
COVID-19 and the Gastrointestinal Tract

1
International Renal Research Institute of Vicenza, San Bortolo Hospital, 36100 Vicenza, Italy
2
American British Cowdray Medical Center, Mexico City 01120, Mexico
3
North Campus, Anahuac University, Mexico City 52786, Mexico
Gastroenterol. Insights 2021, 12(4), 394-404; https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12040038
Submission received: 13 September 2021
/
Revised: 16 October 2021
/
Accepted: 19 October 2021
/
Published: 24 October 2021
(This article belongs to the Collection Gastroenterological Aspects of COVID-19 Infection)
Abstract
:Since it was discovered at the end of 2019; the pandemic of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has made a serious public health threat worldwide, with over 175 million confirmed cases reported globally. Even when COVID-19 was initially considered a respiratory disease, it was actually known to be multisystemic, with gastrointestinal involvement a common clinical finding. Furthermore, COVID-19 may affect patients with gastrointestinal comorbidities, being the clinical intersectionality of utmost interest for gastroenterologists; critical care physicians and all the healthcare team taking care of COVID-19 patients. The present article presents a brief review of the reported gastrointestinal manifestations of COVID-19 disease in both previously healthy individuals and in patients with gastrointestinal comorbidities.
1. Introduction
Discovered at the end of 2019, the pandemic of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global threat to public health, with over 243,331,864 confirmed cases reported [1,2]. Furthermore, the reported case counts underestimate the burden of COVID-19, as not all of the infections are diagnosed. Seroprevalence surveys suggest that the rate of prior exposure to SARS-CoV-2, as reflected by seropositivity, exceeds the number of reported cases by at least tenfold [3,4].
Coronaviruses are enveloped, positive-stranded RNA viruses. Among them, SARS-CoV-2 is a Betacoronavirus in the same subgenus as the severe acute respiratory syndrome (SARS) virus and some bat coronaviruses, but in a different clade [5].
The host receptors for SARS-CoV-2 cell entry includes the angiotensin-converting enzyme 2 (ACE2). SARS-CoV-2 binds to ACE2 through the receptor-binding domain of its spike protein. The cellular protease TMPRSS2 also plays a role in the SARS-CoV-2 cell entry [6,7].
The kidney injury molecule-1 (KIM1), upregulated upon kidney injury, binds to the receptor-binding domain (RBD) of SARS-CoV-2 facilitating its attachment to cellular membranes, with the immunoglobulin variable Ig-like (Ig V) domain of KIM1 having an important role in its recognition. Higher levels of KIM-1 are associated with more severe COVID-19 disease, but the clinical significance of KIM-1-RBD interaction is yet to be fully understood [8,9,10].
The clinical spectrum of COVID-19 disease varies widely, from asymptomatic infection to multiple organ failure, with lethality rates depending on the characteristics of the studied population. It is estimated that at least one-third of SARS-CoV-2 infections are asymptomatic, and nearly three-quarters of the patients with a positive PCR test but no symptoms at the time of diagnosis remain asymptomatic. However, the definition of “asymptomatic” varies across studies, depending on which specific symptoms were assessed [11].
Among symptomatic cases, the spectrum of disease ranges from mild to critical illness; most cases not been severe.
- In a report from the Chinese Center for Disease Control and Prevention (CDC) including about 44,500 confirmed infections, mild disease was reported in 81% of patients. Severe disease (e.g., dyspnea, hypoxia, or >50 percent lung involvement) was reported in 14%. Critical disease was reported in 5%, and the overall case fatality rate was 2.3%, with no deaths among noncritical patients [12].
- Out of 1.3 million cases reported to the United States Centers for Disease Control and Prevention (CDC) through the end of May 2020, 14% of patients were hospitalized, 2% were admitted to the intensive care unit, and 5% died [13].
Nonspecific symptoms (such as cough, myalgias and headache) are the most commonly reported clinical presentation for mild disease, and pneumonia the most common presentation for moderate and severe disease [14]. However, gastrointestinal symptoms and complications may be found all along the clinical spectrum of COVID-19 disease [13].
In a Chinese retrospective study including 651 confirmed COVID-19 cases, 11.4% of patients presented with at least one GI tract symptom (nausea, vomiting or diarrhoea). Increased AST, but not ALT, was significantly higher in patients with GI symptoms. Finally, although the most common radiographic presentations were similar between patients with and without GI symptoms, the rate of unilateral pneumonia was 12.16% in patients with GI symptoms [15].
In the aforementioned study, 22.97% of patients with severe/critical COVID-19 presented with GI symptoms, and increased LDH/glucose levels were the independent risk factors for severe/critical COVID-19 in patients with GI symptoms [15].
A systematic review and meta-analysis reported pooled detection rates for diarrhoea, nausea or vomiting and liver function tests abnormalities and a positive SARS-CoV-2 faecal test. There were 23 published and 6 preprint studies (a total of 4805 patients); 7.4% (95% CI 4.3–12.2%) reported diarrhoea and 4.6% (95% CI 2.6–8.0%) nausea or vomiting. 20% (95% CI 15.3–25.6%) had abnormal AST values and 14.6% (95% CI 12.8–16.6%) an ALT outside the normal range [16].
