
Management of Residual Hearing with Cartilage Conduction Hearing Aid after Lateral Temporal Bone Resection: Our Institutional Experience

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Treatment Strategy for Temporal Bone Squamous Cell Carcinoma at Our Institute
2.3. Audiometric Data
2.4. Image Analysis
3. Results
3.1. Patient Profile
3.2. Reconstruction of the External Auditory Meatus with a Free Flap and Hearing Outcome
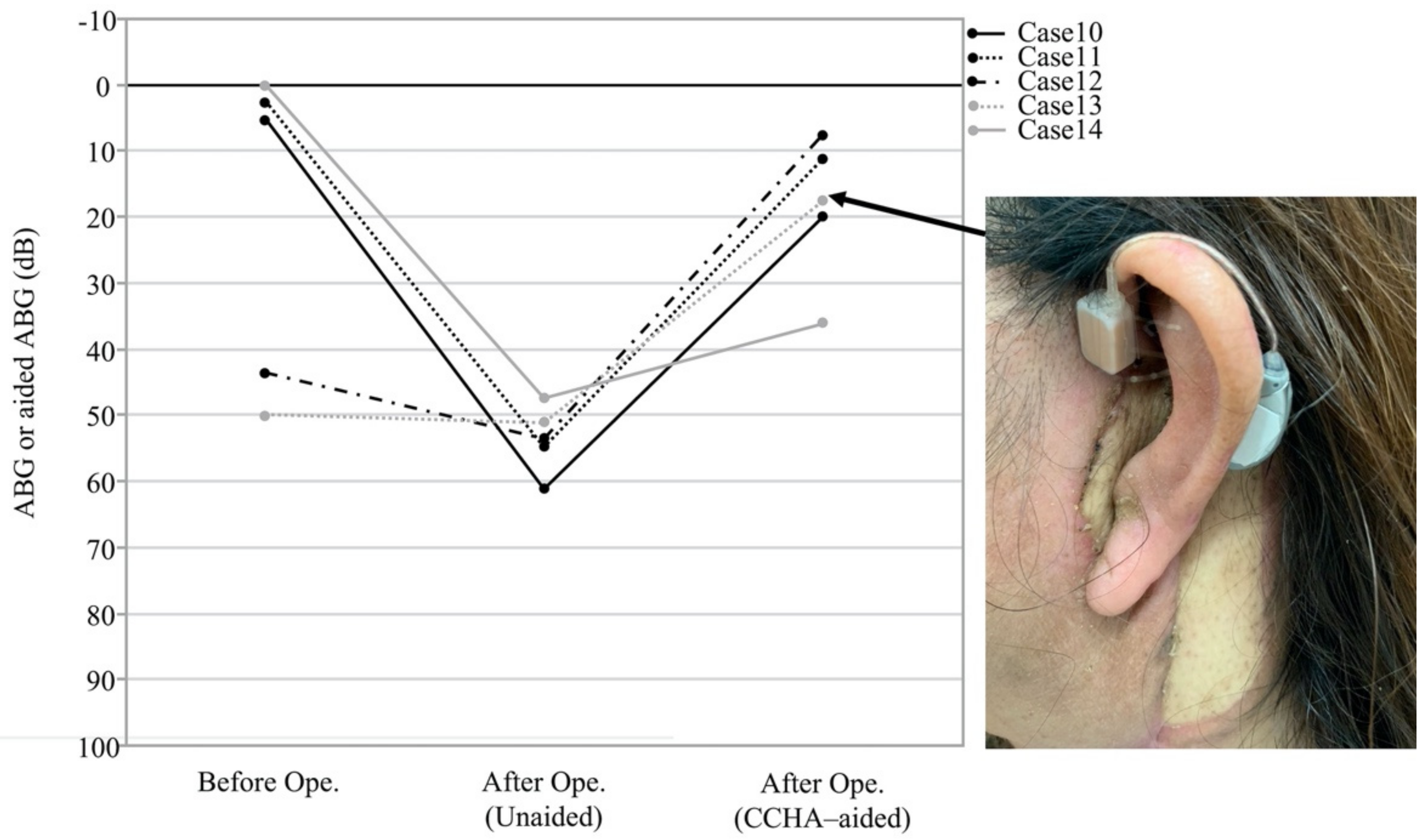
3.3. Effectiveness of the CCHA
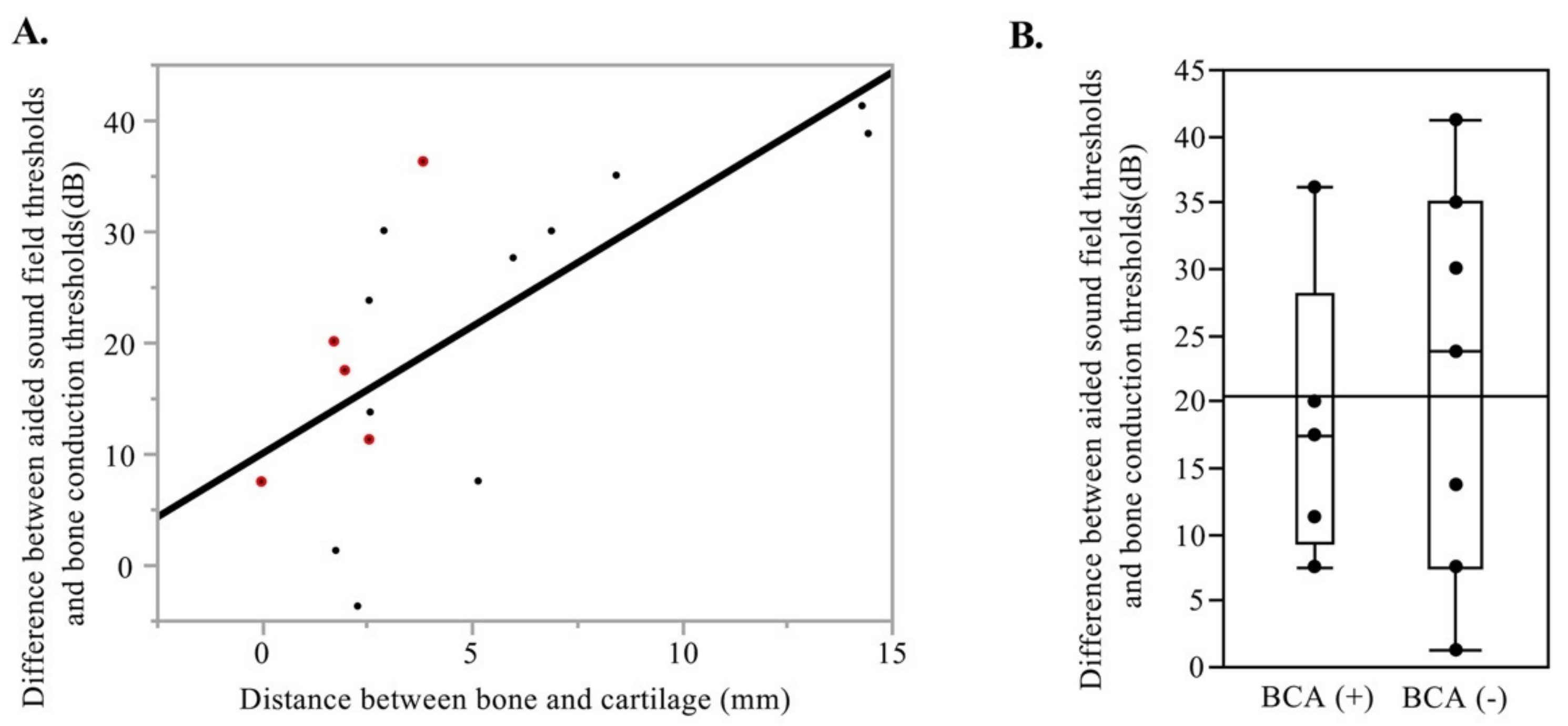
3.4. Bone-Cartilage Anchoring Technique
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lovin, B.D.; Gidley, P.W. Squamous cell carcinoma of the temporal bone: A current review. Laryngoscope Investig. Otolaryngol. 2019, 4, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, S.A.; Hirsch, B.E.; Myers, E.N. Squamous cell carcinoma of the external auditory canal: An evaluation of a staging system. Am. J. Otol. 2000, 21, 582–588. [Google Scholar] [PubMed]
- Morita, S.; Nakamaru, Y.; Homma, A.; Sakashita, T.; Masuya, M.; Fukuda, S. Hearing preservation after lateral temporal bone resection for early-stage external auditory canal carcinoma. Audiol. Neurootol. 2014, 19, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Hoshikawa, H.; Miyashita, T.; Mori, N. Surgical procedures for external auditory canal carcinoma and the preservation of postoperative hearing. Case Rep. Surg. 2012, 2012, 841372. [Google Scholar] [CrossRef] [Green Version]
- Hosoi, H.; Nishimura, T.; Shimokura, R.; Kitahara, T. Cartilage conduction as the third pathway for sound transmission. Auris Nasus Larynx 2019, 46, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Iwakura, T. Benefit of a new hearing device utilizing cartilage conduction. Auris Nasus Larynx 2013, 40, 440–446. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Levitt, H. Is cartilage conduction classified into air or bone conduction? Laryngoscope 2014, 124, 1214–1219. [Google Scholar] [CrossRef]
