Contrast-Enhanced Ultrasound LI-RADS LR-5 in Hepatic Tuberculosis: Case Report and Literature Review of Imaging Features

 , , , and
, , , and
Abstract
:1. Introduction
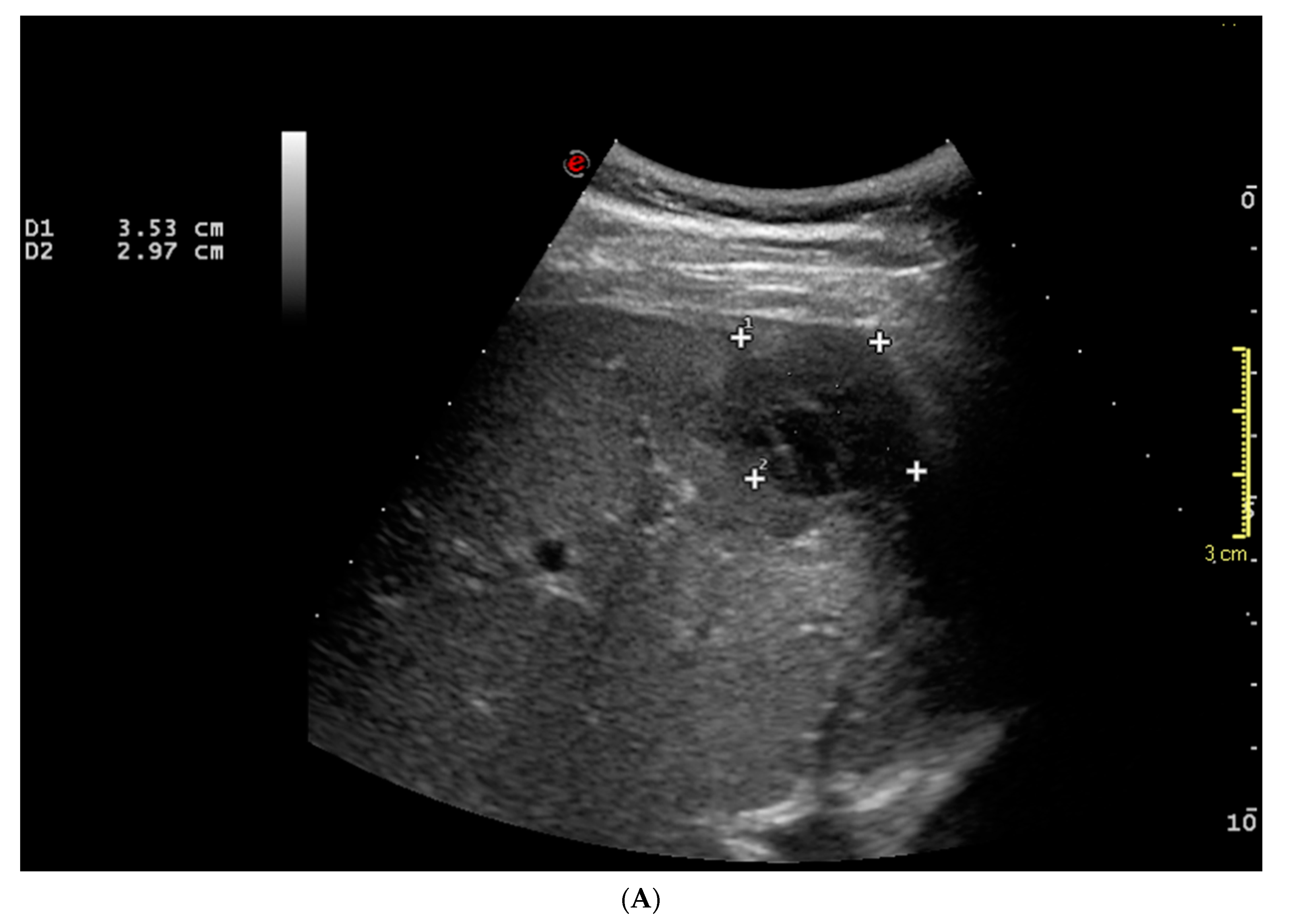
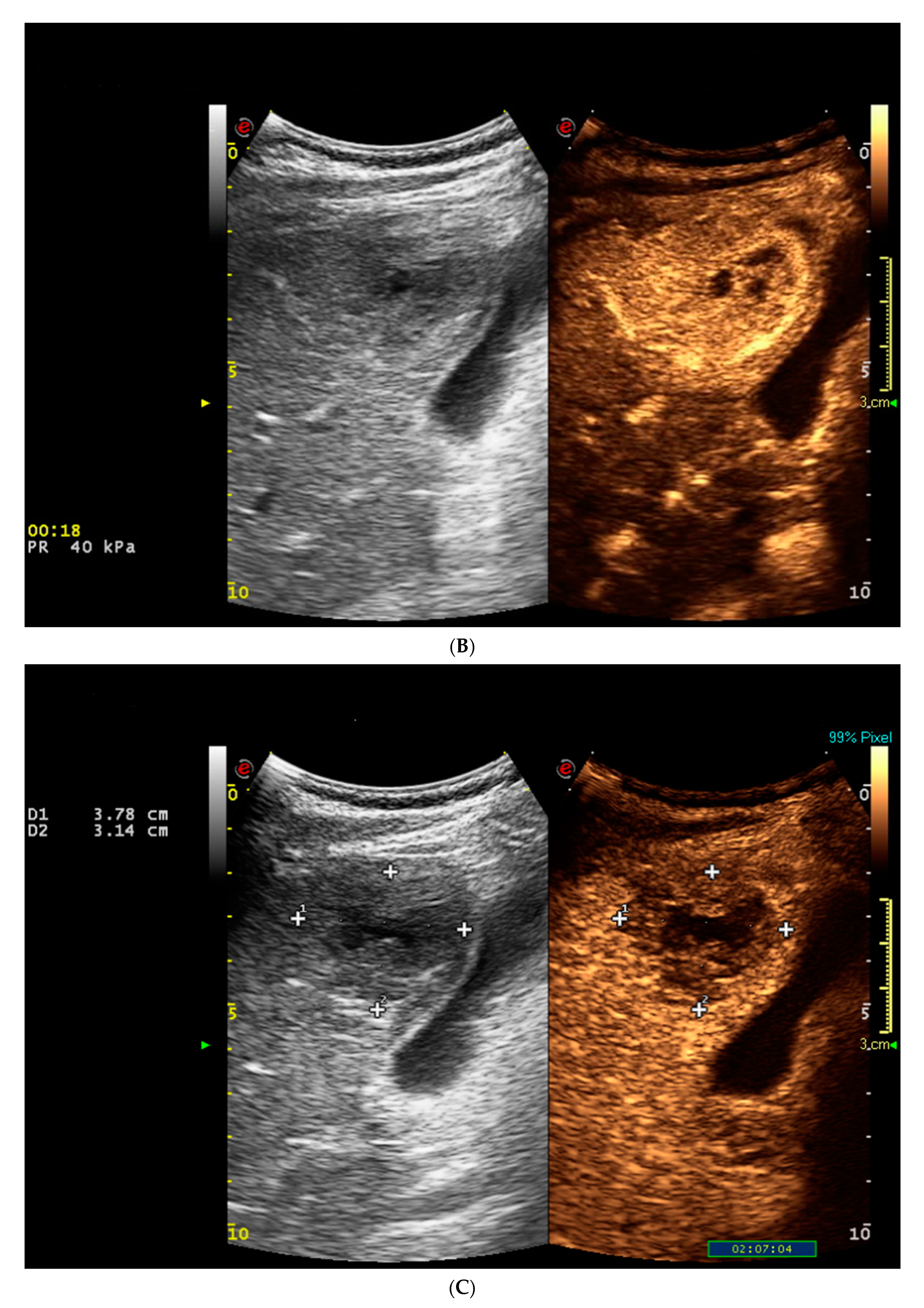
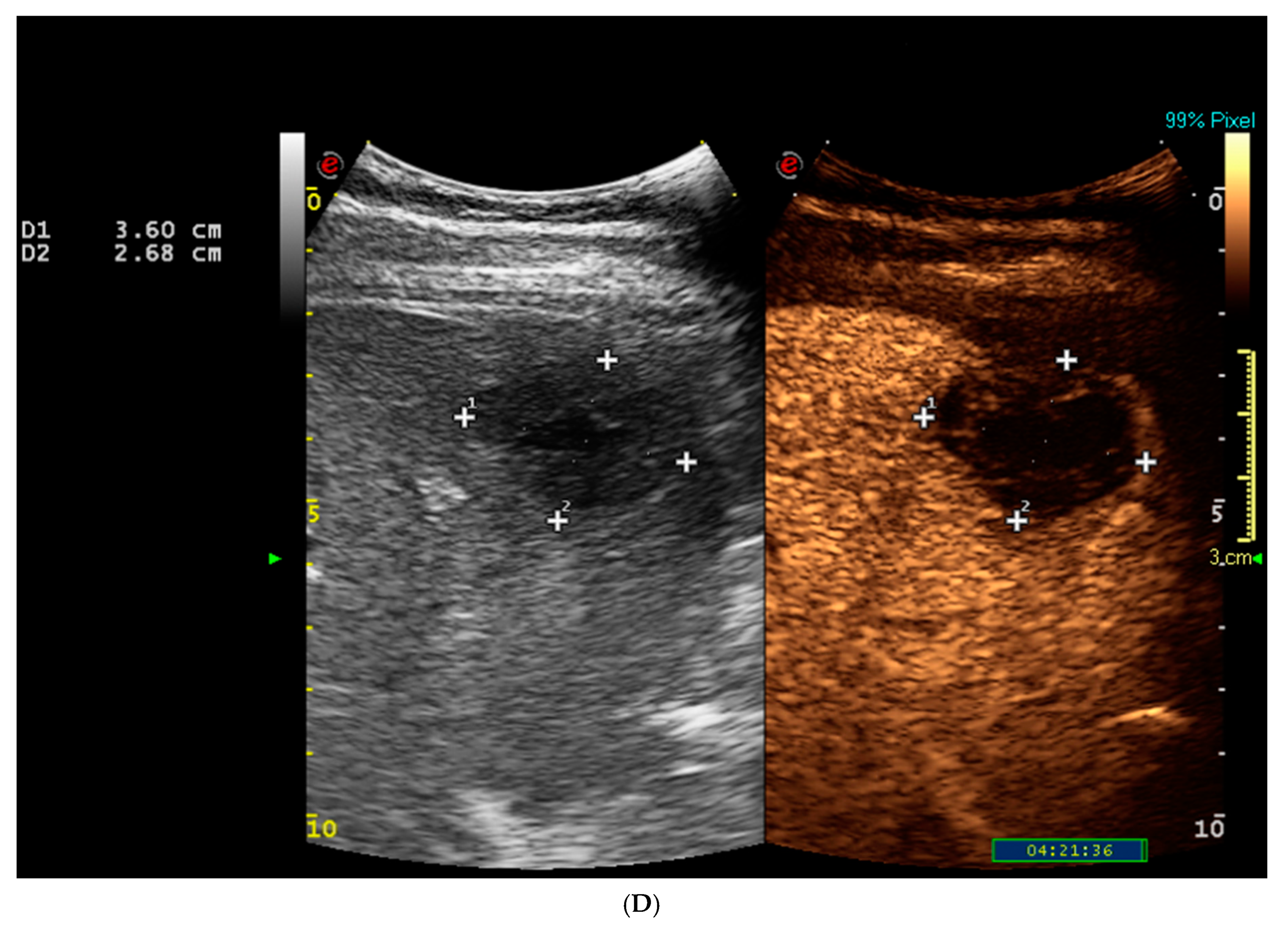
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIDS | Acquired Immunodeficiency Syndrome |
| BAAR | Acid-Alcohol Resistant Bacilli |
| CEUS | Contrast-enhanced Ultrasound |
| CT | Computed Tomography |
| E | Ethambutol |
| H | Isoniazid |
| HCV | Hepatitis C Virus |
| HIV | Human Immunodeficiency Virus |
| LI-RADS | Liver Imaging Reporting and Data System |
| MRI | Magnetic Resonance Imaging |
| PCR | Polymerase Chain Reaction |
| R | Rifampin |
| TB | Hepatic Tuberculosis |
| Z | Pyrazinamide |
References
- Kakkar, C.; Polnaya, A.M.; Koteshwara, P.; Smiti, S.; Rajagopal, K.V.; Arora, A. Hepatic tuberculosis: A multimodality imaging review. Insights Imaging 2015, 6, 647–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaosmanoglu, A.D.; Onur, M.R.; Sahani, D.V.; Tabari, A.; Karcaaltincaba, M. Hepatobiliary Tuberculosis: Imaging Findings. Am. J. Roentgenol. 2016, 207, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhu, J.; Dong, H.; Wang, Y.; Ma, J.; Kou, J.; Li, X.; He, Q. Isolated hepatic tuberculosis in the caudate lobe mimicking intrahepatic carcinoma. Clin. Res. Hepatol. Gastroenterol. 2017, 41, e65–e67. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.-S.; Zhang, S.-Z.; Wu, J.-J.; Li, R.-F. Imaging diagnosis of 12 patients with hepatic tuberculosis. World J. Gastroenterol. 2004, 10, 1639–1642. [Google Scholar] [CrossRef] [PubMed]