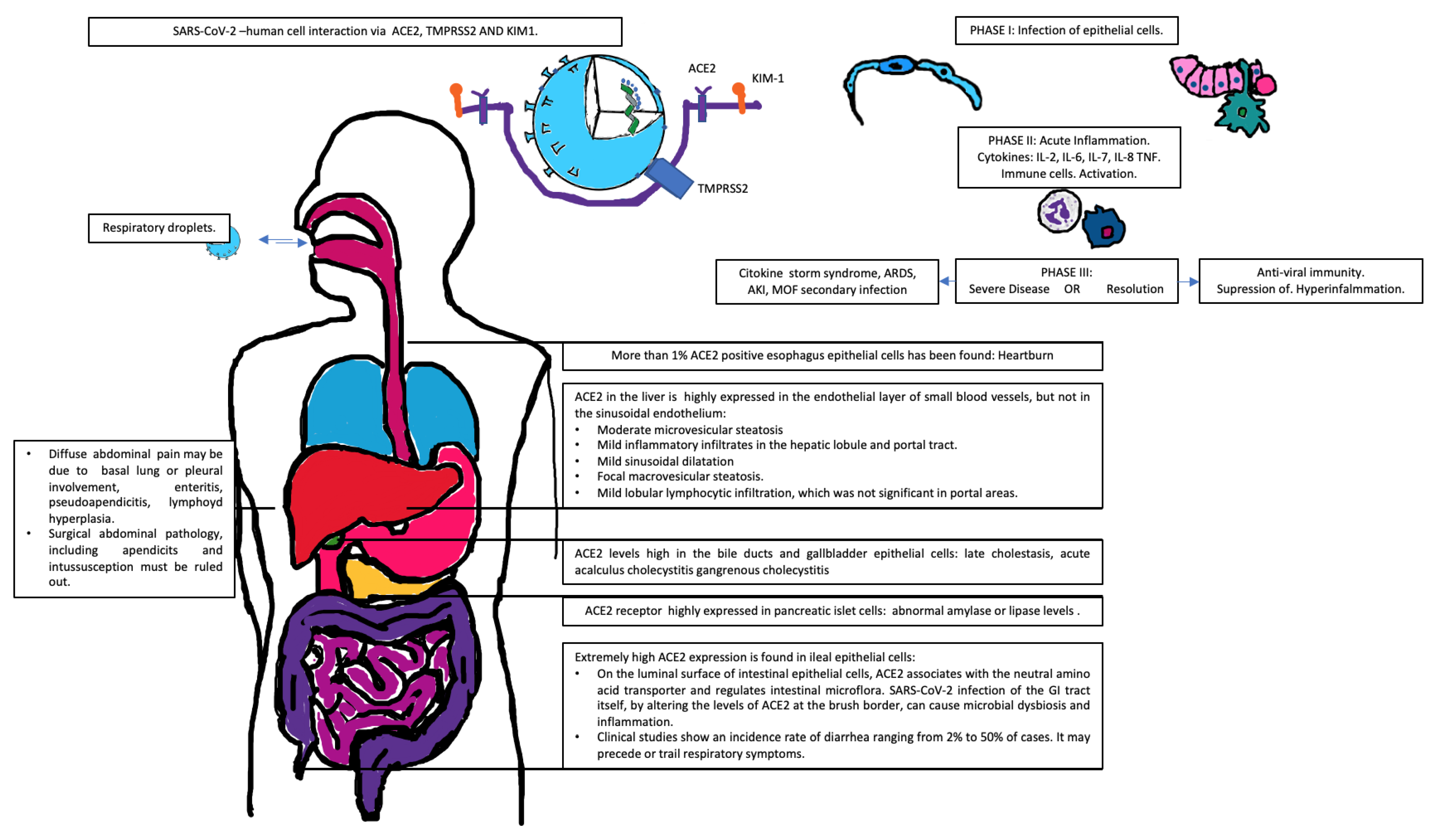
In the following sections, a brief review of organ-specific involvement in both previously healthy patients and those with gastrointestinal-comorbidities will be reviewed. In Figure 1, GI involvement mechanisms and clinical findings in COVID-19 disease are briefly summarized.
2. Upper Gastrointestinal Tract
Single-cell RNA-seq data analysis of ACE2 expression has revealed the differential risk of human organs regarding vulnerability to SARS-CoV-2 infection; more than 1% of ACE2 positive oesophagus epithelial cells has been found, and the esophagus can thus be regarded as high risk. By contrast, gastric and liver cells showed <1%ACE2 positive cell expression levels [17]. ACE2 expression is elevated in the lung and trachea of diet-induced obese male mice and reduced at the oesophagus of obese female mice when compared to lean controls [18].
Even if oesophageal symptomatologies directly attributable to the SARS-CoV-2 infection have not been reported, heartburn is common, (as in the general population) and requires a standard treatment with proton pump inhibitors (PPIs) or H2 receptor antagonists (H2RAs). A plausible benefit with famotidine in COVID-19 patients who were taking famotidine for acid-related reflux prompted a small study that reported an improved clinical course in COVID-19 patients [19].
On the other hand, the impact of acid suppression on SARS-CoV-2 is unknown; previous data revealed that pH ≤3 impairs the infectivity of the similarly severe acute respiratory syndrome coronavirus 1. An online survey that included 53,130 participants found evidence of an independent, dose-response relationship between the use of antisecretory medications and COVID-19 positivity [20].
There is scarce information on the prognostic implications of bariatric surgery history in people living with obesity in the current COVID-19 pandemic [21]. In a study that included 738 post-bariatric surgery patients, COVID-19-likely events occurred in 8.4% of patients, with 6.4% of them having severe COVID-19 requiring in-hospital treatment and a 1.6% fatality rate. Persistent type 2 diabetes and higher percent weight loss since bariatric surgery were associated with hospitalization rates [22].
3. Pancreatic Involvement
Pancreatic injury, defined as abnormal amylase or lipase levels, has been reported to be found in 17% of patients with COVID-19 pneumonia. Being the ACE2 receptor highly expressed in pancreatic islet cells, it is plausible that SARS-CoV-2 exerts direct cytopathic damage-mediated pancreatitis; it is, however, impossible to discard indirect systemic inflammatory and immune-mediated cellular responses, as well as drug-related pancreatic injury, especially considering that most cases are mild and without radiologic abnormalities [23,24].
