
Epstein–Barr Virus (EBV) Viral Load in Tumor Cells Did Not Predict Tumor Extensiveness in Nasopharyngeal Cancer

 ,
,  and
and
Abstract
:1. Introduction
2. Method
2.1. Study Design and Subject Recruitment
2.2. Sample Processing for EBV DNA Quantification
2.3. Tumor Volume Determination
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristics
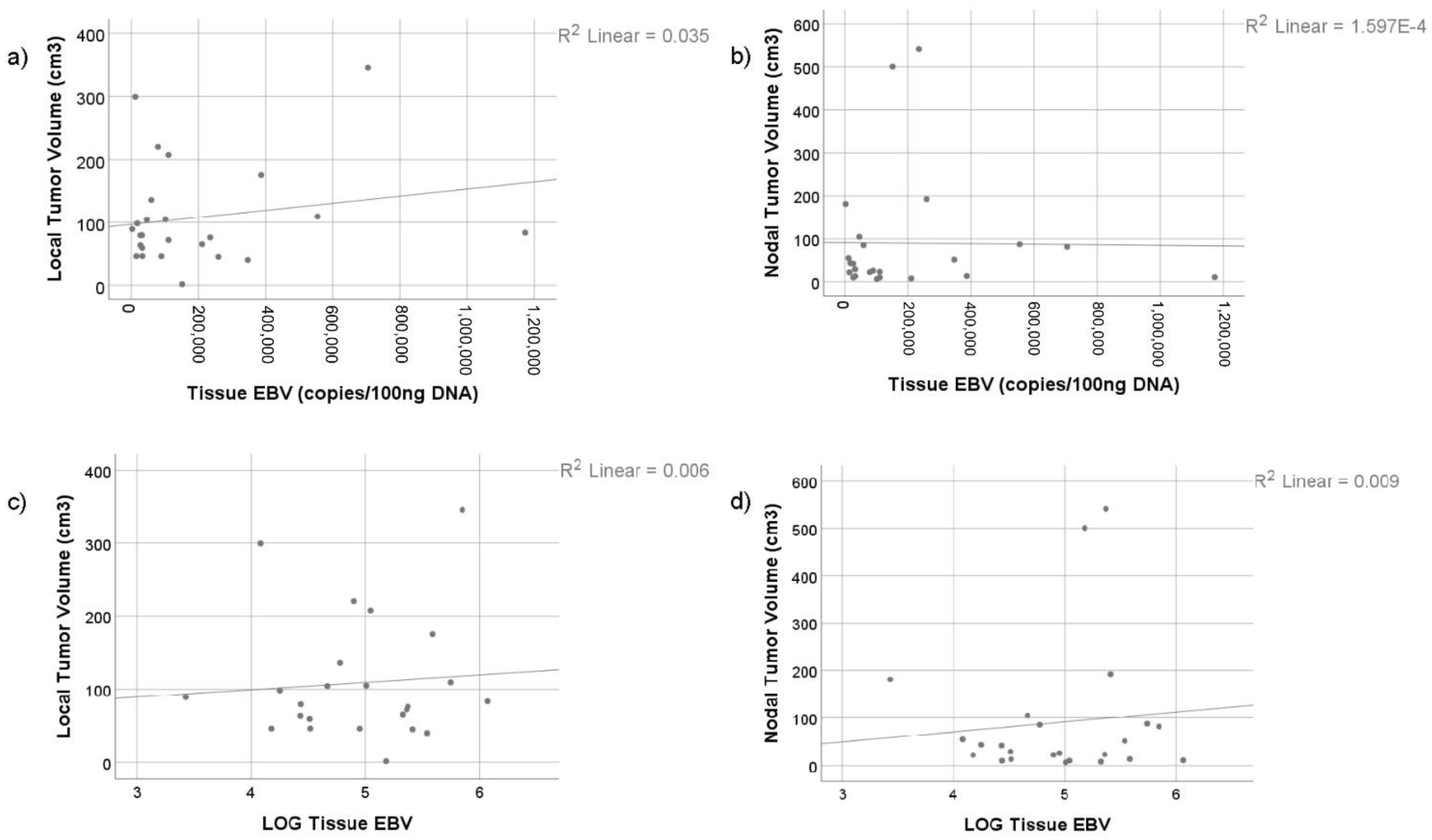
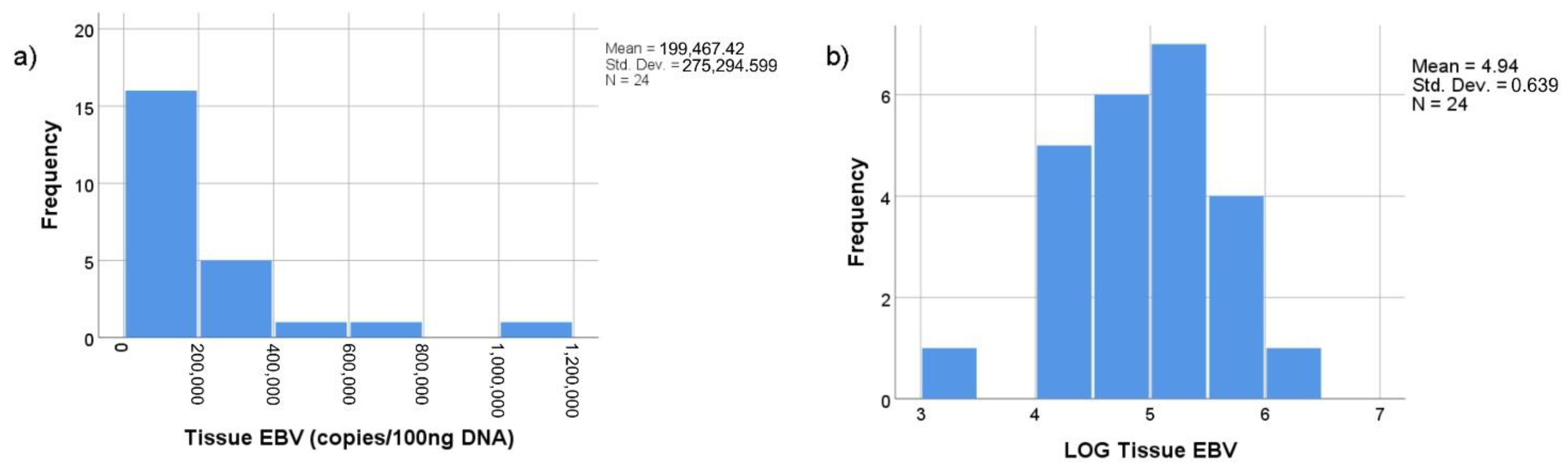
3.2. Relationship between Tumor Volume and EBV Viral Load in Tumor Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gondhowiardjo, S.A.; Adham, M.; Lisnawati, L.; Kodrat, H.; Tobing, D.L.; Handoko, H.; Haryoga, I.M.; Dwiyono, A.G.; Kristian, Y.A. Current Immune-Related Molecular Approach in Combating Nasopharyngeal Cancer. World J. Oncol. 2019, 10, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Rumayor Pina, A.; Dos Santos, H.T.; Carlos, R.; Altemani, A.; de Almeida, O.P. Epstein-Barr Virus in Nasopharyngeal Carcinoma of Guatemalan and Brazilian Patients. Int. J. Surg. Pathol. 2017, 25, 304–309. [Google Scholar] [CrossRef]
- Vaughan, T.L.; A Shapiro, J.; Burt, R.D.; Swanson, G.M.; Berwick, M.; Lynch, C.F.; Lyon, J.L. Nasopharyngeal cancer in a low-risk population: Defining risk factors by histological type. Cancer Epidemiol. Biomarkers Prev. 1996, 5, 587–593. [Google Scholar] [PubMed]
- Cohen, J.I. Epstein-Barr virus infection. N. Engl. J. Med. 2000, 343, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Klein, G.; Giovanella, B.C.; Lindahl, T.; Fialkow, P.J.; Singh, S.; Stehlin, J.S. Direct evidence for the presence of Epstein-Barr virus DNA and nuclear antigen in malignant epithelial cells from patients with poorly differentiated carcinoma of the nasopharynx. Proc. Natl. Acad. Sci. USA 1974, 71, 4737–4741. [Google Scholar] [CrossRef] [Green Version]
- Fåhraeus, R.; Fu, H.L.; Ernberg, I.; Finke, J.; Rowe, M.; Klein, G.; Falk, K.; Nilsson, E.; Yadav, M.; Busson, P.; et al. Expression of Epstein-Barr virus-encoded proteins in nasopharyngeal carcinoma. Int. J. Cancer 1988, 42, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Tsao, S.W.; Tsang, C.M.; Lo, K.W. Epstein–Barr virus infection and nasopharyngeal carcinoma. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 20160270. [Google Scholar] [CrossRef]