- Burrill, J.; Williams, C.J.; Bain, G.; Conder, G.; Hine, A.L.; Misra, R.R. Tuberculosis: A Radiologic Review. Radiographics 2007, 27, 1255–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for Study of Liver; Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terzi, E.; Iavarone, M.; Pompili, M.; Veronese, L.; Cabibbo, G.; Fraquelli, M.; Riccardi, L.; De Bonis, L.; SanGiovanni, A.; Leoni, S.; et al. Contrast ultrasound LI-RADS LR-5 identifies hepatocellular carcinoma in cirrhosis in a multicenter restropective study of 1006 nodules. J. Hepatol. 2018, 68, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Schellhaas, B.; Görtz, R.S.; Pfeifer, L.; Kielisch, C.; Neurath, M.F.; Strobel, D. Diagnostic accuracy of contrast-enhanced ultrasound for the differential diagnosis of hepatocellular carcinoma: ESCULAP versus CEUS-LI-RADS. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuberculosis. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 14 January 2021).
- Global Tuberculosis Report. 2018. Available online: https://www.who.int/tb/publications/global_report/gtbr2018_main_text_12August2019.pdf?ua=1 (accessed on 14 January 2021).
- Sharma, M.; Sinha, S.K.; Singh, A.K.; Samanta, J.; Sharma, A.; Kochhar, R.; Sharma, K. Challenging diagnosis of gastrointestinal tuberculosis made simpler with multi-targeted loop-mediated isothermal amplification assay. Eur. J. Gastroenterol. Hepatol. 2020, 32, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.; Gupta, S.; Singh, K.; Suri, S. Ultrasound guided fine needle aspiration cytology in abdominal tuberculosis. Br. J. Radiol. 1998, 71, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.J.; Gounder, L.; Moosa, M.Y.; Drain, P.K. A systematic review of hepatic tuberculosis with considerations in human im-munodeficiency virus co-infection. BMC Infect. Dis. 2015, 15, 209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambhir, S.; Ravina, M.; Rangan, K.; Dixit, M.; Barai, S.; Bomanji, J. International Atomic Energy Agency Extra-pulmonary TB Consortium. Imaging in extrapulmonary tuberculosis. Int. J. Infect. Dis. 2017, 56, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Sawhney, S.; Gupta, R.G.; Acharya, S.K. Sonographic appearances and percutaneous management of primary tuberculous liver abscess. J. Clin. Ultrasound 1999, 27, 159–163. [Google Scholar] [CrossRef]
