
Management of Hypnotics in Patients with Insomnia and Heart Failure during Hospitalization: A Systematic Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction and Synthesis
2.5. Quality Assessment
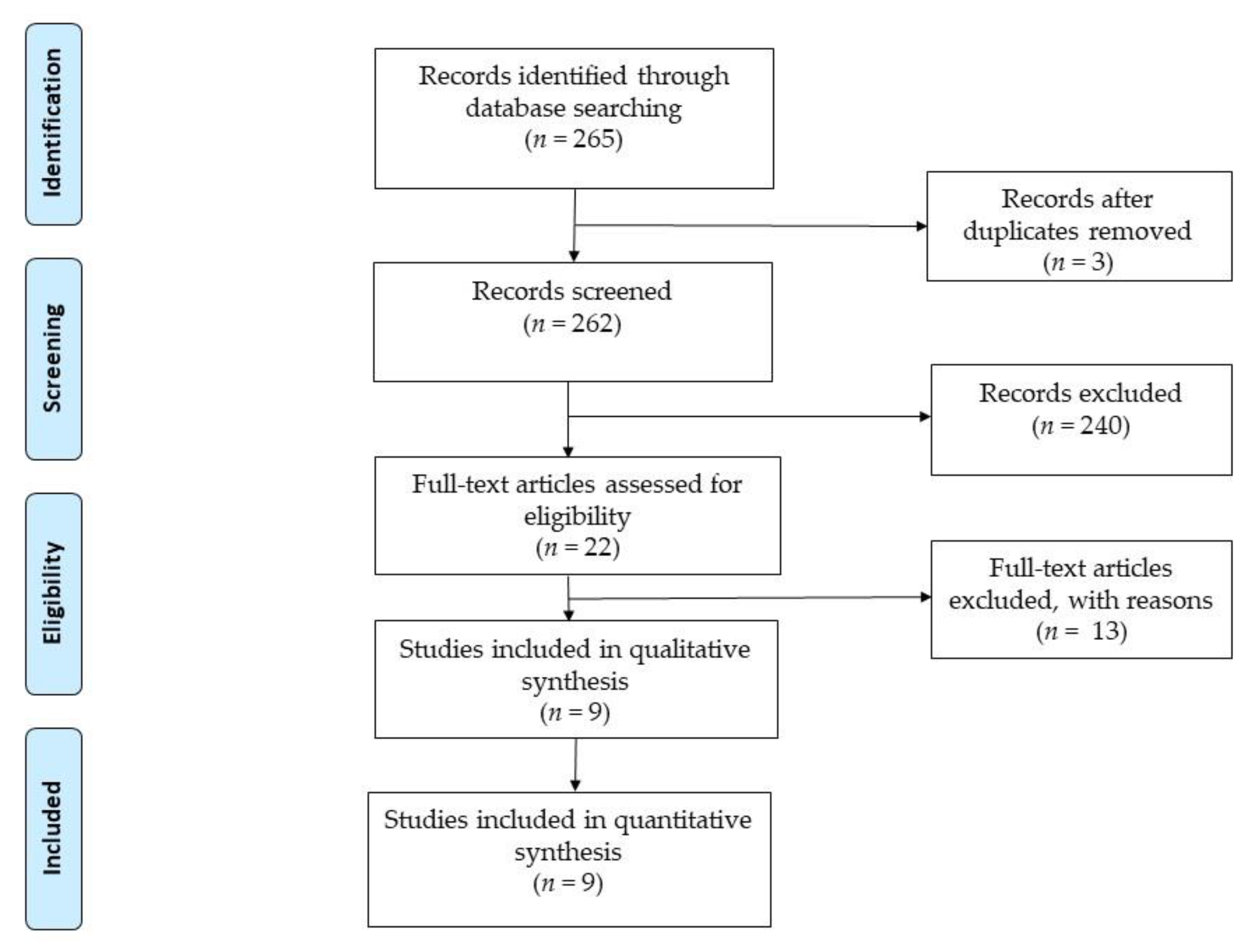
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muñiz García, J.; Crespo Leiro, M.G.; Castro Beiras, A. Epidemiología e importancia del grado de adecuación a las guías de práctica clínica. Rev. Esp. Cardiol. 2006, 6, 2–8. [Google Scholar] [CrossRef]
- Alvina dos Santos, M.; de Souza Guedes, E.; Luís Barbosa, R.; de Almeida Lopes Monteiro da Cruz, D. Dificultades para dormir por los pacientes con insuficiencia cardíaca. Rev. Latino-Am. Enferm. 2012, 20. [Google Scholar] [CrossRef]
- Cosín Aguilar, J. La insuficiencia cardiaca en el siglo XXI. Epidemiología y consecuencias económicas. Cir. Cardiov. 2011, 18, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Artalejo, F.; Banegas Banegas, J.R.; Guallar Castillón, P. Epidemiología de la Insuficiencia cardiaca. Rev. Esp. Cardiol. 2004, 57, 163–170. [Google Scholar] [CrossRef]
- Sayago-Silva, I.; García-López, F.; Segovia Cubero, J. Epidemiología de la insuficiencia cardiaca en España en los últimos 20 años. Rev. Esp. Cardiol. 2013, 66, 649–656. [Google Scholar] [CrossRef]
- Farmakis, D.; Parissis, J.; Lekakis, J.; Filippatos, G. Insuficiencia cardiaca aguda: Epidemiología, factores de riesgo y prevención. Rev. Esp. Cardiol. 2015, 68, 245–248. [Google Scholar] [CrossRef]
- Türoff, A.; Thiem, U.; Fox, H.; Spießhöfer, J.; Bitter, T.; Tamisier, R.; Punjabi, N.M.; Horstkotte, D.; Oldenburg, O. Sleep duration and quality in heart failure patients. Sleep Breath 2017, 21, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Redeker, N.S.; Jeon, S.; Andrews, L.; Cline, J.; Jacoby, D.; Mohsenin, V. Feasibility and Efficacy of a Self-Management Intervention for Insomnia in Stable Heart Failure. J. Clin Sleep Med. 2015, 11, 1109–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javadi, N.; Darvishpour, A.; Mehrdad, N.; Lakeh, N.M. Survey of Sleep Status and its Related Factors among Hospitalized Patients with Heart Failure. J. Heart Cent. 2015, 10, 9–17. Available online: http://jthc.tums.ac.ir/index.php/jthc/article/view/359 (accessed on 3 June 2020).
- Zuurbier, L.A.; Luik, A.L.; Leening, M.J.; Hofman, A.; Freak-Poli, R.; Franco, O.H.; Stricker, B.H.; Tiemeier, H. Associations of Heart Failure with Sleep Quality: The Rotterdam Study. J. Clin. Sleep Med. 2015, 11, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Lennie, T.A.; Heo, S.; Song, E.K.; Moser, D.K. Prognostic importance of sleep quality in patients with heart failure. Am. J. Crit. Care. 2016, 25, 516–525. [Google Scholar] [CrossRef]
