Telemedicine during the Coronavirus Disease (COVID-19) Pandemic: A Multiple Sclerosis (MS) Outpatients Service Perspective

 ,
, 
Abstract
:1. Introduction
2. Methods
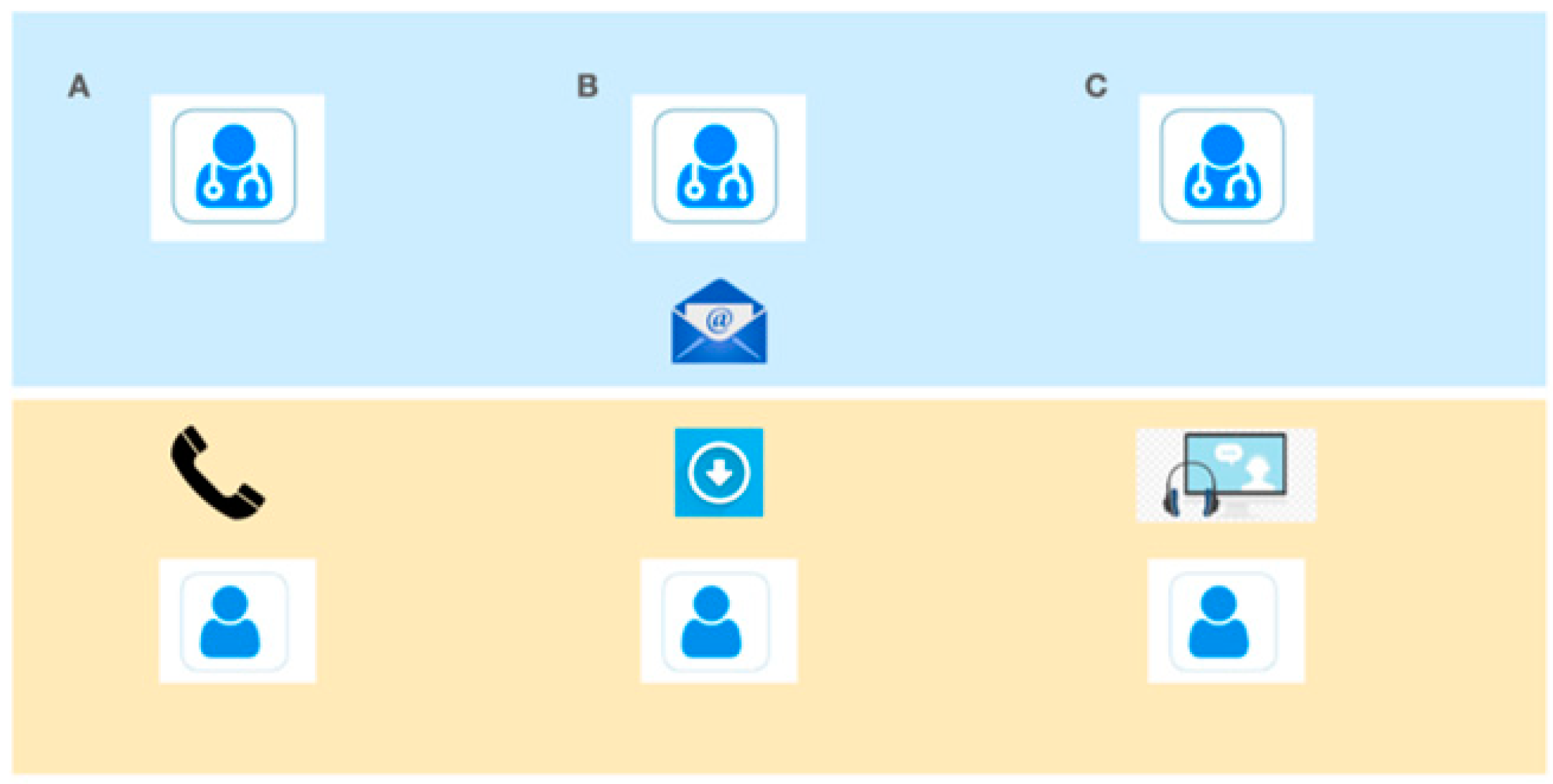
Technical Aspects
3. Results
3.1. Subject Participation
3.2. Demographics
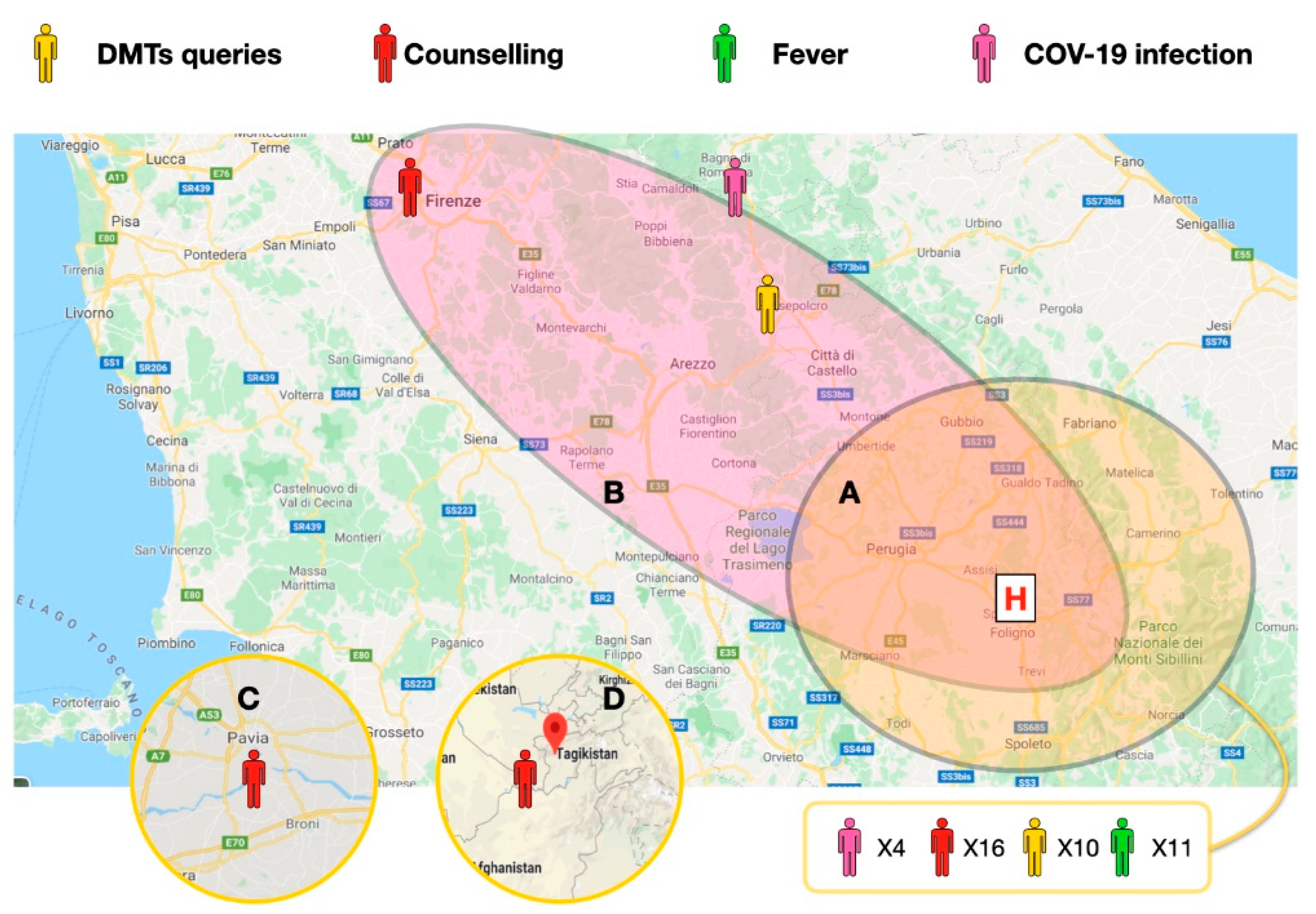
3.3. Reasons for Televisit
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Berardelli, A.; Silani, V.; Barone, P.; Calabresi, P.; Girlanda, P.; Lopiano, L.; Massacesi, L.; Monaco, S.; Onofrj, M.; Tassorelli, C.; et al. Neurology and the COVID-19 emergency. Neurol. Sci. 2020, 41, 1343–1344. [Google Scholar] [CrossRef] [PubMed]
- Zedde, M.; Pezzella, F.R.; Paciaroni, M.; Corea, F.; Reale, N.; Toni, D.; Caso, V. Stroke care in Italy: An overview of strategies to manage acute stroke in COVID-19 time. Eur. Stroke J. 2020, 5, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Caso, V.; Federico, A. No lockdown for neurological diseases during COVID19 pandemic infection. Neurol. Sci. 2020, 41, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, L.; Nuzzaco, G.; Muscia, F.; Gamboni, A.; Zedde, M.; Eusebi, P.; Zampolini, M.; Corea, F. Stroke Networks and Telemedicine: An Italian National Survey. Neurol. Int. 2018, 10, 41–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubert, G.J.; Santo, G.; Vanhooren, G.; Zvan, B.; Campos, S.T.; Alasheev, A.; Abilleira, S.; Corea, F. Recommendations on telestroke in Europe. Eur. Stroke J. 2018, 4, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Robb, J.F.; Hyland, M.H.; Goodman, A.D. Comparison of telemedicine versus in-person visits for persons with multiple sclerosis: A randomized crossover study of feasibility, cost, and satisfaction. Mult. Scler. Relat. Disord. 2019, 36, 101258. [Google Scholar] [CrossRef] [PubMed]
