
Parent Training and Therapy in Children with Autism

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
2.3. Procedures and Tasks
2.4. Statistic Analysis
3. Results
- –
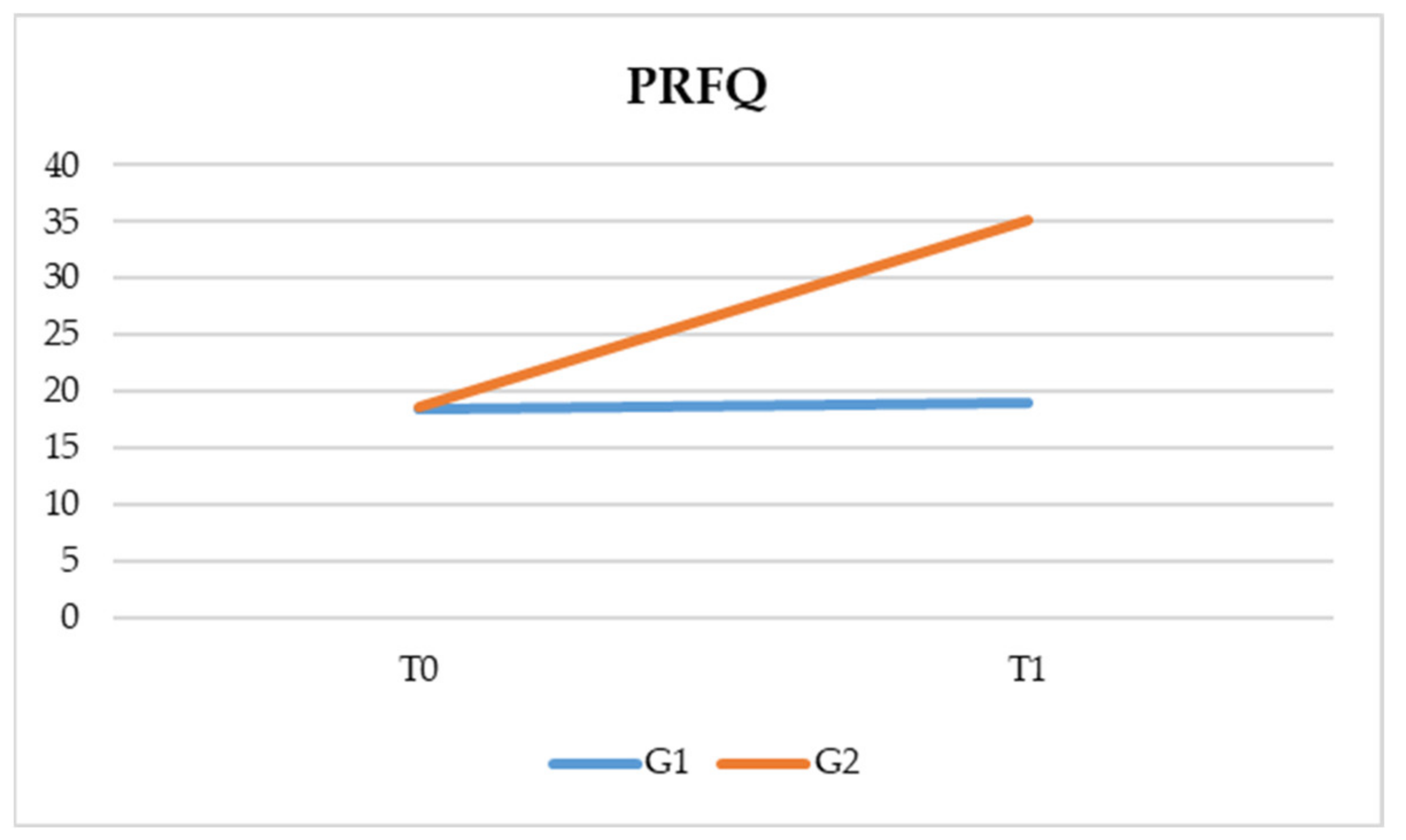
- Time * group interaction is significant (F (1, 82) = 1637.699, p < 0.05). This data indicates that there is a significant interaction between the time and the type of treatment. More specifically, both treatments have a positive effect on parental awareness, but this is even more true for PT based on reflexive functions (G2) (Table 2 and Figure 1).
