Factors Associated with the Regularity of Physical Exercises as a Means of Improving the Public Health System in Vietnam

 ,
,  ,
, 
 ,
,
Abstract
:1. Background
2. Literature Review
3. Materials and Methods
3.1. Materials
3.2. Methods
- –
- “Sex” includes two categories, “Male” and “Female.”
- –
- “Edu” is short for educational background, which includes two groups: “Highschool” (the people with high-school education or less) and “Graduate” (the people with a university education or higher).
- –
- “BMI”, or body mass index, has five categories: <18.5 (Underweight), 18.5–22.99 (Normal), 23–24.99 (Pre-obese), 25–29.99 (Obese level I), and >=30 (Obese level II). During the survey, the subjects were asked to provide their most recent measurements of height (in cm) and weight (in kg), based on which their BMI was calculated using the following formula: BMI = weight/(height × height).
- –
- “ExamTools” is short for habitually checking health status in the family with common medical tools. The question was, “Does your family regularly take simple medical measurements (blood pressure, eyesight, weight, etc.)?” There were two options, “Yes” and “No.”
- –
- “HealthCom” is short for the perception of the participants towards the quality of mass communication on periodic GHEs; it is rated in a scale from 1 to 5, with 1 being the lowest and 5 being the highest.
4. Results
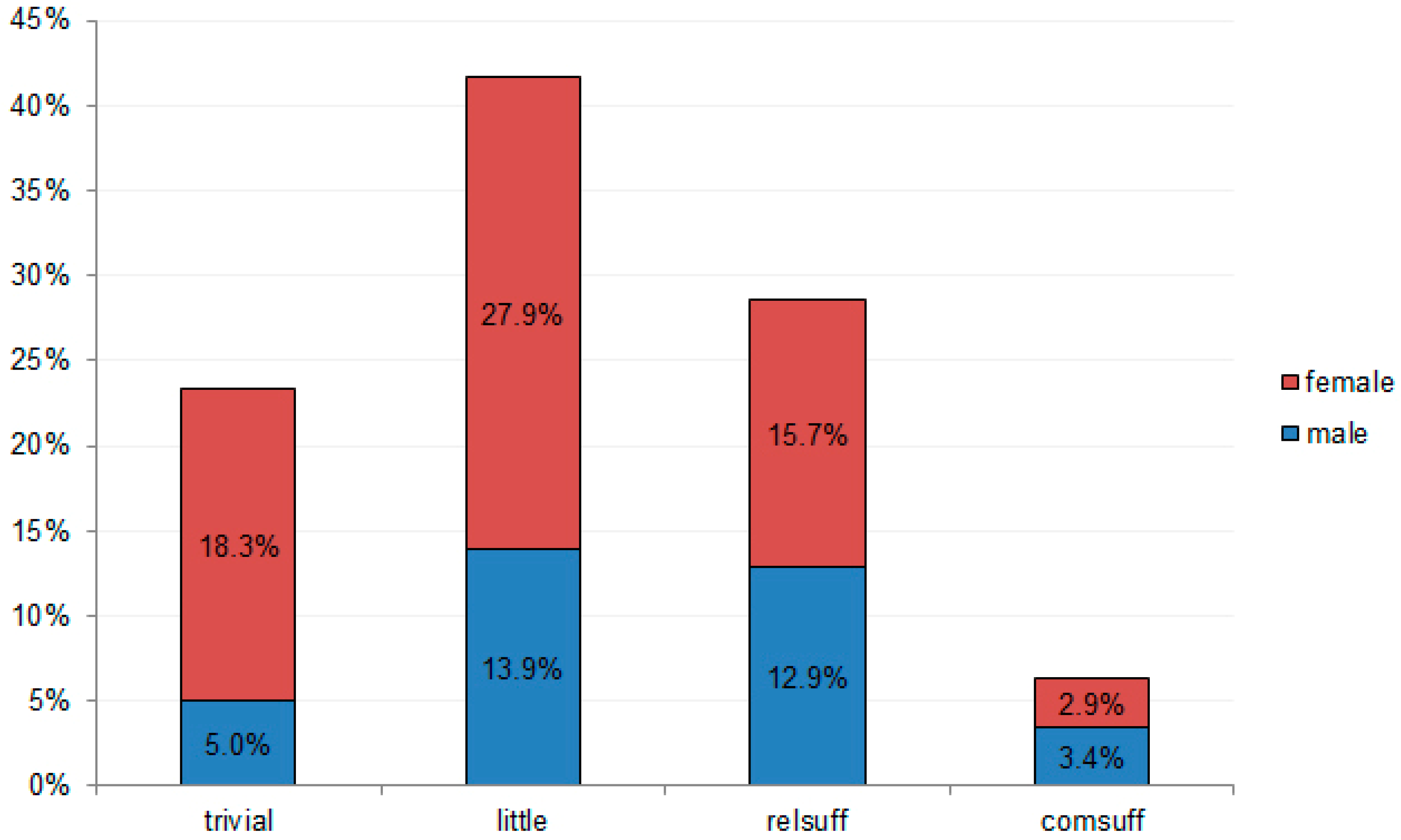
4.1. Descriptive Statistics
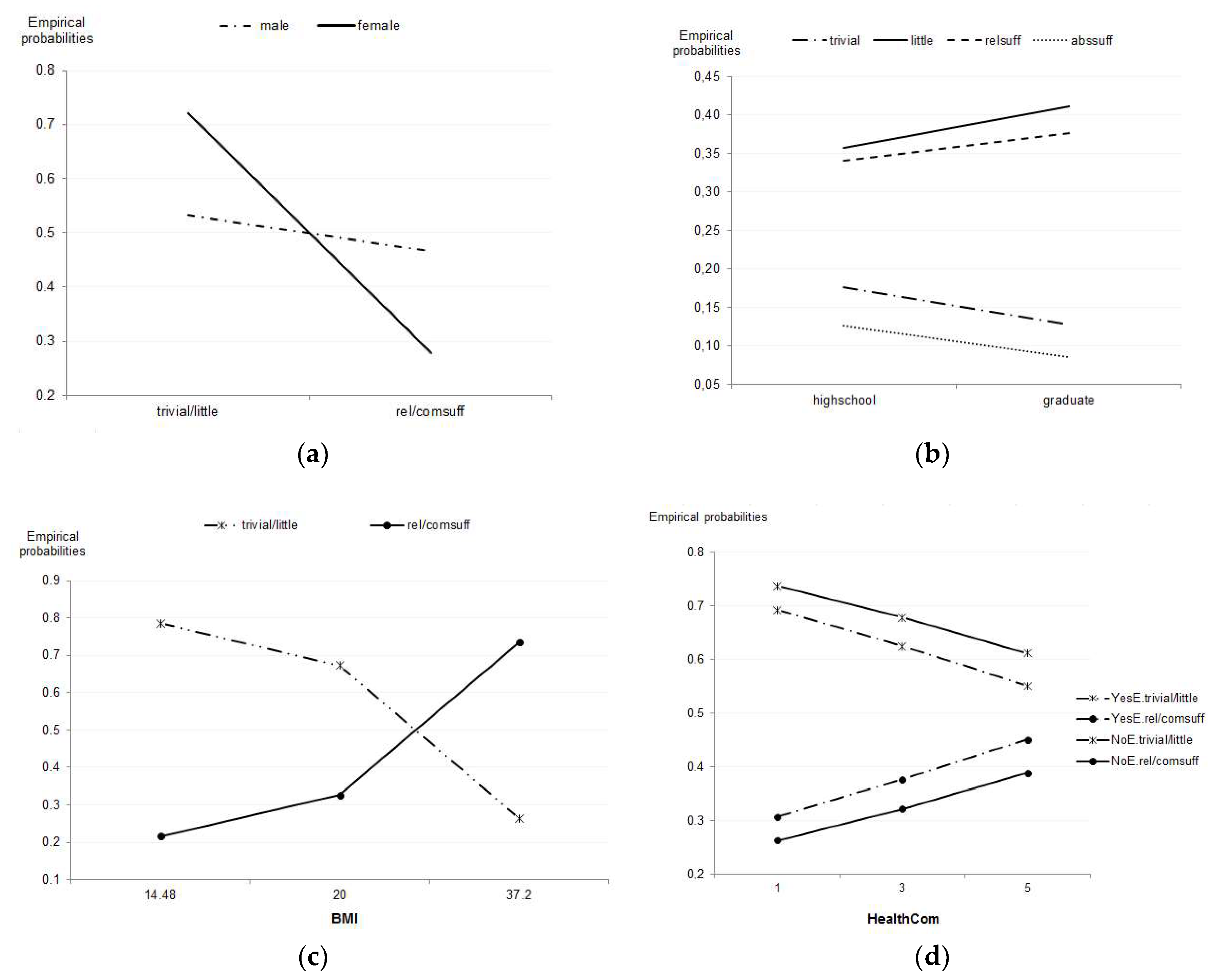
4.2. EAS Regularity Associated with Sex, Educational Background, and BMI
4.3. EAS regularity Associated with Perception on Health Communication Quality and Habitual Health Checks at Home
4.4. Interpretation of Estimation Results
4.4.1. Physiological Factors
4.4.2. External Factors
5. Discussion
5.1. Policy Implications
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| a. Probabilities of EAS regularity towards gender and education. | ||||||||
| “EvalExer” | “trivial” | “little” | “relsuff” | “abssuff” | ||||
| “Edu”|”Sex” | “male” | “female” | “male” | “female” | “male” | “female” | “male” | “female” |
| “highschool” | 0.176 | 0.347 | 0.357 | 0.375 | 0.341 | 0.219 | 0.126 | 0.059 |
| “graduate” | 0.128 | 0.261 | 0.411 | 0.448 | 0.376 | 0.250 | 0.085 | 0.041 |
| b. Probabilities of EAS regularity towards BMI. | ||||||||
| “EvalExer” | ||||||||
| “bmi” | “edu” | “trivial” | “little” | “relsuff” | “abssuff” | |||
| 14.48 | “highschool” | 0.370 | 0.415 | 0.167 | 0.049 | |||
| “graduate” | 0.286 | 0.493 | 0.188 | 0.033 | ||||
