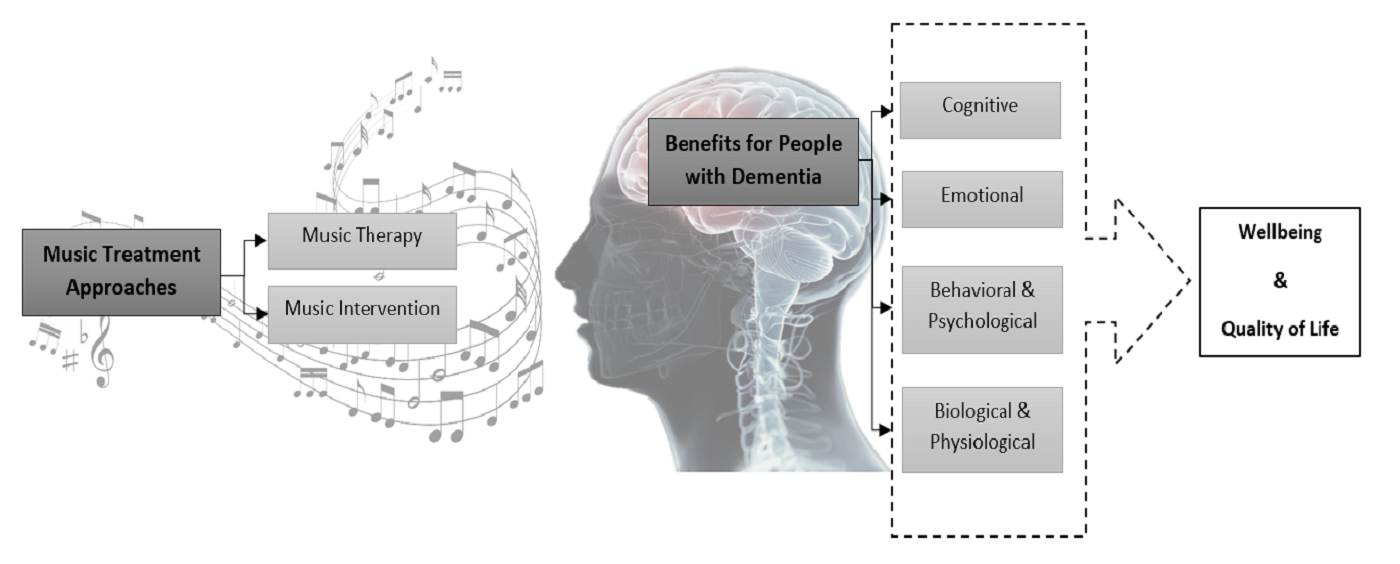
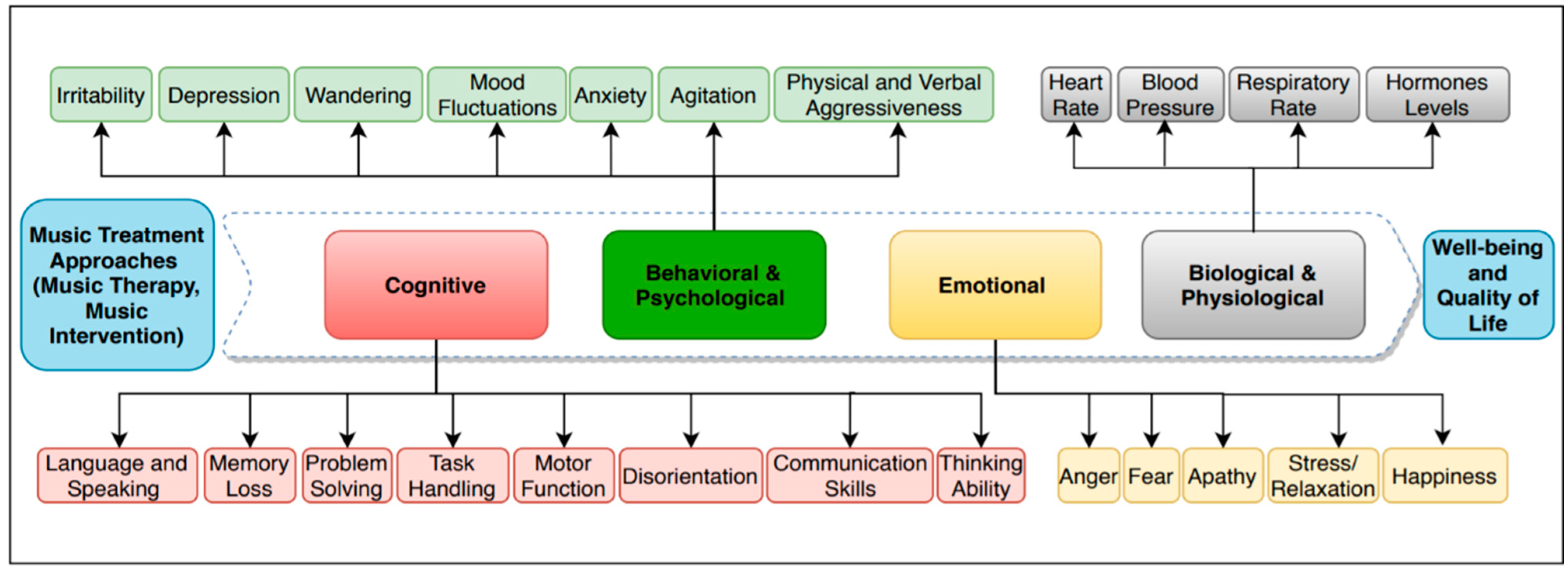
Benefits of Music Treatment for People Living with Dementia
- Cognitive: Music also boosts communication skills, the quality of life, well-being, intimacy, memory, self and environmental awareness, the ability to distinguish between the surroundings and moments of the day, and managing pain [17,22,23]. Among all music advantages, some of the most important ones are enhancement in language skills, verbal and non-verbal expressions, improvement of social activity and communication, raising cognitive levels, and self-awareness [19,24]. PWD who have verbal communication problems can benefit from music as a non-verbal communication solution to express themselves without inhibitions.
- Emotional: Music engages the individual’s attention (apathy) and helps them enjoy their life, improves their self-esteem, and communication, which leads to improvement in behavior [25]. People living with dementia who listened to their favorite music were observed to have a decrease in stress level and an increase in relaxation and happiness [26].
