
Hearing Screening among First-Grade Children in Rural Areas and Small Towns in Małopolskie Voivodeship, Poland

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Data Analysis
3. Results
3.1. Positive Results of Hearing Screening
3.2. Prevalence of Hearing Loss
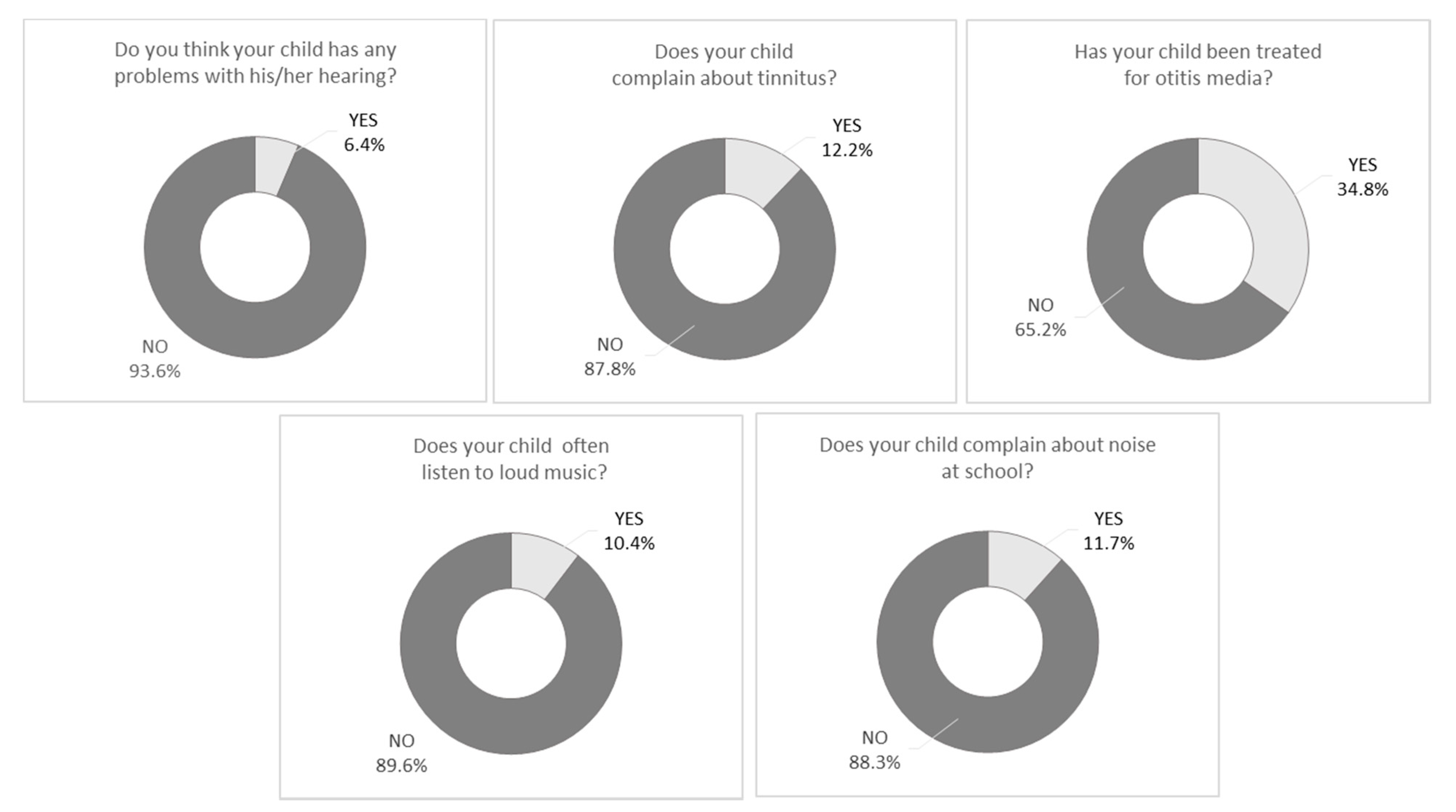
3.3. Questionnaire Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A Systematic analysis for the global burden of disease study 2015. Lancet Lond. Engl. 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Schick, B.; Skalicky, A.; Edwards, T.; Kushalnagar, P.; Topolski, T.; Patrick, D. School placement and perceived quality of life in youth who are deaf or hard of hearing. J. Deaf. Stud. Deaf. Educ. 2013, 18, 47–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgalas, C.; Xenellis, J.; Davilis, D.; Tzangaroulakis, A.; Ferekidis, E. Screening for hearing loss and middle-ear effusion in school-age children, using transient evoked otoacoustic emissions: A feasibility study. J. Laryngol. Otol. 2008, 122, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Fortnum, H.; Ukoumunne, O.C.; Hyde, C.; Taylor, R.S.; Ozolins, M.; Errington, S.; Zhelev, Z.; Pritchard, C.; Benton, C.; Moody, J.; et al. A programme of studies including assessment of diagnostic accuracy of school hearing screening tests and a cost-effectiveness model of school entry hearing screening programmes. Health Technol. Assess. Winch. Engl. 2016, 20, 1–178. [Google Scholar] [CrossRef] [Green Version]
- Kocoń, S.; Wiatr, M.; Stręk, P.; Wiatr, A.; Ziarno, A.; Hartwich, P. Analysis of difficulties occurring during the early auditory screening in children. Otolaryngol. Pol. 2016, 70, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, B.D.; Skowronski, D.M.; Stewart, I.F.; Stewart, L.; Bernauer, M.; Mudarikwa, L. Prevalence of hearing loss in primary school children in Zimbabwe. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Skarżyński, H.; Piotrowska, A. Prevention of communication disorders—Screening Pre-school and school-age children for problems with hearing, vision and speech: European consensus statement. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2012, 18, SR17–SR21. [Google Scholar] [CrossRef] [Green Version]
- Swanepoel, D.W.; Maclennan-Smith, F.; Hall, J.W. Diagnostic pure-tone audiometry in schools: Mobile testing without a sound-treated environment. J. Am. Acad. Audiol. 2013, 24, 992–1000. [Google Scholar] [CrossRef]
- Thorne, J.A. Middle Ear problems in Aboriginal school children cause developmental and educational concerns. Contemp. Nurse 2004, 16, 145–150. [Google Scholar] [CrossRef]
- Clark, J.L. Hearing loss in Mozambique: Current data from Inhambane Province. Int. J. Audiol. 2008, 47 (Suppl. 1), S49–S56. [Google Scholar] [CrossRef]
- Minja, B.M.; Machemba, A. Prevalence of otitis media, hearing impairment and cerumen impaction among school children in rural and urban Dar Es Salaam, Tanzania. Int. J. Pediatr. Otorhinolaryngol. 1996, 37, 29–34. [Google Scholar] [CrossRef]
