2.2. Risk Identification of the Rehabilitation Process Involving ASPIRE Structure
Risk is defined as “the exposure to the possibility of economic or financial loss or gain, physical damage, or injury, or delay as a consequence of the uncertainty associated with pursuing a particular course of action” [
30,
31].
When machineries come into the discussion a special regulation is used to carry on a risk assessment. ISO 12100:2010 “Safety of Machineries—General principles for design—Risk assessment and risk reduction” provides basic terminology, principles, and methodology for analyzing the safety in the design of machinery. Within this regulation are specified principles of risk assessment and risk reduction to help the designer to provide a safe behavior of the machinery [
32].
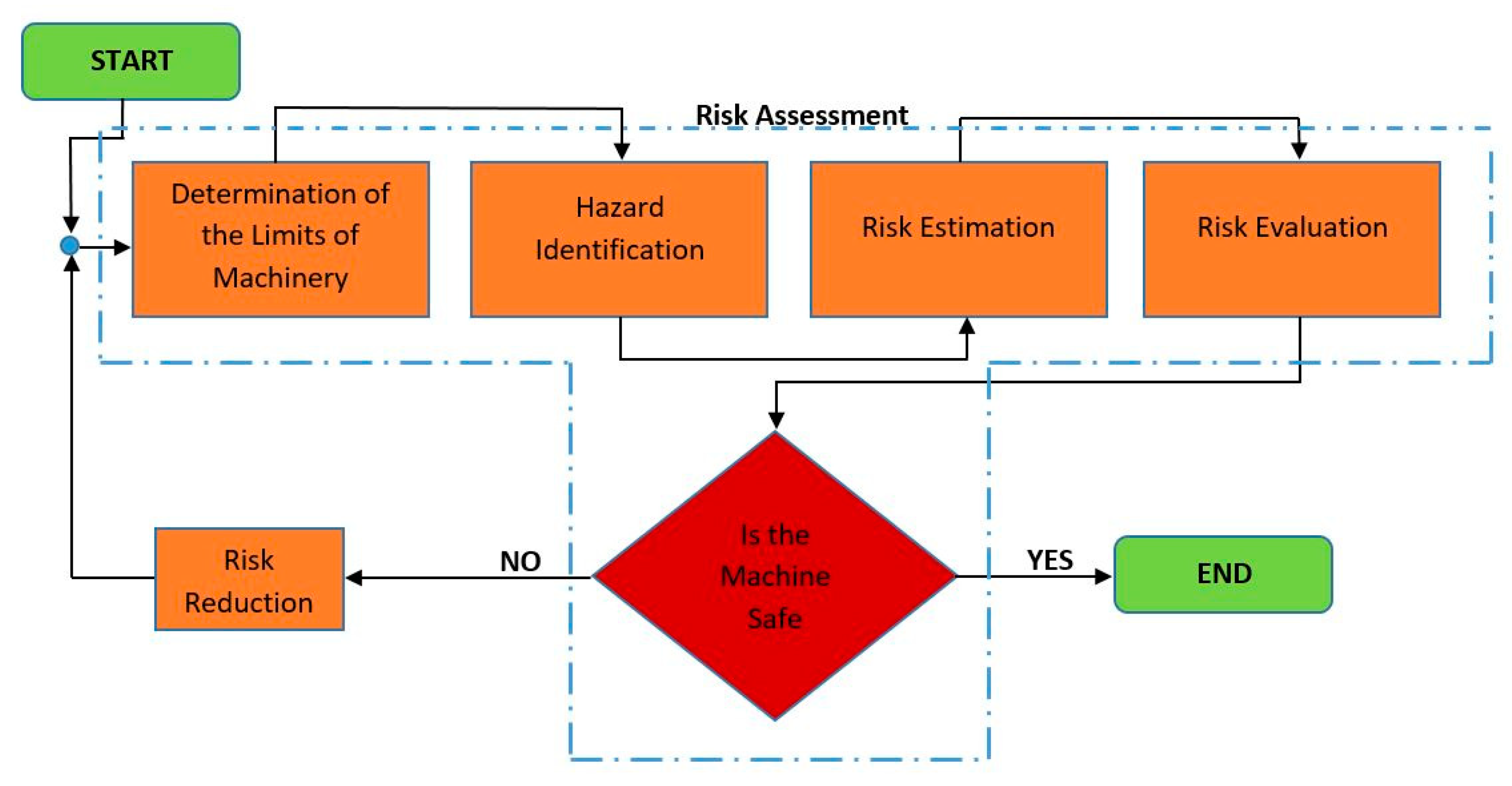
Figure 2 provides a simplified flow chart of the risk management analysis as proposed by ISO 12100:2010. The analysis is divided in five major steps: determination of the limits of the machinery, hazard identification, risk estimation, risk evaluation, and risk reduction. Each step is further analyzed within the paper.
Determination of the limits of the machinery is the first step of the risk management analysis, and it defines the running conditions of the robotic structure in terms of use, space, and time.