- Ai, J.-W.; Li, Y.; Cheng, Q.; Cui, P.; Wu, H.-L.; Xu, B.; Zhang, W. Diagnosis of local hepatic tuberculosis through next-generation sequencing: Smarter, faster and better. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Schininà, V.; Albarello, F.; Cristofaro, M.; Di Stefano, F.; Fusco, N.; Cuzzi, G.; Arend, S.M.; Goletti, D.; Rizzi, E.B. Diagnostic imaging of hepatic tuberculosis: Case series. Int. J. Tuberc. Lung Dis. 2018, 22, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.S.; Pang, J. Isolated giant tuberculomata of the liver detected by computed tomography. Gastrointest. Radiol. 1989, 14, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-C.; Chao, Y.-C.; Shyu, R.-Y.; Hsieh, T.-Y. Isolated tuberculous liver abscesses with multiple hyperechoic masses on ultrasound: A case report and review of the literature. Liver Int. 2003, 23, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.C.; Cheung, A.Y.; Wan, W.Y.; Chen, T.C. Tuberculoma of the liver presenting as a hyperechoic mass on ultrasound. Br. J. Radiol. 1997, 70, 1293–1295. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.-S.; Li, X.-L.; Li, N.; Wang, Z.-Y. The nodular form of hepatic tuberculosis: Contrast-enhanced ultrasonographic findings with pathologic correlation. J. Ultrasound Med. 2010, 29, 881–888. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Time | Event | Findings |
|---|---|---|
| June 2019 | fever associated with night sweats | painless, hard, and fixed mass in the right supraclavicular fossa |
| July 2019 | Chest and Neck CT | Right supraclavicular lymphadenopathy of 26 × 22 mm |
