
Potential Misdiagnosis between COVID-19 and Dengue Infection Using Rapid Serological Test

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Sample Collection from COVID-19 Patients
2.3. Serological Test
2.4. Molecular Test
3. Results
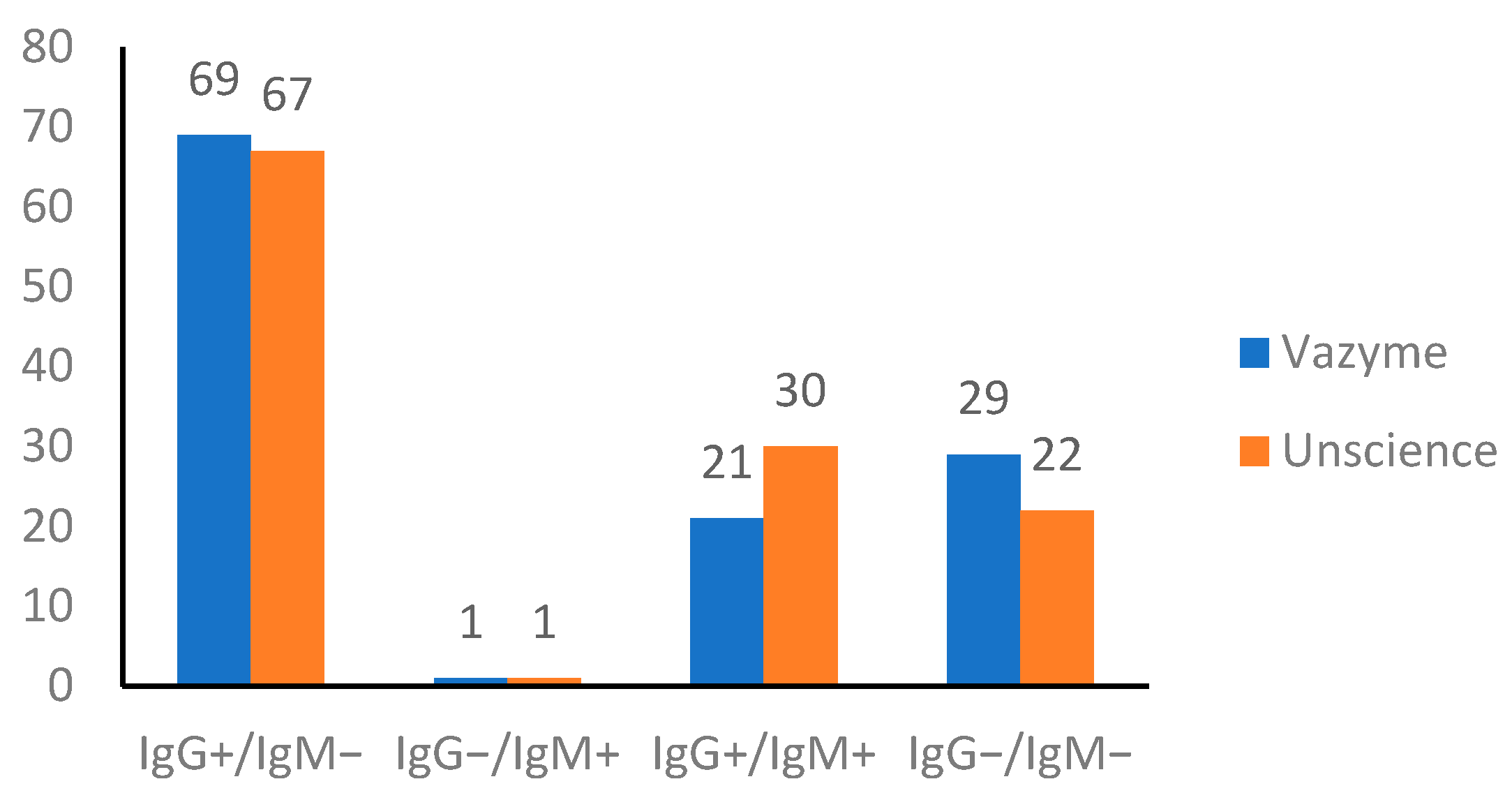