2. Materials and Methods
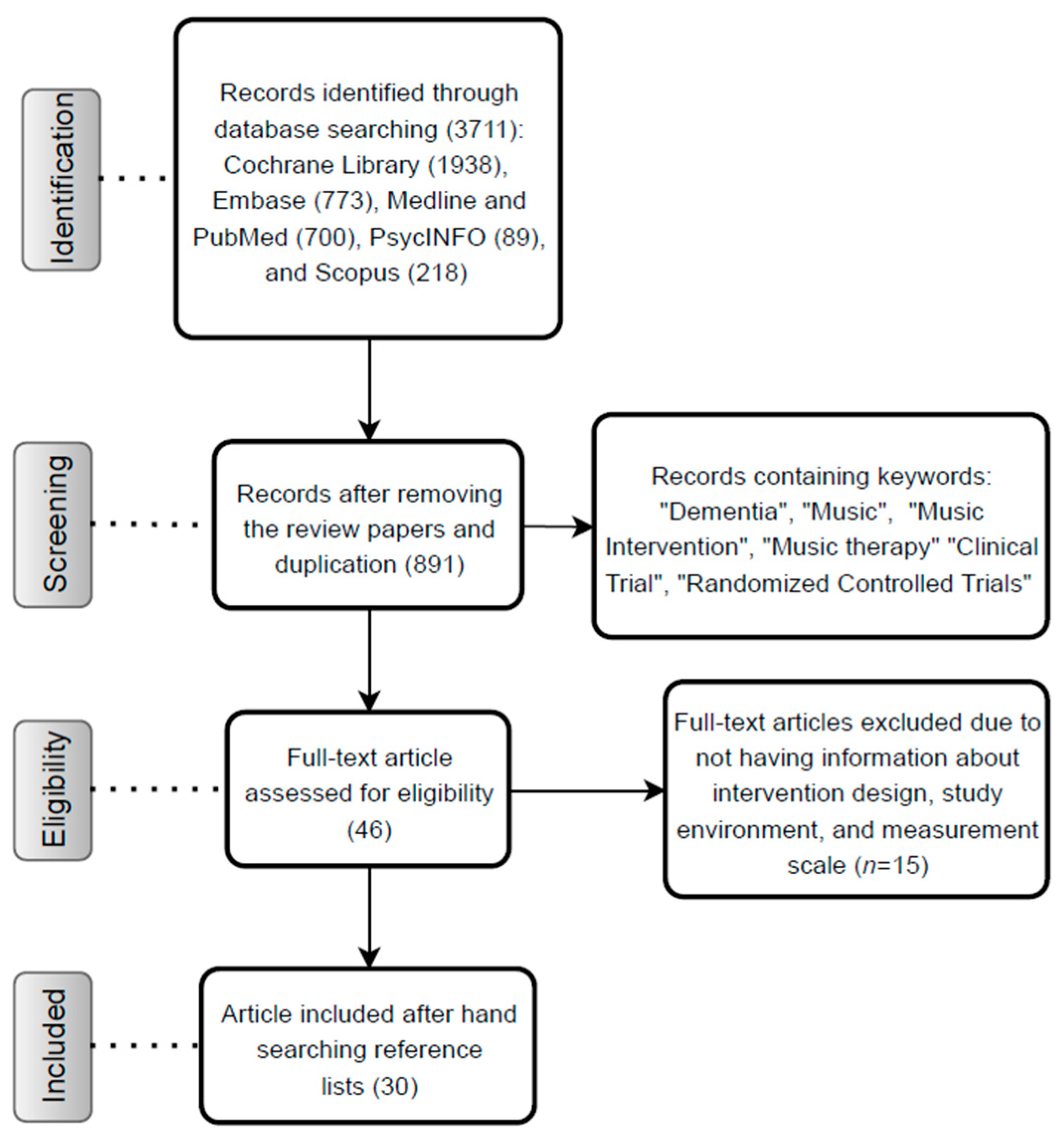
Search Strategy and Selection Criteria
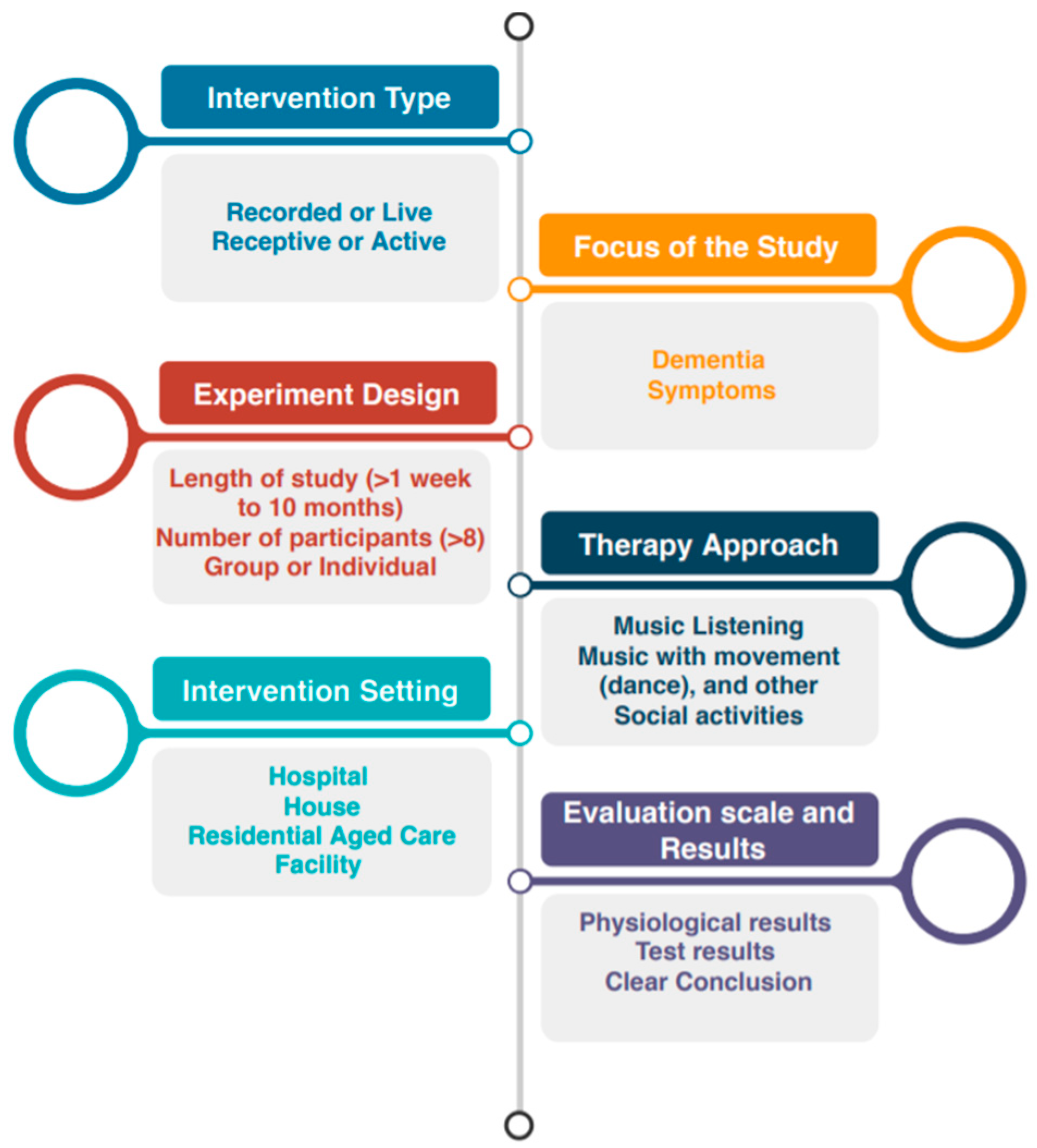
- Intervention type
- The focus of the study
- Experiment design
- Therapy approach
- Intervention setting
- Evaluation scales and results (Figure 2)
3. Data Extraction and Quality Assessment
4. Results
5. Gaps in the Research
- Control group: To compare individuals living with dementia who experience music treatment and others who only receive pharmacological treatment or are involved in other activities, it is necessary to divide people with dementia into two groups: a control group or a study group. Although sixteen papers out of 30 [18,29,30,34,38,50,51,52,53,54,55,56,57,58,59,60] included both groups in their studies, some studies did not have a control group in their experiments [21,26,28,33,61,62,63,64,65,66,67,68,69]. For example, in two studies [54,55] with both control and study groups, a greater behavioral disturbance was noticed between the study group than the control group. Additionally, in another paper [69] with only a study group, no changes was noted in memory. Thus, it is hard to conclude that music is an effective treatment for dementia, especially in the absence of a control group when there is a discrepancy between the results.