| 20 | “highschool” | 0.292 | 0.381 | 0.249 | 0.078 | |||
| “graduate” | 0.224 | 0.447 | 0.277 | 0.052 | ||||
| 37.20 | “highschool” | 0.086 | 0.179 | 0.531 | 0.204 | |||
| “graduate” | 0.066 | 0.209 | 0.589 | 0.135 | ||||
| c. Probabilities of EAS regularity towards health communication quality and usual medical practice in the family. | ||||||||
| “EvalExer” | ||||||||
| “HealthCom” | “Examtools” | “trivial” | “little” | “relsuff” | “abssuff” | |||
| 1 | Yes | 0.265 | 0.427 | 0.256 | 0.051 | |||
| No | 0.283 | 0.454 | 0.234 | 0.029 | ||||
| 3 | Yes | 0.222 | 0.403 | 0.298 | 0.078 | |||
| No | 0.241 | 0.437 | 0.277 | 0.045 | ||||
| 5 | Yes | 0.180 | 0.370 | 0.336 | 0.114 | |||
References
- Van Bui, T.; Blizzard, C.L.; Luong, K.N.; Le Van Truong, N.; Tran, B.Q.; Otahal, P.; Srikanth, V.; Nelson, M.R.; Au, T.B.; Ha, S.T. Physical activity in Vietnam: Estimates and measurement issues. PLoS ONE 2015, 10, e0140941. [Google Scholar]
- Althoff, T.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, P. Vietnamese People among the Most Sedentary in the World—Survey. Available online: https://e.vnexpress.net/news/business/data-speaks/vietnamese-people-among-the-most-sedentary-in-the-world-survey-3613038.html (accessed on 17 April 2018).