- Gan, R.W.C.; Overton, P.; Benton, C.; Daniel, M. Hearing aids for otitis media with effusion: Do children use them? Int. J. Pediatr. Otorhinolaryngol. 2017, 99, 117–119. [Google Scholar] [CrossRef]
- Browning, G.G.; Rovers, M.M.; Williamson, I.; Lous, J.; Burton, M.J. Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children. Cochrane Database Syst. Rev. 2010, CD001801. [Google Scholar] [CrossRef] [PubMed]
- Botasso, M.; Sanches, S.G.G.; Bento, R.F.; Samelli, A.G.; Botasso, M.; Sanches, S.G.G.; Bento, R.F.; Samelli, A.G. Teleaudiometry as a screening method in school children. Clinics 2015, 70, 283–288. [Google Scholar] [CrossRef]
- Yong, M.; Liang, J.; Ballreich, J.; Lea, J.; Westerberg, B.D.; Emmett, S.D. Cost-effectiveness of school hearing screening programs: A scoping review. Otolaryngol. Neck Surg. 2020, 162, 826–838. [Google Scholar] [CrossRef] [PubMed]
- Skarżyński, H.; Piotrowska, A. Screening for pre-school and school-age hearing problems: European consensus statement. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 120–121. [Google Scholar] [CrossRef]
- Śliwa, L.; Hatzopoulos, S.; Kochanek, K.; Piłka, A.; Senderski, A.; Skarżyński, P.H. A comparison of audiometric and objective methods in hearing screening of school children. A preliminary study. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 483–488. [Google Scholar] [CrossRef]
- Skarzynski, P.H.; Kochanek, K.; Skarzynski, H.; Senderski, A.; Wysocki, J.; Szkielkowska, A.; Bartnik, G.; Lorens, A.; Piotrowska, A.; Sliwa, L.; et al. Hearing screening program in school-age children in Western Poland. Int. Adv. Otol. 2011, 7, 194–200. [Google Scholar]
- Skarzynski, P.H.; Wlodarczyk, A.W.; Kochanek, K.; Pilka, A.; Jedrzejczak, W.W.; Olszewski, L.; Bruski, L.; Niedzielski, A.; Skarzynski, H. Central Auditory Processing Disorder (CAPD) Tests in a school-age hearing screening programme—Analysis of 76,429 children. Ann. Agric. Environ. Med. AAEM 2015, 22, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Skarzynski, H.; Kochanek, K.; Senderski, A.; Skarzynski, P.H.; Ludwikowski, M.; Kopaczewski, M.; Bruski, L. Organization of the hearing screening examinations in Polish schools in rural areas and small towns. Cochlear Implant. Int. 2010, 11 (Suppl. 1), 143–147. [Google Scholar] [CrossRef]
- Skarzyński, P.H.; Świerniak, W.; Piłka, A.; Skarżynska, M.B.; Włodarczyk, A.W.; Kholmatov, D.; Makhamadiev, A.; Hatzopoulos, S. A Hearing Screening program for children in primary schools in Tajikistan: A telemedicine model. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2016, 22, 2424–2430. [Google Scholar] [CrossRef] [Green Version]
- Skarżyński, H.; Gos, E.; Świerniak, W.; Skarżyński, P.H. Prevalence of hearing loss among Polish school-age children from rural areas—Results of hearing screening program in the sample of 67 416 children. Int. J. Pediatr. Otorhinolaryngol. 2019, 128, 109676. [Google Scholar] [CrossRef]
