
Neonatal Dyshormonogenetic Goiter with Hypothyroidism Associated with Novel Mutations in Thyroglobulin and SLC26A4 Gene

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
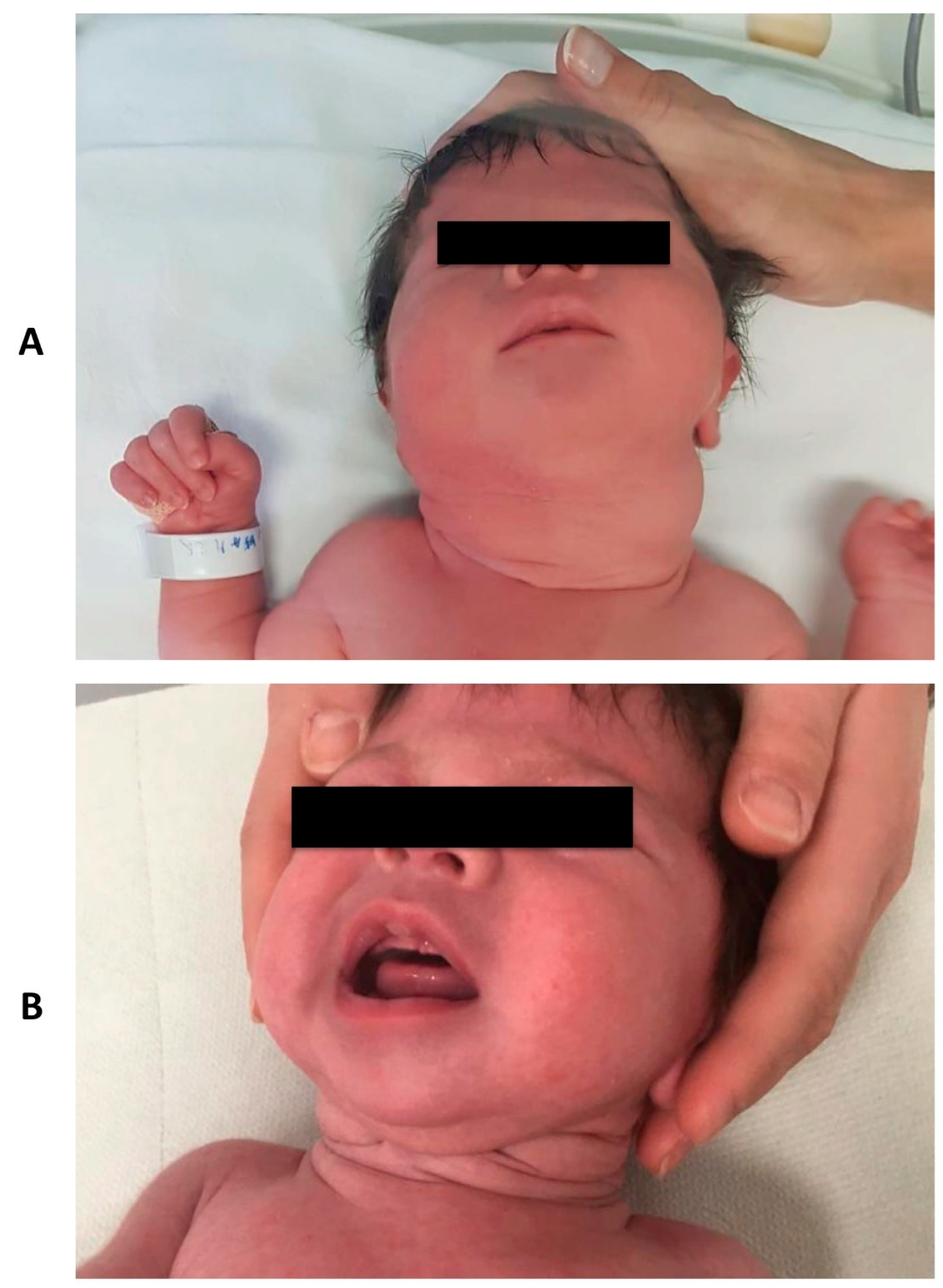
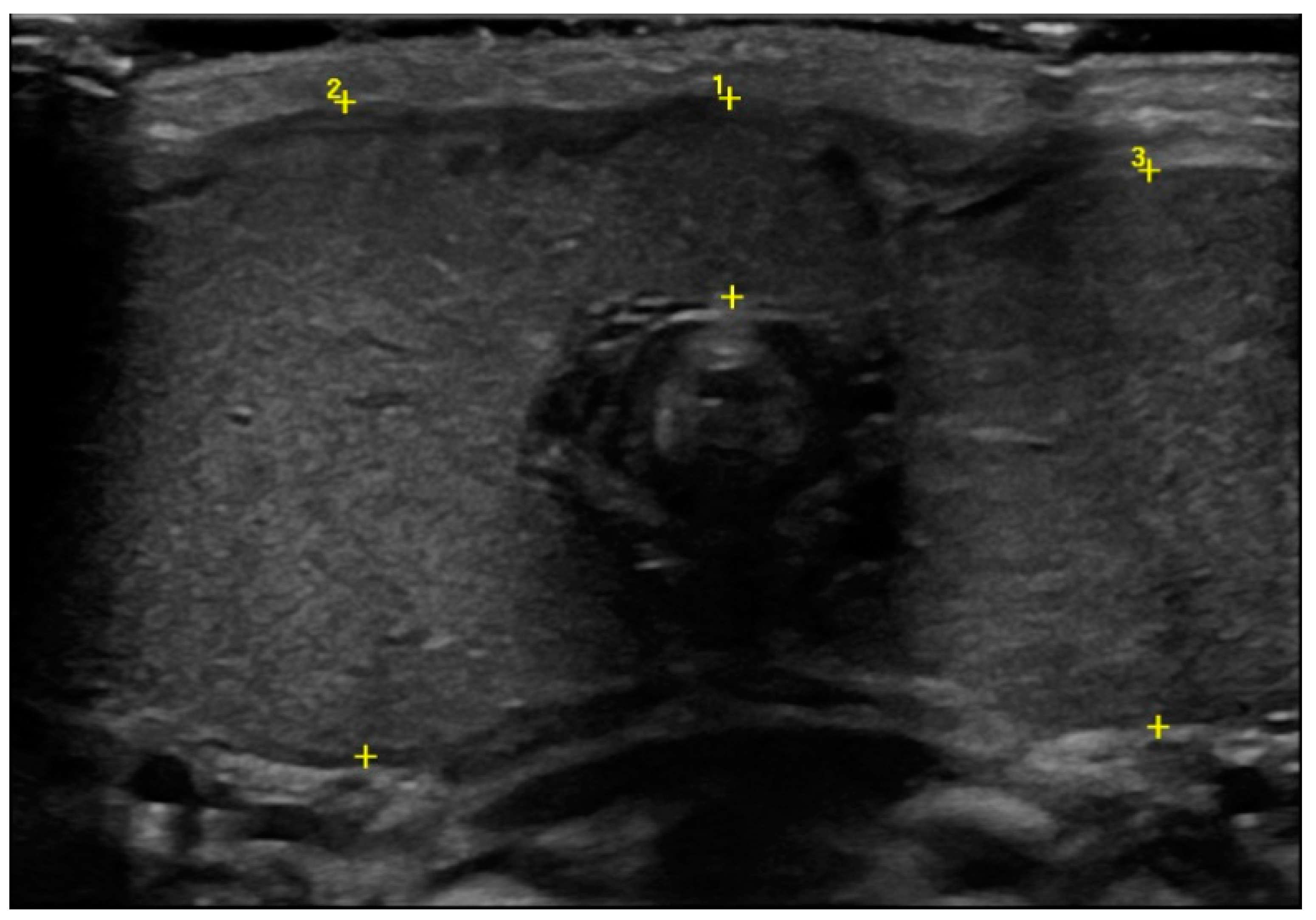
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bansal, A.G.; Oudsema, R.; Masseaux, J.A.; Rosenberg, H.K. US of Pediatric Superficial Masses of the Head and Neck. Radiographics 2018, 38, 1239–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, A.; Lipman Diaz, E.G. Hypothyroidism. Pediatr. Rev. 2014, 35, 336–347, quiz 348–349. [Google Scholar] [CrossRef]
- Blumenfeld, Y.J.; Davis, A.; Milan, K.; Chueh, J.; Hudgins, L.; Barth, R.A.; Hintz, S.R. Conservatively managed fetal goiter: An alternative to in utero therapy. Fetal Diagn. Ther. 2013, 34, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Mastrolia, S.A.; Mandola, A.; Mazor, M.; Hershkovitz, R.; Mesner, O.; Beer-Weisel, R.; Besser, L.; Shelef, I.; Loewenthal, N.; Golan, A.; et al. Antenatal diagnosis and treatment of hypothyroid fetal goiter in an euthyroid mother: A case report and review of literature. J. Matern. Fetal Neonatal Med. 2015, 28, 2214–2220. [Google Scholar] [CrossRef] [PubMed]
- Bagalkot, P.S.; Parshwanath, B.A.; Joshi, S.N. Neck swelling in a newborn with congenital goiter. J. Clin. Neonatol. 2013, 2, 36–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, C.; van Trotsenburg, A.S.P.; Schoenmakers, N. Diagnosis of endocrine disease: Congenital hypothyroidism: Update and perspectives. Eur. J. Endocrinol. 2018, 179, R297–R317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, A.J.; Wassner, A.J. Thyroid hormone therapy in congenital hypothyroidism and pediatric hypothyroidism. Endocrine 2019, 66, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.M.; Falcão, I.; Vilaverde, J.; Freitas, J.; Oliveira, M.J.; Godinho, C.; Dores, J.; Rodrigues, M.C.; Carvalho, C.; Borges, T. Prenatal Diagnosis and Management of a Fetal Goiter Hypothyroidism due to Dyshormonogenesis. Case Rep. Endocrinol. 