- Gender: Although researchers have included different genders (females and males) in their study, only one of the studies identified music’s impact based on gender [61]. In this study, individuals listened to unfamiliar childhood songs or a spoken version of visual stimuli, but no significant difference was observed between genders. Therefore, further cross-sectional studies are needed to determine if gender has any effect.
- Sample size: The sample size of the studies varied from eight to 165 participants. In several studies, the sample size of the experiment was less than ten [28,58,61,70]. For example, one research analyzed the behavior of nine PWD who received music therapy [28], where expressing more positive emotions and improvement in their well-being and communication level were observed. However, two studies [55,69] included a larger population (120 and 59, respectively) in their research, but did not find any significant changes in PWD symptoms. Hence, it is not clear that music caused changes in the level of dementia symptoms because of the use of a smaller sample size.
- Long-term effect: Some studies have found that music had a short-term impact, but it is unclear if music can be beneficial in the long-term. Only two studies reported long-term [28,34], one study reported short-term [50], and one study reported both short- and long-term effects of music [50]. In one study conducted in a residential age care facility [56], residents were divided into three groups doing activities such as music-movement, music listening, and social activities for 12 weeks. The residents’ agitation levels were monitored and compared before, during, and after involvement with the activities. Short-term change in the agitation level of those who were engaged with music-movement activity was noted. In contrast, no changes in agitation level of the residents in other groups were observed. Additionally, in another study conducted for 14 weeks, no statistically significant differences were observed in the memory of the residents [69]. As a result, more high-quality longitudinal studies are needed to monitor the benefits of music in dementia over a period of time, particularly in the long-term.
- Live or recorded music: Music intervention sessions are conducted either as a recorded [18,21,26,28,38,50,54,60,62,66,67,69] or live music [57] based on individual’s preference, or recorded [29,52,53,56,59,61,65] or live music [63] selected by caregivers, while some other studies have employed music therapy sessions either as a recorded music based on the individual’s preference [18,26], recorded [34,51,58,68], or live music [33,70] selected by music therapist. Five studies observed that listening to live music and being engaged with the singer and/or singing the song and/or playing musical instruments boosted the general well-being, mood, quality of life, and PWD’s relationships with others [33,57,63,67,70]. However, in some papers, changes in the health status of individuals living with dementia were observed while listening to recorded music [38,41,52,54,65], which implies no apparent differences in the reviewed studies between playing live or recorded music. Emotions connected to music might change the moods of people living with dementia. Further cross-sectional studies using a control group are required to determine if the music transferring method has any effect.
- Music intervention or music therapy: Researchers have sometimes mixed the definition of music intervention (music medicine) with music therapy and considered any types of music treatment as music therapy. Among the 30 reviewed studies, only nine of them considered music therapy [18,30,33,34,58,64,68,70] and the remaining investigated music intervention. Music therapy was examined either as an active therapy in individual [58,68,70] or group [30,33,34] modes, or receptive group therapy [18,64]. Music intervention is considered either as active [18,29,55,56,57,59,67], receptive [21,38,52,54,60,61,62,63,64,65,69], or both receptive and active modes [28,50]. Although most of the music therapy studies have reported positive changes in the individuals’ symptoms, in one study, no changes in wandering behavior were reported [33]. While more positive responses in emotional states, behavioral and psychological symptoms of dementia (BPSD), and cognition of individual’s living with dementia was reported using active and perceptive music intervention [28,50], researchers did not talk about the differences between active and perceptive modes. Studies that applied only one music transferring method had mixed results, and it is hard to conclude which approach worked better. More studies need to be conducted in order to understand which approach is more effective for dementia treatment.
- Selecting appropriate music and professional therapists: The music treatment approach aims to decrease the costs, and it is not obvious that it is necessary to hire professional music therapists to conduct music sessions, or medical personnel can conduct the therapy session. While some researchers have tried to use PWD’s favorite song [26,38,41,54,56,62,64] played by musicians, singers, music therapists, or trained caregivers (who are taught by a music therapist to conduct the music sessions) [18,33,50,54,57,58,61,63], others chose random songs performed by caregivers or facility staff [30,64,70]. This variation and inconsistency in the delivery of music make it hard to generalize the results. Therefore, further research on performing music with professional music therapists or facility staff is needed. Furthermore, perhaps music should be chosen based on the individual’s preference by asking their family members or conducting a survey to determine which type of music has a more restorative impact on PWD.
- Physiological impact: In addition to changes in psychological data, dementia may cause changes in physiological signals. One study [17] found that music is a beneficial modality to balance vital signs such as blood pressure, heart rate, and respiratory rate. Most of the studies focused on the psychological data and ignored physiological signals. Two studies used wearable sensors to measure physiological signals [58,71]. In one study [71], the impact of music therapy was examined on 12 elderly people with vascular dementia using an Electrocardiogram (ECG) sensor. They noted an increment in heart rate variability (HRV) features such as mean values of inter beat interval (RR), Root Mean Square of the Successive Differences (RMSSD), proportion of NN50 (pNN50), and high frequency band during the music therapy session and a decrease in values of HRV features after the sessions. The drawback of focusing on the statistical analysis of the observed or neurological data is that the collected data in these studies dealt with mostly subjective data rather than taking into consideration the physiological and psychological data that was gathered using wearable sensors, which can capture more accurate changes in physiological and psychological symptoms. Thus, it is impossible to reach an overall conclusion that music can improve PWD’s physiological signals.
- Lack of an exact measurement scale: Although most of the studies employed quantitative measurement mechanisms that used clinical scales, some researchers did not apply any particular measurement scale. Some researchers have monitored changes in PWD’s moods and behavior by observing and analyzing their body or facial expressions [41,57,65], or reviewed self-reported surveys or caregiver notes [53,63,70]. It is difficult to objectively assess the impact of complex multimodal intervention such as music. It seems that using some physiological measures such as heart rate, blood pressure, skin conductance, measuring stress hormones, and analyzing the brain signals would be beneficial to provide us with more reliable measures.
- Combination of music with pharmacological methods: One study [20] pointed out that applying non-pharmacological treatments like music intervention or therapy and pharmacological treatment could mitigate symptoms of anxiety and depression in people with mild dementia, while it is unclear that observing all the changes in individual situations was only due to the addition of music to their treatment or combining music with pharmacological solutions. Therefore, further studies with a control group are necessary to explore whether control variables such as pharmacological treatments affect dementia symptoms.