- Tuan, N.; Tuong, P.; Popkin, B. Body mass index (BMI) dynamics in Vietnam. Eur. J. Clin. Nutr. 2008, 62, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Cuong, T.; Dibley, M.; Bowe, S.; Hanh, T.; Loan, T. Obesity in adults: An emerging problem in urban areas of Ho Chi Minh City, Vietnam. Eur. J. Clin. Nutr. 2007, 61, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.D.; Beresford, S.A.; Drewnowski, A. Trends in overweight by socio-economic status in Vietnam: 1992 to 2002. Public Health Nutr. 2007, 10, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Craig, D. Familiar Medicine: Everyday Health Knowledge and Practice in Today’s Vietnam; University of Hawaii Press: Honolulu, HI, USA, 2002. [Google Scholar]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- De Rezende, L.F.M.; Azeredo, C.M.; Canella, D.S.; Claro, R.M.; de Castro, I.R.R.; Levy, R.B.; do Carmo Luiz, O. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health 2014, 14, 485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heseltine, R.; Skelton, D.A.; Kendrick, D.; Morris, R.W.; Griffin, M.; Haworth, D.; Masud, T.; Iliffe, S. “Keeping Moving”: Factors associated with sedentary behaviour among older people recruited to an exercise promotion trial in general practice. BMC Fam. Pract. 2015, 16, 67. [Google Scholar] [CrossRef] [PubMed]
- Humpel, N.; Owen, N.; Leslie, E. Environmental factors associated with adults’ participation in physical activity: A review. Am. J. Prevent. Med. 2002, 22, 188–199. [Google Scholar] [CrossRef]
- Bonaiuto, M.; Aiello, A.; Perugini, M.; Bonnes, M.; Ercolani, A.P. Multidimensional perception of residential environment quality and neighbourhood attachment in the urban environment. J. Environ. Psychol. 1999, 19, 331–352. [Google Scholar] [CrossRef]
- Minichilli, F.; Gorini, F.; Ascari, E.; Bianchi, F.; Coi, A.; Fredianelli, L.; Licitra, G.; Manzoli, F.; Mezzasalma, L.; Cori, L. Annoyance Judgment and Measurements of Environmental Noise: A Focus on Italian Secondary Schools. Int. J. Environ. Res. Public Health 2018, 15, 208. [Google Scholar] [CrossRef] [PubMed]
- Cassina, L.; Fredianelli, L.; Menichini, I.; Chiari, C.; Licitra, G. Audio-Visual Preferences and Tranquillity Ratings in Urban Areas. Environments 2018, 5, 1. [Google Scholar] [CrossRef]
- Wilson, M.G.; Ellison, G.M.; Cable, N.T. Basic science behind the cardiovascular benefits of exercise. Br. J. Sports Med. 2016, 50, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, W.L.; Wilmore, J.; Costill, D. Physiology of Sport and Exercise, 6th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- McNally, S. Exercise: The Miracle Cure and the Role of the Doctor in Promoting It; Academy of Medical Royal Colleges: London, UK, 2015. [Google Scholar]
- Macera, C.A.; Jones, D.A.; Yore, M.; Ham, S.; Kohl, H.W.; Kimsey Jr, C.; Buchner, D. Prevalence of physical activity, including lifestyle activities among adults-United States, 2000–2001. Morb. Mortality Wkly. Rep. 2003, 52, 764–769. [Google Scholar]
- Beck, B.R.; Daly, R.M.; Singh, M.A.F.; Taaffe, D.R. Exercise and Sports Science Australia (ESSA) position statement on exercise prescription for the prevention and management of osteoporosis. J. Sci. Med. Sport 2017, 20, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; Stowasser, M. Australian association for exercise and sports science position statement on exercise and hypertension. J. Sci. Med. Sport 2009, 12, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Tiedemann, A.; Sherrington, C.; Close, J.C.; Lord, S.R. Exercise and Sports Science Australia position statement on exercise and falls prevention in older people. J. Sci. Med. Sport 2011, 14, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Valderrabano, V.; Steiger, C. Treatment and prevention of osteoarthritis through exercise and sports. J. Aging Res. 2011, 2011, 374653. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; Williams, A.D.; Levinger, I.; Selig, S.; Howden, E.; Coombes, J.S.; Fassett, R.G. Exercise & Sports Science Australia (ESSA) position statement on exercise and chronic kidney disease. J. Sci. Med. Sport 2013, 16, 406–411. [Google Scholar] [PubMed]
