Long-Term Results of Tinnitus Retraining Therapy in Patients Who Failed to Complete the Program

 , ,
, ,
Abstract
:1. Introduction
2. Methods
- Age over 18 years;
- Disabling tinnitus for more than 6 months;
- No tinnitus treatments for at least 1 year before starting or during the TRT program, in terms of specific pharmacologic, physical or nonconventional therapies (i.e., acupuncture);
- No pathologic features at brain MRI scan and Doppler ultrasonography of the epi-aortic vessels;
- Category 1 tinnitus patients according to Jastreboff and Hazell’s classification [14] (tinnitus is an important problem, without subjective hearing loss);
- No diagnosed associated psychiatric disorders precluding full participation or follow-up;
- No cognitive impairment which could influence adherence to the clinical protocol;
- Completion of at least the first phase of the TRT program (directive counselling, tinnitus psychoacoustic measurements and participation in sound therapy);
- Noncompletion of the entire TRT program, namely the therapist did not define the case as successfully closed after 12–18 months of follow-up;
- No previous history of otologic diseases or migrainous vertigo;
- No involvement in litigation or seeking monetary compensation for their tinnitus.
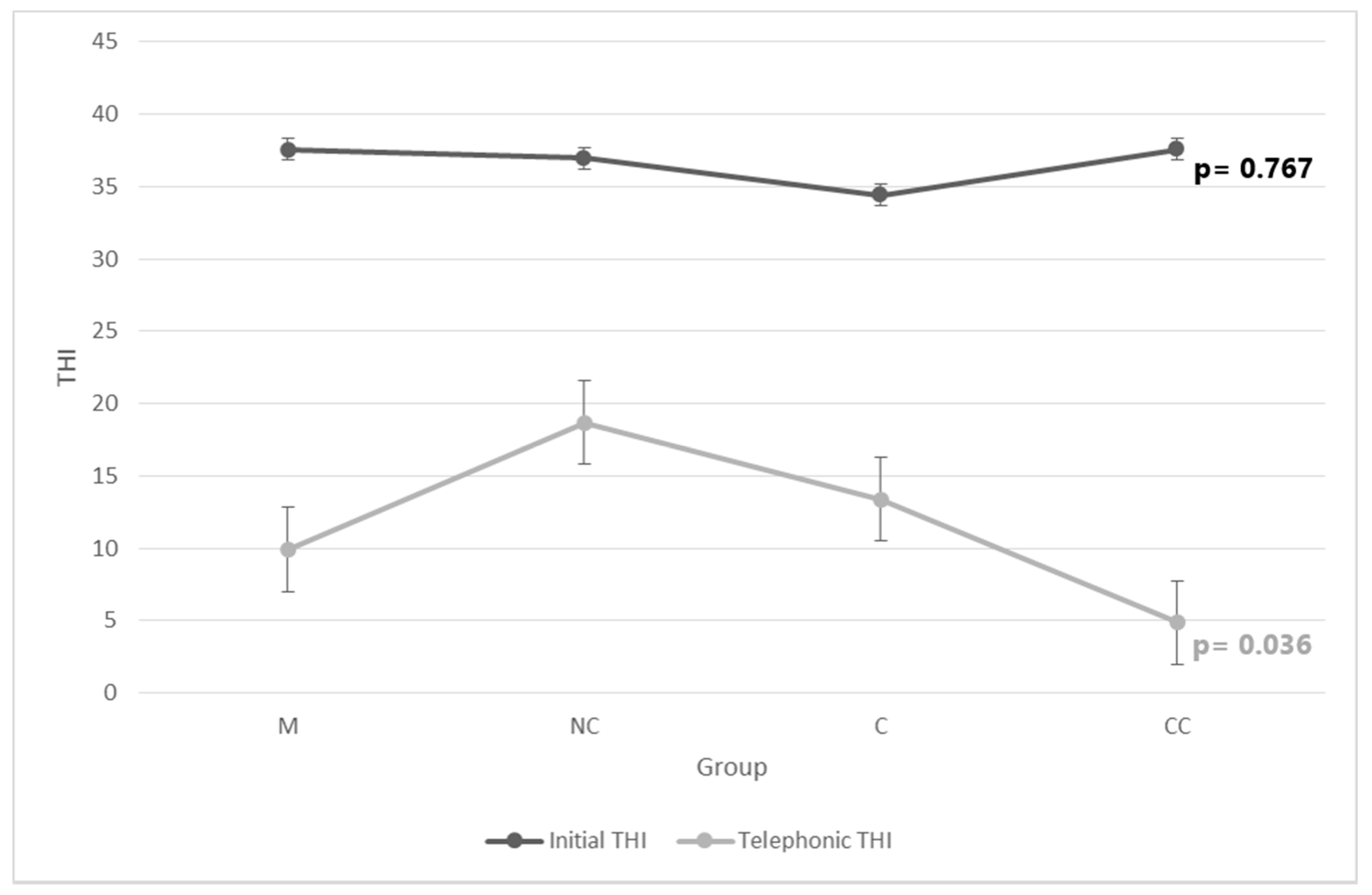
- Missing group (M; n = 36): Patients who completed the first phase of the TRT program but did not return for the second counselling appointment.