4. Gallbladder and Biliary
Given that ACE2 levels are high in the bile ducts and gallbladder epithelial cells [25], it is feasible that direct cytopathic damage, hypoxia, secondary inflammatory damage and thrombosis are responsible for gall bladder and biliary tract involvement, including late cholestasis and acute acalculus cholecystitis gangrenous cholecystitis [26,27].
5. Liver Involvement
ACE2 in the liver is highly expressed in the endothelial layer of small blood vessels, and is highly expressed in cholangiocytes, (59.7%) but its expression is much lower in hepatocytes (2.6%) and it is not expressed in the sinusoidal endothelium, Kupffer cells, or T and B. lymphocytes [28]. Just as in the case of any other extrapulmonary involvement in patients with COVID-19, liver injury may be the result of the interaction of multiple factors, including direct cythopathic damage, inflammation, ischemia, thrombosis, drug-related adverse events, and pre-existing organic damage.
Histopathologic changes reported in post- mortem liver biopsies from COVID-19 patients include: [29,30].
- Moderate microvesicular steatosis.
- Mild inflammatory infiltrates in the hepatic lobule and portal tract.
- Mild sinusoidal dilatation.
- Focal macrovesicular steatosis.
- Mild lobular lymphocytic infiltration, which was not significant in portal areas.
Also, liver biopsies from live patients with COVID-19 had revealed mild to moderate lobular lymphocytic inflammation, a ballooning in hepatocytes, apoptosis, and, most prominently, high mitotic figures indicative of a rapidly proliferative state [31].
In patients with pre-existing liver damage (i.e., chronic hepatic failure, cirrhosis), respiratory tract infections increase hospital admission rate by a factor of 40, with a 2.95-fold increase in 30 day mortality rates for ambulatory patients and an 11-fold increase of the in-hospital death rate.
Two combined international registries on COVID-19 patients with liver disease (named SECURE-Cirrhosis and COVID-HEP registries), had reported, up to June 2021, 1588 COVID-19 cases of COVID-19 in patients with chronic liver diseases and liver transplant. (772 with cirrhosis and 281 liver transplant recipients) [32,33,34].
Mortality among cirrhotic patients with COVID-19 is reported to be 32%, with age, higher Child-Pugh and alcohol-related liver disease associated with higher death rates [35]. There were no differences in rates of major outcomes between patients with autoimmune hepatitis (AIH) and non-AIH CLD, including hospitalization (76% vs. 85%), ICU admission (29% vs. 23%), and death (23% vs. 20%). Factors associated with death within the AIH patients included age and Child-Pugh class B and C [36].
Liver transplant recipients did not differ from non-transplanted patients in hospitalization rates, but had high ICU admission (28%) and mechanical ventilation (20%) rates, with no differences in mortality rate (19%). Serum creatinine concentration and non-liver cancer were associated with death among liver transplant recipients [37].
The prognostic significance and expected clinical course of viral hepatitis and COVID-19 coinfection remains to be fully described:
- A significant increasing trend in COVID-19 mortality rates by HAV susceptibility has been described. The immunity of children against HAV (a virus with similar taxonomy to coronaviruses), acquired either by vaccination in developed countries or by infection in underdeveloped countries, may have contributed to this protection. The loss of immunity to HAV as the result of aging may have led to an increased COVID-19 morbidity in the elderly [38].HAV replication occurs in hepatocyte cytoplasm, thus hepatocellular damage is mediated by direct cytotoxicity. Interferon-gamma (IFN-γ) has a key role in the clearance of HAV of infected hepatocytes. On the other hand, the HAV vaccine is highly immunogenic, inducing seropositivity in 97% of adults after the second dose. The HAV vaccine causes specific proliferation of mononuclear cells in peripheral blood and the release of IFN-γ, thus making it possible that the immune response caused by the HAV vaccine might be protective against COVID-19 infection by an adaptive immunity cross-reaction [39].
- As HBV infection can alter innate immune responses, and uncontrolled innate responses and impaired adaptive immune responses caused by the COVID-19 disease may generate tissue damage, it is plausible that co-infection of SARS-CoV-2 and HBV may synergistically cause disturbances of the immune function and that of the liver.In a retrospective study, Lin et al. reported higher rates of abnormal liver function test in tCOVID-19 positive- HBV inactive carriers compared to their non-HBV carriers counterparts [40]. Similarly, Zou reported higher incidences of liver function test abnormalities among chronic HBV carriers with COVID-19 disease. Among HBV- COVID19 coinfected hospitalized patients, 13.33% developed liver injury; 71.43% recovered after eight days and 28.57% rapidly progressed to acute-on-chronic liver failure; patients with liver injury are more likely to have severe illness, higher incidence of complications and mortality [41].On the other hand, among patients with chronic HBV infection, Liu et al. reported no statistically significant differences in the median time to SARS-CoV2 clearance or progression to severe COVID-19 disease, but three out of 19 patients presented HBV reactivation. Diffuse ballooning degeneration, necrosis of isolated hepatocytes, periportal fibrosis, few inflammatory cells infiltrating the portal tract, positive HBsA and negative hepatitis B core antigen immunohistochemistry were the main histopathological findings [42].
- In a retrospective analysis of the Electronically Retrieved Cohort of HCV Infected Veterans (ERCHIVES), testing rates for SARS-CoV-2 among HCV positive patients was found to be only 8.3%, with 6.2% of tests being positive.HCV positive persons with SARS-CoV-2 coinfection were more likely to be black, have a higher body mass index, diabetes or stroke, with no apparent association between liver fibrosis and infection rate [43].
6. Gut Involvement
There are at least two different physiopathological ways in which the gut may affect clinical outcomes in COVID-19 disease:
- Ileal epithelial cells have high ACE2 expression rates (~30% ACE2-positive cells). [17] COVID-19 leads to the infection of ileal cells followed by expression of the viral nucleocapsid protein, meaning SARS-CoV-2 may spread from infected to uninfected cells in the GI tract, generating mucosal immune cell activation.