- Tyler, R.S.; Wood, E.J. A comparison of manual methods for measuring hearing levels. Audiol. Off. Organ Int. Soc. Audiol. 1980, 19, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Skarżyński, P.H.; Łuszcz, C.; Świerniak, W.; Tarczyński, K.; Matusiak, M.; Włodarczyk, A.W.; Skarżyński, H. Hearing screening of school children in the Warmian-Masurian voivodeship. J. Hear. Sci. 2020, 9, 36–44. [Google Scholar] [CrossRef]
- Feder, K.P.; Michaud, D.; McNamee, J.; Fitzpatrick, E.; Ramage-Morin, P.; Beauregard, Y. Prevalence of hearing loss among a representative sample of canadian children and adolescents, 3 to 19 years of age. Ear Hear. 2017, 38, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skarżyński, P.H.; Świerniak, W.; Gos, E.; Pierzyńska, I.; Walkowiak, A.; Cywka, K.B.; Wołujewicz, K.; Skarżyński, H. Results of hearing screening of school-age children in Bishkek, Kyrgyzstan. Prim. Health Care Res. Dev. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.; Tabangin, M.; Meinzen-Derr, J.; Cohen, A.P.; Greinwald, J.H. High-frequency sensorineural hearing loss in children. Laryngoscope 2016, 126, 1236–1240. [Google Scholar] [CrossRef]
- Niskar, A.S.; Kieszak, S.M.; Holmes, A.; Esteban, E.; Rubin, C.; Brody, D.J. Prevalence of hearing loss among children 6 to 19 years of age: The third national health and nutrition examination survey. JAMA 1998, 279, 1071–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skarżyński, P.H.; Piłka, A.; Ludwikowski, M.; Skarżyńska, M.B. Comparison of the frequency of positive hearing screening outcomes in schoolchildren from Poland and other countries of Europe, Central Asia, and Africa. J. Hear. Sci. 2014, 4, 51–58. [Google Scholar]
- Ross, D.S.; Holstrum, W.J.; Gaffney, M.; Green, D.; Oyler, R.F.; Gravel, J.S. Hearing screening and diagnostic evaluation of children with unilateral and mild bilateral hearing loss. Trends Amplif. 2008, 12, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Sarafraz, M.; Ahmadi, K. A Practical Screening model for hearing loss in Iranian school-aged children. World J. Pediatr. 2009, 5, 46–50. [Google Scholar] [CrossRef]
- Govender, S.; Latiff, N.; Asmal, N.; Ramsaroop, S.; Mbele, T. Evaluating the outcomes of a hearing screening service for grade one learners in urban areas at Durban, South Africa. J. Public Health Afr. 2015, 6. [Google Scholar] [CrossRef] [Green Version]
- Piotrowska, A.; Zapert, A.; Tarczyński, K.; Kochanek, K. Analiza wybranych parametrów audiometrycznych przesiewowych badań słuchu wykonywanych w szkołach. N. Audiofonol. 2014, 3, 9–13. [Google Scholar]
- Mahomed-Asmail, F.; Swanepoel, D.W.; Eikelboom, R.H. Hearing loss in urban South African school children (grade 1 to 3). Int. J. Pediatr. Otorhinolaryngol. 2016, 84, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Bess, F.H. The minimally hearing-impaired child. Ear Hear. 1985, 6, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Czech, D.; Malicka, M.; Kott, E.; Zakrzewska, A. Ocena występowania zaburzeń artykulacyjnych u dzieci z nawracającymi infekcjami górnych dróg oddechowych. Otolaryngol. Przegląd Klin. 2011, 10, 116–120. [Google Scholar]