- Combination of music with other activities: Although some studies have proved that listening to music and being involved with social activities positively impact dementia symptoms, only nine studies combined various activities such as playing games, solving word-puzzles, gardening, and engaging in mental or physical activities [18,29,34,52,56,57,59,60,68]. These studies have shown that combining social activities with music intervention or therapy can improve or postpone dementia symptoms. Additionally, individuals who engaged in social activities demonstrated improvement in communication skills [22]. Several researchers applied music and playing games to reduce agitation, aggression, apathy, and anxiety levels, enhance communication skills, and improve emotional expressions [34]. In another study [60], PWD were divided into three groups engaged in either social activity, listening to music, or music with dance. It was concluded that the combination of music with dance could improve cognitive function, memory, and depressive symptoms while there was no significant changes in agitation among the three groups. In one study [18], short-term reduction in agitation behaviors of PWD was reported while doing either social activities or listen to music played by a music therapist. Researchers incorporated 77 PWD in their study and compared changes in their behavior while listening to the music, singing along to the song and dancing, or doing daily recreational activities such as handwork, solving a puzzle, and cooking designed by the occupational therapists. These outcomes indicated that keeping PWD occupied with functional tasks might help with declining dementia symptoms. These studies are useful, but since they do not study music treatment approach in isolation, it is not apparent that music or other social activities improve their psychological symptoms. To have more reliable and valid results, there should be more studies examining the combined effect of music with other activities involving individuals in both activities during a period of time and observing their behaviors for each type of activity.
- Impact on agitation, wandering, and cognition: The impact of music treatment on the agitation, wandering, and cognition of individuals with moderate or severe dementia is not completely clear. While seven out of 30 studies discussed a reduction in agitation [29,33,34,52,55,57,65], others reported no change in agitation. For example, in one study, no changes were noticed on wandering and agitation [33]. Another study [59] did not find any differences in the individuals’ cognition levels. Thus, more studies are required to investigate the impacts of music on agitation, wandering, and cognition.
- Benefits of music for family members and caregivers: In one study, it was mentioned that music therapy could also increase caregivers’ satisfaction [26]. The impact of music was examined on eight PWD and their caregivers while professional music therapists taught caregivers to play PWD‘s favorite music by themselves at home. The comparison between the data revealed a decrease in the stress level and an increase in both groups’ relaxation and happiness. However, more studies like these should be conducted to determine music’s impact on family members and caregivers.
6. Discussion and Conclusions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Outcome Focus Area | Dementia Alzheimer’s | Intervention Details & Measurement Frequency | No. Participants Control Group (CG)/ Music Therapy (MT) | Study Environment & Conductor | Measurement Method/Results |
|---|---|---|---|---|---|---|
| Moore, 2010 [52] | Apathy, agitation, and appetite | Early to severe Dementia | 3 weeks (25 min, 30 min before lunchtime), twice a week) Recorded familiar music or physical activity (Seated chair exercise and music listening) Music intervention Pre, Post data | 84 (MT and CG) | Residential aged care facility Research assistant | Measurement scales: Frontal systems behavior scale, Cohen–Mansfield Agitation Inventory (CMAI) Results: Significant changes in apathy and dietary intake but no change in agitation or eating ability |
| Raglio et al., 2010 [51] | Behavioral Symptoms | Severe Dementia | 4 weeks (3 sessions in a month, for 30 min, One-month washout) Music therapy Group MT (3 people in a group) | 60 (30: MT, 30: CG) | Residential aged care facility Facility staffs | Measurement scales: Mini-Mental State Examination (MMSE), Barthel Index and Neuropsychiatry Inventory (NPI) Results: A decline in behavioral disorder, improve in delusion, agitation, and apathy |
| Sung et al., 2010 [38] | Anxiety | Dementia | 6 weeks (30 min twice a week) Recorded preferred music Music intervention Pre, End of each week data | 52 (29: MT, 23: CG) | Residential aged care facility Facility staffs | Measurement scale: Rating Anxiety in Dementia (RAID) Result: Lower levels of anxiety |
| Cook et al., 2010 [57] | QOL and Depression | Dementia | 12 weeks (30 min for 3 times in a week) Active, personalized, live music, Reading activity Music intervention Pre, During, Post data | 47 (reading and music groups) | Residential aged care facility Musicians | Measurement scales: Evaluation of Dementia Quality Life (DQOL), Geriatric Depression Scale (GDS) Results: A higher level of midpoint QOL, increase in self-esteem and decrease in depression level |
| Lin et al., 2010 [29] | Agitation | Dementia | 12 MT(Twice a week, 30 min MT for 6 weeks) Group MT, active (rhythmical music and slow-tempo instrumental activities, singing, listening, glockenspiel, musical activities and traditional holidays, music creator) Music intervention Pre, Middle, End, one month after MT data | 100 (49: MT, 51: CG) | Residential aged care facility Facility staffs | Measurement scales: CMAI, Generalized Estimating Equations (GEFs) Results: Reduction in agitation and physical aggressive behavior after beginning MT, reduction in verbal aggressive behaviors only in the middle of MT |
| Stern et al., 2010 [61] | Recognition Ability | Alzheimer’s | 30 min Unfamiliar childhood songs, song lyric or spoken version visual stimuli Music intervention During data | 27 (13: Alzheimer’s, 14: Healthy) | Residential aged care Trained Musician | Measurement scales: ANOVA memory test Results: No differences between genders, healthy individuals had better recognition ability than patients with Alzheimer’s |
| Ho et al., 2011 [65] | Behavior | Dementia | 4 weeks (Twice a day, during meal time) Recorded calming music Music intervention Pre, Post | 22 (M: 10, F: 12) | Hospital-based residential aged care facility Researcher | Measurement scale: CMAI Result: Decline in agitation |
| Nair et al., 2011 [53] | Physical aggressiveness, Verbal abuse, Agitation, wandering and Inappropriate sexual advances | Dementia | 4 weeks (for 4 h) Recorded and Baroque Music Music intervention Pre (2 weeks), During (4 weeks), Post (2 weeks) | 75 (MT and CG) | Residential aged care facility Facility staffs | Measurement scale: Behavior observation Results: Listening to Baroque music has a negative effect on patient behaviors, a more behavioral disturbance was observed between experimental groups than the control group. |