| Fine needle aspiration of the lymphadenopathy of the right supraclavicular fossa; tissue culture and polymerase chain reaction (PCR) amplification. | Mycobacterium tuberculosis isolated from both tissue culture and PCR | |
| July 2019 | Chest X-ray | No signs of pulmonary TB. Diagnosis of tuberculous lymphadenopathy. Normal liver enzymes. HIV negative. |
| July 2019 | Starting treatment with Rifampin (R), Isoniazid (H), Pyrazinamide (Z), and Ethambutol (E) | Well tolerated |
| August 2019 | The patient was tested for viral hepatitis serological markers after detection of elevated AST/ALT, ALP, and GGT | HCV-related chronic hepatitis (genotype 3) |
| October 2019 | Abdominal ultrasound | No liver lesions |
| December 2019 | Chest contrast-enhanced CT | Neither pulmonary nor lymphadenopathy TB. Subcapsular focal liver lesion in liver segment five (S5) suggestive of malignancy |
| January 2020 | Drug-induced liver injury and underlying untreated HCV-related chronic hepatitis | anti-TB therapy was interrupted due to increased liver enzymes (AST 383 U/L, ALT 462 U/L), with progressive normalization of liver enzymes: AST/ALT 180/290 → 132/213 → 80/126 → 41/38 U/L in February 2020. |
| January 2020 | CEUS to further characterize the focal liver lesion | Focal liver lesion with CEUS LI-RADS LR5 pattern (highly suggestive of HCC) |
| January 2020 | 2-dimensional shear wave elastography (because of detection of focal liver lesion) | Liver stiffness of 10.9 kPa (suggestive of advanced chronic liver disease). |
| February 2020 | Liver wedge resection of liver segment five (S5) | Abscess with granulomatous inflammatory reaction with giant and necrotic cells |
| February 2020 | Histological examination and PCR for KB | No malignant cells; PCR positive for KB, sensitive to R; Diagnosis of hepatic TB |
| March 2020 | Antibiotic therapy with R, H, and Levofloxacin was administered. | Well tolerated |
