
Workplace Violence towards Healthcare Workers: An Italian Cross-Sectional Survey

 , ,
, ,  , , , and
, , , and 
Abstract
:1. Background
2. Study
2.1. Aim
2.2. Study Design and Procedures
- In the first part, there was the registry section (age, gender, education, working position, etc.).
- In the second part, the three dimensions of violence were detected: verbal, psychological, and physical.
- The third part showed the variables inherent to the health context.
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nikathil, S.; Olaussen, A.; Gocentas, R.A.; Symons, E.; Mitra, B. Review article: Workplace violence in the emergency department: A systematic review and meta-analysis. Emerg. Med. Australas. 2017, 29, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B.; Lozano, R. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Pien, L.C.; Cheng, Y.; Cheng, W.J. Internal workplace violence from colleagues is more strongly associated with poor health outcomes in nurses than violence from patients and families. J. Adv. Nurs. 2019, 75, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Chappell, D.; Di Martino, V. Violence at Work, 3rd ed.; International Labour Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Ferri, P.; Silvestri, M.; Artoni, C.; Di Lorenzo, R. Workplace violence in different settings and among various health professionals in an Italian general hospital: A cross-sectional study. Psychol. Res. Behav. Manag. 2016, 9, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashton, R.A.; Morris, L.; Smith, I. A qualitative meta-synthesis of emergency department staff experiences of violence and aggression. Int. Emerg. Nurs. 2018, 39, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hills, D.; Lam, L.; Hills, S. Workplace aggression experiences and responses of Victorian nurses, midwives and care personnel. Collegian 2018, 25, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Magnavita, N.; Heponiemi, T. Violence towards health care workers in a Public Health Care Facility in Italy: A repeated cross-sectional study. BMC Health Serv. Res. 2012, 12, 108. [Google Scholar] [CrossRef] [PubMed]
- Baby, M.; Gale, C.; Swain, N. Communication skilss in the management of patient aggression and violence in healthcare. Aggress. Violent Behaviour. 2018, 39, 67–82. [Google Scholar] [CrossRef]
- Ielapi, N.; Andreucci, M.; Bracale, U.M.; Costa, D.; Bevacqua, E.; Bitonti, A.; Mellace, A.; Buffone, G.; Candido, S.; Provenzano, M.; et al. Insomnia Prevalence among Italian Night-Shift Nurses. Nurs. Rep. 2021, 11, 530–535. [Google Scholar] [CrossRef]
- Kleinbaum, D.G.; Kupper, L.L.; Muller, K.E. Collinearity concepts. In Applied Regression Analysis and Other Multi-260 Variable Methods; Wadsworth Publishing Company: Belmont, CA, USA, 1988; pp. 209–214. [Google Scholar]