2018, 19, 9564737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wassner, A.J. Congenital Hypothyroidism. Clin. Perinatol. 2018, 45, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Maciel, L.M.; Kimura, E.T.; Nogueira, C.R.; Mazeto, G.M.; Magalhães, P.K.; Nascimento, M.L.; Nesi-França, S.; Vieira, S.E. Brazilian Society of Endocrinology and Metabolism. Congenital hypothyroidism: Recommendations of the Thyroid Department of the Brazilian Society of Endocrinology and Metabolism. ARQ Bras. Endocrinol. Metabol. 2013, 57, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanou, Y.; Hishinuma, A.; Tsunekawa, K.; Seki, K.; Mizuno, Y.; Fujisawa, H.; Imai, T.; Miura, Y.; Nagasaka, T.; Yamada, C.; et al. Gene Mutations Producing Defective Intracellular Transport of Thyroglobulin Are Associated with Increased Thyroidal Type 2 Iodothyronine Deiodinase Activity. J. Clin. Endocrinol. Metab. 2007, 92, 1451–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, A.K.C.; Leung, A.A.C. Evaluation and management of the child with hypothyroidism. World J. Pediatr. 2019, 15, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Targovnik, H.M.; Esperante, S.A.; Rivolta, C.M. Genetics and phenomics of hypothyroidism and goiter due to thyroglobulin mutations. Mol. Cell Endocrinol. 2010, 322, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Siffo, S.; Adrover, E.; Citterio, C.E.; Miras, M.B.; Balbi, V.A.; Chiesa, A.; Weill, J.; Sobrero, G.; González, V.G.; Papendieck, P.; et al. Molecular analysis of thyroglobulin mutations found in patients with goiter and hypothyroidism. Mol. Cell Endocrinol. 2018, 473, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wémeau, J.L.; Kopp, P. Pendred syndrome. Best Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 213–224. [Google Scholar]