- –
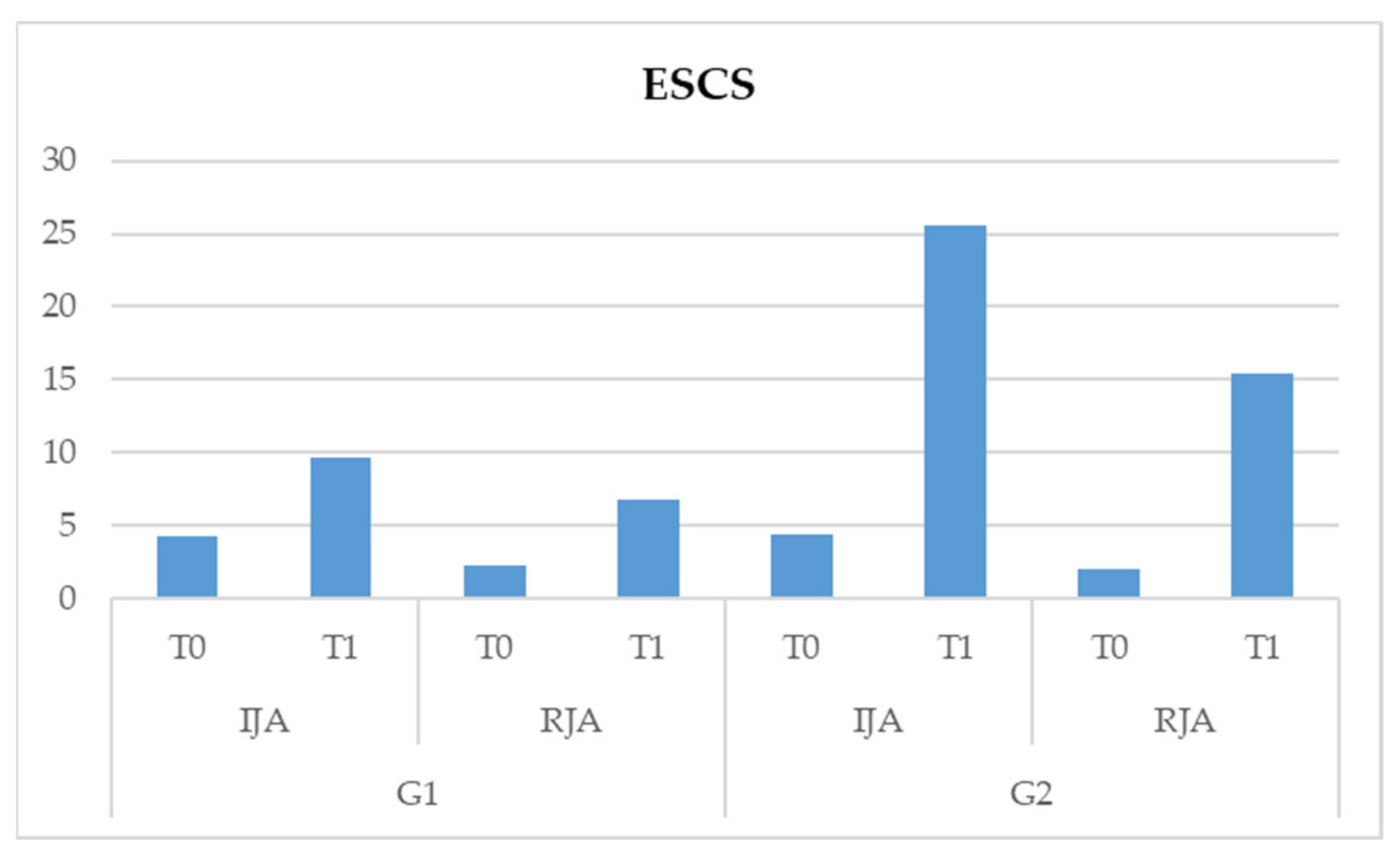
- Interaction scale * time * group is significant (F (1,82) = 161.102, p < 0.05). This data shows us that there is a significant interaction between the two subscales, those being the time and type of treatment. More specifically, both treatments show significant improvements in the two subscales of the ESCS test, but in G2, a more significant improvement in the IJA behaviors of children at T1 is noted (Table 3 and Figure 2).