3.1. Serological SARS-CoV-2 Test
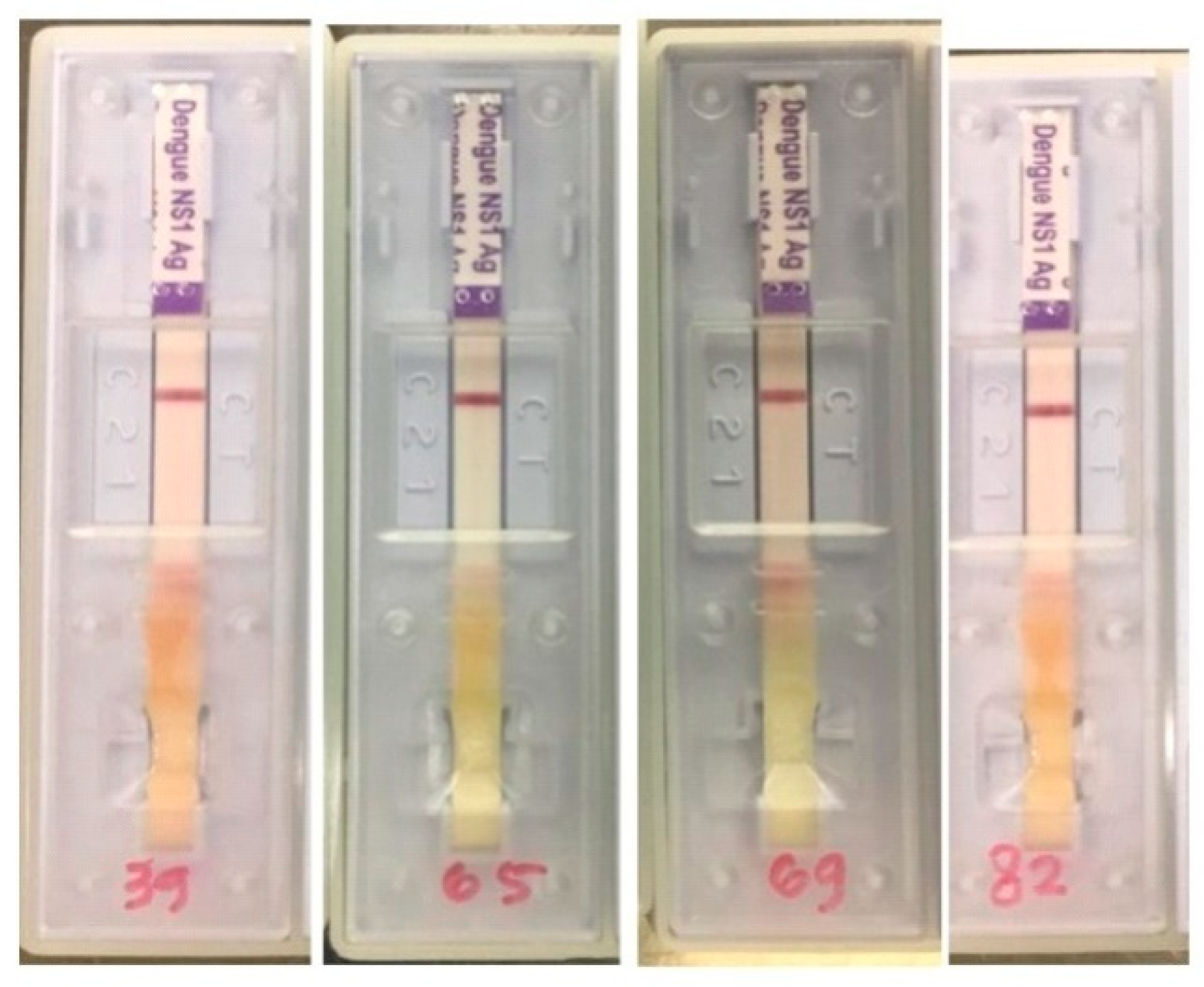
3.2. Serological Dengue and NS1 Tests
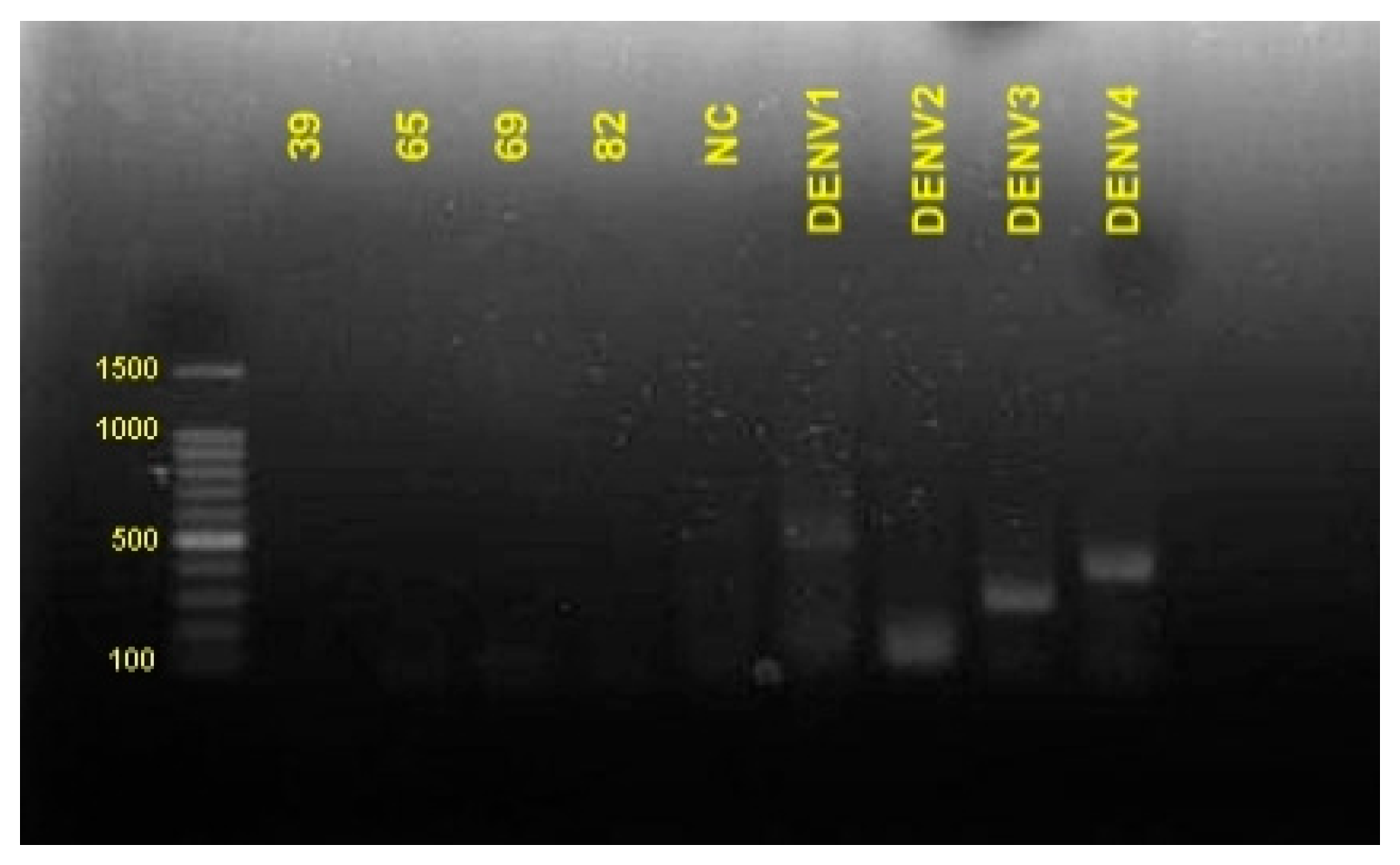
3.3. Amplification of DENV Serotype
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus Disease 2019 (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 6 March 2021).
- Kementrian, K.R.I. Situasi Terkini Perkembangan Novel Coronavirus (COVID-19). Available online: https://covid19.kemkes.go.id/situasi-infeksi-emerging/situasi-terkini-perkembangan-coronavirus-disease-covid-19-04-maret (accessed on 6 March 2021).