- Warner, S.; Dixon, M.A. Competition, gender, and the sport experience: An exploration among college athletes. Sport Educ. Soc. 2015, 20, 527–545. [Google Scholar] [CrossRef]
- Sheel, A.W.; Richards, J.C.; Foster, G.E.; Guenette, J.A. Sex differences in respiratory exercise physiology. Sports Med. 2004, 34, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Hagströmer, M.; Kwak, L.; Oja, P.; Sjöström, M. A 6 year longitudinal study of accelerometer-measured physical activity and sedentary time in Swedish adults. J. Sci. Med. Sport 2015, 18, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Carroll, M.D.; Kit, B.K.; Ogden, C.L. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA 2012, 307, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.J.; Raji, C.A.; Becker, J.T.; Lopez, O.L.; Kuller, L.H.; Hua, X.; Dinov, I.D.; Stein, J.L.; Rosano, C.; Toga, A.W. The effects of physical activity, education, and body mass index on the aging brain. Hum. Brain Mapping 2011, 32, 1371–1382. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.; Stanforth, P.; Gagnon, J.; Rankinen, T.; Leon, A.; Rao, D.; Skinner, J.; Bouchard, C.; Wilmore, J. The effect of sex, age and race on estimating percentage body fat from body mass index: The Heritage Family Study. Int. J. Obesity 2002, 26, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Thornton, J.C.; Russell, M.; Burastero, S.; Heymsfield, S.; Pierson Jr, R.N. Asians have lower body mass index (BMI) but higher percent body fat than do whites: Comparisons of anthropometric measurements. Am. J. Clin. Nutr. 1994, 60, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Johansson, S.-E. The influence of socioeconomic status, ethnicity and lifestyle on body mass index in a longitudinal study. Int. J. Epidemiol. 1998, 27, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rantanen, T.; Parkatti, T.; Heikkinen, E. Muscle strength according to level of physical exercise and educational background in middle-aged women in Finland. Eur. J. Appl. Physiol. Occup. Physiol. 1992, 65, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Keller, P.A.; Lehmann, D.R. Designing Effective Health Communications: A Meta-Analysis. J. Public Policy Mark. 2008, 27, 117–130. [Google Scholar] [CrossRef] [Green Version]
- Regitz-Zagrosek, V. Sex and gender differences in health. Sci. Soc. Ser. Sex Sci. 2012, 13, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansfield, A.K.; Addis, M.E.; Mahalik, J.R. “Why won’t he go to the doctor?”: The psychology of men’s help seeking. Int. J. Men’s Health 2003, 2, 93. [Google Scholar] [CrossRef]
- Wellstead, P. Information behaviour of Australian men experiencing stressful life events: The role of social networks and confidants. Inf. Res. 2011, 16, 12120429. [Google Scholar]
- Block, L.G.; Keller, P.A. Effects of self-efficacy and vividness on the persuasiveness of health communications. J. Consum. Psychol. 1997, 6, 31–54. [Google Scholar] [CrossRef]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Kreps, G.L.; Sivaram, R. Strategic health communication across the continuum of breast cancer care in limited-resource countries. Cancer 2008, 113, 2331–2337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiatt, R.; Pasick, R.; Stewart, S.; Bloom, J.; Davis, P.; Gardiner, P.; Johnston, M.; Luce, J.; Schorr, K.; Brunner, W.; et al. Community-based cancer screening for underserved women: Design and baseline findings from the Breast and Cervical Cancer Intervention Study. Prev. Med. 2001, 33, 190–203. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.H. Vietnam General Health Examinations Propensity Survey 2016. Available online: https://osf.io/afz2w/ (accessed on 23 October 2018).