- –
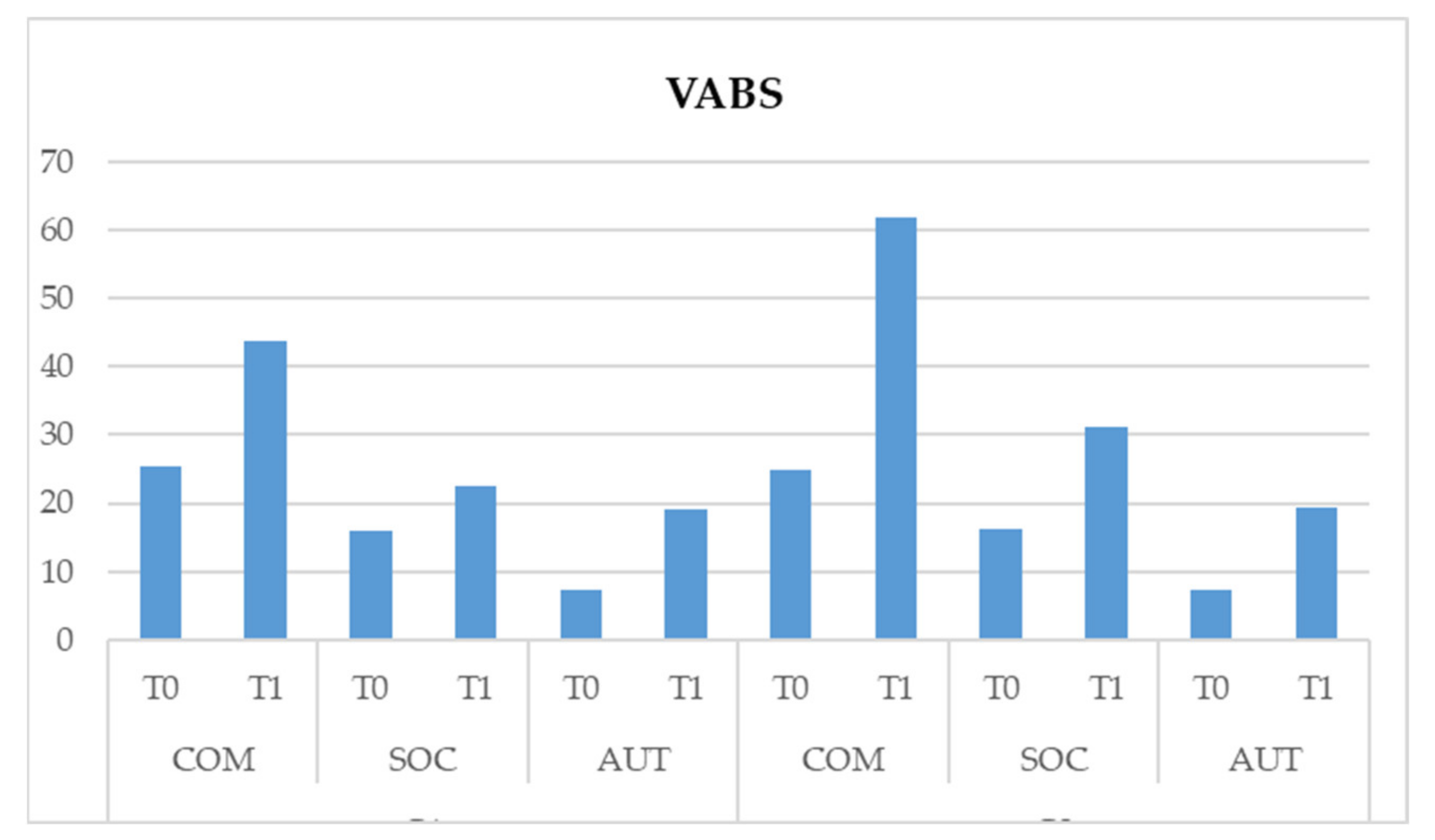
- Interaction scale * time * group is significant (F (1,164) = 424.871, p < 0.05). This data shows us that there is a significant interaction between the three subscales. Both treatments show significant improvements of the three subscales of the VABS test, but there is a more significant improvement in G2 on the communicative and social area of children at T1 (Table 4 and Figure 3).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Arlinghton, VA, USA, 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), 4th ed.; APA: Washington, DC, USA, 2000. [Google Scholar]
- Santocchi, E.; Muratori, F. L’autismo nel DSM-5. Infanz. Adolesc. 2012, 11, 158–174. [Google Scholar]
- Tronick, E.; Adamson, L.B.; Als, H.; Brazelton, T.B. Infant emotions in normal and pertubated interactions. In Proceedings of the Biennial Meeting of the Society for Research in Child Development, Denver, CO, USA, 10–13 April 1975; Volume 28, pp. 66–104. [Google Scholar]
- Adamson, L.B.; Frick, J.E. The Still Face: A History of a Shared Experimental Paradigm. Infancy 2003, 4, 451–473. [Google Scholar] [CrossRef]
- Castelli, I.; Cavalli, G.; Di Terlizzi, E.; Lecciso, F.; Lucchini, B.; Massaro, D.; Petrocchi, S.; Valle, A. Theory of Mind in Typical and Atypical Developmental Settings: Some Considerations from a Contextual Perspective. In Reflective Thinking in Educational Settings; Cambridge University Press: Cambridge, UK, 2014; pp. 102–136. [Google Scholar]
- Lecciso, F.; Petrocchi, S.; Marchetti, A. Hearing mothers and oral deaf children: An atypical relational context for theory of mind. Eur. J. Psychol. Educ. 2013, 28, 903–922. [Google Scholar] [CrossRef]
- Petrocchi, S.; Levante, A.; Baruffaldi, F.; Lecciso, F. Theory of Mind in deaf adults: The role of verbal ability and interpersonal experiences from early years. Life Span Disabil. 2017, 20, 45–61. [Google Scholar]
- Meins, E.; Fernyhough, C.; Wainwright, R.; Das Gupta, M.; Fradley, E.; Tuckey, M. Maternal Mind–Mindedness and Attachment Security as Predictors of Theory of Mind Understanding. Child. Dev. 2002, 73, 1715–1726. [Google Scholar] [CrossRef] [PubMed]
- Meins, E.; Fernyhough, C.; Wainwright, R.; Clark-Carter, D.; Das Gupta, M.; Fradley, E.; Tuckey, M. Pathways to Understanding Mind: Construct Validity and Predictive Validity of Maternal Mind-Mindedness. Child. Dev. 2003, 74, 1194–1211. [Google Scholar] [CrossRef]
- Meins, E.; Fernyhough, C.; Johnson, F.; Lidstone, J. Mind-mindedness in children: Individual differences in in-ternal-state talk in middle childhood. Br. J. Dev. Psychol. 2006, 24, 181–196. [Google Scholar] [CrossRef]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect. Regulation, Mentalization, and the Development of the Self; Routledge: London, UK, 2018. [Google Scholar]
- Fonagy, P.; Target, M. The Mentalization-Focused Approach to Self Pathology. J. Pers. Disord. 2006, 20, 544–576. [Google Scholar] [CrossRef] [Green Version]