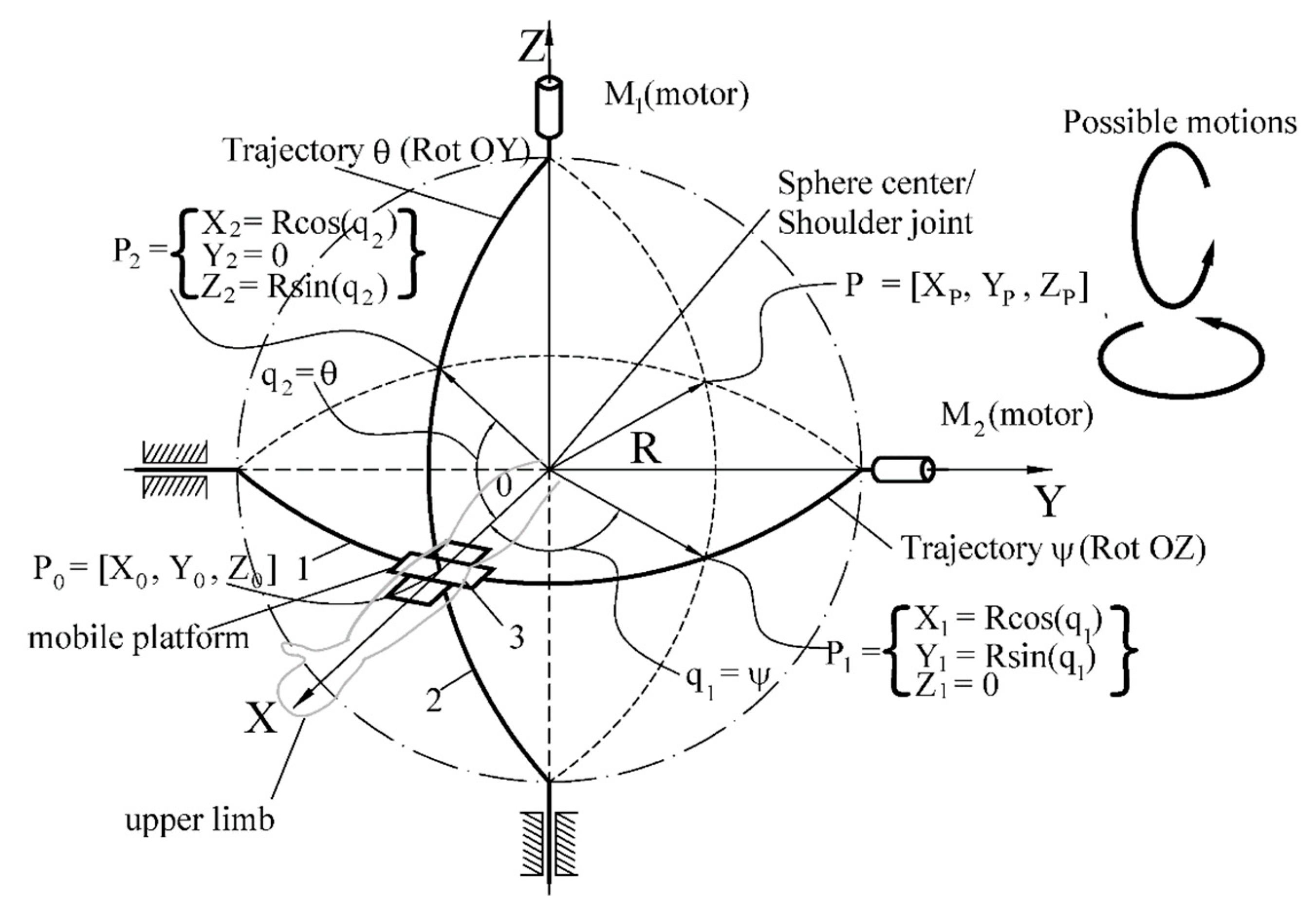
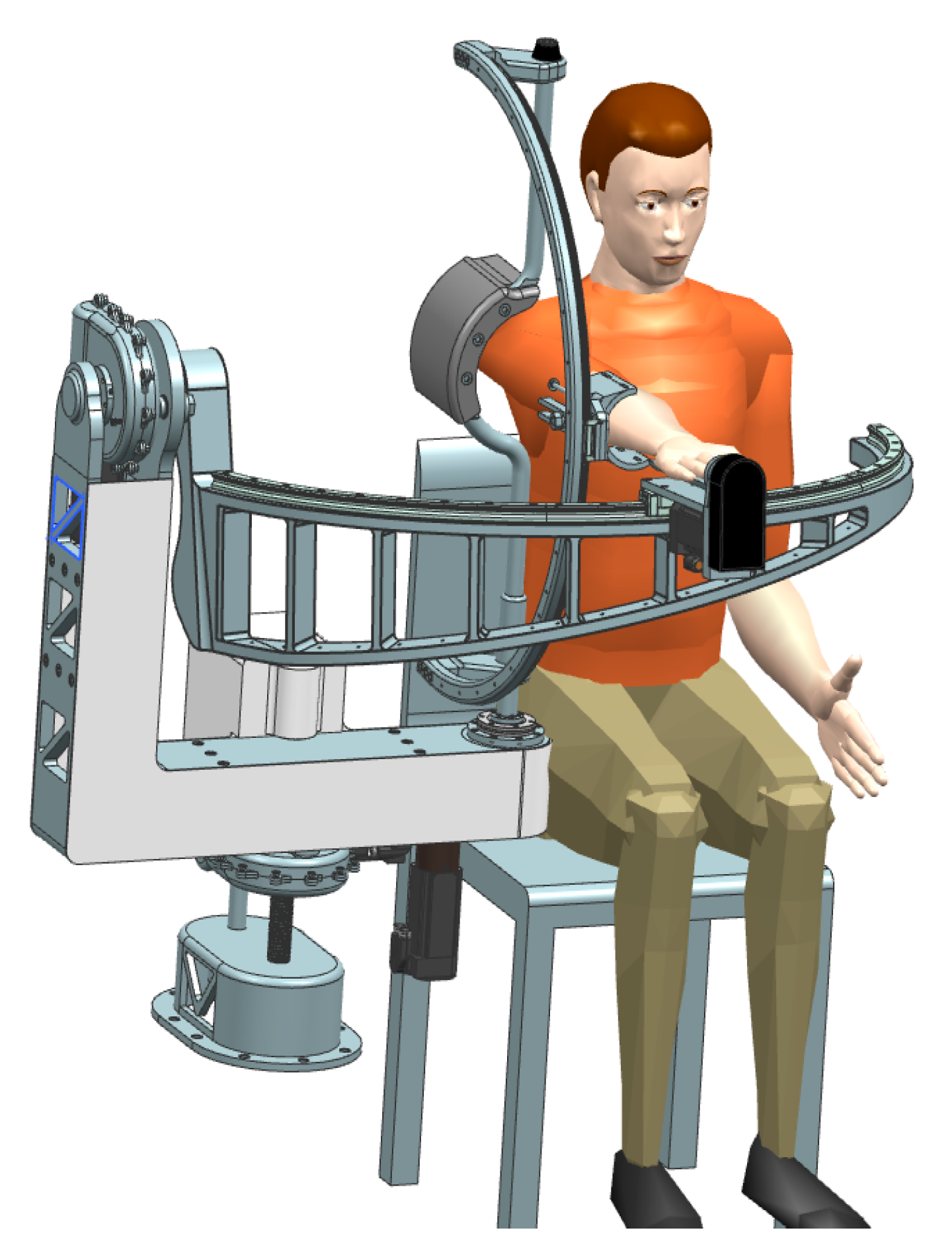
First, the relative position between the patient and the robotic structure is defined. During the rehabilitation procedure the patient is seated with the impaired arm attached to the robotic structure, which must perform motions that would replicate specific exercises defined by medical experts.
Normal running condition of the robotic system implies that the patient is seated with the arm attached on to the rehabilitation mechanism, and the patient, due to his impairment, cannot create any other resistance in the mechanism other than the one created by its own arm. Special attention should be paid when the patient regains some of the lost dexterity and some of the forces within the mechanism are reduced or amplified (depending on the