
Skull Vibration-Induced Nystagmus Test in a Human Model of Horizontal Canal Plugging

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Methods
2.2.1. Skull Vibration-Induced Nystagmus Test (SVINT)
2.2.2. Caloric Test (CaT)
2.2.3. Head Shaking Test (HST)
2.2.4. Video Head Impulse Test (VHIT)
2.2.5. Cervical Vestibular-Evoked Myogenic Potentials (cVEMP)
2.2.6. Audiogram and Subjective Scales
2.3. Statistical Analysis
3. Results
3.1. Vestibular Results
3.2. Correlations between the Different Vestibular Tests
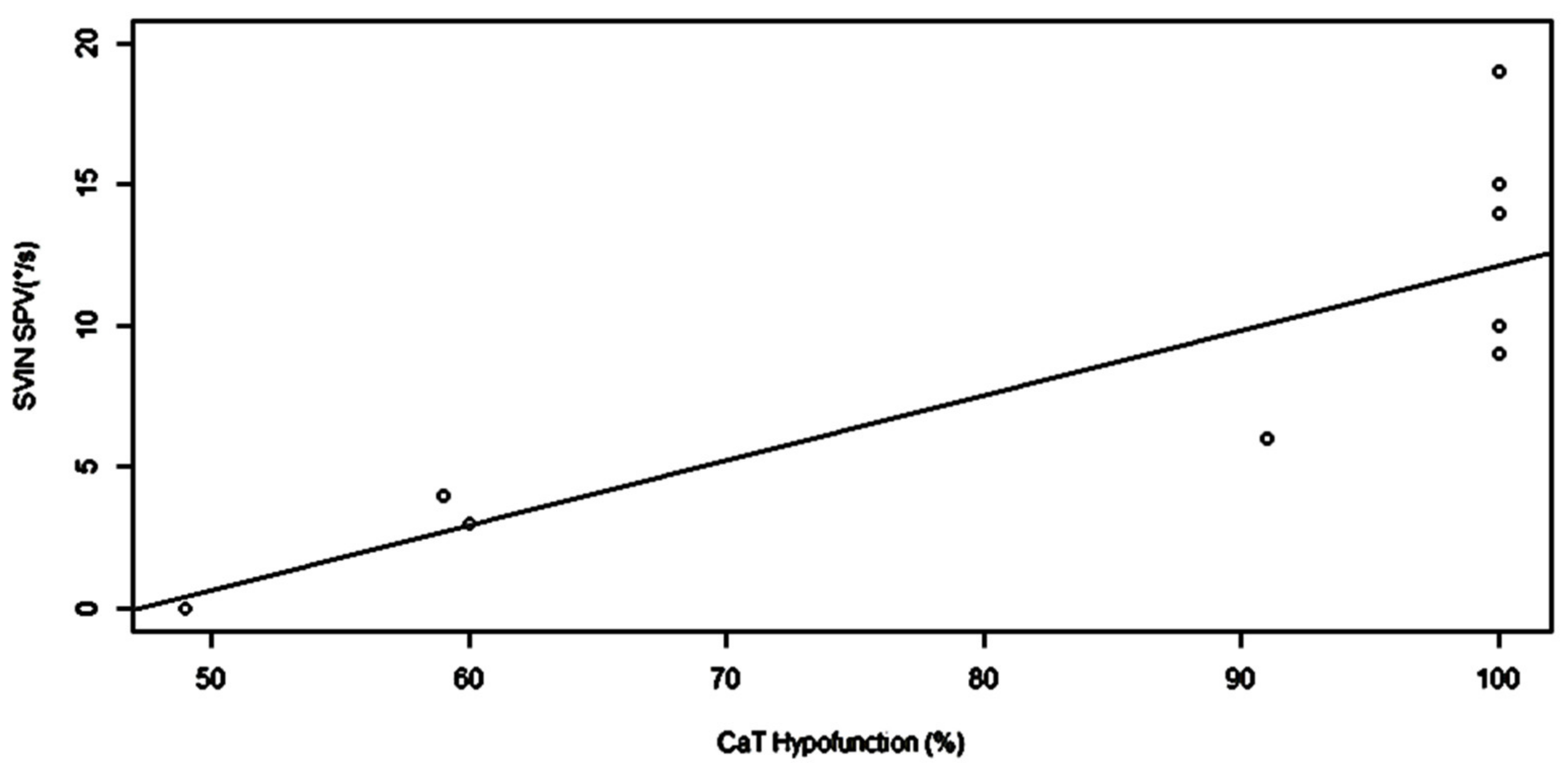
- VIN beating contralaterally vs. CAT ipsilateral hypofunction: p > 0.99 (the tests are identical);
- VIN beating contralaterally vs. VHIT ipsilateral hypofunction: p > 0.99 (the tests are identical);
- VIN beating contralaterally vs. cVEMP ipsilateral hypofunction: p = 0.02 (the two tests are different);
- VIN beating contralaterally vs. HST positivity: p = 0.62 (the two tests are identical).