- Noncompliant group (NC; n = 34): Patients who attended counselling appointments for less than 6 months.
- Compliant group (C; n = 20): Patients who attended counselling appointments for more than 6 months but did not complete the TRT program of 12–18 months duration.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jastreboff, P.J. Phantom auditory perception (tinnitus): Mechanisms of generation and perception. Neurosci. Res. 1990, 8, 221–254. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Jastreboff, M.M. Tinnitus retraining therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J. Am. Acad. Audiol. 2000, 11, 162–177. [Google Scholar] [PubMed]
- Jastreboff, P.J. Tinnitus habituation therapy (THT) and tinnitus retraining therapy (TRT). In Tinnitus Handbook; Tyler, R., Ed.; Singular, Thomson Learning: San Diego, CA, USA, 2000; pp. 357–376. [Google Scholar]
- Molini, E.; Faralli, M.; Calenti, C.; Ricci, G.; Longari, F.; Frenguelli, A. Personal experience with tinnitus retraining therapy. Eur. Arch. Otorhinolaryngol. 2010, 267, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Sheldrake, J.B.; Hazell, J.W.P.; Graham, R.L. Results of tinnitus retraining therapy. In Proceedings of the 6th International Tinnitus Seminar, London, UK, 5–9 September 1999. [Google Scholar]
- Herraiz, C.; Hernandez, F.J.; Plaza, G.; De Los Santos, G. Long-term clinical trial of tinnitus retraining therapy. Otolaryngol. Head Neck Surg. 2005, 133, 774–779. [Google Scholar] [CrossRef]
- Bauer, C.A.; Berry, J.L.; Brozoski, T.J. The effect of tinnitus retraining therapy on chronic tinnitus: A controlled trial. Laryngoscope Investig. Otolaryngol. 2017, 28, 166–177. [Google Scholar] [CrossRef]
- Henry, J.A.; Schechter, M.A.; Zaugg, T.L.; Griest, S.; Jastreboff, P.J.; Vernon, J.A.; Kaelin, C.; Meikle, M.B.; Lyons, K.S.; Stewart, B.J. Outcomes of clinical trial: Tinnitus masking versus tinnitus retraining therapy. J. Am. Acad. Audiol. 2006, 17, 104–132. [Google Scholar] [CrossRef]
- Forti, S.; Costanzo, S.; Crocetti, A.; Pignataro, L.; Del Bo, L.; Ambrosetti, U. Are results of tinnitus retraining therapy maintained over time? 18-month follow-up after completion of therapy. Audiol. Neurootol. 2009, 14, 286–289. [Google Scholar] [CrossRef]
- Jastreboff, P.J. 25 years of tinnitus retraining therapy. HNO 2015, 63, 307–311. [Google Scholar] [CrossRef]
- Hatanaka, A.; Ariizumi, Y.; Kitamura, K. Pros and cons of tinnitus retraining therapy. Acta Otolaryngol. 2008, 128, 365–368. [Google Scholar] [CrossRef]