| Hanser et al., 2011 [26] | Mood and Psychological State | Dementia | 8–20 sessions Favorite music Music therapy Pre, During, Post data | 8 | Residential aged care facility Caregiver | Measurement scale: Visual Analog Scale (VAS) Results: Both patients and caregivers have a higher level of relaxation, happiness, and comfort after MT |
| Terworth & Probst, 2011 [34] | Behavioral and Psychological Symptoms | Mild to Moderate Dementia | 6 months Group MT (6–10 patients), active(singing, playing an elementary musical instrument, listening to biography of music and Playing game (word-association, puzzle)) Music therapy Pre, Post data | 49 (MT: 26 (M: 3, F: 23), CG: 23 (M: 3, F: 20)) | Residential aged care facility Caregivers | Measurement scales: Mini-Mental Status Test (MMST), Global Deterioration Scale Neuropsychiatric Inventory (NPI), GDS, Inventory to Assess Communication, Emotional Expression and Activity in Dementia (ICEA-D) Results: Reduction in agitation, aggression, apathy, and anxiety beside an improvement in communication, emotional expression |
| Janata, 2012 [54] | Agitation and Depression | Moderate and Severe Dementia | 12 weeks (3 h for several times in a day) Recorded and Customized music (Widespread and frequent personalized music) Music intervention Pre, Post data | 38 (25: F, 13: M,19: MT, 19: CG) | Residential aged care facility Music therapist | Measurement scales: CMAI, NPI, Cornell Scale for Depression in Dementia (CSDD), MMSE Results: Reduction in agitation and depression level of patients |
| Vink et al., 2012 [18] | Agitation | Dementia | 4 months (40 min twice a week) Group MT, favorite music or recreational activities Music therapy Daily, Post data | 77 (43: MT, 34: Recreational activities) | Residential aged care facility Trained music therapist | Measurement scales: CMAI Results: Decline in agitation level during listening to music but after music intervention agitation comes back |
| Vleuten et al., 2012 [63] | Quality of life, Communication skills and mental well-being | Mild and Severe Dementia | 45 min (one or a few songs) Intimate live music Group therapy (10 patients in each group) Music intervention Post data | 45 | Residential aged care facility Professional singers | Measurement scales: Behavior observation Results: Improvement in human contact, communication skills, observing more positive emotions and less negative emotion |
| Baker et al., 2012 [66] | Anxiety, Depression, Spousal Relationship | Dementia | 6 weeks (20–30 min 3 sessions per week) Active, familiar/preferred/quiet music Music intervention Pre, post data | 5 couples (M: 2, F: 3) | Home Caregivers | Measurement scales: GDS, Geriatric Anxiety Inventory (GAI), Mutual Communal Behaviors Scale (MCBS), Positive Aspects of Caregiving Questionnaire (PACQ), NPI Results: Improve spouse relationship, satisfaction, enjoyment, and well-being of caregiver, and boost the mood of couples |
| Sakamoto et al., 2013 [50] | Behavioral and Psychological Symptoms | Advanced Dementia | 10 weeks (30 min for once a week) Passive/active, preferred music Music intervention Pre, During, Post data | 39 (3 groups: CG (F: 11, M: 2), passive (F:10, M:3), active (F:11, M:2)) | Residential aged care and Dementia hospital Music facilitator | Measurement scales: Nerve Index and Faces Scale behavioral, Behavioral Pathology in Alzheimer’s Disease (BEHAVE-AD), Heart rate (HR) Results: Improve in emotional states (Both short and long term), more improve in BPSD among active MT group |
| Park, 2013 [62] | Agitation | Dementia | 4 session (30 min twice a week before peeking of agitation) Favorite music Music intervention Pre, During, Post data | 26 | Residential aged care facility Facility staffs | Measurement scale: CMAI Results: Decline in agitation level while listening to music but after music intervention agitation comes back |
| Gold, 2014 [70] | Mood and Behavior | Advanced Dementia | 4 months (once in a week) Active, Live music Music therapy 4 days after each MT session, End of MT sessions | 9 | Hospital Researcher | Measurement scales: Caregiver notes (observation) Result: 8 out of 9 patients showed positive changes |
| Chu et al., 2014 [30] | Depression and Cognition | Dementia | 12 sessions (30 min twice a week) Group therapy, active Music therapy Pre, Middle, End, Post data | 104 (MT, CG) | Residential aged care facility Facility staffs | Measurement scales: Chinese Version of C-CSDD and Salivary Cortisol, The Chinese version of the MMSE for measuring cognitive function Results: Reduction in depression level, improvement in cognitive function |
| Eggert et al., 2015 [64] | Behavioral Changes | Alzheimer’s Dementia | image and music: 1–4 weeks, wash out:4 weeks, image and music:4 weeks (1.5 h per week) Group therapy Music intervention Pre, Post data | 24 | Residential aged care facility Facility staffs | Measurement scales: Individualize Dementia Engagement and Activities Scale tool, Montreal Cognitive Assessment, CMAI Results: Reducing the behavioral disorder |
| Raglio et al., 2014 [17] | Behavioral and Psychological Symptoms (Depression, Anxiety, Apathy, and Cognitive) | Moderate to Severe Dementia | 10 week (20 music 30 min twice a week) Active, individualized music Music intervention Pre, Post data | 120 (3 groups, CG, MT, and Individualized listening to music) | Residential aged care facility Facility staffs | Measurement scales: NPI, CSDD Results: No significant changes in behavioral and psychological symptoms |
| Schall et al., 2015 [28] | communication behavior and emotional well-being | Advanced Dementia | 20 sessions for 6 months (3 cycles of music for 23–39 min) Active/passive, individual video graphed music Music intervention Pre, During, Post data | 9 | Home Caregivers | Measurement scales: NPI, The CODEM instrument for assessing communication behavior, The Positive Response Schedule for Severe Dementia (PRS) for assessing well-being, The Observed Emotion Rating Scale (OERS) for rating positive and negative emotions, Results: Improvement in communication skills, well-being, and expressing more positive emotions |
| Hsu et al., 2015 [58] | Well-being Dementia symptoms | Dementia | 5 months (30 min music once a week) Active, well-known songs Music therapy Pre, During, End, Post data | 17 (MT, CG) | Residential aged care facility Music therapist | Measurement scales: NPI for Nursing Homes for measuring Dementia symptoms, Dementia Care Mapping (DCM) for the well-being Results: Physiological data heart rate and skin conductance, skin temperature and bodily acceleration, Decrease in NPI for MT and increase in NPI for CG after 5 months, Improvement in the well-being of MT and decline in the control group, Improve in the interaction between patients and caregivers |
| Ray and Mittelman, 2017 [33] | Agitation, wandering and Depression | Moderate and severe Dementia | 15 min–60 min Preferred music, live, active group therapy (4–6 patients) Music therapy Pre, During, Post data (each for 2 weeks) | 132 (F: 112, M: 20) | Residential aged care facility Music therapist | Measurement scales: ANOVA Results: A decrease in agitation and depression, no change in wandering |