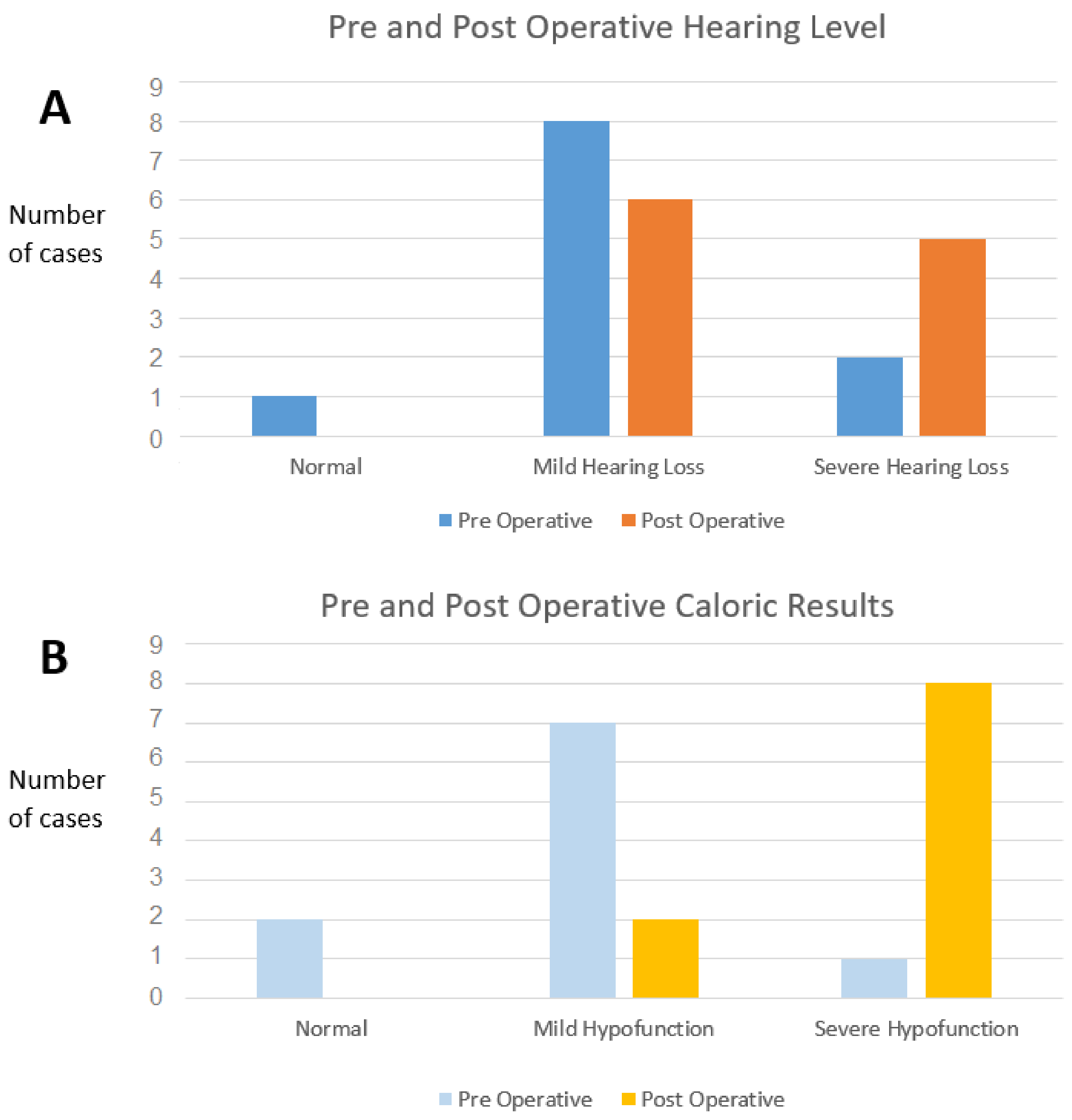
3.3. Pre- and Postoperative Audiometry and Caloric Tests
3.4. Subjective Scales
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charpiot, A.; Rohmer, D.; Gentine, A. Lateral semicircular canal plugging in severe Ménière’s disease: A clinical prospective study about 28 patients. Otol. Neurotol. 2010, 31, 237–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumas, G.; Perrin, P.; Schmerber, S. Nystagmus induced by high frequency vibrations of the skull in total unilateral peripheral vestibular lesions. Acta Otolaryngol. 2008, 128, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Dumas, G.; Perrin, P.; Ouedraogo, E.; Schmerber, S. How to perform the skull vibration-induced nystagmus test (SVINT). Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 343–348. [Google Scholar] [CrossRef]
- Dumas, G.; Curthoys, I.S.; Lion, A.; Perrin, P.; Schmerber, S. The Skull Vibration-Induced Nystagmus Test of Vestibular Function-A Review. Front. Neurol. 2017, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Curthoys, I.S. The new vestibular stimuli: Sound and vibration-anatomical, physiological and clinical evidence. Exp. Brain Res. 2017, 235, 957–972. [Google Scholar] [CrossRef] [PubMed]
- Curthoys, I.S.; Vulovic, V.; Burgess, A.M.; Manzari, L.; Sokolic, L.; Pogson, J.; Robins, M.; Mezey, L.E.; Goonetilleke, S.; Cornell, E.D.; et al. Neural basis of new clinical vestibular tests: Otolithic neural responses to sound and vibration. Clin. Exp. Pharmacol. Physiol. 2014, 41, 371–380. [Google Scholar] [CrossRef]
- Curthoys, I.S.; Grant, J.W. How does high-frequency sound or vibration activate vestibular receptors? Exp. Brain Res. 2015, 233, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, R.; Klinke, R. Discharge properties of afferent fibres of the goldfish semicircular canal with high frequency stimulation. Pflügers Arch. 1980, 388, 111–121. [Google Scholar] [CrossRef]
- Dumas, G.; Lion, A.; Perrin, P.; Ouedraogo, E.; Schmerber, S. Topographic analysis of the skull vibration-induced nystagmus test with piezoelectric accelerometers and force sensors. Neuroreport 2016, 27, 318–322. [Google Scholar] [CrossRef]