- Jain, A.; Chia, W.K.; Toh, H.C. Immunotherapy for nasopharyngeal cancer—A review. Chin. Clin. Oncol. 2016, 5, 22. [Google Scholar] [CrossRef]
- Gondhowiardjo, S. Epstein-Barr virus latent membrane protein 1 (EBV-LMP1) and tumor proliferation rate as predictive factors of nasopharyngeal cancer (NPC) radiation response. Gan kagaku ryoho. Cancer Chemother. 2000, 27, 323–331. [Google Scholar]
- Young, L.S.; Yap, L.F.; Murray, P.G. Epstein-Barr virus: More than 50 years old and still providing surprises. Nat. Rev. Cancer 2016, 16, 789–802. [Google Scholar] [CrossRef]
- Chan, K.A.; Woo, J.K.; King, A.; Zee, B.C.; Lam, W.J.; Chan, S.L.; Chu, S.W.; Mak, C.; Tse, I.O.; Leung, S.Y.; et al. Analysis of Plasma Epstein–Barr Virus DNA to Screen for Nasopharyngeal Cancer. N. Engl. J. Med. 2017, 377, 513–522. [Google Scholar] [CrossRef]
- Shen, T.; Tang, L.-Q.; Luo, D.-H.; Chen, Q.-Y.; Li, P.-J.; Mai, D.-M.; Guo, S.-S.; Liu, L.-T.; Qian, C.-N.; Guo, X.; et al. Different Prognostic Values of Plasma Epstein-Barr Virus DNA and Maximal Standardized Uptake Value of 18F-FDG PET/CT for Nasopharyngeal Carcinoma Patients with Recurrence. PLoS ONE 2015, 10, e0122756. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Yin, L.; Wu, J.; Gu, J.-J.; Jiang, X.-S.; Wang, D.-J.; Zong, D.; Guo, C.; Zhu, H.-F.; Wu, J.-F.; et al. Impact of Plasma Epstein-Barr Virus-DNA and Tumor Volume on Prognosis of Locally Advanced Nasopharyngeal Carcinoma. BioMed Res. Int. 2015, 2015, 1–5. [Google Scholar] [CrossRef]
- Adham, M.; Greijer, A.E.; Verkuijlen, S.A.W.M.; Juwana, H.; Fleig, S.; Rachmadi, L. Epstein-Barr Virus DNA Load in Nasopharyngeal Brushings and Whole Blood in Nasopharyngeal Carcinoma Patients before and after Treatment. Clin. Cancer Res. 2013, 19, 2175–2186. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-C.; Wang, W.-Y.; Chen, K.Y.; Wei, Y.-H.; Liang, W.-M.; Jan, J.-S.; Jiang, R.-S. Quantification of Plasma Epstein–Barr Virus DNA in Patients with Advanced Nasopharyngeal Carcinoma. N. Engl. J. Med. 2004, 350, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, J.S.; Forslund, O.; Andersson, F.C.; Lindstedt, M.; Greiff, L. Intralesional EBV-DNA load as marker of prognosis for nasopharyngeal cancer. Sci. Rep. 2019, 9, 15432. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Shi, D.; Miao, J.; Wu, H.; Chen, J.; Zhou, X. PD-L1 predicts poor prognosis for nasopharyngeal carcinoma irrespective of PD-1 and EBV-DNA load. Sci. Rep. 2017, 7, 43627. [Google Scholar] [CrossRef] [Green Version]