degree of recovery, the patient can help the robotic structure in the rehabilitation process or he can create extra resistive moments into the mechanism by opposing the rehabilitation motion). A detailed analysis of the interaction modalities between the robot and the patient is illustrated in Thompson and Perry [
30].
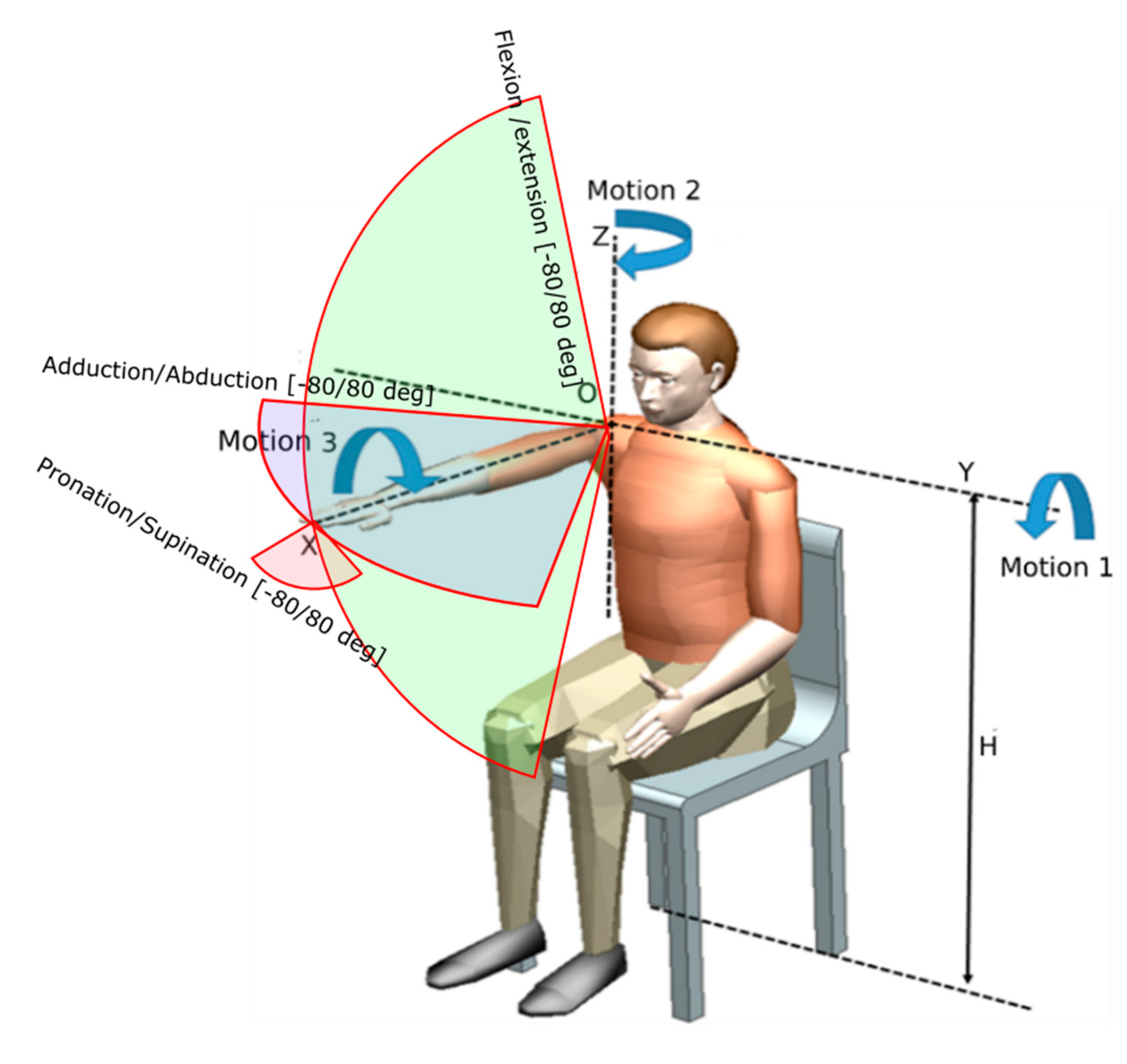
The rehabilitation motions targeted by ASPIRE are also identified using
Figure 3, where
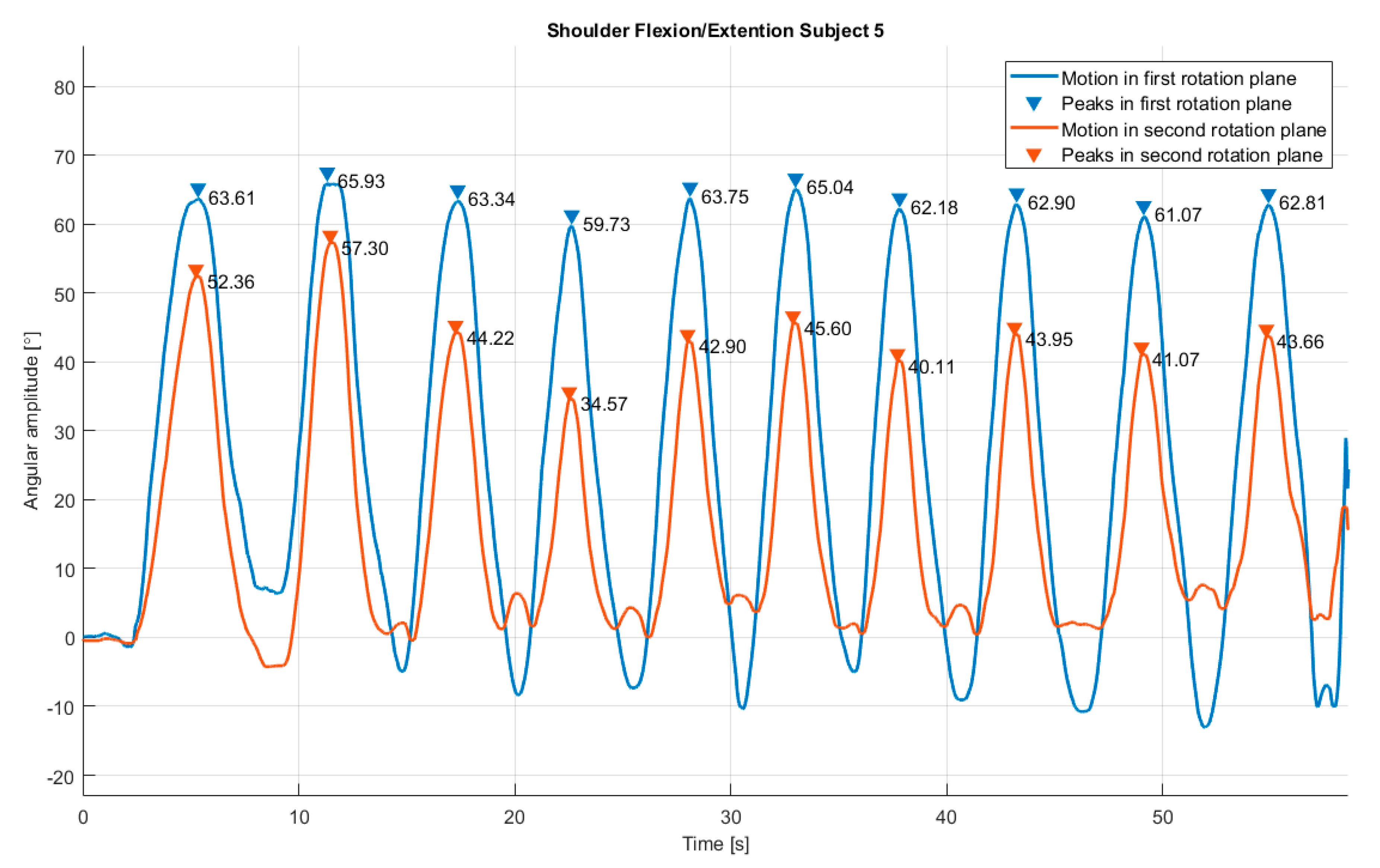
Motion 1—flexion /extension of the shoulder performed around OY axis with a maximum range of ±80;
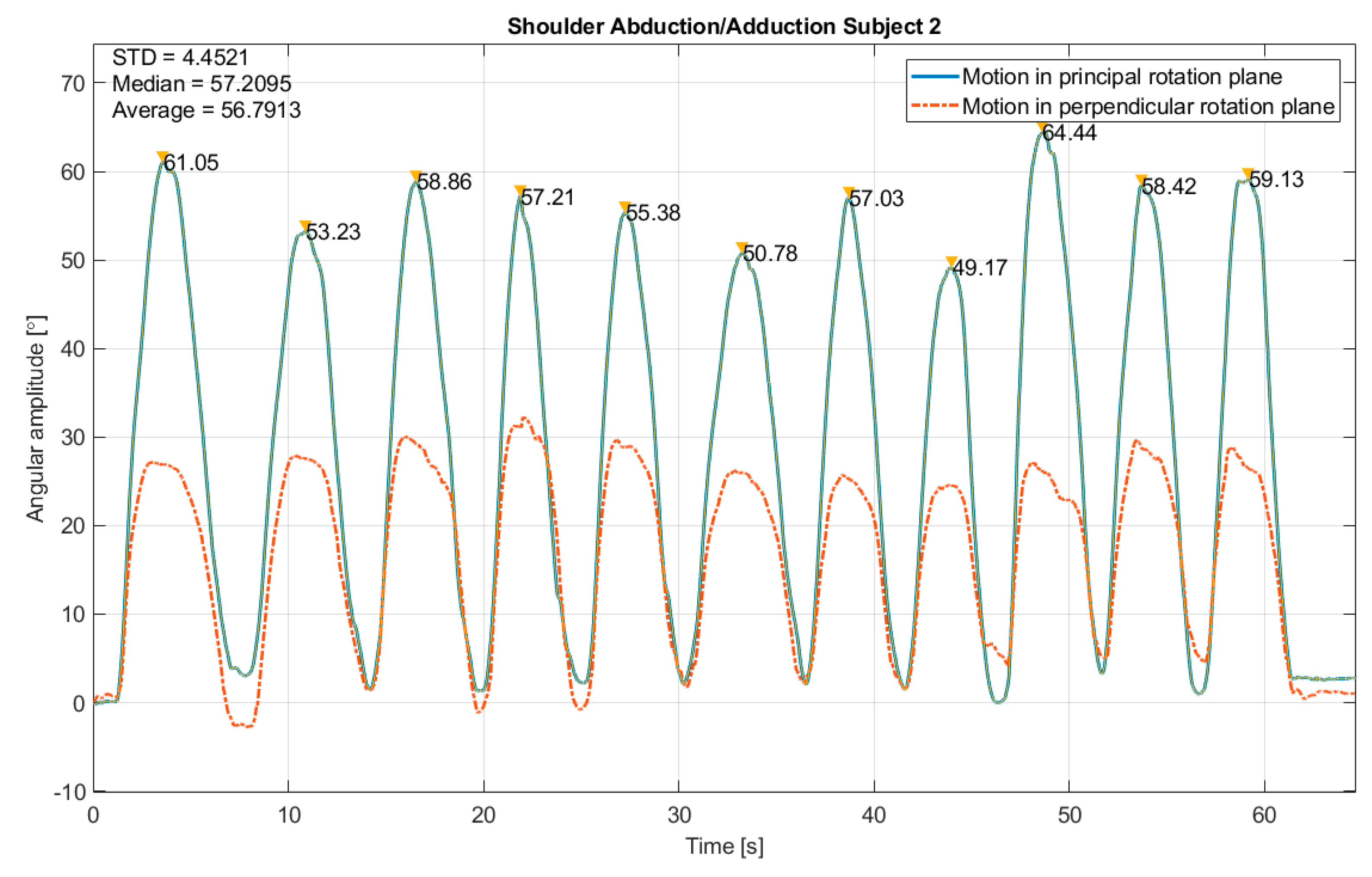
Motion 2—adduction/abduction of the shoulder performed around OZ axis with a maximum range of ±80;
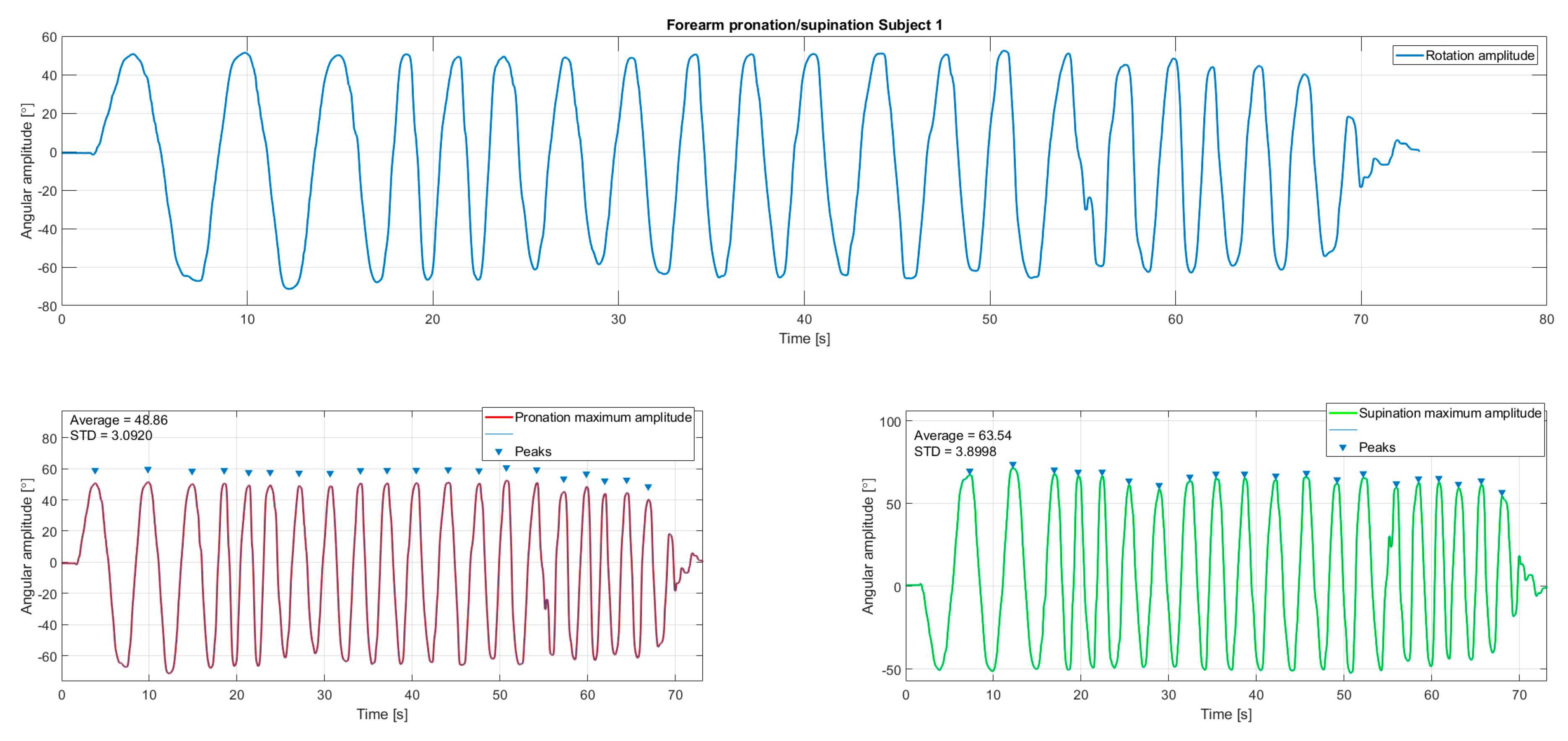
Motion 3—pronation/supination of the forearm performed around OX axis with a maximum range of ±80.