- Dumas, G.; Schmerber, S. Comment faire un examen calorique. Ann. Otolaryngol. Chir. Cervico-Faciale 2005, 122, 315–318. [Google Scholar] [CrossRef]
- Hain, T.C. Head-shaking nystagmus and new technology. Neurology 2007, 68, 1333–1334. [Google Scholar] [CrossRef] [PubMed]
- McGarvie, L.A.; MacDougall, H.G.; Halmagyi, G.M.; Burgess, A.M.; Weber, K.P.; Curthoys, I.S. The Video Head Impulse Test (vHIT) of Semicircular Canal Function-Age-Dependent Normative Values of VOR Gain in Healthy Subjects. Front. Neurol. 2015, 6, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, F.; Simon, F.; Verillaud, B.; Herman, P.; Kania, R.; Hautefort, C. Comparison of Video Head Impulse Test and Caloric Reflex Test in advanced unilateral definite Menière’s disease. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Blödow, A.; Heinze, M.; Bloching, M.B.; von Brevern, M.; Radtke, A.; Lempert, T. Caloric stimulation and video-head impulse testing in Ménière’s disease and vestibular migraine. Acta Otolaryngol. 2014, 134, 1239–1244. [Google Scholar] [CrossRef]
- Nakashima, T.; Pyykkö, I.; Arroll, M.A.; Casselbrant, M.L.; Foster, C.A.; Manzoor, N.F.; Megerian, C.A.; Naganawa, S.; Young, Y.-H. Meniere’s disease. Nat. Rev. Dis. Primers 2016, 2, 16028. [Google Scholar] [CrossRef]
- Xu, M.; Chen, Z.C.; Wei, X.Y.; Zhang, Y.Z.; Yang, F.Y.; Zhang, C.; Chen, F.Y.; Hu, J.; Cheng, Y.; Zhang, Q. [Evaluation of vestibular evoked myogenic potential, caloric test and cochlear electrogram in the diagnosis of Meniere’s disease]. J. Clin. Otorhinolaryngol. Head Neck Surg. 2019, 33, 704–708. [Google Scholar]
- Limviriyakul, S.; Luangsawang, C.; Suvansit, K.; Prakairungthong, S.; Thongyai, K.; Atipas, S. Video head impulse test and caloric test in definite Ménière’s disease. Eur. Arch. Otorhinolaryngol. 2020, 277, 679–686. [Google Scholar] [CrossRef]
- McGarvie, L.A.; Curthoys, I.S.; MacDougall, H.G.; Halmagyi, G.M. What does the dissociation between the results of video head impulse versus caloric testing reveal about the vestibular dysfunction in Ménière’s disease? Acta Otolaryngol. 2015, 135, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Paige, G.D. Caloric responses after horizontal canal inactivation. Acta Otolaryngol. 1985, 100, 321–327. [Google Scholar] [CrossRef]
