
A Scoping Review to Identify Barriers and Enabling Factors for Nurse–Patient Discussions on Sexuality and Sexual Health


Abstract
:1. Introduction
AIM
2. Materials and Methods
2.1. Consulting with Stakeholders
2.2. Ethical Consideration
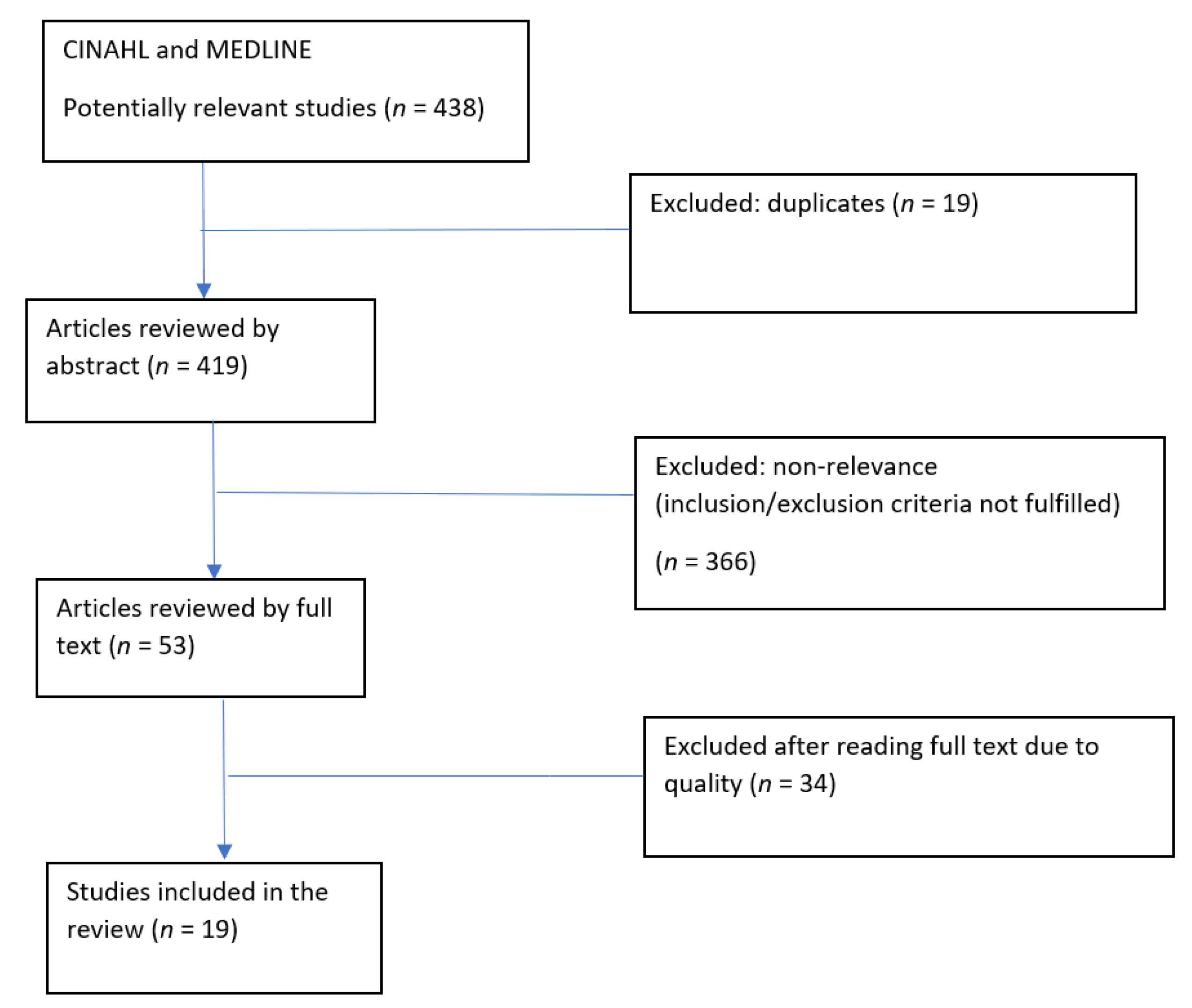
3. Results
3.1. Enabling Factors
3.1.1. Professional Approach, including Core Care Values
3.1.2. Availability of Resources
3.2. Barriers for Discussions on Sexuality and Sexual Health
3.2.1. Beliefs and Attitudes Related to Age, Gender, and Sexual Identity
3.2.2. Fear and Individual Convictions
3.2.3. Work-Related Factors
4. Discussion
4.1. Applying Professionalism through Core Care Values and Relevant Resources
4.2. The Need for a Norm-Critical Approach in Nursing Education and Practice
5. Conclusions
Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Education and Treatment in Human Sexuality: The Training of Health Professionals; Report of a WHO Meeting; World Health Organisation: Geneva, Switzerland, 1975; pp. 5–33. [Google Scholar]
- World Health Organisation. Defining Sexual Health Report of a Technical Consultation on Sexual Health 28–31 January 2002; World Health Organisation: Geneva, Switzerland, 2002. [Google Scholar]
- World Health Organisation. Sexual and Reproductive Health Defining Sexual Health. 2006. Available online: https://www.who.int/reproductivehealth/topics/sexual_health/sh_definitions/en/ (accessed on 28 November 2019).
- World Health Organization. Sexual and Reproductive Health: Defining Sexual Health. 2014. Available online: https://www.who.int/reproductivehealth/publications/sexual_health/defining_sexual_health.pdf (accessed on 28 November 2019).
- Evans, D.T. Sexual Health Matters! Learning for Life: Mapping Client Need and Professional Sexual Health Education for Nurses in England; University of Greenwich: London, UK, 2011. [Google Scholar]