| Melhuish et al., 2017 [68] | QOL | Semantic and frontotemporal Dementia | 50–60 min once a week Active (music from the 1920s to 1960s), Dance/Movement Music therapy | 24 (M:12, F:18) (15: Moderate Dementia, 12: Advanced Dementia) | Residential aged care facility caregivers | Measurement scales: Interpretative phenomenological analysis (IPA) Results: Help caregivers to discover patients’ skills and feeling, improve the connection between caregivers and patients |
| Tang et al., 2018 [59] | Apathy, Cognition | Dementia | 12 weeks (50 min for 3 times in a week) Active, group therapy, playing a musical instrument, nostalgic music (nostalgic red songs, nostalgic nursery rhymes, and nostalgic Cantonese opera) Music intervention | 77 (M: 39, F: 38, 39:CG, 38: MT) | Residential aged care facility Research assistant | Measurement scales: Apathy Evaluation Scale (AES), Mini-Mental State Examination (MMSE) Results: Decrease in apathy, no changes in cognition |
| Garrido et al., 2018 [21] | Psychological and Behavioral Symptoms (Depression, Anxiety, Apathy, and Cognitive) | Dementia | ~30 min (2 min baseline 1–2 playlist (contain 2–4 song) each 8–9 min, 2–3 min between each playlist) Recorded personalized/preferred music (belong to 1930s–1970s) Music intervention Pre, During data | 99 | Residential aged care facility Facility staffs | Measurement scales: Activation of facial action (webcam Observed Emotion Rating), OERC Results: People with high levels of depression and with symptoms of Alzheimer’s type of Dementia demonstrated increased levels of sadness, People with low depression but high levels of apathy demonstrated the highest behavioral evidence of pleasure during music listening, although behavioral evidence declined with the severity of cognitive impairment |
| Cheung et al., 2018 [56] | Cognitive Functions, Depression, and Anxiety | Moderate Dementia | 12 weeks 3 activities (music-with-movement(MM), intervention music listening(IML), and social activity(SA)) Music intervention Pre, Middle, End data | 165 (3 groups; MM: 54, IML: 58, SA: 53) | Residential aged care facility Facility staffs | Measurement scales: Mixed multivariate analysis of variance (MANOVA), RAID scale for measuring anxiety, GDS, MMSE, Fuld’s Object Memory Evaluation (FOME), Modified Fuld Verbal Fluency Test (MVFT), Digit Span Test (DST) for measuring adult intelligence Results: Improvements in memory and depressive symptoms |
| Gulliver et al., 2019 [67] | Well-being, QOL, Mental Health (Depression) | Alzheimer’s Dementia | 40–60 min for 8 weeks Music engagement program based on patients age, culture, and preference Music engagement program Pre, Post data | 19 | Residential aged care facility Facility staffs | Measurement scales: Visual Analogue Survey (VAS) based on WONCA diagram for Feeling and Social Activities, Cornell Scale for Depression in Dementia and quality of life through measuring factors of mood-related signs Result: Improvement in well-being and mental health |
| Cheung et al., 2020 [60] | Agitation | Moderate Dementia | 6 weeks (45 min twice a week) 3 activities (music with movement(MM), music listening(ML), social activity(SA)), preferred music Music intervention Pre, Post data | 165 (3 groups: MM, ML, SA) | Residential aged care facility Facility staffs | Measurement scales: A Chinese version of the CMAI Results: No statistically significant changes in agitation among the three groups, only short-term impact during the MT |
| Kwak et al., 2020 [69] | Agitation, Cognition | Dementia/Alzheimer’s | 14 weeks Preferred recorded music Music intervention Pre, During, and Post data | 59 | Residential aged care facility Facility staffs | Measurement scales: CMAI, NPI-NH Result: No statistically significant changes in memory |
References
- World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Prasad, D. The Impact of Music Therapy on the Cognitive, Behavioural and Psychological Symptoms of Dementia: A Literature Review; Arts and Sciences Program Level IV; McMaster University: Hamilton, ON, Canada, 2019. [Google Scholar]
- Sabanovic, S.; Bennett, C.C.; Chang, W.-L.; Huber, L. PARO robot affects diverse interaction modalities in group sensory therapy for older adults with dementia. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–6. [Google Scholar]
- Lai, N.M.; Chang, S.M.W.; Ng, S.S.; Tan, S.L.; Chaiyakunapruk, N.; Stanaway, F. Animal-assisted therapy for Dementia. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; O’Philbin, L.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for Dementia. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrester, L.T.; Maayan, N.; Orrell, M.; Spector, A.E.; Buchan, L.D.; Soares-Weiser, K. Aromatherapy for Dementia. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamae, T.; Yotsumoto, K.; Tatsumi, E.; Hashimoto, T. Effects of Productive Activities with Reminiscence in Occupational Therapy for People with Dementia: A Pilot Randomized Controlled Study. Hong Kong J. Occup. Ther. 2014, 24, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Wang, Y.; Wang, Z. The effectiveness of massage and touch on behavioural and psychological symptoms of dementia: A quantitative systematic review and meta-analysis. J. Adv. Nurs. 2017, 73, 2283–2295. [Google Scholar] [CrossRef]
- Mitchell, G.; O’Donnell, H. The therapeutic use of doll therapy in dementia. Br. J. Nurs. 2013, 22, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Forbes, D.A.; Blake, C.M.; Thiessen, E.J.; Peacock, S.; Hawranik, P. Light therapy for improving cognition, activities of daily living, sleep, challenging behaviour, and psychiatric disturbances in dementia. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh, S.R.; Holmes, J.; Cardno, A. Art therapy for people with dementia. Cochrane Database Syst. Rev. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Bradt, J.; Dileo, C. Music interventions for mechanically ventilated patients. Cochrane Database Syst. Rev. 2014, 2014. [Google Scholar] [CrossRef]
- Available online: https://www.musictherapy.org/about/musictherapy/ (accessed on 18 October 2020).
- Fang, R.; Ye, S.; Huangfu, J.; Calimag, D.P. Music therapy is a potential intervention for cognition of Alzheimer’s Disease: A mini-review. Transl. Neurodegener. 2017, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Abrams, B.; Wigram, T.; Pedersen, I.N.; Bonde, L.O. (2002). A comprehensive guide to music therapy: Theory, clinical practice, research and training. London: Jessica Kingsley. 384 pages. ISBN 1-84310-083-5. Music. Ther. Perspect. 2003, 21, 51–52. [Google Scholar] [CrossRef]
- Devere, R. Music and Dementia: An overview. Pract. Neurol. 2017, 16, 32–35. [Google Scholar]
- Raglio, A.; Filippi, S.; Bellandi, D.; Stramba-Badiale, M. Global music approach to persons with dementia: Evidence and practice. Clin. Interv. Aging 2014, 9, 1669–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vink, A.; Zuidersma, M.; Boersma, F.; De Jonge, P.; Zuidema, S.U.; Slaets, J.P.J. The effect of music therapy compared with general recreational activities in reducing agitation in people with dementia: A randomised controlled trial. Int. J. Geriatr. Psychiatry 2012, 28, 1031–1038. [Google Scholar] [CrossRef]