- Moradi, M.; Mehrdad, N.; Nikpour, S.; Haghani, H.; Aalaa, M.; Sanjari, M.; Sharifi, F. Sleep quality and associated factors among patients with chronic heart failure in Iran. Med. J. Islam Repub Iran. 2014, 28, 149. [Google Scholar] [PubMed]
- Andrews, L.K.; Coviello, J.; Hurley, E.; Rose, L.; Redeker, N.S. “I’d eat a bucket of nails if you told me it would help me sleep:”Perceptions of insomnia and its treatment in patients with stable heart failure. HeartLung 2013, 42, 339–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, C.; Phelan, C.; Lauver, D.R.; Bratzke, L. Is sleep Quality related to cognition in individuals with heart failure? Heart Lung. 2015, 44, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Juárez-Vela, R.; Sarabia Cobo, C.M.; Antón Solanas, I.; Vellone, E.; Durante, A.; Gea Caballero, V.; Pérez Calvo, J.I. Investigando el autocuidado en una muestra de pacientes con insuficiencia cardiaca descompensada: Un estudio transversal. Rev. Clin. Esp. 2019, 219, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, S.; Alosco, M.L.; Spitznagel, M.B. Poor sleep quality and reduced cognitive function in persons with heart failure. Int. J. Cardiol. 2012, 156, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.J.; Lee, S.C.; Tsay, S.L.; Tung, H.H. Factors influencing heart failure patients sleep quality. J. Adv. Nurs. 2010, 66, 1730–1740. [Google Scholar] [CrossRef]
- Estrella González, I.M.; Torres Prados, M.T. La higiene del sueño en el anciano, una labor cercana a enfermería. Gerokomos 2015, 26, 123–126. [Google Scholar]
- Chen, H.-M.; Clark, A.P.; Tsai, L.-M.; Chao, Y.-F.C. Self reported sleep disturbance of patients with heart failure in Taiwan. Nurse Res. 2009, 58, 63–71. [Google Scholar] [CrossRef]
- Jorge Samitier, P.; Durante, A.; Gea Caballero, V.; Antón Solanas, I.; Fernández Rodrigo, M.T.; Juarez Vela, R. Sleep Quality in patients with heart failure in the Spanish population. Int. J. Environ. Res. Public Health 2020, 17, 7772. [Google Scholar] [CrossRef]
- Kripke, D.F. Hypnotic drug risks of mortality, infection, depression, and cancer: But lack of Benefit. F1000Research 2016, 5, 918. [Google Scholar] [CrossRef] [PubMed]
- PRISMA. Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: http://prisma-statement.org/ (accessed on 2 June 2020).