- Forti, S.; Ambrosetti, U.; Crocetti, A.; Del Bo, L. Tinnitus patients lost to follow-up. Int. J. Audiol. 2010, 49, 877–880. [Google Scholar] [CrossRef]
- Han, J.J.; Lee, J.H.; Oh, S.H.; Chang, S.O.; Suh, M.W. Assessing the effects of tinnitus retraining therapy in patients lost to follow-up: A telephone survey. Otol. Neurotol. 2015, 36, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, P.J.; Hazell, J.W.P. Tinnitus Retraining Therapy Implementing the Neurophysiological Model; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Monzani, D.; Genovese, E.; Marrara, A.; Gherpelli, C.; Pingani, L.; Forghieri, M.; Rigatelli, M.; Guadagnin, T.; Arslan, E. Validity of the Italian adaptation of the Tinnitus Handicap Inventory; focus on quality of life and psychological distress in tinnitus-sufferers. Acta Otorhinolaryngol. Ital. 2008, 28, 126–134. [Google Scholar] [PubMed]
- Phillips, J.S.; McFerran, D. Tinnitus Retraining Therapy (TRT) for tinnitus. Cochrane Database Syst. Rev. 2010, 17, CD007330. [Google Scholar] [CrossRef] [PubMed]
- Hiller, W.; Haerkötter, C. Does sound stimulation have additive effects on cognitive-behavioral treatment of chronic tinnitus? Behav. Res. Ther. 2005, 43, 595–612. [Google Scholar] [CrossRef]
- Grewal, R.; Spielmann, P.M.; Jones, S.E.; Hussain, S.S. Clinical efficacy of tinnitus retraining therapy and cognitive behavioural therapy in the treatment of subjective tinnitus: A systematic review. J. Laryngol. Otol. 2014, 128, 1028–1033. [Google Scholar] [CrossRef]
- Wilson, P.H.; Henry, J.L.; Andersson, G.; Hallam, R.S.; Lindberg, P. A critical analysis of directive counselling as a component of tinnitus retraining therapy. Br. J. Audiol. 1998, 32, 273–286. [Google Scholar] [CrossRef]
- Kroener-Herwig, B.; Biesinger, E.; Gerhards, F.; Goebel, G.; Verena Greimel, K.; Hiller, W. Retraining therapy for chronic tinnitus. A critical analysis of its status. Scand. Audiol. 2000, 29, 67–78. [Google Scholar] [CrossRef]
- Koizumi, T.; Nishimura, T.; Sakaguchi, T.; Okamoto, M.; Hosoi, H. Estimation of factors influencing the results of tinnitus retraining therapy. Acta Otolaryngol. Suppl. 2009, 562, 40–45. [Google Scholar] [CrossRef]
- Bauer, C.A.; Brozoski, T.J. Effect of tinnitus retraining therapy on the loudness and annoyance of tinnitus: A controlled trial. Ear Hear. 2011, 32, 145–155. [Google Scholar] [CrossRef]
- Deci, E.L.; Koestner, R.; Ryan, R.M. A meta-analytic review of experiments examining the effects of extrinsic rewards on intrinsic motivation. Psychol. Bull. 1999, 125, 627–668. [Google Scholar] [CrossRef] [PubMed]