- Dumas, G.; Karkas, A.; Perrin, P.; Chahine, K.; Schmerber, S. High-frequency skull vibration-induced nystagmus test in partial vestibular lesions. Otol. Neurotol. 2011, 32, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Rabbitt, R.D.; Boyle, R.; Highstein, S.M. Physiology of the semicircular canals after surgical plugging. Ann. N. Y. Acad. Sci. 2001, 942, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Batuecas-Caletrío, A.; Martínez-Carranza, R.; García Nuñez, G.M.; Fernández Nava, M.J.; Sánchez Gómez, H.; Santacruz Ruiz, S.; Pérez Guillén, V.; Pérez-Fernández, N. Skull vibration-induced nystagmus in vestibular neuritis. Acta Otolaryngol. 2020, 140, 995–1000. [Google Scholar] [CrossRef]
- Lee, S.-U.; Kee, H.-J.; Sheen, S.S.; Choi, B.Y.; Koo, J.-W.; Kim, J.-S. Head-shaking and Vibration-induced Nystagmus During and Between the Attacks of Unilateral Ménière’s Disease. Otol. Neurotol. 2015, 36, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Teggi, R.; Battista, R.A.; Di Berardino, F.; Familiari, M.; Cangiano, I.; Gatti, O.; Bussi, M. Evaluation of a large cohort of adult patients with Ménière’s disease: Bedside and clinical history. Acta Otorhinolaryngol. Ital. 2020, 40, 444–449. [Google Scholar] [CrossRef]
- Dumas, G.; Fabre, C.; Perottino, F.; Tan, H.; Proy, P.; Schmerber, S. Skull vibration induced nystagmus test in Ménière’s disease. Otorinolaryngologia 2020, 70, 121–127. [Google Scholar]
- Chen, L.; Xu, H.; Wang, W.-Q.; Zhang, Q.-Q.; Lv, Q.-Y.; Song, X.-C. Evaluation of the otolith function using c/oVEMPs in patients with Ménière’s disease. J. Otolaryngol. Head Neck Surg. 2016, 45, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dlugaiczyk, J.; Burgess, A.M.; Curthoys, I.S. Activation of Guinea Pig Irregular Semicircular Canal Afferents by 100 Hz Vibration: Clinical Implications for Vibration-induced Nystagmus and Vestibular-evoked Myogenic Potentials. Otol. Neurotol. 2020, 41, e961–e970. [Google Scholar] [CrossRef]