- Viraemia following lung infection may occur in approximately 1% of cases, leading to a secondary attack of SARS-CoV2 on ACE2 target organs, including the gut and kidney [46].
- Crosstalk between gut microbiota and the lungs contribute to maintain host homeostasis and disease development in association with the immune system, where the distal (gut) immune modulation during respiratory illness is mediated by gut microbiota. Similarly, lung microbiota influences both respiratory and gastrointestinal health [47]. This gut-lung interaction (gut-lung axis) may influence COVID-19 severity [48,49].On the luminal surface of intestinal epithelial cells, ACE2 associates with the neutral amino acid transporter B0AT1 and regulates intestinal microflora. SARS-CoV-2 infection of the GI tract itself alters the levels of ACE2 at the brush border, leading to dysbiosis and inflammation [50].
Multiple studies, (meta-analysis included) have reported a positive impact of different probiotics on diminishing the incidence of respiratory tract infection in different clinical scenarios, including viral respiratory tract infections and ventilator-associated pneumonia, but the fact that not all of the probiotics may be beneficial in the same way and extent to reduce the risk of respiratory infection should be noted [51].
Even when the mechanisms by which probiotics may contribute to improve clinical outcomes in COVID-19 patients have already been described, and include enhancement of the gut epithelial barrier, competition with pathogens for nutrients and adhesion sites, production of anti-microbial substances and immunomodulation [52,53], the exact timing, contraindications and expected clinical benefits of probiotic administration in COVID-19 patients remains to be proved in randomized clinical trials.
In persons living with Inflammatory Bowel Disease (IBD), specific risk factors for developing COVID-19 are yet to be determined. As GI tract permeability may be higher in IBD patients with higher expression of ACE2 in the inflamed bowel, there is a theoretical increased risk of SARS-CoV-2 infection via the gut, but there is no current evidence of increased infection rates or worse clinical outcomes of COVID-19 in persons living with IBD; the reported incidence of COVID-19 in the IBD population in a pooled cohort was approximately 0.3% [54,55].
Medications used in the management of IBD may increase the risk of respiratory tract infections to varying degrees. However, theoretically, there may also be some benefit with certain immunosuppressive medications by reducing the occurrence of a cytokine storm resulting in ARDS [56,57].
By contrast, Burgeño et al. reported that expression of ACE2 and TMPRSS2 was not higher in ileum and colon samples from IBD patients. Furthermore, anti-tumor necrosis factor drugs, vedolizumab, ustekinumab, and steroids were linked to a diminished expression of ACE2 in IBD patients [56,57].
Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) is a large, international registry created to monitor outcomes of IBD patients with confirmed COVID-19. Among 1439 registered cases, 7.8% had severe COVID-19. Using anti-TNF monotherapy as a reference arm, thiopurine monotherapy and anti-TNF plus thiopurine combination therapy were associated with worse clinical outcomes. Any mesalamine/sulfasalazine compared with no mesalamine/sulfasalazine use was associated with an increased risk. Interleukin-12/23 and integrin antagonists were not associated with a significantly different risk than TNF antagonist monotherapy [58].
However, it may not be advisable to withdraw thiopurines in younger adults without additional risk factors for poor COVID-19 outcomes. In older and higher-risk patients, the totality of risk and benefit of thiopurine therapy should be considered, taking into account not only COVID-19 but also well-known risks such as lymphoma, as well as the significant risk of disease flare on withdrawal of thiopurine monotherapy and an increased risk of immunogenicity and hence drug failure where patients are on combination therapy [59].
The incidence of surgical abdomen in COVID-19 patients remains to be described. SARS-CoV2-nduced mucosal injury, hyper-immunity and over-inflammation leading to hypercoagulability and regional ischemia of the gut may lead to different surgical-like clinical presentations, including diffuse acute abdominal pain, enteritis, pseudoappendicitis, appendicitis, and acute mesenteric ischemia [60,61,62,63,64]. Even when COVID-19 has been reported to be associated with intussuception and mesenteric lymphoid hyperplasia (most commonly in children), it has also been reported in adults and must be taken into account in adult patients [65,66,67].
Even when discarding abdominal surgical pathology must be a priority in patients presenting with acute abdominal pain, it should be remembered that COVID-19-related lung base abnormalities, including peripheral and subpleural ground-glass opacities with nodular configuration, may present clinically as abdominal pain [68,69].
7. Vaccine-Related Gastrointestinal Symptoms
Even when the available COVID-19 vaccines offer very good safety profiles, a variety of gastrointestinal adverse events have been described and must be taken into account (Table 1):
- Among patients who received COVID-19 mRNA vaccines, gastrointestinal adverse events were the third most common type of adverse events after immunization, being reported in 25.54% of patients. Among the gastrointestinal symptoms, nausea represented 56.41% of symptoms, followed by vomiting (14.7%) and diarrhea (14.13%) [70].
- Regarding the Ad26.COV2.S vaccine, nausea was the third most common systemic adverse effect, being present in 14.2% of patients [71].
8. Conclusions
Even when respiratory symptoms remain the most common clinical presentation, the multisystemic nature of COVID-19 disease must be always considered. In particular, gastrointestinal manifestations must always be intentionally sought and documented.
The interaction between viral receptor expression patterns, direct cytopathic injury, inflammatory damage, ischemia, multiorganic crosstalk, therapeutic maneuvers and pharmacologic effects give place to a wide range of clinical presentations.
In patients with gastrointestinal comorbidities, a careful monitoring of baseline pathologies and drug-related toxicities and interactions must be closely surveilled, given that the exact expected prognostic significance of the intersectionality of COVID-19 disease and different gastrointestinal pathologies remains to be fully understood.