- Sharp, C.; Fonagy, P. The parent’s capacity to treat the child as a psychological agent: Constructs, measures and implications for developmental psychopathology. Soc. Dev. 2008, 17, 737–754. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.; Leekam, S. What are the Links Between Theory of Mind and Social Relations? Review, Reflections and New Directions for Studies of Typical and Atypical Development. Soc. Dev. 2004, 13, 590–619. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Exploring the Relationship Between Theory of Mind and Social-Communicative Functioning in Children with Autism. In Individual Differences in Theory of Mind: Implications for Typical and Atypical Development. Macquarie Monographs in Cognitive Science; Repacholi, B., Slaughter, V., Eds.; Psychology Press: New York, NY, USA, 2003; pp. 197–212. [Google Scholar]
- Astington, J.W. Sometimes Necessary, Never Sufficient: False Belief Understanding and Social Competence. In Individual Differences in Theory of Mind. Implications for Typical and Atypical Development; Repacholi, B., Slaughter, V., Eds.; Psychology Press: New York, NY, USA, 2003; pp. 13–38. [Google Scholar]
- Corkum, V.; Moore, C. Development of Joint Visual Attention in Infants, Joint Attention: Its Origins and Role in Development; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1995; pp. 61–83. [Google Scholar]
- Carpendale, J.I.; Lewis, C. Constructing an understanding of mind: The development of children’s social understanding within social interaction. Behav. Brain Sci. 2004, 27, 79–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaife, M.; Bruner, J.S. The capacity for joint visual attention in the infant. Nat. Cell Biol. 1975, 253, 265–266. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.; Dunham, P.J. Joint Attention: Its Origins and Role in Development; Psychology Press: New York, NY, USA, 2014. [Google Scholar]
- Vaughan, A.; Mundy, P.; Block, J.; Burnette, C.; Delgado, C.; Gomez, Y.; Meyer, J.; Neal, A.R.; Pomares, Y. Child, Caregiver, and Temperament Contributions to Infant Joint Attention. Infancy 2003, 4, 603–616. [Google Scholar] [CrossRef]
- Frolli, A.; Lombardi, A.; Bosco, A.; Di Carmine, F.; Ricci, M.C. Temperamental patterns and infant joint attention in typical development. Curr. Pediatr. Res. 2021, 25, 336–340. [Google Scholar]
- Fonagy, P.; Steele, M.; Steele, H.; Moran, G.S.; Higgitt, A.C. The capacity for understanding mental states: The reflective self in parent and child and its significance for security of attachment. Infant Ment. Health J. 1991, 12, 201–218. [Google Scholar] [CrossRef]
- Fonagy, P.; Target, M. Attaccamento e Funzione Riflessiva; Selected papers of Peter Fonagy and Mary Target; Cortina: Milano, Italy, 2001. [Google Scholar]
- Muratori, P.; Lochman, J.E.; Lai, E.; Milone, A.; Nocentini, A.; Pisano, S.; Righini, E.; Masi, G. Which dimension of parenting predicts the change of callous unemotional traits in children with disruptive behavior disorder? Compr. Psychiatry 2016, 69, 202–210. [Google Scholar] [CrossRef]
- Ammaniti, M.; Gallese, V. La Nascita della Intersoggettività: Lo Sviluppo del sé tra Psicodinamica e Neurobiologia; Cortina: Milano, Italy, 2014. [Google Scholar]