- Gondhowiardjo, S.A.; Handoko Adham, M.; Rachmadi, L.; Kodrat, H.; Tobing, D.L. Tumor microenvironment predicts local tumor extensiveness in PD-L1 positive nasopharyngeal cancer. PLoS ONE 2020, 15, e0230449. [Google Scholar]
- Elgui de Oliveira, D.; Muller-Coan, B.G.; Pagano, J.S. Viral Carcinogenesis Beyond Malignant Transformation: EBV in the Progression of Human Cancers. Trends Microbiol. 2016, 24, 649–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Zhang, Y.; Guo, B.B.; Chan, F.K.; Tao, Q. Oncogenic induction of cellular high CpG methylation by Epstein-Barr virus in malignant epithelial cells. Chin. J. Cancer 2014, 33, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Chen, Y.; Gong, P.; Cai, L.; Lyu, X.; Jiang, Q. Higher methylation intensity induced by EBV LMP1 via NF-κB/DNMT3b signaling contributes to silencing of PTEN gene. Oncotarget 2016, 7, 40025–40037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrova, Y.I.; Schecterson, L.; Gumbiner, B.M. Roles for E-cadherin cell surface regulation in cancer. Mol. Biol. Cell 2016, 27, 3233–3244. [Google Scholar] [CrossRef]
- Fang, W.; Zhang, J.; Hong, S.; Zhan, J.; Chen, N.; Qin, T. EBV-driven LMP1 and IFN-γ up-regulate PD-L1 in nasopharyngeal carcinoma: Implications for oncotargeted therapy. Oncotarget 2014, 5, 12189–12202. [Google Scholar] [CrossRef] [PubMed]
- Canaan, A.; Haviv, I.; Urban, A.E.; Schulz, V.P.; Hartman, S.; Zhang, Z. EBNA1 regulates cellular gene expression by binding cellular promoters. Proc. Natl. Acad. Sci. USA 2009, 106, 22421–22426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruhne, B.; Sompallae, R.; Marescotti, D.; Kamranvar, S.A.; Gastaldello, S.; Masucci, M.G. The Epstein-Barr virus nuclear antigen-1 promotes genomic instability via induction of reactive oxygen species. Proc. Natl. Acad. Sci. USA 2009, 106, 2313–2318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaul, R.; Murakami, M.; Choudhuri, T.; Robertson, E.S. Epstein-Barr virus latent nuclear antigens can induce metastasis in a nude mouse model. J. Virol. 2007, 81, 10352–10361. [Google Scholar] [CrossRef] [Green Version]