- Blackburn, R.; Bradshaw, T. Music therapy for service users with dementia: A critical review of the literature. J. Psychiatr. Ment. Heal. Nurs. 2014, 21, 879–888. [Google Scholar] [CrossRef]
- Petrovsky, D.; Cacchione, P.Z.; George, M. Review of the effect of music interventions on symptoms of anxiety and depression in older adults with mild dementia. Int. Psychogeriatr. 2015, 27, 1661–1670. [Google Scholar] [CrossRef]
- Garrido, S.; Dunne, L.; Chang, E.; Perz, J.; Stevens, C.J.; Haertsch, M. The Use of Music Playlists for People with Dementia: A Critical Synthesis. J. Alzheimer’s Dis. 2017, 60, 1129–1142. [Google Scholar] [CrossRef] [Green Version]
- Beard, R.L. Art therapies and Dementia care: A systematic review. Dementia 2011, 11, 633–656. [Google Scholar] [CrossRef]
- King, J.B.; Jones, K.G.; Goldberg, E.; Rollins, M.; MacNamee, K.; Moffit, C.; Naidu, S.R.; Ferguson, M.A.; Garcia-Leavitt, E.; Amaro, J.; et al. Increased Functional Connectivity After Listening to Favored Music in Adults with Alzheimer’s Dementia. J. Prev. Alzheimer’s Dis. JPAD 2019, 6, 56–62. [Google Scholar]
- McDermott, O.; Crellin, N.; Ridder, H.M.O.; Orrell, M. Music therapy in dementia: A narrative synthesis systematic review. Int. J. Geriatr. Psychiatry 2013, 28, 781–794. [Google Scholar] [CrossRef]
- Chancellor, B.; Duncan, A.; Chatterjee, A. Art Therapy for Alzheimer’s Disease and Other Dementias. J. Alzheimer’s Dis. 2014, 39, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanser, S.B.; Butterfield-Whitcomb, J.; Kawata, M.; Collins, B.E. Home-based music strategies with individuals who have dementia and their family caregivers. J. Music. Ther. 2011, 48, 2–27. [Google Scholar] [CrossRef] [PubMed]
- Tomaino, C.M. Meeting the Complex Needs of Individuals With Dementia Through Music Therapy. Music. Med. 2013, 5, 234–241. [Google Scholar] [CrossRef]
- Schall, A.; Haberstroh, J.; Pantel, J. Time Series Analysis of Individual Music Therapy in Dementia Effects on Communication Behavior and EmotionalWell-Being. GeroPsych 2015, 28, 113–122. [Google Scholar] [CrossRef]
- Lin, Y.; Chu, H.; Yang, C.Y.; Chen, C.H.; Chen, S.G.; Chang, H.J.; Chou, K.R. Effectiveness of group music intervention against agitated behaviour in elderly persons with Dementia. Int. J. Geriatr. Psychiatry 2011, 26, 670–678. [Google Scholar] [CrossRef]
- Chu, H.; Yang, C.Y.; Lin, Y.; Ou, K.L.; Lee, T.Y.; O’Brien, A.P.; Chou, K.R. The Impact of Group Music Therapy on Depression and Cognition in Elderly Persons with Dementia: A Randomized Controlled Study. Biol. Res. Nurs. 2014, 16, 209–217. [Google Scholar] [CrossRef]
- Tuckett, A.G.; Hodgkinson, B.; Rouillon, L.; Balil-Lozoya, T.; Parker, D. What carers and family said about music therapy on behaviours of older people with dementia in residential aged care. Int. J. Older People Nurs. 2015, 10, 146–157. [Google Scholar] [CrossRef]
- Matthews, S. Dementia and the Power of Music Therapy. Bioethics 2015, 29, 573–579. [Google Scholar] [CrossRef]
- Ray, K.; Mittelman, M.S. Music therapy: A nonpharmacological approach to the care of agitation and depressive symptoms for nursing home residents with dementia. Dementia 2015, 16, 689–710. [Google Scholar] [CrossRef]
- Fischer-Terworth, C.; Probst, P. Evaluation of a TEACCH- and Music Therapy-Based Psychological Intervention in Mild to Moderate Dementia a Controlled Trial. GeroPsych 2011, 24, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Vinoo, D.; Santos, J.M.; Leviyev, M.; Quimbo, P.; Dizon, J.; Diaz, F.; Wittman, C.; Dulgheru, I.; Hughes, R.; Matias, L.; et al. Music and Memory in Dementia Care. Int. J. Neurorehabilit. 2017, 4. [Google Scholar] [CrossRef]
- Aleixo, M.A.R.; Santos, R.L.; Dourado, M.C.D.N. Efficacy of music therapy in the neuropsychiatric symptoms of dementia: Systematic review. J. Bras. Psiquiatr. 2017, 66, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-S.; Chu, H.; Yang, C.-Y.; Tsai, J.-C.; Chung, M.-H.; Liao, Y.-M.; Chi, M.-J.; Liu, M.F.; Chou, K.-R. The efficacy of music therapy for people with dementia: A meta-analysis of randomised controlled trials. J. Clin. Nurs. 2015, 24, 3425–3440. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.-C.; Chang, A.M.; Lee, W.-L. A preferred music listening intervention to reduce anxiety in older adults with dementia in nursing homes. J. Clin. Nurs. 2010, 19, 1056–1064. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, S.K.A.; Andersen, P.N.; Lugo, R.G.; Andreassen, M.; Sütterlin, S. Effects of Music on Agitation in Dementia: A Meta-Analysis. Front. Psychol. 2017, 8, 742. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, L.; Bieleninik, Ł.; Brondino, N.; Chen, X.-J.; Gold, C. The effect of music therapy on cognitive functions in patients with dementia: A systematic review and meta-analysis. Aging Ment. Health 2018, 22, 1103–1112. [Google Scholar] [CrossRef]
- Guess, H. Alzheimer’s disease and the impact of music therapy: A systematic literature review. James Madison Undergrad. Res. J. 2018, 5, 11–20. [Google Scholar]
- Zhang, Y.; Cai, J.; An, L.; Hui, F.; Ren, T.; Ma, H.; Zhao, Q. Does music therapy enhance behavioral and cognitive function in elderly dementia patients? A systematic review and meta-analysis. Ageing Res. Rev. 2017, 35, 1–11. [Google Scholar] [CrossRef]
- Van Der Steen, J.T.; Smaling, H.J.; Van Der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst. Rev. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Vasionytė, I.; Madison, G. Musical intervention for patients with dementia: A meta-analysis. J. Clin. Nurs. 2013, 22, 1203–1216. [Google Scholar] [CrossRef]
- Ing-Randolph, A.R.; Phillips, L.R.; Williams, A.B. Group music interventions for dementia-associated anxiety: A systematic review. Int. J. Nurs. Stud. 2015, 52, 1775–1784. [Google Scholar] [CrossRef]
- Leggieri, M.; Thaut, M.H.; Fornazzari, L.; Schweizer, T.A.; Barfett, J.; Munoz, D.G.; Fischer, C.E. Music Intervention Approaches for Alzheimer’s Disease: A Review of the Literature. Front. Neurosci. 2019, 13, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomaa, Y.S.; Wittwer, J.E.; Grenfell, R.J.; Sawan, S.A.; Morris, M. Music Cued Exercises for People Living with Dementia:A Systematic Review. Int. J. Physiother. 2018, 5, 36–49. [Google Scholar] [CrossRef]
- Dowson, B.; McDermott, O.; Schneider, J. What indicators have been used to evaluate the impact of music on the health and wellbeing of people with dementia? A review using meta-narrative methods. Maturitas 2019, 127, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Morales, C.; Calero, R.; Moreno-Morales, P.; Pintado, C. Music Therapy in the Treatment of Dementia: A Systematic Review and Meta-Analysis. Front. Med. 2020, 7. [Google Scholar] [CrossRef]
- Sakamoto, M.; Ando, H.; Tsutou, A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int. Psychogeriatr. 2013, 25, 775–784. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.; Gentile, S.; Villani, D.; Trabucchi, M. Efficacy of music therapy treatment based on cycles of sessions: A randomised controlled trial. Aging Ment. Health 2010, 14, 900–904. [Google Scholar] [CrossRef]