- Luyten, P.; Mayes, L.C.; Nijssens, L.; Fonagy, P. The parental reflective functioning questionnaire: Development and preliminary validation. PLoS ONE 2017, 12, e0176218. [Google Scholar] [CrossRef] [Green Version]
- Slade, A. Parental reflective functioning: An introduction. Attach. Hum. Dev. 2005, 7, 269–281. [Google Scholar] [CrossRef]
- Slade, A.; Grienenberger, J.; Bernbach, E.; Levy, D.; Locker, A. Maternal reflective functioning, attachment, and the transmission gap: A preliminary study. Attach. Hum. Dev. 2005, 7, 283–298. [Google Scholar] [CrossRef]
- Kelly, K.M.; Slade, A.; Grienenberger, J.F. Maternal reflective functioning, mother–infant affective communication, and infant attachment: Exploring the link between mental states and observed caregiving behavior in the intergenerational transmission of attachment. Attach. Hum. Dev. 2005, 7, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Luyster, R.; Gotham, K.; Guthrie, W.; Coffing, M.; Petrak, R.; Pierce, K.; Lord, C. The Autism Diagnostic Observation Schedule—Toddler Module: A new module of a standardized diagnostic measure for autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1305–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview Revised; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Mundy, P.; Delgado, C.; Block, J.; Venezia, M.; Hogan, A.; Seibert, J. Early Social Communication Scales; University of Miami: Coral Gables, FL, USA, 2003. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland Adaptive Behavior Scales: (Vineland II), Survey Interview Form/Caregiver Rating Form; Pearson Assessments: Livonia, MN, USA, 2005. [Google Scholar]
- IBM. Statistiche IBM SPSS per Windows; Versione 26.0; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Baron-Cohen, S. Mindblindness: An Essay on Autism and Theory of Mind; University of Cambridge: Cambridge, UK, 1995. [Google Scholar]
- Brüne, M.; Brüne-Cohrs, U. Theory of mind—Evolution, ontogeny, brain mechanisms and psychopathology. Neurosci. Biobehav. Rev. 2006, 30, 437–455. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S. Precursors to a Theory of Mind: Understanding Attention in Others. Natural Theories of Mind: Evolution; Springer: Boston, MA, USA, 1991. [Google Scholar]
- Sorce, J.F.; Emde, R.N.; Campos, J.J.; Klinnert, M.D. Maternal emotional signaling: Its effect on the visual cliff behavior of 1-year-olds. Dev. Psychol. 1985, 21, 195. [Google Scholar] [CrossRef]
- Burman, E. Deconstructing Developmental Psychology; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Allen, J.G.; Fonagy, P.; Bateman, A.W. Mentalizing in Clinical Practice; American Psychiatric Publishing Inc.: Washington, DC, USA, 2008. [Google Scholar]
- Bateman, A.W.; Fonagy, P.E. Handbook of Mentalizing in Mental Health Practice; American Psychiatric Publishing Inc.: Washington, DC, USA, 2012. [Google Scholar]
- Rostad, W.L.; Whitaker, D.J. The Association Between Reflective Functioning and Parent–Child Relationship Quality. J. Child. Fam. Stud. 2016, 25, 2164–2177. [Google Scholar] [CrossRef]