- Kettunen, T.; Poskiparta, M.; Gerlander, M. Nurse–patient power relationship: Preliminary evidence of patients’ power messages. Patient Educ. Couns 2002, 47, 101–113. [Google Scholar] [CrossRef]
- Van Ryn, M.V. Developing effective helping relationships in health education practice. Health Educ. Behav. 1997, 24, 683–702. [Google Scholar] [CrossRef] [PubMed]
- Burgoon, M.; Parrot, R.; Burgoon, J.K.; Birk, T.; Pfau, M.; Coker, R. Primary care physicians’ selection of verbal compliance-gaining strategies. Health Commun. 1990, 2, 13–27. [Google Scholar] [CrossRef]
- Holmgren, J. Global nursing: Educating future nurses for tomorrow’s nursing care needs. Nordic J. Nurs. 2017, 37, 172–174. [Google Scholar] [CrossRef] [Green Version]
- Gledhill, S.; Schweitzer, R.D. Sexual desire, erectile dysfunction and the biomedicalization of sex in older heterosexual men. J. Adv. Nurs. 2014, 70, 894–903. [Google Scholar] [CrossRef]
- Hayter, M.; Harrison, C.J.; Jo, C.N. Gendered attitudes towards sexual relationships among adolescents attending nurse led sexual health clinics in England: A qualitative study. J. Clin. Nurs. 2008, 17, 2963–2971. [Google Scholar] [CrossRef] [PubMed]
- Wongpanarak, N.; Fongkaew, W.; Sethabouppha, H.; Marcus, M.T.; Rujkorakarn, D. Early Adolescent Thais’ Perceptions of Sexual Identity. J. Nurs. Res. 2010, 14, 122–136. [Google Scholar]
- Farrag, S.; Hayter, M. A qualitative study of Egyptian school nurses’ attitudes and experiences toward sex and relationship education. J. Sch. Nurs. 2014, 30, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Sweden. Hälsan och hälsans bestämningsfaktorer för transpersoner: En rapport om hälsoläget bland transpersoner i Sverige. 2015. Available online: https://www.folkhalsomyndigheten.se/contentassets/a55cb89cab14498caf47f2798e8da7af/halsan-halsans-bestamningsfaktorer-transpersoner-15038-webb.pdf (accessed on 11 December 2020).
