
Does Less Pain Predict Better Quality of Life among Malaysian Patients with Mild–Moderate Knee Osteoarthritis?



Abstract
:1. Introduction
2. Materials and Methods
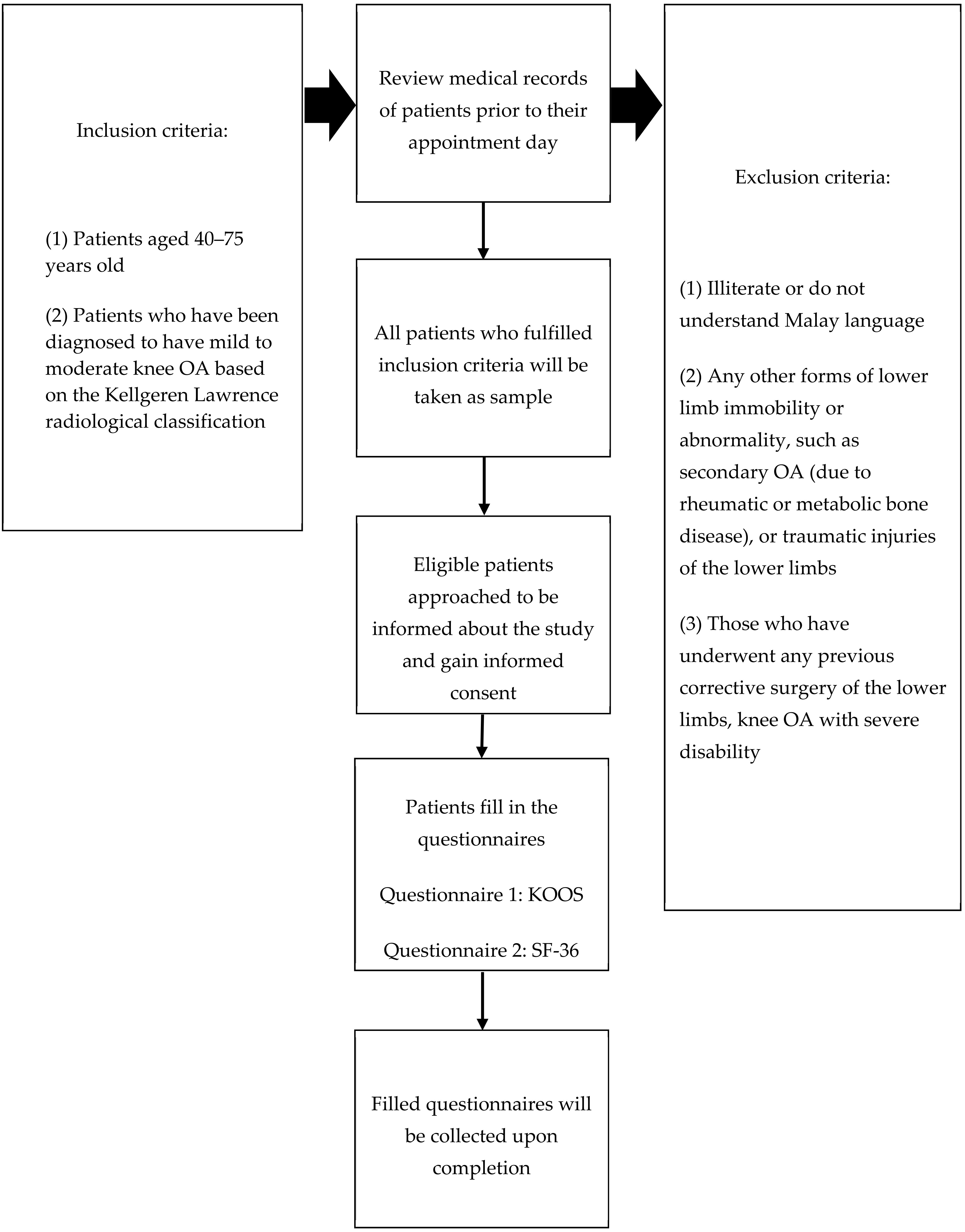
2.1. Study Design and Study Population
2.2. Study Tools
- Functional status using KOOS
- Health-related quality of life (HRQoL) using SF-36
2.3. Sample Size Determination
2.4. Patient Recruitment, Sampling Method, and Data Collection
2.5. Operational Definitions
2.6. Data Entry and Statistical Analysis
3. Results
3.1. Sociodemographic and Knee OA Profiles of Participants
3.2. Functional Status Using KOOS among Study Participants
3.3. Health-Related Quality of Life of the Participants Using SF-36
3.4. Multiple Linear Regression
3.5. Relationship between KOOS and SF-36: Physical Component Summary (PCS) and Mental Component Summary (MCS)
4. Discussion
Strengths, Limitations, and Implications for Clinical Practice and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Ministry of Health of Malaysia. Clinical Practice Guideline Osteoarthritis. J. Am. Acad. Orthop. Surg. 2013, 21, 577–579. [Google Scholar]
- Foo, C.N.; Manohar, A.; Rampal, L.; Lye, M.-S.; Mohd-Sidik, S.; Osman, Z.J. Knee Pain and Functional Disability of Knee Osteoarthritis Patients Seen at Malaysian Government Hospitals. Malays. J. Med. Health Sci. 2017, 13, 7–15. [Google Scholar]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2011, 26, 355–369. [Google Scholar] [CrossRef] [Green Version]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Sutbeyaz, S.T.; Sezer, N.; Koseoglu, B.F.; Ibrahimoglu, F.; Tekin, D. Influence of knee osteoarthritis on exercise capacity and quality of life in obese adults. Obesity 2007, 15, 2071–2076. [Google Scholar] [CrossRef]
- Kawano, M.M.; Araújo, I.L.A.; Castro, M.C.; Matos, M.A. Assessment of quality of life in patients with knee osteoarthritis. Acta Ortop. Dica. Bras. 2015, 23, 307–310. [Google Scholar] [CrossRef]
- Gossec, L.; Paternotte, S.; Maillefert, J.F.; Combescure, C.; Conaghan, P.G.; Davis, A.M.; Gunther, K.P.; Hawker, G.; Hochberg, M.; Katz, J.N.; et al. The role of pain and functional impairment in the decision to recommend total joint replacement in hip and knee osteoarthritis: An international cross-sectional study of 1909 patients. Osteoarthr. Cartil. 2014, 19, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Moriarty, D.G.; Zack, M.M.; Kobau, R. The Centers for Disease Control and Prevention’s Healthy Days Measures–Population tracking of perceived physical and mental health over time. Health Qual. Life Outcomes 2003, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Dominick, K.L.; Ahern, F.M.; Gold, C.H.; Heller, D.A. Relationship of health-related quality of life to health care utilization and mortality among older adults. Aging Clin. Exp. Res. 2002, 14, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharm. Econ. 2016, 34, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Odole, A.; Ogunlana, M.O.; Adegoke, B.O.A.; Ojonima, F.; Useh, U. Depression, pain and physical function in osteoarthritis. Niger. J. Med. Rehabil. 2015, 18, 1–16. [Google Scholar]