Information regarding the long-term prognostic implications of gastrointestinal manifestations remains to be described, as well as the expected gastrointestinal manifestation in the clinical course of a second or a post-vaccination COVID-19 episode.
Until now there has been no specific and effective antiviral treatment for SARS-CoV2; consequently, pharmacological management of gastrointestinal manifestations of COVID-19 remains largely symptomatic: cautious use of anti-emetics to prevent QT prolongation, especially in patients taking chloroquine or azithromycin, may be used to treat nausea. Hydration and racecadotril may be used to treat diarrhoea (this being preferred over loperamide). The specific recommendations for probiotic use in COVID-19 patients, as well as the clinical safety of PPI use in the face of COVID-19 pandemics, remains to be described [76,77].
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| COVID-19 | Coronavirus disease 2019. |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2. |
| SARS | Severe Acute Respiratory Syndrome. |
| ACE2 | Angiotensin-converting enzyme 2. |
| TMPRSS2 | Transmembrane protease, serine 2. |
| KIM1 | kidney injury molecule-1. |
| RBD | Receptor-binding domain. |
| CDC | Center for Disease Control and Prevention. |
| Ig | Immunoglobulin. |
| IgV | Immunoglobulin variable. |
| ALT | Alanine Aminotransferase. |
| AST | Aspartate Aminotransferase. |
| GI | Gastrointestinal. |
| PPIs | proton pump inhibitors. |
| H2Ras | H2 receptor antagonists. |
| AIH | autoimmune hepatitis. |
| CLD | chronic liver disease. |
| ICU | intensive care unit. |
| HAV | Hepatitis A virus. |
| HBV | Hepatitis B virus. |
| HCV | Hepatitis C virus. |
| IFN-γ | Interferon-gamma |
| IBD | Inflammatory Bowel Disease. |
| ARDS | Acute respiratory distress syndrome. |
| TNF | Tumoral necrosis factor. |
References
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 23, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 23 October 2021).
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Havers, F.P.; Reed, C.; Lim, T.; Montgomery, J.M.; Klena, J.D.; Hall, A.J.; Fry, A.M.; Cannon, D.L.; Chiang, C.-F.; Gibbons, A.; et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, March 23–May 12, 2020. JAMA Intern. Med. 2020, 180, 1576. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; De Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Yang, C.; Zhang, Y.; Zeng, X.; Chen, H.; Chen, Y.; Yang, D.; Shen, Z.; Wang, X.; Liu, X.; Xiong, M.; et al. Kidney injury molecule-1 is a potential receptor for SARS-CoV-2. J. Mol. Cell Biol. 2021, 13, 185–196. [Google Scholar] [CrossRef]
- Wan, C.; Zhang, C. Kidney injury molecule-1: A novel entry factor for SARS-CoV-2. J. Mol. Cell Biol. 2021, 13, 159–160. [Google Scholar] [CrossRef]
- Kerget, B.; Kerget, F.; Aksakal, A.; Aşkın, S.; Uçar, E.Y.; Sağlam, L. Evaluation of the relationship between KIM-1 and suPAR levels and clinical severity in COVID-19 patients: A different perspective on suPAR. J. Med. Virol. 2021, 93, 5568–5573. [Google Scholar] [CrossRef]
- Oran, A.D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic: A Systematic Review. Ann. Intern. Med. 2021, 174, 655–662. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; Felix, S.E.B.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance—United States, January 22–May 30, 2020. Morbidity and mortality weekly report. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Lian, J.-S.; Hu, J.-H.; Gao, J.; Zheng, L.; Zhang, Y.-M.; Hao, S.-R.; Jia, H.-Y.; Cai, H.; Zhang, X.-L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parasa, S.; Desai, M.; Chandrasekar, V.T.; Patel, H.K.; Kennedy, K.F.; Roesch, T.; Spadaccini, M.; Colombo, M.; Gabbiadini, R.; Artifon, E.L.A.; et al. Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients with Coronavirus Disease 2019: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2011335. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Sarver, D.C.; Wong, G.W. Obesity alters Ace2 and Tmprss2 expression in lung, trachea, and esophagus in a sex-dependent manner: Implications for COVID-19. Biochem. Biophys. Res. Commun. 2020, 538, 92–96. [Google Scholar] [CrossRef]
- Janowitz, T.; Gablenz, E.; Pattinson, D.; Wang, T.C.; Conigliaro, J.; Tracey, K.; Tuveson, D. Famotidine use and quantitative symptom tracking for COVID-19 in non-hospitalised patients: A case series. Gut 2020, 69, 1592–1597. [Google Scholar] [CrossRef]
- Almario, C.V.; Chey, W.D.; Spiegel, B.M. Increased Risk of COVID-19 Among Users of Proton Pump Inhibitors. Am. J. Gastroenterol. 2020, 115, 1707–1715. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.M.F.; Frühbeck, G. Benefits of Bariatric Surgery Prior to SARS-CoV-2 Infection in Modulating the Response to COVID-19. Obesity 2020, 29, 19. [Google Scholar] [CrossRef]