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Yamanaka, T.; Levitt, H. Cartilage conduction hearing. J. Acoust. Soc. Am. 2014, 135, 1959–1966. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction is characterized by vibrations of the cartilaginous portion of the ear canal. PLoS ONE 2015, 10, e0120135. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Cartilage Conduction Hearing Aids for Severe Conduction Hearing Loss. Otol. Neurotol. 2018, 39, 65–72. [Google Scholar] [CrossRef]
- Komune, N.; Noda, T.; Kogo, R.; Miyazaki, M.; Tsuchihashi, N.A.; Hongo, T.; Koike, K.; Sato, K.; Uchi, R.; Wakasaki, T.; et al. Primary Advanced Squamous Cell Carcinoma of the Temporal Bone: A Single-Center Clinical Study. Laryngoscope 2021, 131, E583–E589. [Google Scholar] [CrossRef]
- Nakagawa, T.; Kumamoto, Y.; Natori, Y.; Shiratsuchi, H.; Toh, S.; Kakazu, Y.; Shibata, S.; Nakashima, T.; Komune, S. Squamous cell carcinoma of the external auditory canal and middle ear: An operation combined with preoperative chemoradiotherapy and a free surgical margin. Otol. Neurotol. 2006, 27, 242–248, discussion 249. [Google Scholar] [CrossRef]
- Yin, M.; Ishikawa, K.; Honda, K.; Arakawa, T.; Harabuchi, Y.; Nagabashi, T.; Fukuda, S.; Taira, A.; Himi, T.; Nakamura, N.; et al. Analysis of 95 cases of squamous cell carcinoma of the external and middle ear. Auris Nasus Larynx 2006, 33, 251–257. [Google Scholar] [CrossRef]
- Howard, B.E.; Nagel, T.H.; Barrs, D.M.; Donald, C.B.; Hayden, R.E. Reconstruction of Lateral Skull Base Defects: A Comparison of the Submental Flap to Free and Regional Flaps. Otolaryngol. Head Neck Surg. 2016, 154, 1014–1018. [Google Scholar] [CrossRef]
- Moncrieff, M.D.; Hamilton, S.A.; Lamberty, G.H.; Malata, C.M.; Hardy, D.G.; Macfarlane, R.; Moffat, D.A. Reconstructive options after temporal bone resection for squamous cell carcinoma. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 607–614. [Google Scholar] [CrossRef]
- Moore, M.G.; Lin, D.T.; Mikulec, A.A.; McKenna, M.J.; Varvares, M.A. The occipital flap for reconstruction after lateral temporal bone resection. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 587–591. [Google Scholar] [CrossRef] [Green Version]