- Yan, G.; Lee, C.K.; Lam, L.T.M.; Yan, B.; Chua, Y.X.; Lim, A.Y.N.; Phang, K.F.; Kew, G.S.; Teng, H.; Ngai, C.H.; et al. Covert COVID-19 and false-positive dengue serology in Singapore. Lancet Infect. Dis. 2020, 20, 536. [Google Scholar] [CrossRef] [Green Version]
- Joob, B.; Wiwanitkit, V. COVID-19 in medical personnel: Observation from Thailand. J. Hosp. Infect. 2020, 104, 453. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (CoVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masyeni, S.; Santoso, M.S.; Widyaningsih, P.D.; Asmara, D.W.; Nainu, F.; Harapan, H.; Sasmono, R.T. Serological cross-reaction and coinfection of dengue and COVID-19 in Asia: Experience from Indonesia. Int. J. Infect. Dis. 2021, 102, 152–154. [Google Scholar] [CrossRef]
- Setianingsih, T.Y.; Wiyatno, A.; Hartono, T.S.; Hindawati, E.; Rosamarlina; Dewantari, A.K.; Myint, K.S.; Lisdawati, V.; Safari, D. Detection of multiple viral sequences in the respiratory tract samples of suspected Middle East respiratory syndrome coronavirus patients in Jakarta, Indonesia 2015–2016. Int. J. Infect. Dis. 2019, 86, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Kementerian Kesehatan, R.I. Informasi Singkat DBD 2020. Available online: https://sehatnegeriku.kemkes.go.id/baca/umum/20201203/2335899/data-kasus-terbaru-dbd-indonesia/ (accessed on 6 March 2021).
- Criado, P.R.; Pagliari, C.; Carneiro, F.R.O.; Quaresma, J.A.S. Lessons from dermatology about inflammatory responses in Covid-19. Rev. Med. Virol. 2020, 30. [Google Scholar] [CrossRef]
- Henrina, J.; Putra, I.C.S.; Lawrensia, S.; Handoyono, Q.F.; Cahyadi, A. Coronavirus Disease of 2019: A Mimicker of Dengue Infection? SN Compr. Clin. Med. 2020, 2, 1109–1119. [Google Scholar] [CrossRef]
- Mulyatno, K.C.; Kotaki, T.; Yotopranoto, S.; Rohmah, E.A.; Churotin, S.; Sucipto, T.H.; Amarullah, I.H.; Wardhani, P.; Soegijanto, S.; Kameoka, M. Detection and serotyping of dengue viruses in aedes aegypti and aedes albopictus (Diptera: Culicidae) collected in Surabaya, Indonesia from 2008 to 2015. Jpn. J. Infect. Dis. 2018, 71, 58–61. [Google Scholar] [CrossRef] [Green Version]
- Vazyme biotech. 2019-nCoV IgG/IgM Detection Kit (Colloidal Gold-Based); Vazyme Biotech: Nanjing, China, 2020. [Google Scholar]
- Wuhan UNscience Biotechnology Co., Ltd. COVID-19 IgG/IgM Rapid Test; Wuhan UNscience Biotechnology: Wuhan, China, 2020. [Google Scholar]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Staines, H.M.; Kirwan, D.E.; Clark, D.J.; Adams, E.R.; Augustin, Y.; Byrne, R.L.; Cocozza, M.; Cubas-Atienzar, A.I.; Cuevas, L.E.; Cusinato, M.; et al. Igg seroconversion and pathophysiology in severe acute respiratory syndrome coronavirus 2 infection. Emerg. Infect. Dis. 2021, 27, 85–91. [Google Scholar] [CrossRef]