- Scott, D.L.; Garrood, T. Quality of life measures: Use and abuse. Baillieres. Best Pr. Res. Clin. Rheumatol. 2000, 14, 663–687. [Google Scholar] [CrossRef] [PubMed]
- Farr, I.I.J.; Miller, L.E.; Block, J.E. Quality of Life in Patients with Knee Osteoarthritis: A Commentary on Nonsurgical and Surgical Treatments. Open Orthop. J. 2013, 7, 619–623. [Google Scholar] [CrossRef] [Green Version]
- Leung, Y.Y.; Pua, Y.H.; Thumboo, J. A perspective on osteoarthritis research in Singapore. Proc. Singap. Healthc. 2013, 22, 31–39. [Google Scholar] [CrossRef]
- Hevellen, A.; Brandi, P.; Godoy, G.; Rejane, N.; Amorim, R.; Edésio, R.; da Costa, R.; Cláudia, R. Investigation of depression, anxiety and quality of life in patients with knee osteoarthritis: A comparative study. Rev. Bras. Reumatol. 2015, 55, 434–438. [Google Scholar]
- Olagbegi, O.; Adegoke, B.; Odole, A.C.; Bolarinde, S.O.; Uduonu, E.M. Pain, Walking Time, Physical Function and Health-related Quality of Life in Nigerians with Knee Osteoarthritis. Indian J. Physiother. Occup. Ther. 2016, 10, 139–144. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Berliner, J.L.; Brodke, D.J.; Chan, V.; SooHoo, N.F.; Bozic, K.J. Can Preoperative Patient-reported Outcome Measures Be Used to Predict Meaningful Improvement in Function After TKA? Clin. Orthop. Relat. Res. 2017, 475, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Bachmeier, C.J.M.; March, L.M.; Cross, M.J.; Lapsley, H.M.; Tribe, K.L.; Courtenay, B.G.; Brooks, P.M. A comparison of outcomes in osteoarthritis patients undergoing total hip and knee replacement surgery. Osteoarthr. Cartil. 2001, 9, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.; Cao, Y.L.; Zheng, Y.X.; Gao, N.Y.; Wang, X.Z.; Chen, B.; Gu, X.F.; Yuan, W.; Zhang, M.; Liu, T.; et al. Influence of pain severity on health-related quality of life in Chinese knee osteoarthritis patients. Int. J. Clin. Exp. Med. 2015, 8, 4472–4479. [Google Scholar] [PubMed]
- Alves, J.C.; Bassitt, D.P. Quality of life and functional capacity of elderly women with knee osteoarthritis. Einstein (São Paulo) 2013, 11, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.; Kim, H.A.; Seo, Y.; Song, Y.W.; Jeong, J.; Kim, D.H. The Prevalence of Knee Osteoarthritis in Elderly Community Residents in Korea. J. Korean Med. Sci. 2010, 25, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Bindawas, S.M.; Vennu, V.; al Snih, S. Differences in Health-Related Quality of Life Among Subjects with Frequent Bilateral or Unilateral Knee Pain: Data From the Osteoarthritis Initiative Study. J. Orthop. Sports Phys. Ther. 2015, 45, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Kiadaliri, A.A.; Lamm, C.J.; Verdier MG de Engström, G.; Turkiewicz, A.; Lohmander, L.S.; Englund, M. Association of knee pain and different definitions of knee osteoarthritis with health-related quality of life: A population-based cohort study in southern Sweden. Health Qual. Life Outcomes 2016, 14, 121. [Google Scholar] [CrossRef] [Green Version]
- Paradowski, P.T.; Bergman, S.; Sundén-lundius, A.; Lohmander, S.; Roos, E.M. Knee complaints vary with age and gender in the adult population. Population-based reference data for the Knee injury and Osteoarthritis Outcome Score (KOOS). BMC Musculoskelet. Disord. 2006, 7, 38. [Google Scholar] [CrossRef]
