Impacts of Coping Mechanisms on Nursing Students’ Mental Health during COVID-19 Lockdown: A Cross-Sectional Survey


Abstract
:1. Introduction
2. Methods
2.1. Design and Sample
2.2. Study Questionnaire
2.3. Data Collection Procedures
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
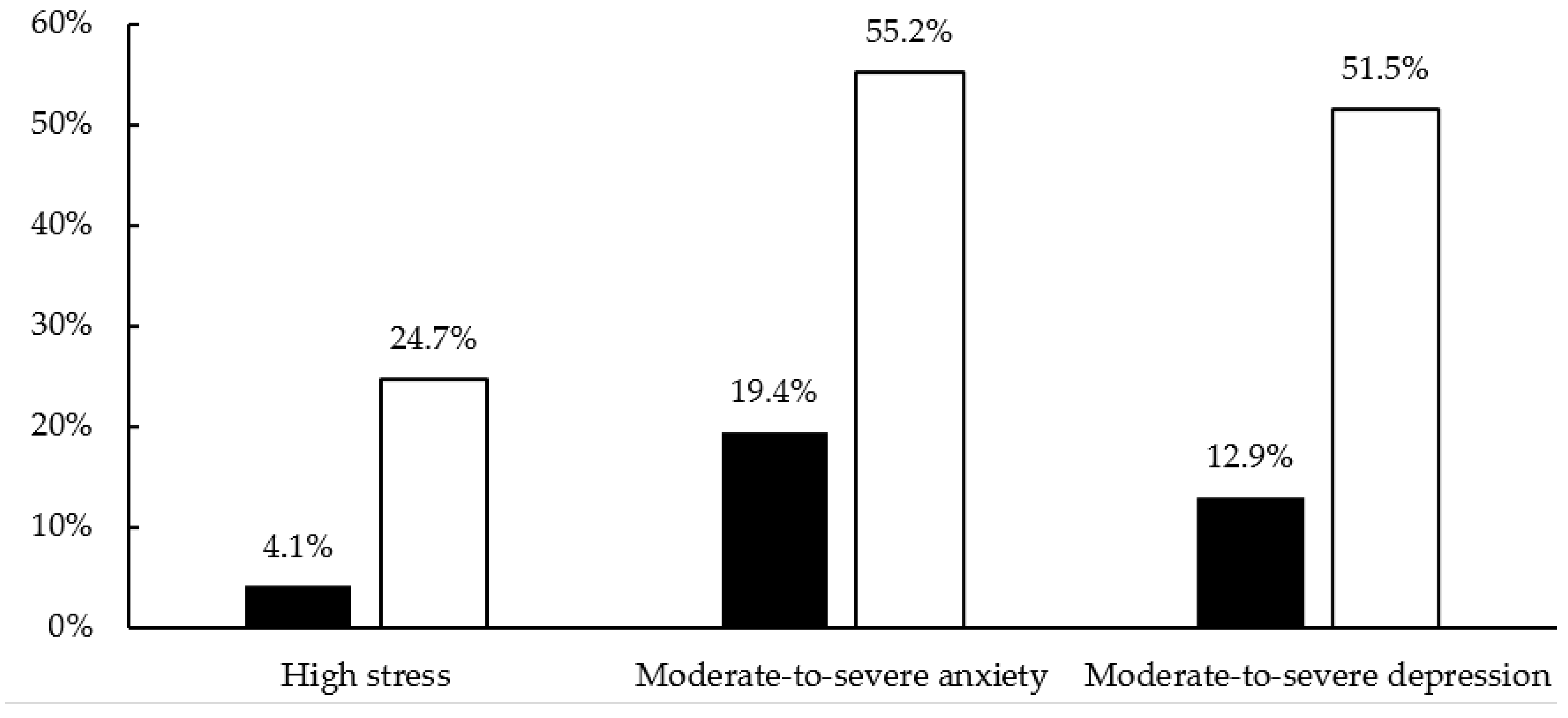
3.2. Mental Health before and during COVID-19 Lockdown
3.3. Predictors of Poor Mental Health
4. Discussion
4.1. Implications for Nursing Education
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Educational, Scientific and Cultural Organization (UNESCO). COVID-19 Educational Disruption and Response. 2020. Available online: https://en.unesco.org/covid19/educationresponse (accessed on 10 July 2020).
- Executive Department, State of California. Executive Order N-33-20. 2020. Available online: https://www.politico.com/states/f/?id=00000170-f5a4-d209-af70-fdae4c930000 (accessed on 22 June 2020).