- Guy, B.; Ooi, E.E.; Ramos-castañeda, J.; Thomas, S.J. When Can One Vaccinate with a Live Vaccine after Wild-Type Dengue Infection? Vaccines 2020, 8, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashshi, A.M.; Alghamdi, S.; El-Shemi, A.G.; Almdani, S.; Refaat, B.; Mohamed, A.M.; Ghazi, H.O.; Azhar, E.I.; Al-Allaf, F.A. Seroprevalence of asymptomatic dengue virus infection and its antibodies among healthy/eligible saudi blood donors: Findings from holy makkah city. Virol. Res. Treat. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Deng, Y.; Jing, Q.; Chen, X.; Du, Z.; Liang, T.; Yang, Z.; Zhang, D.; Hao, Y. Dengue infection spectrum in Guangzhou: A cross-sectional seroepidemiology study among community residents between 2013 and 2015. Int. J. Environ. Res. Public Health 2018, 15, 1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasitsirikul, W.; Pongpirul, K.; Pongpirul, W.A.; Panitantum, N.; Ratnarathon, A.C.; Hemachudha, T. Nurse infected with Covid-19 from a provisional dengue patient. Emerg. Microbes Infect. 2020, 9, 1354–1355. [Google Scholar] [CrossRef] [PubMed]
- Kembuan, G.J. Dengue serology in Indonesian COVID-19 patients: Coinfection or serological overlap? IDCases 2020, 22, e00927. [Google Scholar] [CrossRef] [PubMed]
- Spinicci, M.; Bartoloni, A.; Mantella, A.; Zammarchi, L.; Rossolini, G.M.; Antonelli, A. Low risk of serological cross-reactivity between dengue and COVID-19. Mem. Inst. Oswaldo Cruz 2020, 115. [Google Scholar] [CrossRef]
- Santoso, M.S.; Masyeni, S.; Haryanto, S.; Yohan, B.; Hibberd, M.L.; Sasmono, R.T. Assessment of dengue and COVID-19 antibody rapid diagnostic tests cross-reactivity in Indonesia. Virol. J. 2021, 18, 1–5. [Google Scholar] [CrossRef]
- Yow, K.S.; Aik, J.; Tan, E.Y.M.; Ng, L.C.; Lai, Y.L. Rapid diagnostic tests for the detection of recent dengue infections: An evaluation of six kits on clinical specimens. PLoS ONE 2021, 16. [Google Scholar] [CrossRef]
- Lustig, Y.; Keler, S.; Kolodny, R.; Ben-Tal, N.; Atias-Varon, D.; Shlush, E.; Gerlic, M.; Munitz, A.; Doolman, R.; Asraf, K.; et al. Potential Antigenic Cross-reactivity Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Dengue Viruses. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nath, H.; Mallick, A.; Roy, S.; Sukla, S.; Basu, K.; De, A.; Biswas, S. Dengue antibodies can cross-react with SARS-CoV-2 and vice versa-antibody detection kits can give false-positive results for both viruses in regions where both COVID-19 and Dengue co-exist. MedRxiv 2020. [Google Scholar] [CrossRef]
- Kotaki, T.; Yamanaka, A.; Mulyatno, K.C.; Churrotin, S.; Sucipto, T.H.; Labiqah, A.; Ahwanah, N.L.F.; Soegijanto, S.; Kameoka, M.; Konishi, E. Divergence of the dengue virus type 2 Cosmopolitan genotype associated with two predominant serotype shifts between 1 and 2 in Surabaya, Indonesia, 2008–2014. Infect. Genet. Evol. 2016, 37, 88–93. [Google Scholar] [CrossRef]
