1. Introduction
In hepatology practice, liver transplant recipients (LTRs) and autoimmune hepatitis patients (AIHPs) are in a similar clinical situation, generally requiring lifelong immunosuppression therapy (IST). While lifelong IST can effectively prevent LT rejection and AIH flare-ups, it is associated with adverse events that can vary from mild to severe. Side effects can include weight gain, alopecia, diabetes, hypertension, cytopenias, gastrointestinal symptoms and osteopenia [
1,
2,
3,
4]. More severe complications from chronic IST include the risks of opportunistic infections, chronic kidney disease, metabolic disorders, cardiovascular disease and malignancy [
1,
3,
4,
5].
Both patient populations differ significantly in the approach to immunosuppression withdrawal (ISW). In LTRs, ISW is largely experimental and generally conducted in clinical trials. Clinical trials have studied a variety of age ranges and indications for transplants, finding varying degrees of success in highly select patients (~30–40%) [
4]. On the other hand, ISW is generally part of the long-term management goals of AIHPs, with success rates between 13% and 50% [
6]. Both can derive similar benefits from ISW (e.g., the avoidance of complications associated with IST). Attempting ISW does, however, risk incurring a disease flare-up in AIHPs or rejection in LTRs that may cause significant liver injury and advance liver disease [
1,
5]. These risks must balance the desire to decrease a patient’s morbidity wing to chronic IST. Interestingly, AIH disease flare-ups and LT rejection during the course of or after ISW occur in similar percentages (50–80%) over time, and both respond well to the resumption of IST when detected in a timely fashion. Thus, there are enough commonalities in these patient populations to assess these approaches side-by-side.
However, little has been done to assess what patients desire and value when considering ISW. Patients’ attitudes toward ISW are potentially influenced by many factors outside of its risks and benefits, such as financial burden, number of medications, severity of disease before AIH presentation or liver transplantation and demographic factors, including age and gender. Despite the number of clinical studies in this area in both patient populations, there have not been efforts made to understand what motivates or influences these patients to consider this intervention and how this might play a role in provider patient selection and decision-making. Identifying a relationship between demographics, disease burden, medication burden and financial status has the potential to improve physicians’ abilities to counsel these patients on the prospect of ISW. Therefore, we sought this information utilizing independent, patient-oriented surveys asking similar questions to both populations.
2. Materials and Methods
We designed a survey eliciting LTR and AIHP demographic information, medical history and attitudes toward their IST and interest in attempting ISW, with the latter being scored on a Likert-like scale. (
Table S1) This survey was approved by the institutional review board. Study data were collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Northwestern University [
7,
8]. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. Patients were chosen solely on having AIH or an LT, currently being on an immunosuppression (IS) regimen and being literate. In order to obtain an unbiased sampling across the whole patient population, patients were not excluded based on clinical variables or disease presentations. Patients that were under 18 years old, acutely ill at recruitment, had potentially confounding liver diagnoses or were pregnant or incarcerated at recruitment were excluded from the study. None of the patients had previously been involved in ISW trials at the institution.
All participants were recruited from Northwestern Memorial Hospital in Chicago, Illinois. LTRs and AIHPs who participated in person were identified ahead of time from the clinic schedule. Those who participated electronically were recruited from separate lists of LTRs and AIHPs seen in our practice. Survey participation was elicited either in person during a visit to their hepatology clinic or by phone call or e-mail survey delivery after informed consent was given. Responses to the Likert-like scale questions were dichotomized to endorsing agreement (e.g., strongly agree and agree) or not (e.g., disagree, strongly disagree and neutral). Bivariate analyses (chi-square and Fisher’s exact) were conducted using SPSS statistical software to observe the association between sex, age, race or ethnicity, number of medications, number of disease complications, medication complications or side effect burden, difficulty taking the IS regimen, knowledge of expected side effects, financial burden, discussing ISW with a physician and desire to attempt ISW. Variables that were significantly associated with the desire to attempt ISW in the bivariate analyses were included in a final logistic regression model.