- Arimatsu, M.; Wada, K.; Yoshikawa, T.; Oda, S.; Taniguchi, H.; Aizawa, Y.; Higashi, T. An epidemiological study of work-related violence experienced by physicians who graduated from a medical school in Japan. J. Occup. Health 2008, 50, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Fang, H.; Chen, R.; Jiao, M.; Wei, L.; Zhang, G.; Li, Y.; Wang, Y.; Wang, Y.; Jiang, K.; et al. Workplace violence against healthcare professionals in a multiethnic area: A cross-sectional study in southwest China. BMJ Open 2020, 10, e037464. [Google Scholar] [CrossRef]
- Mento, C.; Silvestri, M.C.; Bruno, A.; Muscatello, M.R.A.; Cedro, C.; Pandolfo, G.; Zoccali, R.A. Workplace violence against healthcare professionals: A systematic review. Aggress. Violent Behav. 2020, 51, 101381. [Google Scholar] [CrossRef]
- Richter, D.; Berger, K. Post-traumatic stress disorder following patient assaults among staff members of mental health hospitals: A prospective longitudinal study. BMC Psychiatry 2006, 6, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, M.; Tsukano, K.; Muraoka, M.; Kaneko, F.; Okamura, H. Psychological impact of verbal abuse and violence by patients on nurses working in psychiatric departments. Psychiatry Clin. Neurosci. 2006, 60, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zafar, W.; Khan, U.R.; Siddiqui, S.A.; Jamali, S.; Razzak, J.A. Workplace Violence and Self-reported Psychological Health: Coping with Post-traumatic Stress, Mental Distress, and Burnout among Physicians Working in the Emergency Departments Compared to Other Specialties in Pakistan. J. Emerg. Med. 2016, 50, 167–177.e1. [Google Scholar] [CrossRef] [PubMed]
- Havaei, F.; Astivia, O.L.O.; MacPhee, M. The impact of workplace violence on medical-surgical nurses’ health outcome: A moderated mediation model of work environment conditions and burnout using secondary data. Int. J. Nurs. Stud. 2020, 109, 103666. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.F.; Geoffrion, S.; Juster, R.P.; Giguère, C.E.; Marchand, A.; Lupien, S.J.; Guay, S. High cortisol awakening response in the aftermath of workplace violence exposure moderates the association between acute stress disorder symptoms and PTSD symptoms. Psychoneuroendocrinology 2019, 104, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Rahim, M.A.; Magner, N.R. Confirmatory factor analysis of the styles of handling interpersonal conflict: First-order factor model and its invariance across groups. J. Appl. Psychol. 1995, 80, 122–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Overall (n = 203) | Men (n = 81) | Women (n = 122) | p |
|---|---|---|---|---|
| Age, years | 40.5 ± 10.8 | 41.4 ± 11.3 | 40.0 ± 10.5 | 0.351 |
| Education, % | ||||
| Bachelor’s Degree | 79.7 | 71.6 | 85.1 | 0.019 |
| Master’s Degree | 30.7 | 37.0 | 26.5 | 0.110 |
| School of Specialty | 16.3 | 23.5 | 11.6 | 0.025 |
| PhD | 3.0 | 3.7 | 2.5 | 0.615 |
| Freelance workers, % | 8.9 | 7.4 | 9.8 | 0.551 |
| Temporary workers, % | 9.9 | 11.1 | 9.0 | 0.624 |
| Full-time workers, % | 81.3 | 81.5 | 81.2 | 0.952 |
| Job, n (%) | ||||
| Medical doctor | 34 (16.7) | 19 (23.5) | 15 (12.3) | 0.037 |