- Resto, V.A.; McKenna, M.J.; Deschler, D.G. Pectoralis major flap in composite lateral skull base defect reconstruction. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Iida, T.; Mihara, M.; Yoshimatsu, H.; Narushima, M.; Koshima, I. Reconstruction of the external auditory canal using a super-thin superficial circumflex iliac perforator flap after tumour resection. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 430–433. [Google Scholar] [CrossRef]
- Homer, J.J.; Lesser, T.; Moffat, D.; Slevin, N.; Price, R.; Blackburn, T. Management of lateral skull base cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S119–S124. [Google Scholar] [CrossRef]
- Patel, N.S.; Modest, M.C.; Brobst, T.D.; Carlson, M.L.; Price, D.L.; Moore, E.J.; Janus, J.R. Surgical management of lateral skull base defects. Laryngoscope 2016, 126, 1911–1917. [Google Scholar] [CrossRef]
- Morimoto, C.; Nishimura, T.; Hosoi, H.; Saito, O.; Fukuda, F.; Shimokura, R.; Yamanaka, T. Sound transmission by cartilage conduction in ear with fibrotic aural atresia. J. Rehabil. Res. Dev. 2014, 51, 325–332. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Pathology | cT | Sex | Age | Side | Approach | Reconstruction | Ope Time | Surgeon | Margin | PORT | (Gy) | BCA | Aided ABG (dB) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ENT | Plastic | |||||||||||||||
| With EAC reconstruction | 1 | w-m SCC | 1 | F | 74 | R | LTBR | ALT | 9 h 22 min | NM | SY | − | − | 0 | − | - |
| 2 | w-m SCC | 1 | M | 62 | R | LTBR | ALT | 10 h 26 min | TN/NM | KK | − | − | 0 | − | - | |
| 3 | w SCC | 1 | F | 61 | R | LTBR | ALT | 10 h 19 min | NM | RS/SY | + | + | 60 | − | - | |
| 4 | w SCC | 1 | F | 78 | R | LTBR | ALT | 6 h 41 min | NM | SY | − | − | 0 | − | - | |
| 5 | w SCC | 4 | F | 72 | R | LTBR | ALT | 10 h 41 min | NK | RS | + | + | 60 | − | 30 | |
| 6 | w-m SCC | 4 | F | 66 | R | LTBR | Groin | 9 h 00 min | NK | SY | − | − | 0 | − | 38.75 | |
| 7 | ACC | 1 | F | 83 | R | LTBR | ALT | 9 h 39 min | NM | SY | − | − | 0 | − | - | |
| 8 | ACC | 2 | M | 58 | R | LTBR | Groin | 9 h 53 min | TNo/NK | HK | + | + | 60 | − | 27.5 | |
| 9 | ACC | 4 | F | 76 | L | LTBR | ALT | 14 h 19 min | TNo/NK | RS | + | + | 70 | − | −3.75 | |
| Without EAC reconstruction | 10 | w SCC | 4 | F | 33 | R | LTBR | ALT | 17 h 57 min | TNo/NK | KI | + | + | 60 | + | 20 |