3. Results
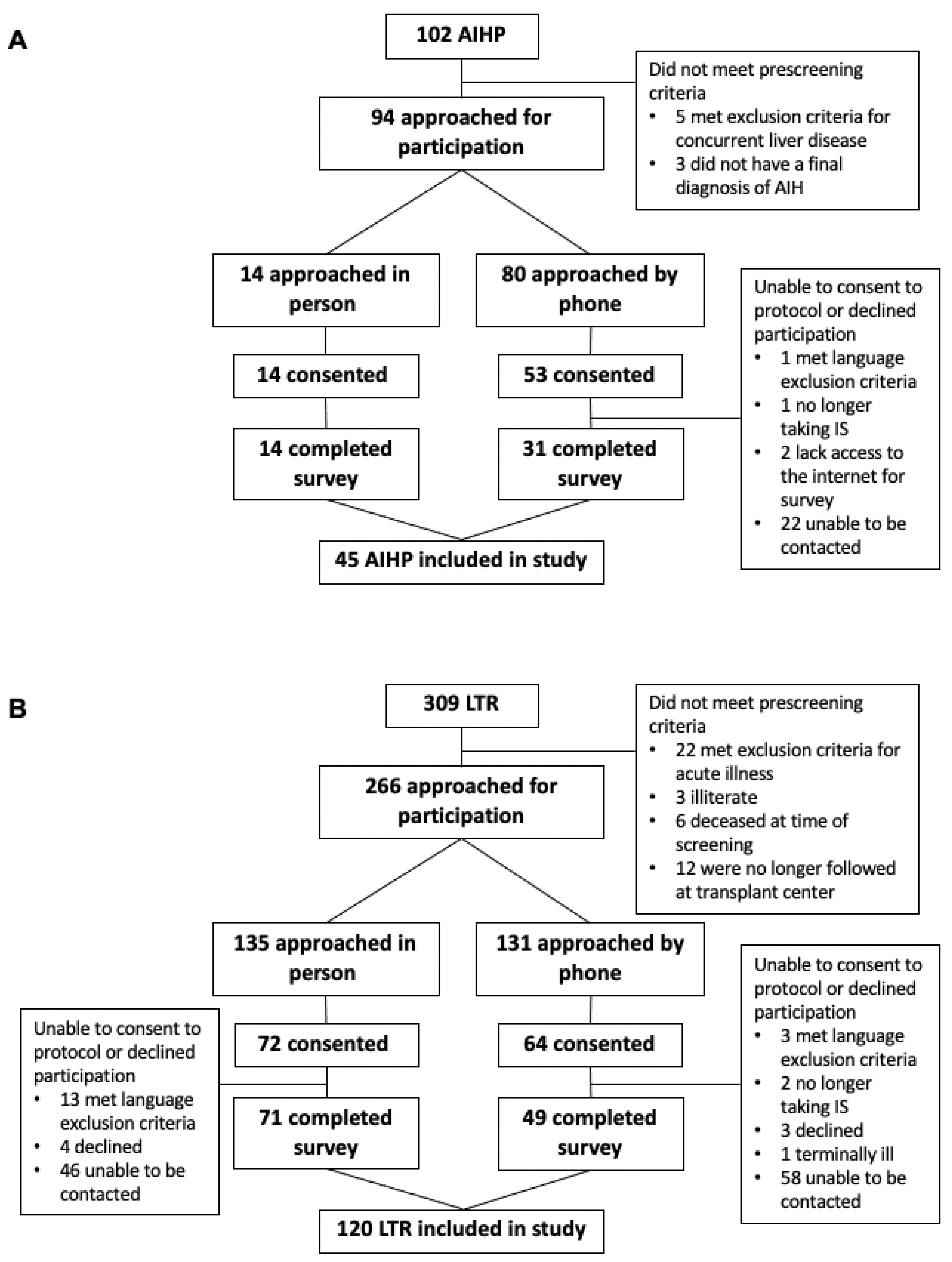
Of the 325 LTRs screened, 120 LTRs completed the survey (
Figure 1): 50% female, 79.5% Caucasian, mean age 58 ± 14 years, mean time since transplant 8 ± 10.5 years and 19.5% experiencing at least one rejection event. Of the 100 AIHPs screened, 45 completed the survey (
Figure 1): 77.8% female, mean age 54 ± 2, 82.2% Caucasian and a mean of 2.42 ± 1.3 AIH flare-ups. As expected, the two populations were significantly different demographically in age (
p = 0.011), sex (
p = 0.00), number of medications they were taking (
p = 0.038) and number of disease complications (
p = 0.001). The AIHPs skewed toward younger female patients taking fewer medications than the LTRs, who experienced more previous disease complications when compared with the AIHPs (
Table 1). The LTRs were less likely to have discussed ISW with their providers than the AIHPs (21.7% vs. 55.5%;
p = 0.00;
Table 2). No participant said that decreased spending on medications was their primary incentive for desiring withdrawal. This corresponded to the low number of participants in either cohort who stated IST was financially burdensome (15% and 22% for LTRs and AIHPs, respectively;
Table 2).