- Moore, J.R. Familiar Physical Activity to Familiar Music: The Effects on Apathy, Agitation, Eating Ability, and Dietary Intake in Institutionalized Older Adults with Dementia; University of Massachusetts Amherst: Springfield, MA, USA, 2010; p. 174. [Google Scholar]
- Nair, K.B.R.; Heim, C.; Krishnan, C.; D’Este, C.; Marley, J.; Attia, J. The effect of Baroque music on behavioural disturbances in patients with dementia. Australas. J. Ageing 2012, 30, 11–15. [Google Scholar] [CrossRef]
- Janata, P. Effects of Widespread and Frequent Personalized Music Programming on Agitation and Depression in Assisted Living Facility Residents With Alzheimer-Type Dementia. J. Music. Med. 2012, 4, 8–15. [Google Scholar] [CrossRef]
- Raglio, A.; Filippi, S.; Leonardelli, L.; Trentini, E.; Bellandi, D. The Global Music Approach to Dementia (GMA-D): Evidences from a case report. Aging Clin. Exp. Res. 2018, 30, 1533–1536. [Google Scholar] [CrossRef]
- Cheung, D.S.K.; Lai, C.K.Y.; Wong, F.K.Y.; Leung, M.C.P. The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: A randomized controlled trial. Aging Ment. Health 2018, 22, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.; Moyle, W.; Shum, D.; Harrison, S.; Murfield, J. Randomized Controlled Trial Exploring the Effect of Music on Quality of Life and Depression in Older People with Dementia. J. Health Psychol. 2010, 15, 765–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, M.H.; Flowerdew, R.; Parker, M.; Fachner, J.; Odell-Miller, H. Individual music therapy for managing neuropsychiatric symptoms for people with Dementia and their carers: A cluster-randomized controlled feasibility study. BMC Geriatr. 2015, 15, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Q.; Zhou, Y.; Yang, S.; Thomas, W.K.S.; Smith, G.D.; Yang, Z.; Yuan, L.; Chung, J.W.-Y. Effect of music intervention on apathy in nursing home residents with dementia. Geriatr. Nurs. 2018, 39, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Cheung, D.S.K.; Lai, C.K.Y.; Wong, F.K.Y.; Leung, M.C.P. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate Dementia? A randomized controlled trial. Dementia 2020, 19, 1413–1425. [Google Scholar] [CrossRef] [PubMed]
- Simmons-Stern, N.R.; Budson, A.E.; Ally, B.A. Music as a memory enhancer in patients with Alzheimer’s disease. Neuropsychologia 2010, 48, 3164–3167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H. The effect of individualized music on agitation for home-dwelling persons with dementia. Open J. Nurs. 2013, 3, 453–459. [Google Scholar] [CrossRef] [Green Version]
- Van Der Vleuten, M.; Visser, A.; Meeuwesen, L. The contribution of intimate live music performances to the quality of life for persons with dementia. Patient Educ. Couns. 2012, 89, 484–488. [Google Scholar] [CrossRef]
- Eggert, J.; Dye, C.J.; Vincent, E.; Parker, V.G.; Daily, S.B.; Pham, H.; Watson, A.T.; Summey, H.; Roy, T. Effects of viewing a preferred nature image and hearing preferred music on engagement, agitation, and mental status in persons with dementia. SAGE Open Med. 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.Y.; Lai, H.L.; Jeng, S.Y.; Tang, C.W.; Sung, H.C.; Chen, P.W. Effects of Researcher-Composed Music at Mealtime on Agitation in Nursing Home Residents with Dementia. Arch. Psychiatr. Nurs. 2011, 25, 49–55. [Google Scholar] [CrossRef]
- Baker, F.A.; Grocke, D.; Pachana, N.A.; Nancy, A.; Clair, A.; Alicia, A. Connecting through Music: A Study of a Spousal Caregiver-Directed Music Intervention Designed to Prolong Fulfilling Relationships in Couples Where One Person Has Dementia. Aust. J. Music Ther. 2012, 23, 4–21. [Google Scholar]
- Gulliver, A.; Pike, G.; Banfield, M.; Morse, A.R.; Katruss, N.; Pescud, M.; West, S. Evaluation of the Music Engagement Program for people with Alzheimer’s disease and Dementia: Study protocol for a pilot trial. Contemp. Clin. Trials Commun. 2019, 15, 100419. [Google Scholar] [CrossRef] [PubMed]
- Melhuish, R.; Beuzeboc, C.; Guzmán, A. Developing relationships between care staff and people with dementia through Music Therapy and Dance Movement Therapy: A preliminary phenomenological study. Dementia 2017, 16, 282–296. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.; Anderson, K.; Valuch, K.O. Findings From a Prospective Randomized Controlled Trial of an Individualized Music Listening Program for Persons With Dementia. J. Appl. Gerontol. 2020, 39, 567–575. [Google Scholar] [CrossRef]
- Gold, K. But does it do any good? Measuring the impact of music therapy on people with advanced dementia: (Innovative practice). Dementia 2013, 13, 258–264. [Google Scholar] [CrossRef]
- Takahashi, T.; Matsushita, H. Long-Term Effects of Music Therapy on Elderly with Moderate/Severe Dementia. J. Music. Ther. 2006, 43, 317–333. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Mazzola, P.; Bellandi, D.; Giovagnoli, A.; Farina, E.; Stramba-Badiale, M.; Gentile, S.; Gianelli, M.; Ubezio, M.; et al. Music, music therapy and dementia: A review of literature and the recommendations of the Italian Psychogeriatric Association. Maturitas 2012, 72, 305–310. [Google Scholar] [CrossRef]
- Davalos, D.B.; Luxton, I.; Thaut, M.; Cross, J.E. B Sharp—The cognitive effects of a pilot community music program for people with dementia-related disorders. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 592–596. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Ng, Y.-M.; Lee, M.M.; Kwok, T.C.; Wong, S.Y. Receptive Music Therapy Is More Effective than Interactive Music Therapy to Relieve Behavioral and Psychological Symptoms of Dementia: A Systematic Review and Meta-Analysis. J. Am. Med Dir. Assoc. 2018, 19, 568–576. [Google Scholar] [CrossRef]




| Type of Cognitive Disorder | Intervention Type | Individual/Group Therapy | Intervention Setting |
|---|---|---|---|
| Dementia (all type): 83.4% Alzheimer’s only: 3.3% Dementia (all types) & Alzheimer’s: 13.3% | Active MI: 26.6% Receptive MI: 36.6% Receptive & Active MI: 6.7% Active MT: 13.3% Receptive MT: 16.7% Live: 10% Recorded: 90% | Group: 30% Individual: 70% | Family home: 6.7% Hospital: 6.7% Residential aged care facility: 86.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soufineyestani, M.; Khan, A.; Sufineyestani, M. Impacts of Music Intervention on Dementia: A Review Using Meta-Narrative Method and Agenda for Future Research. Neurol. Int. 2021, 13, 1-17. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010001
Soufineyestani M, Khan A, Sufineyestani M. Impacts of Music Intervention on Dementia: A Review Using Meta-Narrative Method and Agenda for Future Research. Neurology International. 2021; 13(1):1-17. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010001
Chicago/Turabian StyleSoufineyestani, Mahsa, Arshia Khan, and Mina Sufineyestani. 2021. "Impacts of Music Intervention on Dementia: A Review Using Meta-Narrative Method and Agenda for Future Research" Neurology International 13, no. 1: 1-17. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010001