- Krasner, L. The therapist as a social reinforcement machine. In Research in Psychotherapy; Strupp, H., Luborsky, L., Eds.; American Psychological Association: Washington, DC, USA, 1962; pp. 61–94. [Google Scholar]
- Tyler, R.S.; Haskell, G.B.; Gogel, S.A.; Gehringer, A.K. Establishing a tinnitus clinic in your practice. Am. J. Audiol. 2008, 17, 25–37. [Google Scholar] [CrossRef]
- Tyler, R.S.; Haskell, G.B.; Preece, J.; Bergan, C. Nurturing patient expectations to enhance the treatment of tinnitus. Semin. Heart 2001, 22, 15–22. [Google Scholar] [CrossRef]
- Hallam, R.; Rachman, S.; Hinchcliffe, R. Psychological aspects of tinnitus. In Contributions to Medical Psychology; Rachman, S., Ed.; Pergamon Press: Oxford, UK, 1984; Volume 3, pp. 31–53. [Google Scholar]
- Molini, E.; Faralli, M.; Calzolaro, L.; Ricci, G. Impact of identifying factors which trigger bothersome tinnitus on the treatment outcome in tinnitus retraining therapy. ORL J. Otorhinolaryngol. Relat. Spec. 2014, 76, 81–88. [Google Scholar] [CrossRef]
- Lux-Wellenhof, G.; Hellweg, F.C. Long-term follow-up of TRT in Frankfurt. In Proceedings of the VIIth International Tinnitus Seminar, Fremantle, Australia, 5–9 March 2002. [Google Scholar]



{kind=link}
{kind=link}
| M | NC | C | CC | p | ||
|---|---|---|---|---|---|---|
| Yes | 28 (78%) | 30 (88%) | 16 (80%) | 26 (93%) | 0.33 |
| No | 8 (22%) | 4 (12%) | 4 (20%) | 2 (7%) | ||
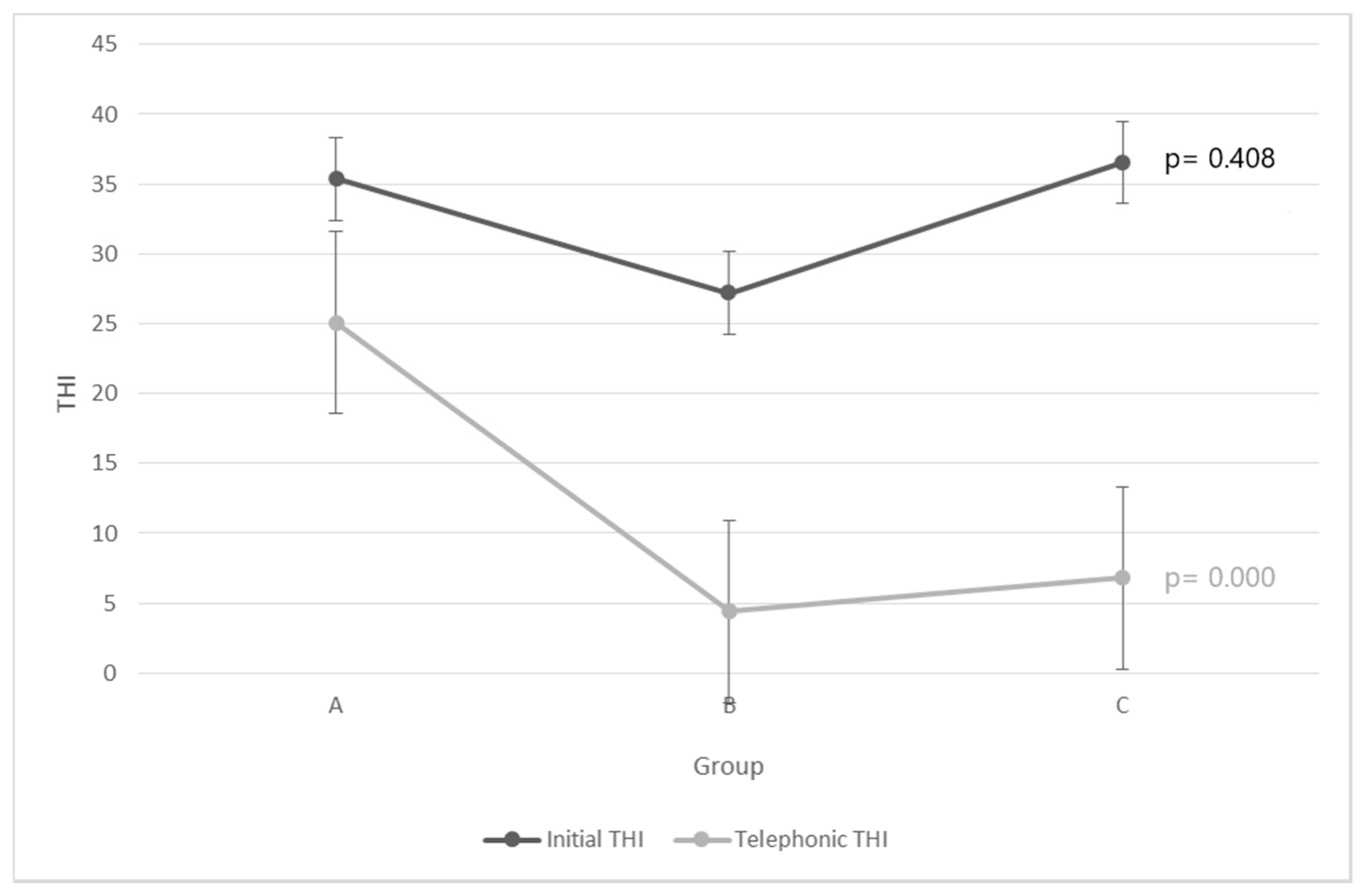
| (A) “an insurmountable problem” | 4 (11%) | 8 (24%) | 4 (20%) | 2 (7%) | 0.59 |
| (B) “a lifelong partner” | 20 (56%) | 16 (47%) | 10 (50%) | 14 (50%) | ||
| (C) “no longer a problem” | 12 (33%) | 10 (29%) | 6 (30%) | 12 (43%) | ||
| (A) I did not accept the effectiveness of TRT | 18 (50%) | 18 (53%) | 4 (20%) | - | 0.023 |
| (B) My tinnitus was cured after the first counselling session | 4 (11%) | 10 (29%) | 6 (30%) | - | ||
| (C) Other reasons (for example: illness, distance, occupation) | 14 (39%) | 6 (18%) | 10 (50%) | - | ||
| Yes | 4 (11%) | 6 (18%) | 8 (40%) | 10 (36%) | 0.29 |
| No | 32 (89%) | 28 (82%) | 12 (60%) | 18 (64%) | ||
| Yes | 4 (11%) | 8 (24%) | 0 (0%) | 0 (0%) | 0.007 |
| No | 32 (89%) | 26 (76%) | 20 (100%) | 28 (100%) | ||
| M (n = 36) | NC (n = 34) | C (n = 20) | CC (n = 28) | p | |||
|---|---|---|---|---|---|---|---|
| THI | I | 37.57 ± 20.53 | 36.94 ± 18.69 | 34.4 ± 17.15 | 37.57 ± 20.53 | pA = 0.767 | |