| 11 | w-m SCC | 2 | F | 67 | R | LTBR | ALT | 12 h 44 min | NK | RS/KI | − | + | 50 | + | 11.25 | |
| 12 | w SCC | 2 | M | 56 | L | LTBR | PAT | 5 h 32 min | NK | RS | − | − | 0 | + | 7.5 | |
| 13 | w SCC | 2 | F | 55 | L | LTBR | ALT | 8 h 56 min | NK | SY | − | + | 60 | + | 17.5 | |
| 14 | w SCC | 4 | F | 66 | L | LTBR | ALT | 13 h 8 min | NK | RS | − | − | 0 | + | 36.25 | |
| 15 | w-p SCC | 2 | F | 69 | L | LTBR | TM | 7 h 30 min | NK | NK | − | + | 60 | − | 30 | |
| 16 | w SCC | 4 | F | 48 | L | LTBR | ALT | 15 h 38 min | NK | SF | − | − | 0 | − | 41.25 | |
| 17 | w SCC | 1 | F | 68 | L | LTBR | ALT | 9 h 36 min | NK | HK | − | − | 0 | − | 35 | |
| 18 | w SCC | 4 | F | 60 | R | LTBR | ALT | 10 h 21 min | NK | KI | − | − | 0 | − | 23.75 | |
| 19 | w SCC | 3 | F | 66 | R | LTBR | TM | 6 h 31 min | NK | NK | − | − | 0 | − | 13.75 | |
| 20 | w SCC | 4 | F | 71 | R | LTBR | ALT | 12 h 48 min | NK | CO | − | + | 60 | − | 7.5 | |
| 21 | w SCC | 2 | M | 66 | L | LTBR | PAT | 6 h 51 min | NK | YI | − | − | 0 | − | 1.25 | |
| Hearing Loss Compensation after Temporal Bone Resection | ||
| Advantages | Disadvantages | |
| Free Flap Reconstruction | ||
| 1. The possibility to maintain the hearing level without hearing aid | 1. The postoperative volume of the flap can’t be predicted preoperatively. Thusly, surgeon should explain the staged surgery to reduce the volume of the flap to maintain the external ear canal if necessary | |
| 2. The easy detection of the tumor recurrence through the canal | 2. Need to clean the auditory canal regularly | |
| 3. The possibility to use the hearing aid with ear mold | 3. The possibility of recurrent tumor exposure | |
| 4. The ear mold is needed to be renewed depends on the volume of the flap | ||
| Local Flap Reconstruction | ||
| 1. Less invasive | 1. Deterioration of the conductive hearing loss and otorrhea, caused by Stenosis, Contracture, chronic infection and bone exposure | |
| 2. The possibility to maintain the hearing level without hearing aid | 2. Delay wound healing | |
| 3. The easy detection of the tumor recurrence through the canal | 3. Dual local flaps and skin grafting are often needed | |