- Fugazzola, L.; Mannavola, D.; Cerutti, N.; Maghnie, M.; Pagella, F.; Bianchi, P.; Weber, G.; Persani, L.; Beck-Peccoz, P. Molecular analysis of the Pendred’s syndrome gene and magnetic resonance imaging studies of the inner ear are essential for the diagnosis of true Pendred’s syndrome. J. Clin. Endocrinol. Metab. 2000, 85, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Persani, L.; Rurale, G.; de Filippis, T.; Galazzi, E.; Muzza, M.; Fugazzola, L. Genetics and management of congenital hypothyroidism. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Ares Segura, S.; Temboury Molina, C.; Chueca Guindulain, M.J.; Grau Bolado, G.; Alija Merillas, M.J.; Caimari Jaume, M.; Casano Sancho, P.; Moreno Navarro, J.C.; Rial Rodríguez, J.M.; Rodríguez Sánchez, A. Recommendations for the diagnosis and follow up of the foetus and newborn child born to mothers with autoimmune thyroid disease. An. Pediatr. 2018, 89, 254.e1–254.e7. [Google Scholar]
- Braham, E.; Rejeb, H.B.; Marghli, A.; Kilani, T.; El Mezni, F. A rare and particular form of goiter to recognize. Ann. Transl. Med. 2013, 1, 21. [Google Scholar] [PubMed]
- Trovato, M. A historical excursus of diagnostic methods for Hashimoto thyroiditis and Graves’ disease. Gazz. Med. Ital. Arch. Sci. Med. 2020, 179, 479–485. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Lamberti, R.; Viggiano, C.; Gatto, S.; Spaccini, L.; Lista, G.; Zuccotti, G. Neonatal Dyshormonogenetic Goiter with Hypothyroidism Associated with Novel Mutations in Thyroglobulin and SLC26A4 Gene. Pediatr. Rep. 2021, 13, 210-215. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020029
Calcaterra V, Lamberti R, Viggiano C, Gatto S, Spaccini L, Lista G, Zuccotti G. Neonatal Dyshormonogenetic Goiter with Hypothyroidism Associated with Novel Mutations in Thyroglobulin and SLC26A4 Gene. Pediatric Reports. 2021; 13(2):210-215. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020029
Chicago/Turabian StyleCalcaterra, Valeria, Rossella Lamberti, Claudia Viggiano, Sara Gatto, Luigina Spaccini, Gianluca Lista, and Gianvincenzo Zuccotti. 2021. "Neonatal Dyshormonogenetic Goiter with Hypothyroidism Associated with Novel Mutations in Thyroglobulin and SLC26A4 Gene" Pediatric Reports 13, no. 2: 210-215. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020029