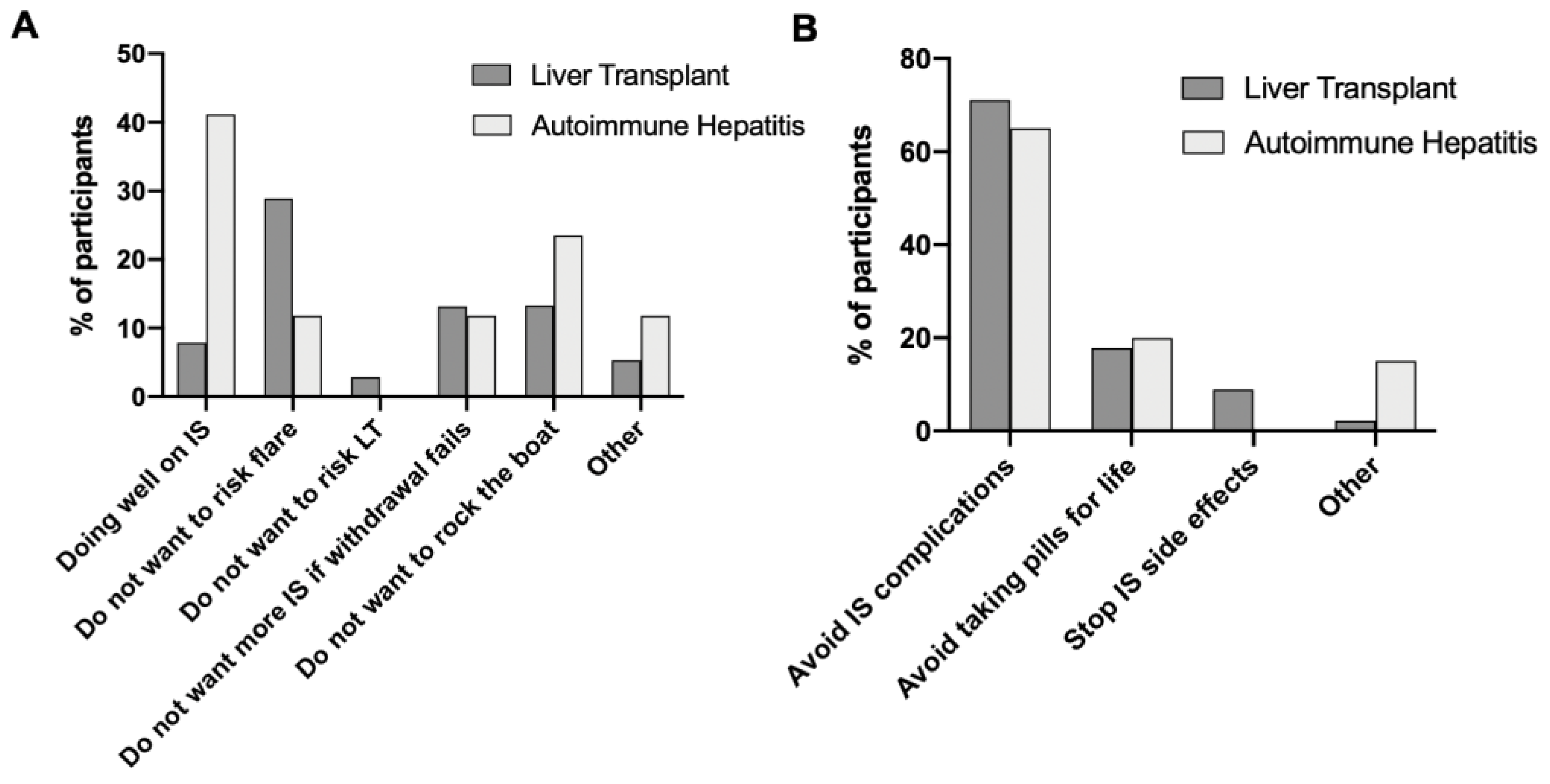
Among the LTRs that indicated they desired to attempt ISW (37.5%,
Table 2), most patients indicated wanting to avoid the risk of major IS complications (71.1%,
Figure 2) and reliance on lifelong medications (31.1%). Among those that indicated they would not attempt ISW, most indicated that they were doing well in their IST as the primary (42.1%,
Figure 2) and secondary (36.8%) reasons. Of the AIHPs who endorsed a desire for ISW (44.4%,
Table 2), most people stated wanting to avoid IS (65.0%,
Figure 1) as their primary reason and avoiding lifelong medication use (55.0%) as their secondary reason. Among the patients indicating they did not want to attempt ISW, the most common primary reason was to avoid the risk of an AIH flare-up (41.2%,
Figure 1), and the most selected secondary reason was because they were doing well in their IST (41.2%).