- Bove, R.; Bevan, C.; Crabtree, E.; Zhao, C.; Gomez, R.; Garcha, P.; Morrissey, J.; Dierkhising, J.; Green, A.J.; Hauser, S.L.; et al. Toward a low-cost, in-home, telemedicine-enabled assessment of disability in multiple sclerosis. Mult. Scler. J. 2018, 25, 1526–1534. [Google Scholar] [CrossRef]
- Hubert, G.J.; Corea, F.; Schlachetzki, F. The role of telemedicine in acute stroke treatment in times of pandemic. Curr. Opin. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Trojano, M.; Bergamaschi, R.; Amato, M.P.; Comi, G.; Ghezzi, A.; Lepore, V.; Marrosu, M.G.; Mosconi, P.; Patti, F.; Ponzio, M.; et al. The Italian multiple sclerosis register. Neurol. Sci. 2019, 40, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healey, K.M.; Zabad, R.; Young, L.; Lindner, A.; Lenz, N.; Stewart, R.; Charlton, M. Multiple Sclerosis at Home Access (MAHA): An Initiative to Improve Care in the Community. Int. J. MS Care 2019, 21, 101–112. [Google Scholar] [CrossRef] [PubMed]
- D’Haeseleer, M.; Eelen, P.; Sadeghi, N.; D’Hooghe, M.B.; Van Schependom, J.; Nagels, G. Feasibility of Real Time Internet-Based Teleconsultation in Patients with Multiple Sclerosis: Interventional Pilot Study. J. Med. Internet Res. 2020, 22, e18178. [Google Scholar] [CrossRef] [PubMed]
- Shaw, M.T.; Best, P.; Frontario, A.; Charvet, L.E. Telerehabilitation benefits patients with multiple sclerosis in an urban setting. J. Telemed. Telecare 2019. [Google Scholar] [CrossRef]