- Wardhani, P.; Aryati, A.; Yohan, B.; Trimarsanto, H.; Setianingsih, T.Y.; Puspitasari, D.; Arfijanto, M.V.; Bramantono, B.; Suharto, S.; Sasmono, R.T. Clinical and virological characteristics of dengue in Surabaya, Indonesia. PLoS ONE 2017, 12, e0178443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bicudo, N.; Bicudo, E.; Costa, J.D.; Castro, J.A.L.P.; Barra, G.B. Co-infection of SARS-CoV-2 and dengue virus: A clinical challenge. Braz. J. Infect. Dis. 2020, 24, 452–454. [Google Scholar] [CrossRef]
- Figueredo, M.S.; Amâncio, T.A.; Salvatierra, J.A.; de Brito, B.B.; da Silva, F.A.F.; Queiroz, D.M.M.; de Melo, F.F. COVID-19 and dengue coinfection in Brazil. World J. Clin. Infect. Dis. 2020, 10, 51–54. [Google Scholar] [CrossRef]
- Nasomsong, W.; Luvira, V.; Phiboonbanakit, D. Case report: Dengue and COVID-19 coinfection in Thailand. Am. J. Trop. Med. Hyg. 2021, 104, 487–489. [Google Scholar] [CrossRef] [PubMed]
- Verduyn, M.; Allou, N.; Gazaille, V.; Andre, M.; Desroche, T.; Jaffar, M.C.; Traversier, N.; Levinid, C.; Lagrange-Xelot, M.; Moiton, M.P.; et al. Co-infection of dengue and covid-19: A case report. PLoS Negl. Trop. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sample No. | COVID-19 * | Dengue | |||||
|---|---|---|---|---|---|---|---|
| Vazyme | Unscience | IgG | IgM | NS1 | |||
| IgG | IgM | IgG | IgM | ||||
| 39 **** | ** + | *** − | + | − | + | − | − |
| 65 **** | + | + | + | + | + | − | − |
| 69 **** | − | − | − | − | + | − | − |
| 82 **** | + | − | + | + | + | − | − |
| Sample | IgG (+), IgM (+) | IgG (+), IgM (−) | IgG (−), IgM (+) | IgG (−), IgM (−) |
|---|---|---|---|---|
| NS1 (+) * | 0/38 | 1/38 | 0/38 | 0/38 |
| NS (−) ** | 0/38 | 1/38 | 0/38 | 0/38 |
| Sample Number | Blood Collection (Days after Positive COVID-19 Confirmation) | qPCR | Serological Detection | |||||
|---|---|---|---|---|---|---|---|---|
| CT Value | Vazyme | UNscience | ||||||
| Orf1ab | N | Host | IgG | IgM | IgG | IgM | ||
| 1 | 0 | 37.46 | 39.86 | 23.45 | + | − | + | + |
| 2 | 0 | NA * | NA | NA | + | − | + | − |
| 3 | 0 | NA | NA | NA | + | − | + | − |
| 4 | 3 | NA | NA | NA | + | + | + | + |
| 5 | 3 | NA | NA | NA | + | − | + | + |
| 6 | 3 | 36.77 | 37.78 | − ** | + | − | + | − |
| 7 | 3 | NA | NA | NA | + | − | + | − |
| 8 | 8 | NA | NA | NA | − | − | − | − |
| 9 | 9 | 37.1 | 37.59 | 29.92 | − | − | + | − |
| 10 | 10 | NA | NA | NA | + | − | + | − |
| 11 | 9 | NA | NA | NA | − | − | + | + |
| 12 | 9 | NA | NA | NA | + | − | + | − |
| 13 | 4 | 37.66 | 39.05 | − | + | − | + | − |
| 14 | 9 | 37.3 | 37.5 | − | + | − | + | + |
| 15 | 3 | 33.04 | 33.59 | 24.07 | + | + | + | + |
| 16 | 1 | 22.96 | 24.5 | − | − | − | − | − |
| 17 | 9 | 32.51 | 33.17 | 20.44 | + | − | + | + |
| 18 | 8 | 36.15 | 35.92 | 24.89 | + | + | + | + |
| 19 | 9 | 36.29 | − | 36.87 | − | − | − | − |
| 20 | 9 | 36.31 | 38.5 | 24.6 | + | − | + | + |
| 21 | 11 | NA | NA | NA | + | − | + | + |
| 22 | 7 | 27.42 | 27.7 | 20.51 | + | − | + | − |
| 23 | 0 | 33.67 | 33.96 | 20.85 | + | − | + | − |
| 24 | 2 | 38.38 | 39.67 | 24.59 | + | − | + | + |
| 25 | 3 | 33.95 | 34.38 | 23.86 | + | − | + | − |