- Minovi, A.; Dazert, S. Diseases of the middle ear in childhood. GMS. Curr. Top. Otorhinolaryngol. Head Neck Surg. 2014, 13, Doc11. [Google Scholar] [CrossRef]
- Skarżyński, P.H.; Ludwikowski, M. Hearing screening around the world. Excursus Hear. Loss 2018. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, S.A.; Saunders, K.; Osborn, A.H.; Arnold, A.; Wunderlich, J.; Kelly, T.; Collins, V.; Wilcox, L.J.; McKinlay Gardner, R.; Kamarinos, M.; et al. High frequency hearing loss correlated with mutations in the GJB2 gene. Hum. Genet. 2000, 106, 399–405. [Google Scholar] [CrossRef]
- Stelmachowicz, P.G.; Pittman, A.L.; Hoover, B.M.; Lewis, D.E.; Moeller, M.P. The importance of high-frequency audibility in the speech and language development of children with hearing loss. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 556–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, D.S.; Visser, S.N.; Holstrum, W.J.; Qin, T.; Kenneson, A. Highly variable population-based prevalence rates of unilateral hearing loss after the application of common case definitions. Ear Hear. 2010, 31, 126–133. [Google Scholar] [CrossRef]
- Vila, P.; Lieu, J.E.C. Asymmetric and unilateral hearing loss in children. Cell Tissue Res. 2015, 361, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watkin, P.M.; Baldwin, M.; Laoide, S. Parental suspicion and identification of hearing impairment. Arch. Dis. Child. 1990, 65, 846–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engel, J.; Anteunis, L.; Volovics, A.; Hendriks, J.; Marres, E. Predictive value of parent-reported symptoms in the assessment of otitis media with effusion during infancy. Scand. J. Prim. Health Care 2000, 18, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, P.S.Y.; Tong, M.C.F.; Wong, E.M.C.; van Hasselt, C.A. Parental suspicion of hearing loss in children with otitis media with effusion. Eur. J. Pediatr. 2006, 165, 851–857. [Google Scholar] [CrossRef]
- Rosing, S.N.; Schmidt, J.H.; Wedderkopp, N.; Baguley, D.M. Prevalence of tinnitus and hyperacusis in children and adolescents: A systematic review. BMJ Open 2016, 6, e010596. [Google Scholar] [CrossRef] [Green Version]
- Raj-Koziak, D.; Skarżyński, H.; Kochanek, K.; Fabijańska, A. [The prevalence of tinnitus in children in Poland]. Otolaryngol. Pol. 2013, 67, 149–153. [Google Scholar] [CrossRef]
- Niskar, A.S.; Kieszak, S.M.; Holmes, A.E.; Esteban, E.; Rubin, C.; Brody, D.J. Estimated prevalence of noise-induced hearing threshold shifts among children 6 to 19 years of age: The third national health and nutrition examination survey, 1988–1994, United States. Pediatrics 2001, 108, 40–43. [Google Scholar] [CrossRef]
- Henderson, E.; Testa, M.A.; Hartnick, C. Prevalence of noise-induced hearing-threshold shifts and hearing loss among US youths. Pediatrics 2011, 127, e39–e46. [Google Scholar] [CrossRef]