- Zakaria, Z.F.; Bakar, A.A.; Hasmoni, H.M.; Rani, F.A.; Kadir, S.A. Health-related quality of life in patients with knee osteoarthritis attending two primary care clinics in Malaysia: A cross-sectional study. Asia Pac. Fam. Med. 2009, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Zulkifli, M.; Kadir, A.; Elias, A.; Bea, K.; Sadagatullah, A. Psychometric Properties of the Malay Language Version of Knee Injury and Osteoarthritis Outcome Score (KOOS) Questionnaire among Knee Osteoarthritis Patients: A Confirmatory Factor Analysis. Malays. Orthop. J. 2017, 11, 7–14. [Google Scholar]
- Maruish, M.E. SF-36v2 Health Survey, 3rd ed.; Quality Metric, Incorporated: Lincoln, RI, USA, 2011. [Google Scholar]
- Sararaks, S.; Azman, A.B.; Low, L.L.; Rugayah, B.; Aziah, A.M.; Hooi, L.N.; Razak, A.M.; Norhaya, M.R.; Lim, K.B.; Azian, A.A.; et al. Validity and reliability of the SF-36: The Malaysian context. Malays. Med. J. 2005, 41, 790–800. [Google Scholar]
- Al-Ahaideb, A.; Alrushud, A.; El-Sobkey, S.; Hafez, A. Impact of knee osteoarthritis on the quality of life among Saudi elders: A comparative study. Saudi J. Sports Med. 2013, 13, 10. [Google Scholar] [CrossRef]
- Mahmoudi, S.F.; Toulgui, E.; ben Jeddou, K.; Gaddour, M.; Jemni, S.; Khachnaoui, F. Quality of life for patient with knee osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, e158–e159. [Google Scholar] [CrossRef]
- Mahmoud, G.A.; Moghazy, A.; Fathy, S.; Niazy, M.H. Osteoarthritis knee hip quality of life questionnaire assessment in Egyptian primary knee osteoarthritis patients: Relation to clinical and radiographic parameters. Egypt. Rheumatol. 2018, 41, 65–69. [Google Scholar] [CrossRef]
- Helminen, E.E.; Sinikallio, S.H.; Valjakka, A.L.; Väisänen-Rouvali, R.H.; Arokoski, J.P.A.A. Determinants of pain and functioning in knee osteoarthritis: A one-year prospective study. Clin. Rehabil. 2016, 30, 890–900. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.; Kim, H.A.; Seo, Y.-I.; Song, Y.W.; Hunter, D.J.; Jeong, J.Y.; Kim, D.H. Tibiofemoral osteoarthritis affects quality of life and function in elderly Koreans, with women more adversely affected than men. BMC Musculoskelet. Disord. 2011, 11, 129. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.K.; Owens, B.D.; Akelman, M.R.; Karamchedu, N.P.; Fadale, P.D.; Hulstyn, M.J.; Shalvoy, R.M.; Badger, G.J.; Fleming, B.C. Preoperative KOOS and SF-36 Scores Are Associated With the Development of Symptomatic Knee Osteoarthritis at 7 Years After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2018, 46, 869–875. [Google Scholar] [CrossRef]
- Heuts, P.H.T.G.; Vlaeyen, J.W.S.; Roelofs, J.; de Bie, R.A.; Aretz, K.; van Weel, C.; van Schayck, O.C.P. Pain-related fear and daily functioning in patients with osteoarthritis. Pain 2004, 110, 228–235. [Google Scholar] [CrossRef]
- Skou, S.T.; Rasmussen, S.; Simonsen, O.; Roos, E.M. Knee Confidence as It Relates to Self-reported and Objective Correlates of Knee Osteoarthritis: A Cross-sectional Study of 220 Patients. J. Orthop. Sports Phys. Ther. 2015, 45, 765–771. [Google Scholar] [CrossRef]