- Vuong, Q.H.; Ho, T.M.; Nguyen, H.K.; Vuong, T.T. Healthcare consumers’ sensitivity to costs: A reflection on behavioural economics from an emerging market. Palgrave Commun. 2018, 4, 70. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; La, V.-P.; Vuong, T.-T.; Ho, M.-T.; Nguyen, H.-K.T.; Nguyen, V.-H.; Pham, H.-H.; Ho, M.-T. An open database of productivity in Vietnam’s social sciences and humanities for public use. Sci. Data 2018, 5, 180188. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; da Silva Santos, L.B.; Bourne, P.E. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, Q.H. Survey data on Vietnamese propensity to attend periodic general health examinations. Scientific Data 2017, 4, 170142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agresti, A. Categorical Data Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Vuong, Q.H.; Vuong, T.T.; Ho, T.M.; Nguyen, H.V. Psychological and socio-economic factors affecting social sustainability through impacts on perceived health care quality and public health: The case of Vietnam. Sustainability 2017, 9, 1456. [Google Scholar] [CrossRef]
- State Audit of Vietnam. Nghi Quyet 21 NQ-TW cua Ban Chap Hanh Trung Uong Dang Ve Cong Tac Dan So Trong Tinh Hinh Doi Moi [Resolution 21 of Central Steering Committee on Population Works in a New era]. Available online: http://vanban.sav.gov.vn/2072-1-ddt/nghi-quyet-21nqtw-ngay-25102017-cua-ban-chap-hanh-trung-uong-ve-cong-tac-dan-so-trong-tinh-hinh-moi.sav (accessed on 17 April 2018).
- Duy Tien. Vietnamese among the Shortest, Research Reveals. Available online: http://en.cand.com.vn/Law-Society/Vietnamese-among-the-shortest-research-reveals-459912/ (accessed on 3 October 2018).
- World Health Organization. UN Interagency Task Force on NCDs Joint Country Mission to Viet Nam. Available online: http://www.who.int/ncds/un-task-force/vietnam-mission-september-2016/en/ (accessed on 17 April 2018).