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. Available online: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/ (accessed on 21 April 2020). [CrossRef] [PubMed]
- PRISMA 2009 Checkllist. Available online: http://www.prisma-statement.org/documents/PRISMA%202009%20checklist.pdf (accessed on 5 May 2020).
- Motter, F.R.; Fritzen, J.S.; Hilmer, S.N.; Paniz, É.V.; Paniz, V.M.V. Potentially inappropriate medication in the elderly: A systematic review of validated explicit criteria. Eur. J. Clin. Pharmacol. 2018, 74, 679. [Google Scholar] [CrossRef] [PubMed]
- Ishak, W.W.; Bagot, K.; Thomas, S.; Magakian, N.; Bedwani, D.; Larson, D.; Zaky, C. Quality of life in patients suffering from insomnia. Innov. Clin. Neurosci. 2012, 9, 13–26. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC3508958/ (accessed on 6 May 2020). [PubMed]
- Buxo Pirla, M.J.; Minguell Roig, M.E.; Batalla Mesado, N.; Peregrina Fernández, E.; Pérez Miravet, S. Prevalencia e implicaciones pronósticas de los trastornos del sueño en la insuficiencia cardiaca crónica. Rev. Rol. Enferm. 2018, 41, 38–42. [Google Scholar]
- De Pablos, G.D.; Sánchez Lechuga, E. Ansiolíticos e hipnóticos en insuficiencia respiratoria y cardíaca. FMC Form. Med. Contin. Aten. Primaria. 2009, 16, 232–241. [Google Scholar] [CrossRef]
- Garrido, M.M.; Prigerson, H.G.; Penrod, J.D.; Jones, S.C.; Boockvar, K.S. Uso de benzodiacepinas y sedantes-hipnóticos entre veteranos mayores gravemente enfermos: ¿elegir sabiamente? Clin. Ther. 2014, 36, 1547–1554. [Google Scholar] [CrossRef]
- Gatti, R.; Burke, P.R.; Otuyama, L.J.; Almeida, D.R.; Tufik, S.; Poyares, D. Efectos de Zolpidem CR sobre el sueño y la ventilación nocturna en pacientes con insuficiencia cardíaca. Sueño 2016, 39, 1501–1505. [Google Scholar] [CrossRef]
- Chung, W.S.; Lai, C.Y.; Lin, C.L.; Kao, C.H. Eventos respiratorios adversos asociados con el uso de hipnóticos en pacientes con enfermedad pulmonar obstructiva crónica. Medicine 2015, 94, 27. [Google Scholar] [CrossRef]
- Hayes, D.I.; Anstead, M.; Ho, J.; Phillips, B.A. Insomnia and chronic heart failure. Heart Fail. Rev. 2008, 14, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Nichols, J.; Alper, C.; Milkin, T. Estrategias para el manejo del insomnio: Una actualización sobre las terapias farmacológicas. Formul. North. Olmsted. 2007, 42, 86. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01777122/full (accessed on 8 May 2020).