- Public Health Agency of Sweden. Utvecklingen av hälsan och hälsans bestämningsfaktorer bland homo- och bisexuella personer: Resultat från nationella folkhälsoenkäten Hälsa på lika villkor. 2014. Available online: https://www.folkhalsomyndigheten.se/globalassets/nyheter-press/dokument-nyheter/2014/utv-halsan-bestamningsfaktorer-homo-bi-fina-2014.pdf (accessed on 9 June 2020).
- Julien, J.O.; Thom, B.; Kline, N.E. Identification of barriers to sexual health assessment in oncology nursing practice. Oncol. Nurs. Forum 2010, 37, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Magnan, M.; Reynolds, K.E.; Galvin, E.A.J.M.N. Barriers to addressing patient sexuality in nursing practice. MedSurg Nurs. 2005, 14, 282. [Google Scholar]
- World Health Organisation. Sexual Health, Human Rights and the Law; World Health Organization: Geneva, Switzerland, 2015; 49p. [Google Scholar]
- Kawachi, I.; Subramanian, S.; Almeida-Filho, N.; Health, C. A glossary for health inequalities. J. Epidemiol. Community Health 2002, 56, 647–652. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. 10 Facts on Health Inequities and Their Causes. 2017. Available online: https://www.who.int/features/factfiles/health_inequities/en/#:~:text=Health%20inequities%20are%20differences%20in,right%20mix%20of%20government%20policies (accessed on 4 November 2020).
- Whitehead, M. The concepts and principles of equity and health. Health Promot. Int. 1991, 6, 217–228. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Haboubi, N.; Lincoln, N. Views of health professionals on discussing sexual issues with patients. Disabil. Rehabil. 2003, 25, 291–296. [Google Scholar] [CrossRef]
- Dyer, K.; das Nair, R. Why don’t healthcare professionals talk about sex? A systematic review of recent qualitative studies conducted in the United Kingdom. J. Sex. Med. 2013, 10, 2658–2670. [Google Scholar] [CrossRef]
- Ali, R.M.A.; Abed, M.A.; Khalil, A.A.; Al-Kloub, M.I.; Ashour, A.F.; Alnsour, I.A. A survey on sexual counseling for patients with cardiac disease among nurses in Jordan. J. Cardiovasc. Nurs. 2018, 33, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Daudt, H.M.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Fulop, N. Studying the Organisation and Delivery of Health Services: Research Methods; Psychology Press: London, UK, 2001. [Google Scholar]
- Karolinska Institutet Library. Subject Headings and Free Text. 2018. Available online: https://kib.ki.se/en/search-evaluate/searching-information/subject-headings-and-free-text. (accessed on 29 November 2019).
- Swedish Agency for Health Technology Assessment and Assessment of Social Services. The Process of Producing a Systematic Review. 2016. Available online: https://www.sbu.se/en/method/ (accessed on 29 November 2019).