- le Clercq, C.M.P.; Goedegebure, A.; Jaddoe, V.W.V.; Raat, H.; Baatenburg de Jong, R.J.; van der Schroeff, M.P. Association between portable music player use and hearing loss among children of school age in the Netherlands. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 668–675. [Google Scholar] [CrossRef] [Green Version]
- Sulkowski, W.J.; Kochanek, K.; Jalocha-Kaczka, A.; Owczarek, K.; Olszewski, J. Music-induced hearing loss in schoolage children: Data from a questionnaire, otological examination, and audiometry. J. Hear. Sci. 2020, 8, 9–15. [Google Scholar] [CrossRef]
- Jamieson, D.G.; Kranjc, G.; Yu, K.; Hodgetts, W.E. Speech intelligibility of young school-aged children in the presence of real-life classroom noise. J. Am. Acad. Audiol. 2004, 15, 508–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harmes, K.; Blackwood, R.A.; Burrows, H.; Cooke, J.M.; Harrison, R.V.; Passamani, P. Otitis media: Diagnosis and treatment. Am. Fam. Physician 2013, 88, 435–440. [Google Scholar] [PubMed]
- Arrieta, A.; Singh, J. Management of recurrent and persistent acute otitis media: New options with familiar antibiotics. Pediatr. Infect. Dis. J. 2004, 23, S115–S124. [Google Scholar] [CrossRef] [PubMed]
- Krzyżak, A.; Zagólski, O.; Pawełek, M.; Stręk, P. Paediatric otitis media with effusion is connected to deficits in music perception. Logoped. Phoniatr. Vocol. 2017, 43, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Gunasekera, H.; Morris, P.S.; McIntyre, P.; Craig, J.C. Management of children with otitis media: A summary of evidence from recent systematic reviews. J. Paediatr. Child Health 2009, 45, 554–563. [Google Scholar] [CrossRef]


{kind=link}
| FFPTA and/or LFPTA and/or HFPTA HL | FFPTA HL | LFPTA HL | HFPTA HL | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | |
| Total | 5029 | 581 | 11.6 | 10.7–12.4 | 328 | 6.5 | 5.8–7.2 | 410 | 8.2 | 7.4–8.9 | 384 | 7.6 | 6.9–8.4 |
| Girls | 2281 | 257 | 11.3 | 10.0–12.6 | 163 | 7.1 | 6.1–8.2 | 200 | 8.8 | 7.6–9.9 | 157 | 6.9 | 5.8–7.9 |
| Boys | 2784 | 324 | 11.8 | 10.6–13.0 | 165 | 6.0 | 5.1–6.9 | 210 | 7.6 | 6.6–8.6 | 227 | 8.3 | 7.2–9.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swierniak, W.; Skarzynski, P.H.; Gos, E.; Czajka, N.; Matusiak, M.; Hartwich, P.; Skarzynska, M.B. Hearing Screening among First-Grade Children in Rural Areas and Small Towns in Małopolskie Voivodeship, Poland. Audiol. Res. 2021, 11, 275-283. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020025
Swierniak W, Skarzynski PH, Gos E, Czajka N, Matusiak M, Hartwich P, Skarzynska MB. Hearing Screening among First-Grade Children in Rural Areas and Small Towns in Małopolskie Voivodeship, Poland. Audiology Research. 2021; 11(2):275-283. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020025
Chicago/Turabian StyleSwierniak, Weronika, Piotr Henryk Skarzynski, Elzbieta Gos, Natalia Czajka, Monika Matusiak, Patryk Hartwich, and Magdalena Beata Skarzynska. 2021. "Hearing Screening among First-Grade Children in Rural Areas and Small Towns in Małopolskie Voivodeship, Poland" Audiology Research 11, no. 2: 275-283. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020025