The total space volume occupied by the robotic structure should not exceed the height of the patient when seated and the reach of his arm during the rehabilitation process.
The robotic structure should be reliable enough to ensure the repetitive motion of the impaired limb of several patients in clinical or home conditions.
The robotic structure should have a fixed base, independent of the patient reference system to ensure the stability during the rehabilitation process.
The patient can be moved and seated during the rehabilitation procedure using a wheel chair.
Based on calculated anthropomorphic data, the robot should have adjustable elements that would fit with different patient sizes without any influence upon the actual limb motion.
Hazard identification is a crucial step in risk assessment process, because within this stage all the dangerous situations than can occur have to be identified. If a hazard is not taken into consideration it will be also missed in this step in the risk reduction phase.
There are various types of hazards: mechanical, electrical, thermal, noise, vibration, radiation, material, ergonomic, running environment, or a combination of all the above. The identified hazards are presented in the following lines.
Mechanical hazards:
MH1: Arm crushing caused by wrong motion of the spherical mechanism (this hazard can be created by the therapist by introduction wrong parameters not correlated with the patient anthropomorphic characteristics, by wrongly inserting the patient within the rehabilitation system, or it can even be a consequence of a power supply failure).
MH2: Cuts/scratches caused by edges of metal parts (this hazard can be created by improperly design or manufacturing of the mechanical parts of the robotic system).
MH3: Body parts crushing by moving parts of the robotic structure (this hazard can be created by the therapist by introduction wrong parameters not correlated with the patient anthropomorphic characteristics or by wrongly inserting the patient within the rehabilitation system).
MH4: Over limit motion caused by mechanical end-stroke parts malfunction.
MH5: Impact between the robotic structure and patient.
Electrical hazards:
EH1: Risk of electrocution of the patient.
EH2: Risks of harming the patient by sensor system malfunction.
EH3: Over limit motion caused by end-stroke sensor malfunction.
EH4: Risk of short-circuit.
EH5: Risk of overload.