- Lassen, P.B.; Poitou, C.; Genser, L.; Marchelli, F.; Aron-Wisnewsky, J.; Ciangura, C.; Jacques, F.; Moreau, P.; Oppert, J.; Clément, K.; et al. COVID-19 and its Severity in Bariatric Surgery-Operated Patients. Obesity 2020, 29, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.P.; Patel, P.A.; Vunnam, R.R.; Hewlett, A.T.; Jain, R.; Jing, R.; Vunnam, S.R. Gastrointestinal, hepatobiliary, and pancreatic manifestations of COVID-19. J. Clin. Virol. 2020, 128, 104386. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients with Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruni, A.; Garofalo, E.; Zuccalà, V.; Currò, G.; Torti, C.; Navarra, G.; De Sarro, G.; Navalesi, P.; Longhini, F.; Ammendola, M. Histopathological findings in a COVID-19 patient affected by ischemic gangrenous cholecystitis. World J. Emerg. Surg. WJES 2020, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ying, M.; Lu, B.; Pan, J.; Lu, G.; Zhou, S.; Wang, D.; Li, L.; Shen, J.; Shu, J. COVID-19 with acute cholecystitis: A case report. BMC Infect. Dis. 2020, 20, 1–4. [Google Scholar] [CrossRef]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and the liver. J. Hepatol. 2020, 73, 1231–1240. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.-Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Shi, L.; Wang, Y. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Chau, T.N.; Lee, K.C.; Yao, H.; Tsang, T.Y.; Chow, T.C.; Yeung, Y.C.; Choi, K.W.; Tso, Y.K.; Lau, T.; Lai, S.T.; et al. SARS-associated viral hepatitis caused by a novel coronavirus: Report of three cases. Hepatology 2004, 39, 302–310. [Google Scholar] [CrossRef]
- Velasco, J.V.-R.; García-Jiménez, E.; Remes-Troche, J. Manifestaciones hepáticas y repercusión en el paciente cirrótico de COVID-19. Rev. Gastroenterol. Mex. 2020, 85, 303–311. [Google Scholar] [CrossRef]
- Xu, L.; Ying, S.; Hu, J.; Wang, Y.; Yang, M.; Ge, T.; Huang, C.; Xu, Q.; Zhu, H.; Chen, Z.; et al. Pneumonia in patients with cirrhosis: Risk factors associated with mortality and predictive value of prognostic models. Respir. Res. 2018, 19, 242. [Google Scholar] [CrossRef]
- Zou, B.; Yeo, Y.H.; Jeong, D.; Sheen, E.; Park, H.; Nguyen, P.; Hsu, Y.-C.; Garcia, G.; Nguyen, M.H. Higher mortality and hospital charges in patients with cirrhosis and acute respiratory illness: A population-based study. Sci. Rep. 2018, 8, 9969. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef]
- Marjot, T.; Buescher, G.; Sebode, M.; Barnes, E.; Barritt, A.S.; Armstrong, M.J.; Baldelli, L.; Kennedy, J.; Mercer, C.; Ozga, A.-K.; et al. SARS-CoV-2 infection in patients with autoimmune hepatitis. J. Hepatol. 2021, 74, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Webb, G.J.; Marjot, T.; Cook, J.A.; Aloman, C.; Armstrong, M.J.; Brenner, E.J.; Catana, M.A.; Cargill, T.; Dhanasekaran, R.; García-Juárez, I.; et al. Outcomes following SARS-CoV-2 infection in liver transplant recipients: An international registry study. Lancet Gastroenterol. Hepatol. 2020, 5, 1008–1016. [Google Scholar] [CrossRef]
- Sarialioğlu, F.; Belen, F.B.; Hayran, K.M. Hepatitis A susceptibility parallels high COVID-19 mortality. Turk. J. Med. Sci. 2021, 51, 382–384. [Google Scholar] [CrossRef]
- Sarialioglu, F.; Apak, F.B.B.; Haberal, M. Can Hepatitis A Vaccine Provide Protection Against COVID-19? Exp. Clin. Transplant. 2020, 18, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Yuan, J.; Long, Q.; Hu, J.; Deng, H.; Zhao, Z.; Chen, J.; Lu, M.; Huang, A. Patients with SARS-CoV-2 and HBV co-infection are at risk of greater liver injury. Genes Dis. 2020, 8, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Fang, M.; Li, S.; Wu, L.; Gao, B.; Gao, H.; Ran, X.; Bian, Y.; Li, R.; Ling, J.; et al. Characteristics of Liver Function in Patients With SARS-CoV-2 and Chronic HBV Coinfection. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2021, 19, 597–603. [Google Scholar] [CrossRef]
- Liu, J.; Wang, T.; Cai, Q.; Sun, L.; Huang, D.; Zhou, G.; He, Q.; Wang, F.; Liu, L.; Chen, J. Longitudinal changes of liver function and hepatitis B reactivation in COVID-19 patients with pre-existing chronic hepatitis B virus infection. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2020, 50, 1211–1221. [Google Scholar] [CrossRef]
- Butt, A.A.; Yan, P. Rates and characteristics of SARS-CoV-2 infection in persons with hepatitis C virus infection. Liver Int. Off. J. Int. Assoc. Study Liver 2020, 41, 76–80. [Google Scholar] [CrossRef]
- Villar, L.M.; de Paula, V.S.; Pinto, L.C.M.; Marques, B.C.L.; da Costa, V.D.; da Silva, L.L.; Santos, A.C.; Nascimento, G.P.D.; Miguel, J.C.; Mendonça, A.C.D.F.; et al. Clinical and laboratory characteristics of hepatitis C and COVID-19 coinfection: Prolonged RNA shedding in nonhospitalized case. Clin. Case Rep. 2021, 9. [Google Scholar] [CrossRef]
- Butt, A.A.; Yan, P.; Chotani, R.A.; Shaikh, O.S. Mortality is not increased in SARS-CoV-2 infected persons with hepatitis C virus infection. Liver Int. Off. J. Int. Assoc. Study Liver 2021, 41, 1824–1831. [Google Scholar] [CrossRef]
- Neurath, M.F. COVID-19 and immunomodulation in IBD. Gut 2020, 69, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Dumas, A.; Bernard-Raichon, L.; Poquet, Y.; Lugo, G.; Neyrolles, O. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell Microbiol. 2018, 20, e12966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aktas, B.; Aslim, B. Gut-lung axis and dysbiosis in COVID-19. Turk. J. Boil. 2020, 44, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Zeppa, S.D.; Agostini, D.; Piccoli, G.; Stocchi, V.; Sestili, P. Gut Microbiota Status in COVID-19: An Unrecognized Player? Front. Cell Infect. Microbiol. 2020, 10, 576551. [Google Scholar] [CrossRef]