| April, May, October, and December 2020 | Clinical and biochemical re-evaluation: no pathological findings. | In December 2020 the patient was asymptomatic. Laboratory: AST 64 U/L, ALT 65 U/L; and the CT scan was negative for disease recurrence. Anti-TB therapy was stopped. Anti-viral (HCV) therapy was scheduled. |
| Imaging | Contrast-Enhanced Ultrasound | Computed Tomography | Magnetic Resonance Imaging |
|---|---|---|---|
| Unenhanced scan | Mainly hypoechoic but also isoechoic or hyperechoic nodules * | hypodense lesions ° | hypointense on T1-weighted images, isointense or hyperintense lesions with a peripheral hypointense rim on T2-weighted images # |
| Arterial phase | Rim enhancement with a hypoenhanced or non-enhanced center or complete hyperenhancement of the lesion ^ | Peripheral contrast enhancement ° | Rim heterogenous contrast enhancement |
| Late phase | Wash-out | Wash-out | Wash-out |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forgione, A.; Tovoli, F.; Ravaioli, M.; Renzulli, M.; Vasuri, F.; Piscaglia, F.; Granito, A. Contrast-Enhanced Ultrasound LI-RADS LR-5 in Hepatic Tuberculosis: Case Report and Literature Review of Imaging Features. Gastroenterol. Insights 2021, 12, 1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010001
Forgione A, Tovoli F, Ravaioli M, Renzulli M, Vasuri F, Piscaglia F, Granito A. Contrast-Enhanced Ultrasound LI-RADS LR-5 in Hepatic Tuberculosis: Case Report and Literature Review of Imaging Features. Gastroenterology Insights. 2021; 12(1):1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010001
Chicago/Turabian StyleForgione, Antonella, Francesco Tovoli, Matteo Ravaioli, Matteo Renzulli, Francesco Vasuri, Fabio Piscaglia, and Alessandro Granito. 2021. "Contrast-Enhanced Ultrasound LI-RADS LR-5 in Hepatic Tuberculosis: Case Report and Literature Review of Imaging Features" Gastroenterology Insights 12, no. 1: 1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010001