Thermal hazards:
Noise hazards:
Vibration hazards:
Ergonomic hazards:
Risk estimation was carried out in order to find out the severity of each risk. Several methods as risk matrix, risk graph, or numerical scoring are used to estimate the risk. All risks are estimated depending on their severity and probability of occurrence.
The severity of a risk can be numerically estimated as
Catastrophic: 100;
Serious: 90–99;
Moderate: 30–89;
Minor: 0–29.
The probability score can be numerically estimated as
Very likely: 100;
Likely: 70–99;
Unlikely: 30–69;
Remote: 0–29.
The final scoring of each hazard is computed by adding the two values from severity and probability.
In order to estimate the above identified hazards regarding the ASPIRE system 10 design engineers with a background in medical applications were interviewed and asked to fulfill the questionnaire provided in
Appendix A, using
Table A1 to record the severity and
Table A2 to record the probability of the hazard; their scores are displayed in
Table 1 and
Table 2.
In
Table 3 the mean values of recorded data are displayed and the overall score is computed by adding the severity score and the probability score.
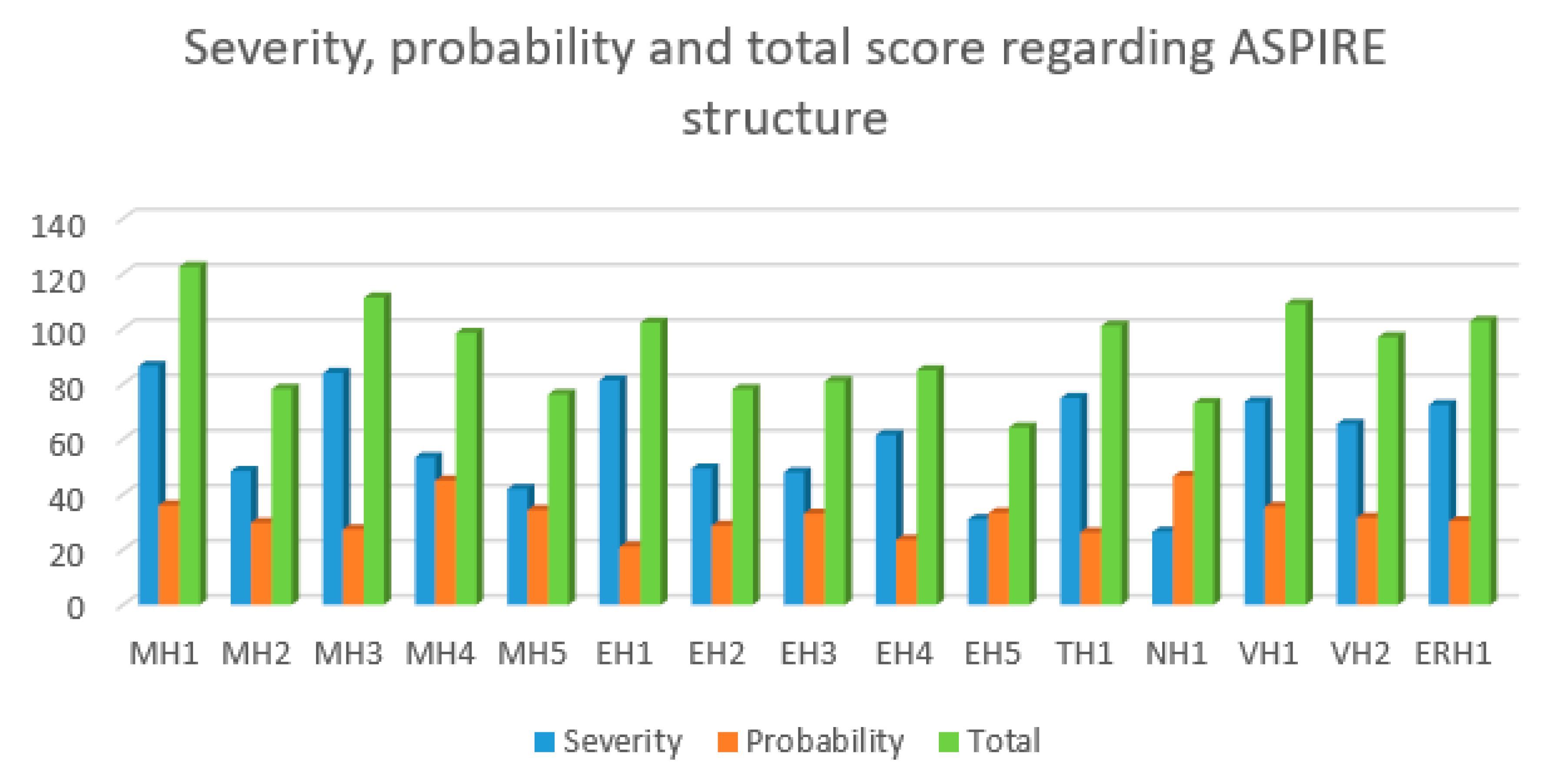
Below, the scores of each identified hazard are graphically represented using bar charts.
The most severe hazard (
Figure 4, blue bar) was identified to be MH1 (arm crushing caused by wrong motion of the spherical mechanism), the highest probability was scored by NH1 (acoustic discomfort caused by close-to-the-ear functioning mechanisms (
Figure 4, orange bar) and the highest overall scorer was MH1 (
Figure 4, green bar).