- Solà-Valls, N.; Blanco, Y.; Sepulveda, M.; Llufriu, S.; Martinez-Hernandez, E.; La Puma, D.; Graus, F.; Villoslada, P.; Saiz, A. Walking function in clinical monitoring of multiple sclerosis by telemedicine. J. Neurol. 2015, 262, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Capra, R.; Mattioli, F.C. Tele-health in neurology: An indispensable tool in the management of the SARS-CoV-2 epidemic. J. Neurol. 2020, 267, 1885–1886. [Google Scholar] [CrossRef] [PubMed]
- Moccia, M.; Lanzillo, R.; Morra, V.B.; Bonavita, S.; Tedeschi, G.; Leocani, L.; Lavorgna, L. Assessing disability and relapses in multiple sclerosis on tele-neurology. Neurol. Sci. 2020, 41, 1369–1371. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.L.; Bever, C.T.; Ehrmantraut, M.; Forte, A.; Culpepper, W.J.; Wallin, M.T. Teleneurology in patients with multiple sclerosis: EDSS ratings derived remotely and from hands-on examination. J. Telemed. Telecare 2008, 14, 190–194. [Google Scholar] [CrossRef]
- Neurology, T.L. COVID-19: A catalyst for flexibility and creativity in neurology. Lancet Neurol. 2020, 19, 557. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age, Mean Years (SD) | 42.8 (10.8) |
| Gender, female | 30 (65.2%) |
| Race | |
| Caucasian | 46 (100%) |
| Other | 0 |
| MS Type | |
| Relapsing remitting | 40 (86.9%) |
| Secondary progressive | 6 (13.1%) |
| Disease Duration | |
| <10 years | 40 (86.9%) |
| ≥10 and ≤20 | 5 (10.8%) |
| >20 years | 1(2.1%) |
| Disease Modifying Therapy | |
| Injectable | 16 (34.7%) |
| Oral | 20 (43.4%) |
| IV | 10 (21.7%) |
| None | 0 |
| Education | |
| High school graduate | 8 (17.3%) |