- Yodchai, K.; Hutchinson, A.M.; Oumtanee, A. Nephrology nurses’ perceptions of discussing sexual health issues with patients who have end-stage kidney disease. J. Ren. Care 2018, 44, 229–237. [Google Scholar] [CrossRef]
- Baker-Green, R. Nurses experiences discussing sexuality with urinary catheter patients. Int. J. Urol. Nurs. 2017, 11, 6–12. [Google Scholar] [CrossRef]
- Fitch, M.I.; Beaudoin, G.; Johnson, B. Challenges having conversations about sexuality in ambulatory settings: Part II—Health care provider perspectives. Can. Oncol. Nurs. J./Rev. Can. Soins Infirm. Oncol. 2013, 23, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, T.; Lesman-Leegte, I.; Couperus, M.F.; Sanderman, R.; Jaarsma, T. What keeps nurses from the sexual counseling of patients with heart failure? Heart Lung 2012, 41, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klaeson, K.; Hovlin, L.; Guvå, H.; Kjellsdotter, A. Sexual health in primary health care–a qualitative study of nurses’ experiences. J. Clin. Nurs. 2017, 26, 1545–1554. [Google Scholar] [CrossRef] [Green Version]
- Saunamäki, N.; Engström, M. Registered nurses’ reflections on discussing sexuality with patients: Responsibilities, doubts and fears. J. Clin. Nurs. 2014, 23, 531–540. [Google Scholar] [CrossRef]
- Zeng, Y.C.; Liu, X.; Loke, A.Y. Addressing sexuality issues of women with gynaecological cancer: Chinese nurses’ attitudes and practice. J. Adv. Nurs. 2012, 68, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Reese, J.B.; Beach, M.C.; Smith, K.C.; Bantug, E.T.; Casale, K.E.; Porter, L.S.; Bober, S.L.; Tulsky, J.A.; Daly, M.B.; Lepore, S.J. Effective patient-provider communication about sexual concerns in breast cancer: A qualitative study. Supportive Care Cancer 2017, 25, 3199–3207. [Google Scholar] [CrossRef] [PubMed]
- Martel, R.; Crawford, R.; Riden, H. ‘By the way…. how’s your sex life?’—A descriptive study reporting primary health care registered nurses engagement with youth about sexual health. J. Prim. Health Care 2017, 9, 22–28. [Google Scholar] [CrossRef]
- Quinn, C.; Platania-Phung, C.; Bale, C.; Happell, B.; Hughes, E. Understanding the current sexual health service provision for mental health consumers by nurses in mental health settings: Findings from a survey in Australia and England. Int. J. Ment. Health Nurs. 2018, 27, 1522–1534. [Google Scholar] [CrossRef]
- Vermeer, W.M.; Bakker, R.M.; Stiggelbout, A.M.; Creutzberg, C.L.; Kenter, G.G.; Ter Kuile, M.M. Psychosexual support for gynecological cancer survivors: Professionals’ current practices and need for assistance. Supportive Care Cancer 2015, 23, 831–839. [Google Scholar] [CrossRef]
- Saunamäki, N.; Andersson, M.; Engström, M. Discussing sexuality with patients: Nurses’ attitudes and beliefs. J. Adv. Nurs. 2010, 66, 1308–1316. [Google Scholar] [CrossRef]
- Van Ek, G.F.; Gawi, A.; Nicolai, M.P.; Krouwel, E.M.; Den Oudsten, B.L.; Den Ouden, M.E.; Schaapherder, A.F.; Putter, H.; Pelger, R.C.M.; Elzevier, H.W. Sexual care for patients receiving dialysis: A cross-sectional study identifying the role of nurses working in the dialysis department. J. Adv. Nurs. 2018, 74, 128–136. [Google Scholar] [CrossRef]
- Evcili, F.; Demirel, G. Patient’s Sexual Health and Nursing: A Neglected Area. Int. J. Caring Sci. 2018, 11, 1282–1288. [Google Scholar]
- Ussher, J.M.; Perz, J.; Gilbert, E.; Wong, W.T.; Mason, C.; Hobbs, K.; Kirsten, L. Talking about sex after cancer: A discourse analytic study of health care professional accounts of sexual communication with patients. Psychol. Health 2013, 28, 1370–1390. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.-L.; Pu, J.; Liu, L.-H.; Du, X.-B.; Wang, J.; Li, J.-Y.; Yao, W.-X.; Zhu, X.-Q.; Zhang, R.; Zhao, Y.; et al. Cancer department nurses’ attitudes and practices in response to the sexual issues of pelvic radiation patients: A survey in Sichuan, China. Contemp. Nurse 2013, 43, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Akinci, A.C. The comfort levels of nurses during clinical experiences which include sexual topics. Sex. Disabil. 2011, 29, 239. [Google Scholar] [CrossRef]
- Maree, J.; Fitch, M.I.J. Holding conversations with cancer patients about sexuality: Perspectives from Canadian and African healthcare professionals. Can. Oncol. Nurs. 2019, 29, 64. [Google Scholar]
- Arikan, F.; Meydanlioglu, A.; Ozcan, K.; Ozer, Z.C.J.S. Disability. Attitudes and beliefs of nurses regarding discussion of sexual concerns of patients during hospitalization. Sex. Disabil. 2015, 33, 327–337. [Google Scholar] [CrossRef]
- The Swedish Society of Nursing. Värdegrund för Omvårdnad (Basic Principles for Nursing Care). 2016. Available online: https://www.swenurse.se/globalassets/01-svensk-sjukskoterskeforening/publikationer-svensk-sjukskoterskeforening/etik-publikationer/vardegrund.for.omvardnad_reviderad_2016.pdf (accessed on 27 April 2016).