- Stevens, B.R.; Ellory, J.C.; Preston, R.L. B0AT1 Amino Acid Transporter Complexed with SARS-CoV-2 Receptor ACE2 Forms a Heterodimer Functional Unit: In Situ Conformation Using Radiation Inactivation Analysis. Function 2021, 2, zqab027. [Google Scholar] [CrossRef]
- Baud, D.; Dimopoulou Agri, V.; Gibson, G.R.; Reid, G.; Giannoni, E. Using Probiotics to Flatten the Curve of Coronavirus Disease COVID-2019 Pandemic. Front. Public Health 2020, 8, 186. [Google Scholar] [CrossRef] [PubMed]
- Brito, M.B.; Diaz, J.P.; Muñoz-Quezada, S.; Llorente, C.G.; Gil, A. Probiotic Mechanisms of Action. Ann. Nutr. Metab. 2012, 61, 160–174. [Google Scholar] [CrossRef]
- de Oliveira, G.L.V.; Oliveira, C.N.S.; Pinzan, C.F.; de Salis, L.V.V.; Cardoso, C.R.D.B. Microbiota Modulation of the Gut-Lung Axis in COVID-19. Front. Immunol. 2021, 12, 635471. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.; Fatima, R.; Haghbin, H.; Lee-Smith, W.; Nawras, A. The Incidence and Outcomes of COVID-19 in IBD Patients: A Rapid Review and Meta-analysis. Inflamm. Bowel Dis. 2020, 26, e132–e133. [Google Scholar] [CrossRef] [PubMed]
- Al-Ani, A.; Prentice, R.; Rentsch, C.; Johnson, D.; Ardalan, Z.; Heerasing, N.; Garg, M.; Campbell, S.; Sasadeusz, J.; Macrae, F.; et al. Review article: Prevention, diagnosis and management of COVID-19 in the IBD patient. Aliment. Pharmacol. Ther. 2020, 52, 54–72. [Google Scholar] [CrossRef]
- Brenner, E.J.; Ungaro, R.; Colombel, J.F.; Kappelman, M.D. Secure-IBD Database Public Data Update 2020. Available online: www.covidibd.org/current-data (accessed on 31 August 2021).
- Burgueño, J.F.; Reich, A.; Hazime, H.; Quintero, M.A.; Fernandez, I.; Fritsch, J.; Santander, A.M.; Brito, N.; Damas, O.M.; Deshpande, A.; et al. Expression of SARS-CoV-2 Entry Molecules ACE2 and TMPRSS2 in the Gut of Patients With IBD. Inflamm. Bowel Dis. 2020, 26, 797–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungaro, R.C.; Brenner, E.J.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Steinwurz, F.; et al. Effect of IBD medications on COVID-19 outcomes: Results from an international registry. Gut 2020, 70, 725–732. [Google Scholar] [CrossRef]
- Lees, C.W.; Irving, P.M.; Beaugerie, L. COVID-19 and IBD drugs: Should we change anything at the moment? Gut 2020, 70, 632–634. [Google Scholar] [CrossRef]
- Ahmed, A.O.E.; Badawi, M.; Ahmed, K.; Mohamed, M.F.H. Case Report: COVID-19 Masquerading as an Acute Surgical Abdomen. Am. J. Trop. Med. Hyg. 2020, 103, 841–843. [Google Scholar] [CrossRef]
- Kecler-Pietrzyk, A.; Orsi, G.; Carthy, J.; Torreggiani, W.C. Enteritis and Severe Abdominal Pain as the First Presentation of Covid-19. Ir. Med. J. 2020, 113, 102. [Google Scholar] [PubMed]
- Suwanwongse, K.; Shabarek, N. Pseudo-Appendicitis in an Adolescent with COVID-19. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Malbul, K.; Katwal, S.; Maharjan, S.; Shrestha, S.; Dhital, R.; Rajbhandari, A.P. Appendicitis as a presentation of COVID-19: A case report. Ann. Med. Surg. 2021, 69, 102719. [Google Scholar] [CrossRef] [PubMed]
- Pirola, L.; Palermo, A.; Mulinacci, G.; Ratti, L.; Fichera, M.; Invernizzi, P.; Viganò, C.; Massironi, S. Acute mesenteric ischemia and small bowel imaging findings in COVID-19: A comprehensive review of the literature. World J. Gastrointest. Surg. 2021, 13, 702–716. [Google Scholar] [CrossRef] [PubMed]
- Giovanni, J.E.; Hrapcak, S.; Melgar, M.; Godfred-Cato, S. Global Reports of Intussusception in Infants With SARS-CoV-2 Infection. Pediatr. Infect. Dis. J. 2020, 40, e35–e36. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Hartman, L.; Navarro, Y.J.S.; Rossini, C.J.; Burdett, C.; Pennell, C. Pediatric Covid-19 mesenteric lymphoid hyperplasia associated intussusception: A case report and literature review. J. Pediatr. Surg. Case Rep. 2021, 73, 101988. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.M.; Sabbota, A.L. Right hemicolectomy for ileocolonic intussusception in an adult with active COVID-19 infection: A case report. J. Surg. Case Rep. 2021, 2021, rjab205. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.; Chang, P.J.; Jarou, Z.J.; Paushter, D.M.; Harmath, C.B.; Ben Arevalo, J.; Dachman, A. Lung Base Findings of Coronavirus Disease (COVID-19) on Abdominal CT in Patients with Predominant Gastrointestinal Symptoms. Am. J. Roentgenol. 2020, 215, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Pautrat, K.; Chergui, N. SARS-CoV-2 infection may result in appendicular syndrome: Chest CT scan before appendectomy. J. Visc. Surg. 2020, 157, S63–S64. [Google Scholar] [CrossRef]
- Mauro, A.; De Grazia, F.; Lenti, M.V.; Penagini, R.; Frego, R.; Ardizzone, S.; Savarino, E.; Radaelli, F.; Bosani, M.; Orlando, S.; et al. Upper gastrointestinal bleeding in COVID-19 inpatients: Incidence and management in a multicenter experience from Northern Italy. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101521. [Google Scholar] [CrossRef]