| T | 9.89 ± 10.94 | 18.70 ± 14.01 | 13.40 ± 19.16 | 4.86 ± 8.79 | pK = 0.036 | ||
| p | pW = 0.000 | pW = 0.051 | pW = 0.012 | pW = 0.001 | |||
| VAS | L | I | 6.06 ± 1.53 | 5.82 ± 2.26 | 6.28 ± 1.39 | 6.12 ± 1.30 | pK = 0.706 |
| T | 4.19 ± 3.16 | 5.18 ± 2.92 | 4.45 ± 3.12 | 4.14 ± 2.50 | pK = 0.659 | ||
| p | pW = 0.006 | pW = 0.313 | pW = 0.185 | pW = 0.014 | |||
| A | I | 6.67 ± 2.09 | 6.76 ± 2.43 | 7 ± 2.23 | 7.23 ± 1.64 | pK = 0.992 | |
| T | 3.77 ± 2.90 | 5.08 ± 2.79 | 4.15 ± 2.83 | 2.46 ± 2.24 | pK = 0.058 | ||
| p | pW = 0.001 | pW = 0.034 | pW = 0.01 | pW = 0.001 | |||
| E | I | 4.37 ± 3.57 | 5.03 ± 3.04 | 6.05 ± 2.67 | 4.42 ± 2.48 | pK = 0.603 | |
| T | 2.72 ± 2.19 | 2.85 ± 3.15 | 2.85 ± 3.15 | 1.43 ± 1.97 | pK = 0.243 | ||
| p | pW = 0.006 | pW = 0.12 | pW = 0.036 | pW = 0.005 | |||
| A | B | C | p | ||
|---|---|---|---|---|---|
| THI | I | 35.35 ± 16.48 | 27.2 ± 20.09 | 36.53 ± 18.57 | pA = 0.408 |
| T | 25.09 ± 17.21 | 4.4 ± 5.15 | 6.8 ± 6.18 | pK = 0.000 | |
| p | pT = 0.029 | pT = 0.002 | pW = 0.000 | ||
| VAS L | I | 6.58 ± 1.94 | 5 ± 1.78 | 6.4 ± 1.72 | pA = 0.083 |
| T | 6 ± 2.97 | 2.9 ± 2.78 | 3.93 ± 2.55 | pK = 0.009 | |
| p | pT = 0.337 | pW = 0.041 | pT = 0.008 | ||
| VAS A | I | 6.95 ± 1.81 | 5.85 ± 2.73 | 7.26 ± 2.19 | pA = 0.266 |
| T | 5.775 ± 2.68 | 2.55 ± 2.49 | 3.7 ± 2.45 | pK = 0.002 | |
| p | pW = 0.061 | pW = 0.006 | pT = 0.000 | ||
| VAS E | I | 5.35 ± 3.20 | 4 ± 2.91 | 6.13 ± 2.58 | pK = 0.161 |
| T | 4.475 ± 2.96 | 0.95 ± 1.23 | 2.56 ± 2.06 | pK = 0.005 | |
| p | pW = 0.234 | pW = 0.022 | pT = 0.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapenna, R.; Molini, E.; Cipriani, L.; Del Zompo, M.R.; Giommetti, G.; Faralli, M.; Ricci, G. Long-Term Results of Tinnitus Retraining Therapy in Patients Who Failed to Complete the Program. Audiol. Res. 2021, 11, 1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11010001
Lapenna R, Molini E, Cipriani L, Del Zompo MR, Giommetti G, Faralli M, Ricci G. Long-Term Results of Tinnitus Retraining Therapy in Patients Who Failed to Complete the Program. Audiology Research. 2021; 11(1):1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11010001
Chicago/Turabian StyleLapenna, Ruggero, Egisto Molini, Laura Cipriani, Maria Rita Del Zompo, Giorgia Giommetti, Mario Faralli, and Giampietro Ricci. 2021. "Long-Term Results of Tinnitus Retraining Therapy in Patients Who Failed to Complete the Program" Audiology Research 11, no. 1: 1-9. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11010001