- Rutherford, M.M. GNE. Nursing 2014, 32, 283. [Google Scholar]
- Stewart, K.; O’Reilly, P. Exploring the attitudes, knowledge and beliefs of nurses and midwives of the healthcare needs of the LGBTQ population: An integrative review. Nurse Educ. Today 2017, 53, 67–77. [Google Scholar] [CrossRef]
- Kellett, P.; Fitton, C. Supporting transvisibility and gender diversity in nursing practice and education: Embracing cultural safety. Nurs. Enq. 2017, 24, e12146. [Google Scholar] [CrossRef]
- Tengelin, E.; Dahlborg, E.; Berndtsson, I.; Bülow, P. From political correctness to reflexivity: A norm-critical perspective on nursing education. Nurs. Inq. 2020, 27, e12344. [Google Scholar] [CrossRef] [PubMed]
- Olsson, C.; Berglund, A.-L.; Larsson, M.; Athlin, E. Patient’s sexuality–A neglected area of cancer nursing? Eur. J. Oncol. Nurs. 2012, 16, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Manzer, D.; O’Sullivan, L.F.; Doucet, S. Myths, misunderstandings, and missing information: Experiences of nurse practitioners providing primary care to lesbian, gay, bisexual, and transgender patients. Can. J. Hum. Sex. 2018, 27, 157–170. [Google Scholar] [CrossRef]
- Crombie, I.K.; Irvine, L.; Elliott, L.; Wallace, H.; World Health Organization. Closing the Health Inequalities Gap: An International Perspective; WHO Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- World Health Organisation. Reducing Inequalities in Health and Health Care—WHO/Europe Brussels, Belgium: World Health Organization European Region. 2015. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/272660/EuroHealth_V21n1_WEB_060315.pdf?ua=1 (accessed on 4 November 2020).
- Mead, N.; Bower, P. Patient-centredness: A conceptual framework and review of the empirical literature. Soc. Sci. Med. 2000, 51, 1087–1110. [Google Scholar] [CrossRef]
- Reynolds, A. Patient-centered Care. Radiol. Technol. 2009, 81, 133–147. [Google Scholar] [PubMed]
- Constand, M.K.; MacDermid, J.C.; Dal Bello-Haas, V.; Law, M. Scoping review of patient-centered care approaches in healthcare. BMC Health Serv. Res. 2014, 14, 271. [Google Scholar] [CrossRef] [Green Version]
- Sundbeck, M. Sexuell hälsa i vården: En metodbok för sjuksköterskor; Studentlitteratur: Lund, Sweden, 2013. [Google Scholar]
- Poorchangizi, B.; Borhani, F.; Abbaszadeh, A.; Mirzaee, M.; Farokhzadian, J. The importance of professional values from nursing students’ perspective. BMC Nurs. 2019, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Martinsson, L.; Reimers, E. Norm-Struggles: Sexualities in Contentions; Cambridge Scholars Publishing: Cambridge, UK, 2010. [Google Scholar]
- Collins, P.H. Gender, black feminism, and black political economy. Ann. Am. Acad. Political Soc. Sci. 2000, 568, 41–53. [Google Scholar] [CrossRef]
- Tengelin, E.; Dahlborg-Lyckhage, E. Discourses with potential to disrupt traditional nursing education: Nursing teachers’ talk about norm-critical competence. Nurs. Inq. 2017, 24, e12166. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.; Gordon, J.; MacLeod, A. Reflection and reflective practice in health professions education: A systematic review. Adv. Health Sci. Educ. 2009, 14, 595. [Google Scholar] [CrossRef] [PubMed]
- Norrie, C.; Hammond, J.; D’Avray, L.; Collington, V.; Fook, J. Doing it differently? A review of literature on teaching reflective practice across health and social care professions. Reflective Pract. 2012, 13, 565–578. [Google Scholar] [CrossRef]