- He, Y.; Zhang, M.; Lin, E.H.; Bruffaerts, R.; Posada-Villa, J.; Angermeyer, M.C.; Levinson, D.; De Girolamo, G.; Uda, H.; Mneimneh, Z.; et al. Mental disorders among persons with arthritis: Results from the World Mental Health Surveys. Psychol. Med. 2008, 38, 1639–1650. [Google Scholar] [CrossRef]
- Smith, B.W.; Zautra, A.J. The Effects of Anxiety and Depression on Weekly Pain in Women with Arthritis. Pain 2008, 138, 354–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Questionnaire | Variables | Description |
|---|---|---|
| KOOS [26] | Symptom | Questions on symptoms such as swelling, restricted range of motion, and mechanical symptoms. |
| Pain | Level of pain experienced while bending the knee, straightening the knee, walking on flat surface, standing upright, and at night while in bed. | |
| Function in daily activities | Limitation experienced during function in daily activities. | |
| Function in recreational activities | Limitation experienced during function in recreational activities. | |
| Knee-specific quality of life | Questions on patients’ knee-specific quality of life. | |
| SF-36-PCS [31] | Physical Functioning | Severe and minor physical limitations in extremes of physical activities, including lifting and carrying groceries, climbing stairs, bending, kneeling, stooping, and walking moderate distances. |
| Role Physical | Physical health-related role limitations, including: (a) limitations in the kind of work or other usual activities, (b) reductions in the amount of time spent on work or other usual activities, (c) difficulty performing work or other usual activities, (d) accomplishing less. | |
| Bodily pain | Comprises 2 items: (a) pertaining to the intensity of bodily pain, (b) measuring the extent of interference with normal work activities due to pain. | |
| General Health | A rating of health (excellent to poor) and four items addressing the views and expectations of his or her health. | |
| SF-36-MCS [30] | Vitality | Measure of energy level and fatigue, developed to capture differences in subjective well-being |
| Social Functioning | Health-related effects on quantity and quality of social activities, asking specifically about the impact of either physical or emotional problems on social activities. | |
| Role emotional | Mental health-related role limitations in terms of: (a) time spent on work or other usual activities, (b) amount of work or activities accomplished, (c) the care with which work or other activities were performed | |
| Mental Health | One or more items from each of four major mental health dimensions (anxiety, depression, loss of behavioural/emotional control, and psychological well-being). |
| Variables | n (%) | Mean (±SD) |
|---|---|---|
| Age (years) | 66.8 (±7.06) | |
| Gender: | ||
| Male | 123 (42.4) | |
| Female | 167 (57.6) | |
| Ethnicity: | ||
| Malay | 231 (79.7) | |
| Chinese | 35 (12.1) | |
| Indian | 24 (8.3) | |
| Education: | ||
| No formal education | 17 (5.9) | |
| Primary level | 74 (25.1) | |
| Secondary level | 134 (46.2) | |
| Tertiary level | 65 (22.4) | |
| Occupational status: | ||