| 4. The possibility to use the hearing aid with ear mold | 4. Need to clean the auditory canal regularly | |
| Bone Conductive Haring Aid (No ear canal) | ||
| 1. No need of postoperative clean-up of the auditory canal | 1. Strong contact to the skin and pressure against the cranial bone of bone-conductive hearing aid cause the skin erosion and patient’s pain. | |
| 2. The maintain the hearing level with hearing aid | 2. Residual and recurrent disease need to be detected only by radiological examination. | |
| 3. Prevent the tumor exposure when the tumor is recurrent | 3. Expensive (purchasing expense, repair cost, etc.) | |
| Cartilage Conductive Hearing (No ear canal) | ||
| 1. No need of postoperative clean-up of the auditory canal | 1. Residual and recurrent disease need to be detected only by radiological examination. | |
| 2. Hearing aid is small and right | 2. Expensive (purchasing expense, repair cost, etc.) | |
| 3. Prevent the tumor exposure when the tumor is recurrent | ||
| 4. No strong pressure to the skin and cranial bone | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komune, N.; Higashino, Y.; Ishikawa, K.; Tabuki, T.; Masuda, S.; Koike, K.; Hongo, T.; Sato, K.; Uchi, R.; Miyazaki, M.; et al. Management of Residual Hearing with Cartilage Conduction Hearing Aid after Lateral Temporal Bone Resection: Our Institutional Experience. Audiol. Res. 2021, 11, 263-274. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020024
Komune N, Higashino Y, Ishikawa K, Tabuki T, Masuda S, Koike K, Hongo T, Sato K, Uchi R, Miyazaki M, et al. Management of Residual Hearing with Cartilage Conduction Hearing Aid after Lateral Temporal Bone Resection: Our Institutional Experience. Audiology Research. 2021; 11(2):263-274. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020024
Chicago/Turabian StyleKomune, Noritaka, Yoshie Higashino, Kazuha Ishikawa, Tomoko Tabuki, Shogo Masuda, Kensuke Koike, Takahiro Hongo, Kuniaki Sato, Ryutaro Uchi, Masaru Miyazaki, and et al. 2021. "Management of Residual Hearing with Cartilage Conduction Hearing Aid after Lateral Temporal Bone Resection: Our Institutional Experience" Audiology Research 11, no. 2: 263-274. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020024