{kind=link}
| Search | Date | Database | Search Terms | Number of Hits | Number of Abstracts Read | Full Text Read | No. of Eligible Articles |
|---|---|---|---|---|---|---|---|
| #1 | 28 January 2019 | CINAHL complete Medline | Nurs* AND “discussing sexuality” | 18 | 18 | 15 | 9 |
| #2 | 28 January 2019 | CINAHL complete Medline | Nurs* AND (“Talking to patients” OR Dialog* OR Address* OR Approach* OR Discuss* OR Communicat* OR “Sex talk”) AND (Sexual* OR “Sexual health”) AND (Barrier* OR Problem* OR Difficult* OR Challenge*) | 315 | 314 (313) 1 duplicates | 16 (15) 1duplicate | 4 (3) 1 duplicate |
| #3 | 29 January 2019 | CINAHL complete Medline | Nurs* AND (MH “sexual health”) OR (MH “Sexuality”) OR (MH “Attitude to Sexuality”) AND (MH “Communication”) OR (MH “Communication Barriers”) | 64 | 64 (49) 15 duplicates | 27 (12) 15 duplicates | 12 (3) 9 duplicates |
| #4 | 30 January 2019 | CINAHL complete Medline | Nurs* OR “Healthcare providers” AND Sex* AND “Talking to” | 37 | 37 | 8 | 1 |
| #5 | 4 February 2019 | CINAHL complete Medline | Nurs* AND “Sexual topics” OR “Patient’s sexual health” | 4 | 4 | 3 | 2 |
| Search | Eligible Articles (Total 19) * = Duplicates (Total 10) |
|---|---|
| #1 | 1. Arikan, F., Meydanlioglu, A., Ozcan, K., and Canli Ozer, Z. (2015). 2. Baker, G. R. (2017). 3. Ek, G. F., Gawi, A., Nicolai, M. P. J., Krouwel, E. M., Den Oudsten, B. L., Den Ouden, M. E. M., … Elzevier, H. W. (2018). 4. Hoekstra, T., Lesman-Leegte, I., Couperus, M. F., Sanderman, R., and Jaarsma, T. (2012). 5. Li-Li Huang, Jing Pu, Li-Hua Liu, Xiao-Bo Du, Jin Wang, Jun-Ying Li, … Mei He. (2013). 6. Saunamäki N, Andersson M, and Engström M. (2010). 7. Saunamäki, N., and Engström, M. (2014). 8. Vermeer, W. M., Bakker, R. M., Stiggelbout, A. M., Creutzberg, C. L., Kenter, G. G., and Ter Kuile, M. M. (2015). 9. Yodchai, K., Hutchinson, A. M., and Oumtanee, A. (2018). |
| #2 | 1. Fitch, M. I., Beaudoin, G., and Johnson, B. (2013). 2. Maree, J., and Fitch, M. I. (2019). 3. Ussher, J. M., Perz, J., Gilbert, E., Wong, W. K. T., Mason, C., Hobbs, K., and Kirsten, L. (2013). 4. *Saunamäki N, Andersson M, and Engström M. (2010). |
| #3 | 1. Klaeson, K., Hovlin, L., Guvå, H., and Kjellsdotter, A. (2017). 2. Reese, J., Beach, M., Smith, K., Bantug, E., Casale, K., Porter, L., … Lepore, S. J. (2017). 3. Zeng, Y. C., Liu, X., and Loke, A. Y. (2012). 4. *Arikan, F., Meydanlioglu, A., Ozcan, K., and Canli Ozer, Z. (2015). 5. *Baker, G. R. (2017). 6. *Fitch, M. I., Beaudoin, G., and Johnson, B. (2013). 7. *Hoekstra, T., Lesman-Leegte, I., Couperus, M. F., Sanderman, R., and Jaarsma, T. (2012). 8. *Li-Li Huang, Jing Pu, Li-Hua Liu, Xiao-Bo Du, Jin Wang, Jun-Ying Li, … Mei He. (2013). 9. *Ussher, J. M., Perz, J., Gilbert, E., Wong, W. K. T., Mason, C., Hobbs, K., and Kirsten, L. (2013). 10. *Saunamäki N, Andersson M, and Engström M. (2010). 11. *Vermeer, W. M., Bakker, R. M., Stiggelbout, A. M., Creutzberg, C. L., Kenter, G. G., and Ter Kuile, M. M. (2015). 12. *Yodchai, K., Hutchinson, A. M., and Oumtanee, A. (2018). |
| #4 | 1. Martel, R., Crawford, R., and Riden, H. (2017). 2. Quinn, C., Platania, P. C., Bale, C., Happell, B., and Hughes, E. (2018). |
| #5 | 1. Akinci, A. (2011). 2. Evcili, F., and Demirel, G. (2018). |
| Author (Year) | Study Location | Aim | Study Design | Participants |