Our bivariate analyses found the following initial results in the LTRs. Those who discussed ISW with a physician were more likely to desire full ISW, and female LTRs were more likely to desire ISW than male LTRs. After including the other predictive factors in the final logistic regression model, only discussion of ISW with a physician remained significantly associated with desiring ISW (p = 0.02; OR = 2.781 (95% CI = 1.125, 6.872)). LTR sex was not significantly associated with whether or not their physician discussed ISW with them (p = 0.330).
In the AIHPs, bivariate analyses found that those experiencing more medication complications were less likely to desire ISW than those experiencing fewer complications. However, this association was no longer significant when other predictive factors were accounted for in the final logistic regression model.
There were no associations between the side effect burden of medications, participants’ knowledge of side effects or financial burden of IST and interest in ISW in either population.
4. Discussion
To our knowledge, this is the first study assessing patient opinions on ISW from two groups commonly seen in hepatology practice: LTRs and AIHPs. Our findings relating to interest in attempting ISW revealed differences between these patient populations. The significant association between LTRs discussing ISW with their physician and desiring to attempt ISW was not as apparent in AIHPs. That said, over half of the AIHPs had discussed ISW with their physicians, compared with 21.7% of the LTRs (
p = 0.001,
Table 2). This difference could reflect differences in the course of disease between the groups, with AIHPs more likely to be offered ISW as a normal part of management per society guidelines. Another potential explanation is that LTRs have undergone an extensive process of learning and communication with their transplant team, which may create a stronger connection between practitioner and patient and thus make this population more amenable to conversations regarding disease education and options for their care.
Although female LTRs were more likely to endorse interest in withdrawal in the bivariate chi-squared analysis (
p = 0.045,
Table 3), this association was no longer significant in the final logistic regression model (
p = 0.067; OR = 2.057 (95% CI = 0.951, 4.450)). This suggests that variation in other predictors may confound the relationship between LTR sex and desire to withdraw therapy, or that we would be able to identify a significant relationship with a larger sample size. We were unable to demonstrate a confounding relationship between female sex and discussing ISW with their physician in LTRs (
p = 0.330). Further investigation would be required to properly identify the influence of LTR sex on ISW and related variables.
It is important to note that avoiding IST complications was the most common reason LTRs cited in explaining why they desired ISW, illustrating that the study participants were aware of and concerned about the possible deleterious effects of lifelong IST. On the other hand, LTRs that did not desire ISW most often explained that they were doing well on their IS regimen. Together, this may suggest that there are two different patient groups that value being on IST differently. This could potentially be explained by variables such as the time since a liver transplant, such that patients who have taken IST for longer may become more concerned about the effects of IST than those who have had a transplant more recently, who would be more concerned with prioritizing graft health. Future work can explore a potential temporal relationship in LTRs regarding their perception of their IST. Interestingly, physician discussion about ISW was the only predictive factor of patient interest above other potential reasons, such as side effect burden and financial implications. This reinforces the importance of physician–patient communication in discussing the risks and benefits of IST and what patients desire long-term.