| 26 | 3 | 37.69 | 37.26 | 22.27 | + | − | + | + |
| 27 | 6 | 36.35 | 38.53 | 23.1 | + | + | + | + |
| 28 | 1 | 37.4 | 38.8 | 21.58 | + | − | + | − |
| 29 | 1 | 30.29 | 30.53 | 20.72 | + | − | + | − |
| 30 | 4 | NA | NA | NA | − | − | − | − |
| 31 | 8 | NA | NA | NA | − | − | − | − |
| 32 | 4 | 28.83 | 29.71 | 22.04 | − | − | − | − |
| 33 | 4 | NA | NA | NA | − | − | − | − |
| 34 | 5 | 35.86 | 36.56 | 24.49 | + | − | + | − |
| 35 | 5 | 38.83 | 22.28 | − | − | − | − | − |
| 36 | 5 | 36.14 | 38.28 | 24.11 | − | − | − | − |
| 37 | 1 | 35.58 | 37.96 | 23.18 | + | − | + | − |
| 38 | 0 | 39.77 | 21.81 | − | + | + | + | + |
| 39 | 8 | 36.46 | 38.45 | 24.45 | + | − | + | − |
| 40 | 8 | 38.56 | 39.6 | 27.63 | + | − | + | − |
| 41 | 4 | NA | NA | NA | + | − | + | − |
| 42 | 7 | 39.51 | 29 | − | − | + | − | + |
| 43 | 5 | 38.02 | 38.94 | − | + | − | + | − |
| 44 | 1 | 39.09 | 39.42 | − | + | − | + | − |
| 45 | 0 | 38.59 | − | − | − | − | − | − |
| 46 | 3 | 33.22 | 33.74 | 23.56 | + | + | + | − |
| 47 | 6 | 35.44 | 36.66 | 29.28 | − | − | − | − |
| 48 | 0 | 28.87 | 29.48 | 27.29 | − | − | − | − |
| 49 | 8 | NA | NA | NA | + | − | + | − |
| 50 | 3 | 32.45 | 32.35 | 23.33 | + | + | + | − |
| 51 | 8 | 35.93 | 36.5 | 25.02 | + | − | + | − |
| 52 | 13 | 32.37 | 32.99 | 27.93 | − | − | + | − |
| 53 | 2 | 34.33 | 35.39 | 23.6 | + | + | + | − |
| 54 | 8 | 31.4 | 32.86 | 23.98 | + | + | + | + |
| 55 | 13 | 33.08 | 33.96 | 23.23 | + | − | + | − |
| 56 | 2 | 27.46 | 27.81 | 22.66 | − | − | − | − |
| 57 | 7 | 35.89 | 37.41 | 23.62 | + | − | + | − |
| 58 | 3 | 36.36 | 34.78 | 25.23 | + | − | + | − |
| 59 | 6 | 31.12 | 31.31 | 23.65 | + | − | + | − |
| 60 | 3 | 37.08 | 38.56 | 26.9 | − | − | + | − |
| 61 | 7 | 36.77 | 37.13 | 23.78 | − | − | + | − |
| 62 | 3 | 39.33 | 39.21 | 23.13 | + | − | + | − |
| 63 | 0 | 37.14 | 36.69 | 22.29 | + | − | + | + |
| 64 | 11 | 38.46 | 39.49 | 22.64 | − | − | − | − |
| 65 | 6 | 23.5 | 23.91 | 21.98 | + | + | + | + |
| 66 | 2 | 30.41 | 30.14 | 24.8 | − | − | + | − |
| 67 | 7 | 35.46 | 35.64 | 24.16 | + | − | + | − |
| 68 | 5 | 38.36 | − | 23.94 | + | + | + | + |
| 69 | 11 | NA | NA | NA | − | − | − | − |
| 70 | 2 | 32.45 | 32.35 | 23.33 | + | − | + | − |
| 71 | 6 | 36.5 | 36.48 | 23.72 | − | − | − | − |
| 72 | 6 | 34.33 | 35.39 | 23.6 | + | − | + | − |
| 73 | 5 | 35.15 | 35.04 | 24.01 | + | − | + | − |
| 74 | 8 | − | 38.18 | 22.57 | + | − | + | − |
| 75 | 2 | − | 35.97 | 31.27 | + | − | + | − |
| 76 | 2 | 34.05 | 30.43 | 27.47 | + | − | + | − |
| 77 | 5 | 34.21 | 35.17 | 24.7 | − | − | − | − |
| 78 | 5 | 33.65 | 34.7 | − | + | − | + | − |
| 79 | 8 | 31.4 | 32.86 | 23.98 | + | − | + | − |
| 80 | 7 | 35.46 | 35.64 | 24.16 | + | − | + | − |
| 81 | 2 | 30.41 | 30.14 | 24.8 | + | − | + | − |
| 82 | 2 | 36.225 | − | − | + | − | + | + |
| 83 | 0 | 34.12 | 33.66 | 24.54 | + | |||
| 84 | 5 | 34.05 | 32.67 | 25.99 | + | + | + | + |
| 85 | 6 | 31.15 | 28.17 | 21.45 | + | − | + | − |