{kind=link}
{kind=link}
| Characteristics | N | Percentage (%) |
|---|---|---|
| Age | ||
| <30 | 1306 | 63.15 |
| 30–49 | 643 | 31.09 |
| ≥50 | 119 | 5.76 |
| Sex | ||
| Male | 728 | 35.20 |
| Female | 1340 | 64.80 |
| Educational background | ||
| High school or less | 558 | 26.98 |
| University or above | 1.510 | 73.02 |
| BMI | ||
| <18.5 (Underweight) | 408 | 19.73 |
| 18.5–22.99 (Normal) | 1242 | 60.06 |
| 23–24.99 (Pre-obese) | 279 | 13.49 |
| 25–29.99 (Obese level I) | 128 | 6.19 |
| >=30 (Obese level II) | 11 | 0.53 |
| Checking up health at home regularly (blood pressure, weight, eyesight, etc.) | ||
| Yes | 1242 | 60.06 |
| No | 826 | 39.94 |
| The level of exercise and sports regularity | ||
| Completely sufficient | 132 | 6.38 |
| Relatively sufficient | 591 | 28.58 |
| Little | 863 | 41.73 |
| Trivial | 482 | 23.31 |
| Characteristics | Min | Max | Average | SD | CI |
|---|---|---|---|---|---|
| Age | 18 | 83 | 29.17 | 10.09 | 28.73–29.60 |
| BMI | 14.48 | 37.20 | 20.85 | 2.69 | 20.73–20.96 |
| Health communication quality perception | 1 | 5 | 2.83 | 1.170 | 2.79–2.87 |
| (3a) | Intercept | “Sex” | “Edu” |
| “Male” | “Highschool” | ||
| logit(trivial|comsuff) | 1.846 *** [12.065] | −1.437 *** [−6.926] | −0.071 [−0.338] |
| logit(little|comsuff) | 2.387 *** [16.134] | −0.808 *** [−4.256] | −0.536 ** [−2.686] |
| logit(relsuff|comsuff) | 1.805 *** [11.818] | −0.315 [−1.623] | −0.491 * [−2.394] |
| Significant codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1; z−value in square brackets; baseline category for “Sex” = “Female” and “Edu” = “Graduate”. Log-likelihood: −36.94 with 3 degrees of freedom. Residual deviance: 4.17 with 3 degrees of freedom. | |||
| (3b) | Intercept | “Edu” | “BMI” |
| “Highschool” | |||
| logit(trivial|comsuff) | 4.006 *** [5.297] | −0.14 [−0.677] | −0.127 *** [−3.586] |
| logit(little|comsuff) | 4.158 *** [5.837] | −0.568 ** [−2.860] | −0.100 ** [−3.025] |
| logit(relsuff|comsuff) | 1.919 ** [2.658] | −0.514 * [−2.510] | −0.012 [−0.366] |
| Significant codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1; z−value in square brackets; baseline category for “Edu” = “Graduate”. Log-likelihood: −2533.25 with 6195 degrees of freedom. Residual deviance: 5066.50 with 6195 degrees of freedom | |||
| (3c) | Intercept | “ExamTools” | “HealthCom” |
| “Yes” | |||
| logit(trivial|comsuff) | 2.563 *** [7.566] | −0.622 ** [−2.867] | −0.297 ** [−2.976] |
| logit(little|comsuff) | 2.973 *** [9.144] | −0.616 ** [−2.960] | −0.236 * [−2.497] |
| logit(relsuff|comsuff) | 2.205 *** [6.600] | −0.464 * [−2.171] | −0.132 [−1.358] |
| Significant codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1; z−value in square brackets; baseline category for “ExamTools” = “No”. Log-likelihood: −2546.62 with 6195 degrees of freedom. Residual deviance: 5093.25 with 6195 degrees of freedom. | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vuong, Q.-H.; Hoang, A.-D.; Vuong, T.-T.; La, V.-P.; Nguyen, H.K.T.; Ho, M.-T. Factors Associated with the Regularity of Physical Exercises as a Means of Improving the Public Health System in Vietnam. Sustainability 2018, 10, 3828. https://0-doi-org.brum.beds.ac.uk/10.3390/su10113828
Vuong Q-H, Hoang A-D, Vuong T-T, La V-P, Nguyen HKT, Ho M-T. Factors Associated with the Regularity of Physical Exercises as a Means of Improving the Public Health System in Vietnam. Sustainability. 2018; 10(11):3828. https://0-doi-org.brum.beds.ac.uk/10.3390/su10113828
Chicago/Turabian StyleVuong, Quan-Hoang, Anh-Duc Hoang, Thu-Trang Vuong, Viet-Phuong La, Hong Kong T. Nguyen, and Manh-Tung Ho. 2018. "Factors Associated with the Regularity of Physical Exercises as a Means of Improving the Public Health System in Vietnam" Sustainability 10, no. 11: 3828. https://0-doi-org.brum.beds.ac.uk/10.3390/su10113828