- Dumas, G.; Tan, H.; Dumas, L.; Perrin, P.; Lion, A.; Schmerber, S. Skull vibration induced nystagmus in patients with superior semicircular canal dehiscence. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 263–272. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Age | Lesion Side | Hearing Loss | Subjective Scales Post Op | Caloric Test Ipsi lat Hypofunction (%) | L-VHIT Post Op(%) | HST Direction Postop | cVEMP Hypofunction Postop | SVIN-SPV Postop (°/s) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Preop. | Postop. | AAO | DHI | Preop. | Postop. | Gain Ipsilat | Asymmetry | |||||||
| 1 | M | 78 | L | Mild | Sev | 1 | 6 | NA | NA | 21 | 72 | R | L | 8 |
| 2 | F | 52 | R | Mild | Sev | 1 | 12 | 77 | 100 | 76 | 26 | L | N | 9 |
| 3 | F | 59 | L | Mild | Mild | 4 | 46 | 92 | 100 | 62 | 38 | L | N | 15 |
| 4 | M | 50 | R | N | Mild | 1 | 18 | 62 | 91 | 73 | 25 | L | R | 6 |
| 5 | M | 45 | R | Mild | Sev | 1 | 0 | 66 | 100 | 91 | 11 | N | R | 14 |
| 6 | F | 77 | R | Mild | Mild | 1 | 4 | 0 | 100 | 33 | 65 | L | N | 19 |
| 7 | M | 57 | L | Mild | Mild | 2 | 6 | 84 | 59 | 39 | 64 | R | N | 4 |
| 8 | M | 45 | L | Sev | Anacusis | 3 | 32 | 0 | 100 | 27 | 72 | N | N | 10 |
| 9 | F | 44 | R | Mild | Mild | 4 | 50 | 64 | 49 | 50 | 37 | L | N | 0 |
| 10 | M | 66 | L | Mild | Sev | 2 | 46 | 9 | 60 | 26 | 41 | N | N | 3 |
| 11 | M | 62 | R | Mild | Sev | 2 | 4 | 51 | 100 | 6 | 92 | L | R | 9 |
| Test positivity (%) | 70 | 100 | 91 | 73 | 27 | 91 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumas, G.; Fabre, C.; Charpiot, A.; Fath, L.; Chaney-Vuong, H.; Perrin, P.; Schmerber, S. Skull Vibration-Induced Nystagmus Test in a Human Model of Horizontal Canal Plugging. Audiol. Res. 2021, 11, 301-312. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11030028
Dumas G, Fabre C, Charpiot A, Fath L, Chaney-Vuong H, Perrin P, Schmerber S. Skull Vibration-Induced Nystagmus Test in a Human Model of Horizontal Canal Plugging. Audiology Research. 2021; 11(3):301-312. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11030028
Chicago/Turabian StyleDumas, Georges, Christol Fabre, Anne Charpiot, Lea Fath, Hella Chaney-Vuong, Philippe Perrin, and Sébastien Schmerber. 2021. "Skull Vibration-Induced Nystagmus Test in a Human Model of Horizontal Canal Plugging" Audiology Research 11, no. 3: 301-312. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11030028