| Nurse | 125 (61.7) | 42 (51.9) | 83 (68.0) | 0.020 |
| Patient care assistant | 10 (4.9) | 7 (8.6) | 3 (2.5) | 0.046 |
| Others | 34 (16.7) | 13 (16.0) | 21 (17.2) | 0.828 |
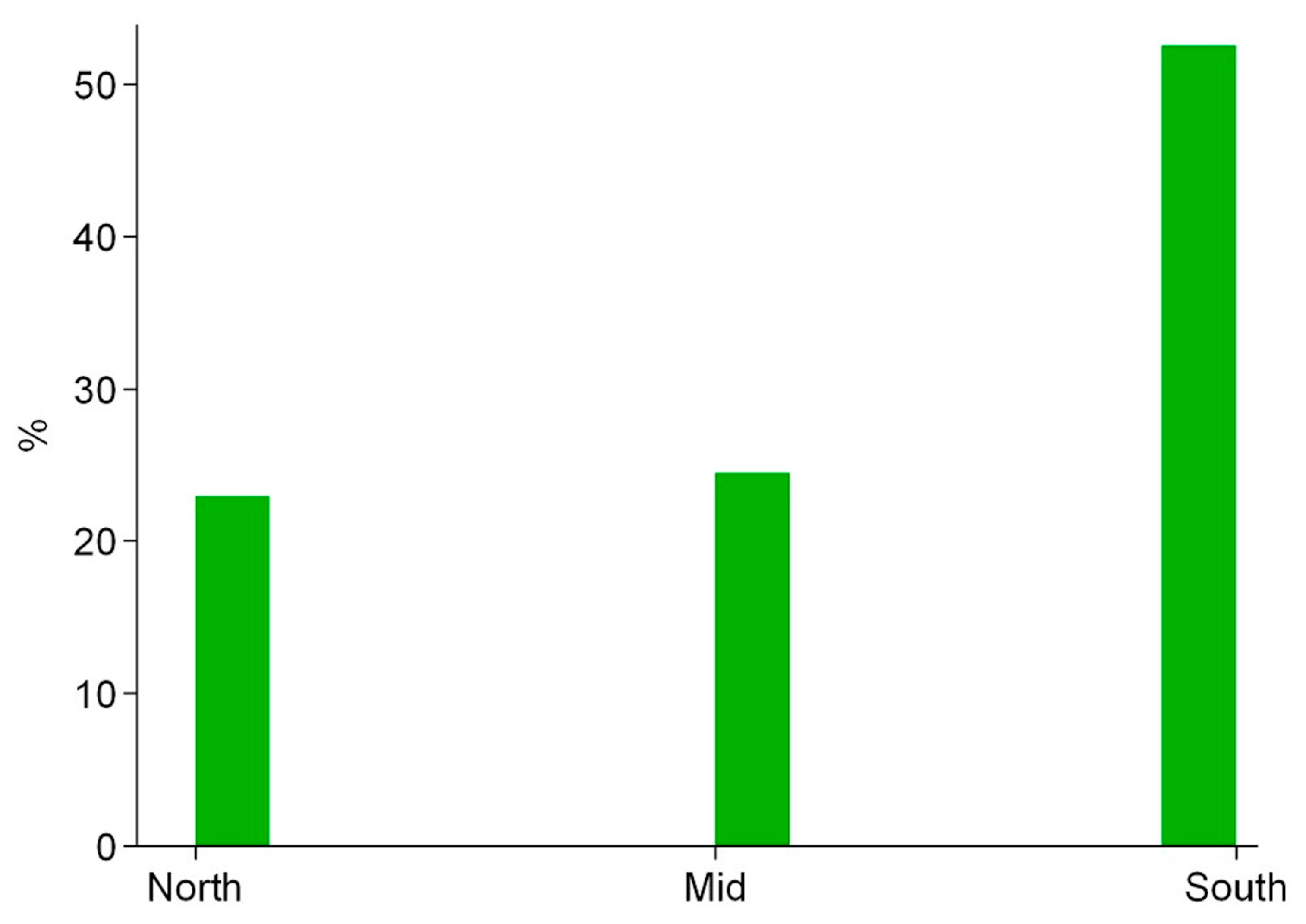
| Working Region, % | 0.792 | |||
| North Italy | 23.0 | 24.7 | 21.9 | |
| Middle Italy | 24.5 | 22.2 | 26.0 | |
| South Italy | 52.5 | 53.1 | 52.1 | |
| Time of work, years | 11 (5–21) | 10 (5–21) | 12 (5–21) | 0.445 |
| Verbal aggression, % | 88.2 | 81.5 | 92.6 | 0.016 |
| Source of verbal aggression, % | ||||
| Patient | 54.2 | 53.1 | 54.9 | 0.798 |
| Colleague | 24.6 | 30.9 | 20.5 | 0.093 |
| Relative | 55.2 | 53.1 | 56.6 | 0.626 |
| Man | 63.6 | 61.7 | 64.8 | 0.661 |
| Woman | 49.8 | 49.4 | 50.0 | 0.931 |
| Psychological aggression, % | 64.0 | 64.2 | 63.9 | 0.969 |
| Source of psychological aggression, % | ||||
| Patient | 33.5 | 39.5 | 29.5 | 0.143 |
| Colleague | 21.7 | 24.7 | 19.7 | 0.314 |
| Relative | 37.9 | 49.4 | 30.3 | 0.009 |
| Man | 57.6 | 63.0 | 54.1 | 0.211 |
| Woman | 34.5 | 34.6 | 34.4 | 0.983 |
| Physical aggression, % | 32.0 | 38.3 | 27.9 | 0.020 |
| Source of physical aggression, % | ||||
| Patient | 23.2 | 24.7 | 22.1 | 0.672 |
| Colleague | 4.9 | 8.6 | 2.5 | 0.046 |
| Relative | 9.4 | 13.6 | 6.6 | 0.033 |
| Man | 28.6 | 35.8 | 23.7 | 0.043 |
| Woman | 12.8 | 12.4 | 13.1 | 0.872 |
| Severity of aggression, % | ||||
| Very mild | 5.4 | 6.2 | 4.9 | 0.699 |
| Mild | 3.5 | 6.2 | 1.6 | 0.083 |
| Severe | 2.0 | 1.2 | 2.5 | 0.539 |
| Site of aggression, % | ||||
| Public structure | 52.7 | 46.9 | 56.6 | 0.178 |
| Private structure | 4.4 | 6.2 | 3.3 | 0.327 |
| Emergency department | 16.3 | 23.5 | 11.5 | 0.023 |
| Variables | Odds Ratio (n = 203) | 95% (CI) (n = 81) | p |
|---|---|---|---|
| Gender, female vs. male | 2.59 | 1.09–5.81 | 0.034 |
| Time of work, for 1 year | 1.05 | 1.00–1.10 | 0.046 |
| Job, nurse vs. others | 3.90 | 1.47–10.38 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ielapi, N.; Andreucci, M.; Bracale, U.M.; Costa, D.; Bevacqua, E.; Giannotta, N.; Mellace, S.; Buffone, G.; Cerabona, V.; Arturi, F.; et al. Workplace Violence towards Healthcare Workers: An Italian Cross-Sectional Survey. Nurs. Rep. 2021, 11, 758-764. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11040072
Ielapi N, Andreucci M, Bracale UM, Costa D, Bevacqua E, Giannotta N, Mellace S, Buffone G, Cerabona V, Arturi F, et al. Workplace Violence towards Healthcare Workers: An Italian Cross-Sectional Survey. Nursing Reports. 2021; 11(4):758-764. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11040072
Chicago/Turabian StyleIelapi, Nicola, Michele Andreucci, Umberto Marcello Bracale, Davide Costa, Egidio Bevacqua, Nicola Giannotta, Sabrina Mellace, Gianluca Buffone, Vito Cerabona, Franco Arturi, and et al. 2021. "Workplace Violence towards Healthcare Workers: An Italian Cross-Sectional Survey" Nursing Reports 11, no. 4: 758-764. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep11040072