- Chen, G.; Li, X.; Sun, M.; Zhou, Y.; Yin, M.; Zhao, B.; Li, X. COVID-19 mRNA Vaccines Are Generally Safe in the Short Term: A Vaccine Vigilance Real-World Study Says. Front. Immunol. 2021, 12, 669010. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.-S.; Hung, I.F.; Chan, P.P.; Lung, K.; Tso, E.; Liu, R.; Ng, Y.; Chu, M.Y.; Chung, T.W.; Tam, A.R.; et al. Gastrointestinal manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples from a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Siddique, S.; Singh, S.; Altayar, O.; Caliendo, A.M.; Davitkov, P.; Feuerstein, J.D.; Kaul, V.; Lim, J.K.; Mustafa, R.A.; et al. AGA Rapid Review and Guideline for SARS-CoV2 Testing and Endoscopy Post-Vaccination: 2021 Update. Gastroenterology 2021, 161, 1011–1029.e11. [Google Scholar] [CrossRef]
- Perisetti, A.; Gajendran, M.; Boregowda, U.; Bansal, P.; Goyal, H. COVID-19 and gastrointestinal endoscopies: Current insights and emergent strategies. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2020, 32, 715–722. [Google Scholar] [CrossRef] [Green Version]
- Hunt, R.H.; East, J.E.; Lanas, A.; Malfertheiner, P.; Satsangi, J.; Scarpignato, C.; Webb, G.J. COVID-19 and Gastrointestinal Disease. Implications for the Gastroenterologist. Dig. Dis. 2020, 39, 119–139. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Gastrointestinal involvement in COVID-19 disease: After SARS-CoV-2 -host interaction with host’s ACE2, KIM-1 and/or KIM-1, clinical findings result from infection of epithelial cells, inflammation, (including immune cells activation and/or cytokine storm) and secondary damage including ischemic insult. ACE2: Angiotensin-converting enzyme 2. TMPRSS2: Transmembrane protease serine 2. KIM1: kidney injury molecule. AKI: Acute Kidney Injury. MOF: Multiple Organ Failure. TNF: Tumoral necrosis factor.
Figure 1.
Gastrointestinal involvement in COVID-19 disease: After SARS-CoV-2 -host interaction with host’s ACE2, KIM-1 and/or KIM-1, clinical findings result from infection of epithelial cells, inflammation, (including immune cells activation and/or cytokine storm) and secondary damage including ischemic insult. ACE2: Angiotensin-converting enzyme 2. TMPRSS2: Transmembrane protease serine 2. KIM1: kidney injury molecule. AKI: Acute Kidney Injury. MOF: Multiple Organ Failure. TNF: Tumoral necrosis factor.


{kind=link}
Table 1.
Gastroenterological consideration for clinical practice in COVID-19 patients.
| Epidemiological risk. | Questions remain regarding fecal-oral transmission. SARS-CoV-2 RNA can be detected in the endoscopic specimens from the oesophagus, stomach, duodenum and rectum [72]. Substantial amounts of SARS-CoV-2 RNA can be detected in stool specimens from COVID-19 patients [73]. SARS-CoV-2 RNA has been detected in the sewage of hospitals treating patients with SACOVID-19 disease and the virus remained infectious up to 2 weeks in sewage water [74]. |
| Diagnostic procedures | COVID-19 could possibly be transmitted by endoscopes; theoretically due to contact with mucous membranes and body fluids. GI societies have advocate for rescheduling non-urgent procedures and perform only emergent or urgent ones. Pre-endoscopy screening was initially recommended; upgraded guidelines state that, with widespread vaccination of health care workers and the general population, pre-endoscopy screening may not always be necessary, and placed a high value on minimizing additional delays in patient care [74,75]. |
| Current medication history | Plausible clinical benefit with famotidine in COVID-19 cases [19]. Impact of acid suppression on risk for COVID-19 is unknown so far [20]. Immunosupression schedule in patients with IBD must be reassessed on a personalized basis [55]. |
| Expected clinical course among patients with known comorbidities. | Among patients with bariatric surgery history and COVID-19 disease 1.6% fatality rate. Persistent type 2 diabetes and higher percent weight loss since bariatric surgery are associated with severe COVID-19 [22]. Mortality among patients with COVID-19 and cirrhosis has been reported to be 32%, being older age, higher Child-Pugh and alcohol related liver disease the main factors associated with death [35]/ Similar hospitalization rates, ICU admission and death between patients with AIH and non-AIH CLD [36]. Among persons living with chronic HBV infection, it has been reported that there is no statistically significant differences in the median time to SARS-CoV2 clearance or progression to severe COVID-19 disease [42]. COVID-19-HCV coinfected patients have been reported to have higher hospitalization rates, but ICU admission and mortality are similar between those with and without HCV infection [45]. No current evidence of increased infection rates or worse disease severity of COVID-19 in IBD patients [54]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mucino-Bermejo, M.-J. COVID-19 and the Gastrointestinal Tract. Gastroenterol. Insights 2021, 12, 394-404. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12040038
AMA Style
Mucino-Bermejo M-J. COVID-19 and the Gastrointestinal Tract. Gastroenterology Insights. 2021; 12(4):394-404. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12040038
Chicago/Turabian StyleMucino-Bermejo, María-Jimena. 2021. "COVID-19 and the Gastrointestinal Tract" Gastroenterology Insights 12, no. 4: 394-404. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12040038