| College graduate | 30 (65.2%) |
| Higher degree | 8 (17.3%) |
| Income | |
| <25,000 | 0 |
| 25,000–49,999 | 31 (67.3%) |
| 50,000–99,999 | 15 (32.6%) |
| >100,000 | 0 |
| Declined | 0 |
| Employed | 30 (65.2%) |
| Drive Distance Time | |
| 0–30 min | 20 (43.4%) |
| 31–60 min | 20 (43.4%) |
| 61–120 min | 3 (6.5%) |
| >120 min | 3 (6.5%) |
| Main Complaint | DMTs Use /Dosage | Fever of Unknown Cause | COVID-19 Infection | Counselling on Social Distancing | Imaging | Others |
|---|---|---|---|---|---|---|
| Number of patients | 46 | 10 | 5 | 46 | 25 | 3 |
| % | 100 | 21.7 | 10.8 | 100 | 54.3 | 6.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corea, F.; Ciotti, S.; Cometa, A.; De Carlo, C.; Martini, G.; Baratta, S.; Zampolini, M. Telemedicine during the Coronavirus Disease (COVID-19) Pandemic: A Multiple Sclerosis (MS) Outpatients Service Perspective. Neurol. Int. 2021, 13, 25-31. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010003
Corea F, Ciotti S, Cometa A, De Carlo C, Martini G, Baratta S, Zampolini M. Telemedicine during the Coronavirus Disease (COVID-19) Pandemic: A Multiple Sclerosis (MS) Outpatients Service Perspective. Neurology International. 2021; 13(1):25-31. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010003
Chicago/Turabian StyleCorea, Francesco, Silvia Ciotti, Antonella Cometa, Claudia De Carlo, Giancarlo Martini, Silvano Baratta, and Mauro Zampolini. 2021. "Telemedicine during the Coronavirus Disease (COVID-19) Pandemic: A Multiple Sclerosis (MS) Outpatients Service Perspective" Neurology International 13, no. 1: 25-31. https://0-doi-org.brum.beds.ac.uk/10.3390/neurolint13010003