- Dewart, G.; Corcoran, L.; Thirsk, L.; Petrovic, K. Nursing education in a pandemic: Academic challenges in response to COVID-19. Nurse Educ. Today 2020, 92, 104471. [Google Scholar] [CrossRef]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- American College Health Association. National College Health Assessment: Reference Group Executive Summary. 2018. Available online: https://www.acha.org/documents/ncha/NCHA-II_Fall_2018_Reference_Group_Executive_Summary.pdf (accessed on 7 July 2020).
- Bartlett, M.L.; Taylor, H.; Nelson, J.D. Comparison of mental health characteristics and stress between baccalaureate nursing students and non-nursing students. J. Nurs. Educ. 2016, 55, 87–90. [Google Scholar] [CrossRef]
- Chen, C.J.; Chen, Y.C.; Sung, H.C.; Hsieh, T.C.; Lee, M.S.; Chang, C.Y. The prevalence and related factors of depressive symptoms among junior college nursing students: A cross-sectional study. J. Psychiatr. Ment. Health Nurs. 2015, 22, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health. 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Zhao, H. The impact of COVID-19 on anxiety in Chinese university students. Front. Psychol. 2020, 11, 1168. [Google Scholar] [CrossRef] [PubMed]
- Savitsky, B.; Findling, Y.; Ereli, A.; Hendel, T. Anxiety and coping strategies among nursing students during the COVID-19 pandemic. Nurse Educ. Pract. 2020, 46, 102809. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Jeong, H.; Yim, H.W.; Song, Y.J.; Ki, M.; Min, J.A.; Cho, J.; Chae, J.H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, e2016048. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- Brooks, S.K.; Dunn, R.; Amlot, R.; Rubin, G.J.; Greenberg, N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, P.; Chang, S.; Yu, Y. A support group for home-quarantined college students exposed to SARS: Learning from practice. J. Spec. Group Work 2006, 30, 363–374. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.J.; Ok, U.; Robbins, M. Religion and happiness: A study among university students in Turkey. J. Relig. Health 2017, 56, 1335–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, K.; Handal, P.J.; Clark, E.M.; Vander Wal, J.S. The relationship between religion and religious coping: Religious coping as a moderator between religion and adjustment. J. Relig. Health 2009, 48, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Bryan, J.L.; Lucas, S.; Quist, M.C.; Steers, M.N.; Foster, D.W.; Young, C.M.; Lu, Q. God, can I tell you something? The effect of religious coping on the relationship between anxiety over emotional expression, anxiety, and depressive symptoms. Psychol. Relig. Spirit. 2016, 8, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Greer, T.M.; Brown, P. Minority status and coping processes among African American college students. J. Divers. High. Educ. 2011, 4, 26–38. [Google Scholar] [CrossRef]
- Cleary, M.; Visentin, D.; West, S.; Lopez, V.; Kornhaber, R. Promoting emotional intelligence and resilience in undergraduate nursing students: An integrative review. Nurse Educ. Today 2018, 68, 112–120. [Google Scholar] [CrossRef]
- Chow, K.M.; Tang, W.K.F.; Chan, W.H.C.; Sit, W.H.J.; Choi, K.C.; Chan, S. Resilience and well-being of university nursing students in Hong Kong: A cross-sectional study. BMC Med. Educ. 2018, 18, 13. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.; Liu, Y.; Li, G.; Fang, Y.; Kang, X.; Li, P. Resilience moderates the relationship between emotional intelligence and clinical communication ability among Chinese practice nursing students: A structural equation model analysis. Nurse Educ. Today 2016, 46, 64–68. [Google Scholar] [CrossRef]
- Slatyer, S.; Cramer, J.; Pugh, J.D.; Twigg, D.E. Barriers and enablers to retention of Aboriginal diploma of nursing students in Western Australia: An exploratory descriptive study. Nurse Educ. Today 2016, 42, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ai, A.L.; Tice, T.N.; Peterson, C.; Huang, B. Prayers, spiritual support, and positive attitudes in coping with the September 11 national crisis. J. Personal. 2005, 73, 763–791. [Google Scholar] [CrossRef] [PubMed]