| Desk work | 70 (24.1) | |
| Labour worker | 44 (15.2) | |
| Unemployed | 105 (36.2) | |
| Retiree | 71 (24.1) | |
| Personal income (RM): | ||
| B40 (<4360) | 219 (75.5) | |
| M40 (4360–9619) | 71 (24.5) | |
| Smoking status: | ||
| Yes | 27 (9.3) | |
| No | 263 (90.7) | |
| OA Severity: | ||
| Mild | 151 (52.1) | |
| Moderate | 139 (47.9) | |
| Family history of knee OA: | ||
| Yes | 75 (25.9) | |
| No | 215 (74.1) | |
| Current knee OA treatment: | ||
| Not on any medication | 59 (20.3) | |
| Topical treatment | 150 (51.7) | |
| Oral medication | 62 (21.4) | |
| Intra-articular injection | 19 (6.6) | |
| Ever have physiotherapy session: | ||
| Yes | 99 (34.1) | |
| No | 191 (65.9) | |
| Walking assistance: | ||
| No | 267 (92.1) | |
| Walking stick/walking frame | 18 (6.2) | |
| Others/Wheelchair | 5 (1.7) |
| No. | Domains | Mean | ±SD |
|---|---|---|---|
| 1 | Symptom | 50.28 | 14.81 |
| 2 | Pain | 49.68 | 14.71 |
| 3 | Function in daily activities | 53.51 | 13.65 |
| 4 | Function in recreational activities | 43.53 | 20.28 |
| 5 | Knee-specific quality of life | 41.03 | 18.69 |
| Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Physical Functioning | 41.5 | 8.0 | 21.18 | 57.54 |
| Role-Physical | 36.1 | 7.0 | 21.23 | 57.16 |
| Bodily Pain | 44.6 | 6.67 | 25.71 | 62.00 |
| General Health | 39.9 | 4.2 | 28.46 | 54.61 |
| Physical Component Summary | 45.2 | 5.3 | 32.38 | 62.44 |
| Vitality | 42.8 | 6.1 | 22.89 | 58.54 |
| Social Functioning | 37.6 | 3.3 | 22.25 | 47.31 |
| Role-Emotional | 29.8 | 8.8 | 14.39 | 56.17 |
| Mental Health | 31.2 | 8.6 | 11.63 | 53.48 |
| Mental Component Summary | 31.4 | 8.7 | 8.49 | 48.78 |
| Subdomains of HRQoL | Adj. B (95%CI) | Standardised Coefficient Beta | t | p-Value | R2 |
|---|---|---|---|---|---|
| * Physical Component Summary | |||||
| Constant | 2.139 | 36.494 | |||
| Symptom | 0.029 (0.049, 0.107) | 0.186 | 2.174 | 0.002 | 0.211 |
| Pain | 0.063 (0.044, 0.169) | 0.345 | 3.143 | 0.001 | |
| Function in daily living | 0.168 (0.073, 0.284) | 0.335 | 3.133 | 0.002 | |
| ** Mental Component Summary | |||||
| Constant | 2.071 | 22.076 | |||
| Function in daily living | 0.624 (0.478, 0.769) | 0.677 | 8.445 | <0.001 | 0.213 |
| Function in recreational activities | 0.237 (0.335, 0.139) | 0.382 | 4.762 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohd Yusuf, S.Y.; Md-Yasin, M.; Mohd Miswan, M.F. Does Less Pain Predict Better Quality of Life among Malaysian Patients with Mild–Moderate Knee Osteoarthritis? Clin. Pract. 2022, 12, 219-230. https://0-doi-org.brum.beds.ac.uk/10.3390/clinpract12020026
Mohd Yusuf SY, Md-Yasin M, Mohd Miswan MF. Does Less Pain Predict Better Quality of Life among Malaysian Patients with Mild–Moderate Knee Osteoarthritis? Clinics and Practice. 2022; 12(2):219-230. https://0-doi-org.brum.beds.ac.uk/10.3390/clinpract12020026
Chicago/Turabian StyleMohd Yusuf, Salma Yasmin, Mazapuspavina Md-Yasin, and Mohd Fairudz Mohd Miswan. 2022. "Does Less Pain Predict Better Quality of Life among Malaysian Patients with Mild–Moderate Knee Osteoarthritis?" Clinics and Practice 12, no. 2: 219-230. https://0-doi-org.brum.beds.ac.uk/10.3390/clinpract12020026