In this study, we profiled two patient cohorts, LTRs and AIHPs, as they are both involved in ISW discussions in hepatology practice but are indeed different in regard to prior transplantation. Overall, the comparison of these cohorts from our academic research center aligns with what might have been assumed from clinical experience. Not surprisingly, we found that AIHPs were more likely to be younger with a female predilection compared to LTRs, and LTRs reported higher rates of polypharmacy and disease complications. Management of IST in LTRs may be more complex than in AIHPs, and there are fewer solid guidelines that are agreed upon by practitioners and societies [
3,
9,
10]. The main difference is that ISW is considered a standard of care option in AIHPs, while it is generally only an option in LTRs in clinical research studies unless clinically warranted in rare circumstances (e.g., severe opportunistic infections, post-transplant lymphoproliferative disorder and metastatic cancer).
There are important limitations to acknowledge for our findings. Data was collected at a single high-volume academic center that conducts ISW trials specifically in LTRs. We would expect similar studies at centers not engaging in such trials to report smaller percentages of participants desiring ISW or having had a discussion about it with their physicians. Our findings are also vulnerable to response and recall bias by nature of data collection by surveying participants. Additionally, the limited racial diversity might underrepresent the disease complications, since multiple studies have shown that non-caucasian patients with AIH present with more severe liver disease and symptoms [
11,
12]. Lastly, AIH is a rarer disease with less formal institutional organization than LT, which contributed to a lower number of participants and analytical power.
5. Conclusions
We have conducted the first study on patient opinions from two groups in hepatology practice considered for ISW: LTRs and AIHPs. We have demonstrated evidence of sufficient patient interest in ISW, confirming that it is not only the providers but also patients who are interested. Therefore, patients need to be informed of this intervention and properly counseled on current knowledge and practices to enhance patient-reported outcomes and quality of life.
Supplementary Materials
The following are available online at
https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/gastroent12020013/s1, Table S1: survey-LTAIH. This survey was provided to participants through REDCap. Once patients chose whether they were LTR or AIHPs, the survey would branch to allow for appropriate questions regarding rejection or flare ups accordingly, as well as transplant date. Both branches of the survey are included.
Author Contributions
Conceptualization, J.L.; methodology, J.L.; formal analysis, P.C.; investigation, E.S. and A.C.; data curation, P.C.; writing—original draft preparation, E.S. and A.C.; writing—review and editing, J.L.; supervision, J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Northwestern University (ID STU00207617, approved 10/3/19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis. Clin. Liver Dis. 2015, 19, 57–79. [Google Scholar] [CrossRef]
- Czaja, A.J.; Menon, K.V.N.; Carpenter, H.A. Sustained remission after corticosteroid therapy for type 1 autoimmune hepatitis: A retrospective analysis. Hepatology 2002, 35, 890–897. [Google Scholar] [CrossRef]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- Whitehouse, G.P.; Sanchez-Fueyo, A. Immunosuppression withdrawal following liver transplantation. Clin. Res. Hepatol. Gastroenterol. 2014, 38, 676–680. [Google Scholar] [CrossRef]
- Levitsky, J.; Feng, S. Tolerance in clinical liver transplantation. Hum. Immunol. 2018, 79, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Lucey, M.R.; Terrault, N.; Ojo, L.; Hay, J.E.; Neuberger, J.; Blumberg, E.; Teperman, L.W. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transplant. 2013, 19, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Charlton, M.; Levitsky, J.; Aqel, B.; O’Grady, J.; Hemibach, J.; Rinella, M.; Fung, J.; Ghabril, M.; Thomason, R.; Burra, P.; et al. International Liver Transplantation Society Consensus Statement on Immunosuppression in Liver Transplant Recipients. Transplantation 2018, 102, 727–743. [Google Scholar] [CrossRef]
- Verma, S.; Torbenson, M.; Thuluvath, P.J. The impact of ethnicity on the natural history of autoimmune hepatitis. Hepatology 2007, 46, 1828–1835. [Google Scholar] [CrossRef]
- Zolfino, T.; A Heneghan, M.; Norris, S.; Harrison, P.M.; Portmann, B.C.; McFarlane, I.G. Characteristics of autoimmune hepatitis in patients who are not of European Caucasoid ethnic origin. Gut 2002, 50, 713–717. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}