|---|---|---|---|---|
| Akinci (2011) | Turkey | To determine nurses’ comfort levels and factors affecting their comfort levels during clinical experiences, which include sexual topics. | Cross-sectional | 141 nurses working at the medical and surgical units at two state hospitals in Hatay, Turkey. |
| Arikan et al. (2014) | Turkey | To determine the attitude and beliefs of nurses regarding sexuality and to establish the obstacles preventing them from offering counselling on sexuality. | Cross-sectional | 162 nurses working in a University Hospital i.e., 88 from internal medicine, 58 from surgery, 5 from psychiatry, and 11 from obstetrics. |
| Baker-Green (2017) | UK | To explore nurses’ experiences of communicating with patients with an indwelling urinary catheter about sexual quality of life. | Qualitative semi-structured interviews | Nine registered nurses employed by the National Health Service and working in the district nursing service |
| Van Ek et al. (2018). | The Netherlands | To explore to which extent Dutch nurses working with patients receiving dialysis discuss sexual dysfunction and to identify possible barriers restraining nurses from discussing sexual dysfunction. | Cross-sectional | 551 nurses |
| Evcili and Demirel (2018) | Turkey | To define the views of the nurses about the evaluation of the sexual health of the patients and the obstacles they experienced during the evaluation of sexual health. | Cross-sectional | 188 nurses |
| Fitch, Beaudoin, and Johnson (2013) | Canada | To understand healthcare providers’ perspectives of the barriers to having conversations about sexuality in daily ambulatory cancer care and how these might be overcome. | In-depth semi-structured qualitative interview | 34 cancer care professionals (nurses, physicians, social workers, and radiation therapists) |
| Hoekstra et al. (2012) | The Netherlands | To examine the current practice of discussing sexual health by heart failure (HF) nurses, and to explore which barriers prevent nurses from discussing sexuality. | Cross-sectional | 146 nurses working with heart failure patients |
| Klaeson et al. (2017) | Sweden | To illuminate nurses’ experiences and opportunities to discuss sexual health with patients in primary healthcare. | Semi-structured qualitative interviews | 9 primary healthcare nurses |
| Huan et al. (2013) | China | To investigate cancer department nurses’ attitudes and practices in response to pelvic radiation patients’ sexual issues in Sichuan, China. | Cross-sectional | 128 nurses cancer care nurses |
| Martel, Crawford and Riden (2017) | New Zealand | To identify what facilitates primary healthcare nurses to discuss sexual health with youths. | Mixed methods | 23 primary healthcare nurses |
| Maree and Fitch (2019) | Canada and Zimbabwe | To gain an increased understanding about the dialogue between cancer care professionals and cancer patients regarding the topic of sexuality. | Qualitative interviews in Canada and focus group discussions in Zimbabwe. | 34 healthcare professionals in Canada and 27 Zimbabwean nurses engaged in a focus group discussion |
| Saunamäki, Andersson and Engström (2010) | Sweden | To describe registered nurses’ attitudes and beliefs toward discussing sexuality with patients. | Cross-sectional | 88 registered nurses |
| Saunamaki and Engström (2014) | Sweden | To describe how RNs reflect on discussing sexuality with patients. | Qualitative interviews | 10 registered nurses |