- Ensink, K.; Mayes, L.C. The Development of Mentalisation in Children from a Theory of Mind Perspective. Psychoanal. Inq. 2010, 30, 301–337. [Google Scholar] [CrossRef]
- Schultheis, A.M.; Mayes, L.C.; Rutherford, H.J.V. Associations between Emotion Regulation and Parental Reflective Functioning. J. Child. Fam. Stud. 2019, 28, 1094–1104. [Google Scholar] [CrossRef]
- Frolli, A.; La Penna, I.; Cavallaro, A.; Ricci, M.C. Theory of Mind: Autism and Typical Development. Acad. J. Ped. Neonatol. 2018, 8, 555799. [Google Scholar]
- Fonagy, P.; Target, M. Attachment and reflective function: Their role in self-organization. Dev. Psychopathol. 1997, 9, 679–700. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Mentalization-Based Treatment. Psychoanal. Inq. 2013, 33, 595–613. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Test | Group | Time | t | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | |||||
| PRFQ | 1 | T0 | 55.38 | 4.29 | ||
| 2 | T0 | 55.73 | 4.34 | 0.379 | 0.706 | |
| ESCS | 1 | T0 | 6.59 | 1.71 | ||
| 2 | T0 | 6.50 | 1.36 | 0.282 | 0.779 | |
| VABS | 1 | T0 | 48.50 | 3.24 | ||
| 2 | T0 | 48.42 | 3.10 | 0.103 | 0.918 |
| Time | Group 1 | Group 2 | F | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| T0 | 18.46 | 2.01 | 18.57 | 1.83 | ||
| T1 | 18.96 | 1.72 | 35.14 | 2.92 | 1637.699 | <0.05 * |
| Group | ESCS | Time | F | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | |||||
| 1 | IJA | T0 | 4.33 | 1.39 | ||
| T1 | 9.69 | 1.84 | ||||
| RJA | T0 | 2.26 | 0.88 | |||
| T1 | 6.83 | 1.22 | ||||
| 2 | IJA | T0 | 4.42 | 1.34 | ||
| T1 | 25.61 | 2.68 | ||||
| RJA | T0 | 2.07 | 0.89 | |||
| T1 | 15.42 | 1.53 | 161.102 | <0.05 * | ||
| Group | VABS | Time | F | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | |||||
| 1 | COM | T0 | 25.33 | 1.67 | ||
| T1 | 43.66 | 2.24 | ||||
| SOC | T0 | 15.92 | 2.21 | |||
| T1 | 22.45 | 2.70 | ||||
| AUT | T0 | 7.23 | 1.35 | |||
| T1 | 19.23 | 1.30 | ||||
| 2 | COM | T0 | 24.81 | 1.83 | ||
| T1 | 61.85 | 1.69 | ||||
| SOC | T0 | 16.19 | 1.81 | |||
| T1 | 31.21 | 2.08 | ||||
| AUT | T0 | 7.42 | 1.15 | |||
| T1 | 19.38 | 1.30 | 424.871 | <0.05 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frolli, A.; Bosco, A.; Di Carmine, F.; Cavallaro, A.; Lombardi, A.; Sergi, L.; Corrivetti, G.; Ricci, M.C. Parent Training and Therapy in Children with Autism. Pediatr. Rep. 2021, 13, 216-226. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020030
Frolli A, Bosco A, Di Carmine F, Cavallaro A, Lombardi A, Sergi L, Corrivetti G, Ricci MC. Parent Training and Therapy in Children with Autism. Pediatric Reports. 2021; 13(2):216-226. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020030
Chicago/Turabian StyleFrolli, Alessandro, Antonia Bosco, Francesca Di Carmine, Antonella Cavallaro, Agnese Lombardi, Luana Sergi, Giulio Corrivetti, and Maria Carla Ricci. 2021. "Parent Training and Therapy in Children with Autism" Pediatric Reports 13, no. 2: 216-226. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric13020030