- Takada, K. Role of EBER and BARF1 in nasopharyngeal carcinoma (NPC) tumorigenesis. Semin. Cancer Biol. 2012, 22, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Baumforth, K.R.; Birgersdotter, A.; Reynolds, G.M.; Wei, W.; Kapatai, G.; Flavell, J.R.; Kalk, E.; Piper, K.; Lee, S.; Machado, L.; et al. Expression of the Epstein-Barr Virus-Encoded Epstein-Barr Virus Nuclear Antigen 1 in Hodgkin’s Lymphoma Cells Mediates Up-Regulation of CCL20 and the Migration of Regulatory T Cells. Am. J. Pathol. 2008, 173, 195–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, X.-H.; Lu, L.-X.; Li, X.-Z.; Jia, W.-H. Quantification of Epstein-Barr virus DNA load in nasopharyngeal brushing samples in the diagnosis of nasopharyngeal carcinoma in southern China. Cancer Sci. 2015, 106, 1196–1201. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Number of Subjects (%) | |
|---|---|---|
| Age | ||
| ≤50 years old | 13 (54.2%) | |
| >50 years old | 11 (45.8%) | |
| Gender | ||
| Male | 18 (75%) | |
| Female | 6 (25%) | |
| Stage * | ||
| III | 4 (16.7%) | |
| IVA | 12 (50%) | |
| IVB | 8 (33.3%) | |
| Total | 24 (100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gondhowiardjo, S.A.; Handoko; Adham, M.; Rachmadi, L.; Kodrat, H.; Tobing, D.L.; Haryoga, I.M.; Dwiyono, A.G.; Kristian, Y.A.; Permata, T.B.M.; et al. Epstein–Barr Virus (EBV) Viral Load in Tumor Cells Did Not Predict Tumor Extensiveness in Nasopharyngeal Cancer. Microbiol. Res. 2021, 12, 150-156. https://0-doi-org.brum.beds.ac.uk/10.3390/microbiolres12010011
Gondhowiardjo SA, Handoko, Adham M, Rachmadi L, Kodrat H, Tobing DL, Haryoga IM, Dwiyono AG, Kristian YA, Permata TBM, et al. Epstein–Barr Virus (EBV) Viral Load in Tumor Cells Did Not Predict Tumor Extensiveness in Nasopharyngeal Cancer. Microbiology Research. 2021; 12(1):150-156. https://0-doi-org.brum.beds.ac.uk/10.3390/microbiolres12010011
Chicago/Turabian StyleGondhowiardjo, Soehartati A., Handoko, Marlinda Adham, Lisnawati Rachmadi, Henry Kodrat, Demak Lumban Tobing, I Made Haryoga, Agustinus Gatot Dwiyono, Yoseph Adi Kristian, Tiara Bunga Mayang Permata, and et al. 2021. "Epstein–Barr Virus (EBV) Viral Load in Tumor Cells Did Not Predict Tumor Extensiveness in Nasopharyngeal Cancer" Microbiology Research 12, no. 1: 150-156. https://0-doi-org.brum.beds.ac.uk/10.3390/microbiolres12010011