- Smilkstein, G.; Ashworth, C.; Montano, D. Validity and reliability of the family APGAR as a test of family function. J. Fam. Pract. 1982, 15, 303–311. [Google Scholar] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Sampson, M.; Melnyk, B.M.; Hoying, J. Intervention effects of the MINDBODYSTRONG cognitive behavioral skills building program on newly licensed registered nurses’ mental health, healthy lifestyle behaviors, and job satisfaction. J. Nurs. Adm. 2019, 49, 487–495. [Google Scholar] [CrossRef]
- Sampson, M.; Melnyk, B.M.; Hoying, J. The MINDBODYSTRONG intervention for new nurse residents: 6-month effects on mental health outcomes, healthy lifestyle behaviors, and job satisfaction. Worldviews Evid. Based Nurs. 2020, 17, 16–23. [Google Scholar] [CrossRef]
- Huang, L.; Xu, F.; Liu, H. Emotional responses and coping strategies of nurses and nursing college students during COVID-19 outbreak. MedRxiv 2020. [Google Scholar] [CrossRef]
- Boardman, L. Building resilience in nursing students: Implementing techniques to foster success. Int. J. Emerg. Ment. Health Hum. Resil. 2016, 18, 1–5. [Google Scholar]
- Rios-Risquez, M.I.; Garcia-Izquierdo, M.; Sabuco-Tebar, E.L.; Carrillo-Garcia, C.; Martinez-Roche, M.E. An exploratory study of the relationship between resilience, academic burnout and psychological health in nursing students. Contemp. Nurse 2016, 52, 430–439. [Google Scholar] [CrossRef]
- Onan, N.; Karaca, S.; Unsal Barlas, G. Evaluation of a stress coping course for psychological resilience among a group of university nursing students. Perspect. Psychiatr. Care 2019, 55, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Sauer, K.S.; Jungmann, S.M.; Witthöft, M. Emotional and behavioral consequences of the COVID-19 pandemic: The role of health anxiety, intolerance of uncertainty, and distress (in)tolerance. Int. J. Environ. Res. Public Health 2020, 17, 7241. [Google Scholar] [CrossRef] [PubMed]
- Lanz, J.J. Evidence-based resilience interventions for nursing students: A randomized controlled pilot trial. Int. J. Appl. Posit. Psychol. 2020, 5, 217–230. [Google Scholar] [CrossRef]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann. Acad. Med. Singap. 2020, 49, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.; Shand, F.; Lal, T.J.; Mott, B.; Bryant, R.A.; Harvey, S.B. Resilience@Work mindfulness program: Results from a cluster randomized controlled trial with first responders. J. Med. Internet Res. 2019, 21, e12894. [Google Scholar] [CrossRef]


{kind=link}
| High Stress (r) | Moderate-to-Severe Anxiety (r) | Moderate-to-Severe Depression (r) | |
|---|---|---|---|
| Age | −0.07 | −0.14 | −0.09 |
| Female | 0.09 | 0.01 | 0.03 |
| Pre-licensure undergraduate students | 0.11 | 0.02 | 0.06 |
| Quarantine or self-isolation experience | 0.10 | 0.06 | −0.03 |
| High resilience a | −0.20 * | −0.22 ** | −0.23 ** |
| High family functioning b | −0.22 ** | −0.24 ** | −0.28 *** |
| High spiritual support c | −0.08 | −0.21 * | −0.24 ** |
| OR | 95%CI | p-Value | |
|---|---|---|---|
| High stress | |||
| High resilience a | 0.46 | 0.22–0.98 | 0.045 |
| High family functioning b | 0.41 | 0.20–0.86 | 0.018 |
| Moderate-to-severe anxiety | |||
| High resilience a | 0.47 | 0.25–0.90 | 0.022 |
| High family functioning b | 0.41 | 0.21–0.80 | 0.009 |
| Moderate-to-severe depression | |||
| High resilience a | 0.50 | 0.26–0.95 | 0.036 |
| High family functioning b | 0.41 | 0.20–0.81 | 0.011 |
| High spiritual support c | 0.48 | 0.24–0.95 | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.C.; Sloan, C.; Montejano, A.; Quiban, C. Impacts of Coping Mechanisms on Nursing Students’ Mental Health during COVID-19 Lockdown: A Cross-Sectional Survey. Nurs. Rep. 2021, 11, 36-44. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11010004
Kim SC, Sloan C, Montejano A, Quiban C. Impacts of Coping Mechanisms on Nursing Students’ Mental Health during COVID-19 Lockdown: A Cross-Sectional Survey. Nursing Reports. 2021; 11(1):36-44. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11010004
Chicago/Turabian StyleKim, Son Chae, Christine Sloan, Anna Montejano, and Carlota Quiban. 2021. "Impacts of Coping Mechanisms on Nursing Students’ Mental Health during COVID-19 Lockdown: A Cross-Sectional Survey" Nursing Reports 11, no. 1: 36-44. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11010004