{kind=link}
| Database | Search Formula |
|---|---|
| Pubmed | (“Heart Failure”[Mesh]) AND (“Hypnotics and Sedatives”[Mesh] OR benzodiazepine) |
| Cochrane | “heart failure” AND hypnotics AND benzodiazepine |
| Scopus | “heart failure” AND hypnotics AND benzodiazepine |
| Dialnet | Insuficiencia cardiaca (insomnio OR hipnótico) |
| Total | 265 |
| EPHPP | A Selection Bias | B Study Design | C Confounders | D Blinding | D Data Collection Method | E Withdrawals and Dropouts | GLOBAL RATING |
|---|---|---|---|---|---|---|---|
| Motter | 1 | 1 | 1 | 1 | 1 | 1 | Weak |
| Garrido | 2 | 3 | 3 | 1 | 2 | 1 | Weak |
| Ishak | 1 | 1 | 1 | 1 | 1 | 1 | Weak |
| Buxó | 2 | 3 | 3 | 1 | 1 | 1 | Weak |
| De Pablos | 1 | 1 | 1 | 1 | 1 | 1 | Weak |
| Gatti | 1 | 1 | 1 | 1 | 1 | 1 | Strong |
| Chung | 1 | 2 | 1 | 3 | 1 | 1 | Moderate |
| Hayes | 1 | 1 | 1 | 1 | 1 | 1 | Weak |
| Nichols | 1 | 1 | 1 | 1 | 1 | 1 | Weak |
| Author and Year | Aim | Study Design | Sample | Studied Drug | Major Side Effect | Studied Risk | Recommendation |
|---|---|---|---|---|---|---|---|
| Nichols et al., 2007 | Insomnia management strategies description | Narrative review | Cognitive therapy Antihistamines Anti-depressants Bz* AgoBz** Melatonin agonist receptor | Anticholinergic effects in the elderly Sedation Daytime sleepiness Tolerance Dependence | Cardiovascular complications Adverse Breathing Events Delirium Abuse | Cognitive therapy AgoBz** | |
| Hayes et al., 2009 | Review of the effects of medication on SD in HF patients | Narrative review | Medications for the management of HF Medication for the management of insomina Cognitive therapy | Tolerance, dependence and rebound insomnia | Daytime sleepiness | AgoBz** have fewer adverse events than Bz* | |
| De Pablos et al., 2009 | Description of therapies used in patients >65 with respiratory and cardiac insufficiencies with insomnia and/or anxiety | Narrative review | Bz* AgoBz** Serotonergic Anxiolytics Antihistamines Clomethiazole | Sleepiness, decreased mental acuity and motor skills | Dependence and withdrawal in short lived Bz | Lorazepam, zolpidem, clomethiazole | |
| Ishak et al., 2012 | Study of the impact of insomnia on the quality of life | Systematic review | 58 | Bz* Non-pharmacological treatment | Psychiatric or physical comorbidity. Increased medication or psychosocial problem | Long-term dependence and tolerance. Deteriorating quality of life. Increased morbidity and mortality | AgoBz** to address insomnia. |
| Garrido et al., 2014 | Study of inappropriate use of Bz* in >65 | Descriptive | 222 | Psychotropics Bz* | Dependence, cognitive impairment, ataxia, syncope, falls, delirium and readmission to hospital | Use Bz* and AgoBz** | Reduce Bz* prescription Strict control of Bz* treatment in the long term |
| Chung et al., 2015 | To assess the effects of hypnotics on the risk of adverse events in patients with cardiopulmonary problems | Retrospective analytical case control study | 22.684 | Bz* and no Bz* | Pneumonia Acute Exacerbation Acute respiratory failure Cardiorespiratory arrest | High risk of adverse respiratory events | Medical management of hypnotic treatment of patients with cardiorespiratory problems |
| Gatti et al., 2016 | To assess the effects of zolpidem in patients with HF and sleep disorder | Double-blind, randomized, placebo-controlled analysis | 15 | Zolpidem | No adverse effects | Possible adverse effects | No adverse effects using Zolpidem |
| Buxo et al. 2018 | Prevalence of insomnia in HF patients studied | Descriptive | 68 | Non-pharmacological measures | |||
| Motter et al., 2018 | Study of potentially inappropriate drugs in >65 | Systematic review | 36 | Bz* | Cognitive impairment, Respiratory failure | Falls, fractures, delirium | Avoid using Bz* |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jorge-Samitier, P.; Fernández-Rodrigo, M.T.; Juárez-Vela, R.; Antón-Solanas, I.; Gea-Caballero, V. Management of Hypnotics in Patients with Insomnia and Heart Failure during Hospitalization: A Systematic Review. Nurs. Rep. 2021, 11, 373-381. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020036
Jorge-Samitier P, Fernández-Rodrigo MT, Juárez-Vela R, Antón-Solanas I, Gea-Caballero V. Management of Hypnotics in Patients with Insomnia and Heart Failure during Hospitalization: A Systematic Review. Nursing Reports. 2021; 11(2):373-381. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020036
Chicago/Turabian StyleJorge-Samitier, Pablo, María Teresa Fernández-Rodrigo, Raúl Juárez-Vela, Isabel Antón-Solanas, and Vicente Gea-Caballero. 2021. "Management of Hypnotics in Patients with Insomnia and Heart Failure during Hospitalization: A Systematic Review" Nursing Reports 11, no. 2: 373-381. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11020036