| 86 | NA | NA | NA | NA | + | − | + | − |
| 87 | 6 | 39.42 | 36.2 | 0 | + | + | + | + |
| 88 | 6 | 23.12 | 17.01 | 24.02 | + | − | + | − |
| 89 | 6 | 30.93 | 27.86 | 21.02 | + | − | + | − |
| 90 | 3 | 37.29 | 34.43 | 28.46 | + | − | + | − |
| 91 | 5 | 29.17 | 28.34 | 25.78 | + | − | + | − |
| 92 | 6 | 37.65 | 36.99 | 23.64 | + | + | + | + |
| 93 | 1 | 31.79 | 28.39 | 21.05 | − | − | − | − |
| 94 | NA | NA | NA | NA | + | + | + | + |
| 95 | 7 | 38.53 | 34.57 | 28.3 | + | − | + | + |
| 96 | 5 | 35.65 | 33.73 | 26.61 | + | − | + | − |
| 97 | 1 | 29.72 | 28.42 | 28.57 | + | + | + | + |
| 98 | 1 | 18.97 | 15.8 | 27.28 | − | − | − | − |
| 99 | 7 | 39.02 | 37.03 | 27.57 | + | + | + | + |
| 100 | 5 | 37.17 | 33.83 | 23.91 | − | − | − | − |
| 101 | 5 | 32.3 | 30.87 | 26.87 | + | + | + | − |
| 102 | 1 | 29.72 | 28.42 | 28.57 | + | + | + | + |
| 103 | 5 | 29.59 | 28.28 | 23.01 | + | + | − | − |
| 104 | 1 | 36.68 | 35.61 | 26.01 | + | − | + | − |
| 105 | 5 | 37.47 | 25.49 | − | + | + | + | + |
| 106 | 5 | 37.9 | − | 26.71 | + | − | + | − |
| 107 | 4 | 30.98 | 30.18 | 26.11 | + | − | + | − |
| 108 | 5 | 37.27 | 37.12 | 25.23 | − | − | + | − |
| 109 | 7 | 36.61 | 36 | 27.48 | − | − | + | − |
| 110 | 8 | 28.94 | 27.87 | 25.49 | − | − | − | − |
| 111 | 8 | 32.89 | 31.63 | 25.83 | + | − | + | − |
| 112 | 8 | 31.07 | 29.97 | 27.39 | + | − | + | − |
| 113 | 8 | 30.78 | 29.33 | 25.18 | + | − | + | − |
| 114 | 8 | 26.2 | 24.72 | 24.75 | + | − | + | − |
| 115 | 8 | 33.07 | 32.03 | 26.19 | + | − | + | − |
| 116 | 8 | 33.84 | 32.46 | 25.6 | + | + | − | |
| 117 | 8 | 33.57 | 32.47 | 25.48 | + | − | + | − |
| 118 | 12 | 33.86 | 33.05 | 25.01 | + | − | + | − |
| 119 | 11 | 26.92 | 23.55 | 23.93 | + | − | + | − |
| 120 | 11 | 36.63 | 36.09 | 32.51 | + | − | + | − |
| 121 | 8 | 34.95 | 34.44 | 27.3 | + | − | + | + |
| 122 | 6 | NA | NA | NA | + | − | + | |
| 123 | 11 | 40 | 37.75 | 28.36 | + | − | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khairunisa, S.Q.; Amarullah, I.H.; Churrotin, S.; Fitria, A.L.; Amin, M.; Lusida, M.I.; Soegijanto, S. Potential Misdiagnosis between COVID-19 and Dengue Infection Using Rapid Serological Test. Infect. Dis. Rep. 2021, 13, 540-551. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13020050
Khairunisa SQ, Amarullah IH, Churrotin S, Fitria AL, Amin M, Lusida MI, Soegijanto S. Potential Misdiagnosis between COVID-19 and Dengue Infection Using Rapid Serological Test. Infectious Disease Reports. 2021; 13(2):540-551. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13020050
Chicago/Turabian StyleKhairunisa, Siti Qamariyah, Ilham Harlan Amarullah, Siti Churrotin, Anisa Lailatul Fitria, Mochammad Amin, Maria Inge Lusida, and Soegeng Soegijanto. 2021. "Potential Misdiagnosis between COVID-19 and Dengue Infection Using Rapid Serological Test" Infectious Disease Reports 13, no. 2: 540-551. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13020050