| Ussher et al. (2013) | Australia | To examine healthcare providers’ constructions of sexuality post-cancer, the subject positions adopted in relation to sexual communication, and the ways in which discourses and subject positions shape information provision and communication about sexuality. | Semi-structured qualitative interviews | 38 healthcare providers (9 doctors, 11 nurses, 10 psychologists, and 8 social workers) |
| Quinn et al. (2018) | Australia and England | To gather information about how nurses working in mental health settings respond to sexual health issues within their routine practice: what sexual health issues nurses address during their consultations with mental health consumers; and their view on their role on promoting sexual health for mental health consumers. | Cross-sectional | 303 nurses working in public mental health settings (Australia = 219; England = 84). |
| Zeng, Liu, and Loke (2012) | China | To describe Chinese nurses’ attitudes and beliefs with regard to discussing sexuality concerns with people with gynecological cancer, to investigate their current practice in addressing gynecological cancer patients’ sexuality concerns, and to explore the possible facilitators or barriers influencing these Chinese nurses’ practice. | Cross-sectional | 202 nurses working in gynecological units |
| Yodchai, Hutchinson and Oumtanee (2018) | Thailand | To explore nephrology nurses’ perceptions of discussing sexual health issues with patients receiving dialysis. | Semi-structured qualitative interviews | 20 nephrology nurses working in dialysis units |
| Reese et al. (2017) | USA | To characterize the experiences, needs, and intervention preferences of breast cancer survivors and healthcare providers with respect to patient–provider communication about sexual concerns in an effort to inform intervention development. | Qualitative interviews with HCPs 5 focus groups with partnered breast cancer survivors 4 interviews with unpartnered breast cancer survivors | 28 women treated for breast cancer 11 healthcare providers (breast cancer oncologists and nurses) |
| Vermeer et al. (2015) | The Netherlands | To assess healthcare providers’ (HCPs) current psychosexual support practices, barriers to provide psychosexual support, and HCP needs for training and assistance. | In-depth qualitative interviews | 30 HCPs involved in the care of women with gynecological malignancies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Åling, M.; Lindgren, A.; Löfall, H.; Okenwa-Emegwa, L. A Scoping Review to Identify Barriers and Enabling Factors for Nurse–Patient Discussions on Sexuality and Sexual Health. Nurs. Rep. 2021, 11, 253-266. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020025
Åling M, Lindgren A, Löfall H, Okenwa-Emegwa L. A Scoping Review to Identify Barriers and Enabling Factors for Nurse–Patient Discussions on Sexuality and Sexual Health. Nursing Reports. 2021; 11(2):253-266. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020025
Chicago/Turabian StyleÅling, Maria, Agnes Lindgren, Hillevi Löfall, and Leah Okenwa-Emegwa. 2021. "A Scoping Review to Identify Barriers and Enabling Factors for Nurse–Patient Discussions on Sexuality and Sexual Health" Nursing Reports 11, no. 2: 253-266. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020025