The risk evaluation process consists of deciding whether a hazard requires risk reduction and to determine whether reduction process has created new hazards or increased the existent risks.
The overall scoring of each identified hazard will be compared with the following evaluation scale:
High: over 151;
Medium: 101–150:
Low 61–100;
Negligible: 0–50.
The risk evaluation is carried on in
Table 4.
The identified hazards that need reduction have to score a medium or high score. A total of six identified hazards (MH1, MH3, EH1, TH1, VH1, and ERH1) scored a medium value the rest of the hazard scoring low values. During the constructive design phase of the ASPIRE system all the identified hazards shall be taken into account, but special care should be paid regarding MH1, MH3, EH1, TH1, VH1, and ERH1.
When developing the risk reduction methods each previously identified hazard was individually analyzed, the outcome of the analysis being presented in
Table 5.
2.3. Failure Mode and Effects Analysis of ASPIRE Robotic System
Another method to identify, reduce, and eliminate risks within a system is Failure Modes and Effects Analysis (FMEA). FMEA is a systematic method for failure analysis developed by reliability engineers [
32], and it implies analyzing as many as possible elements of a system to identify possible failures and the causes and effects of these failures.
The FMEA process for the ASPIRE robotic structure is displayed in
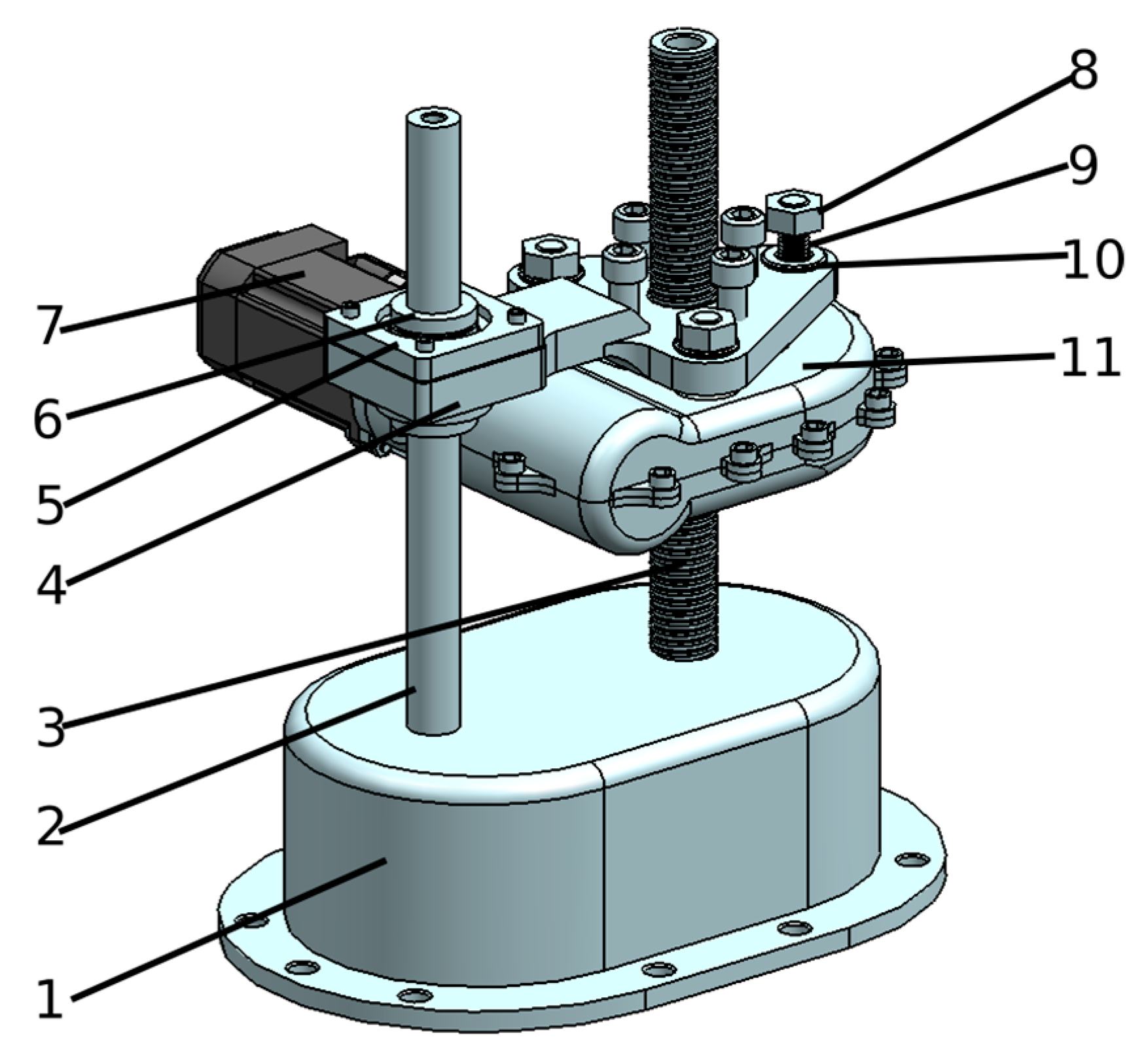
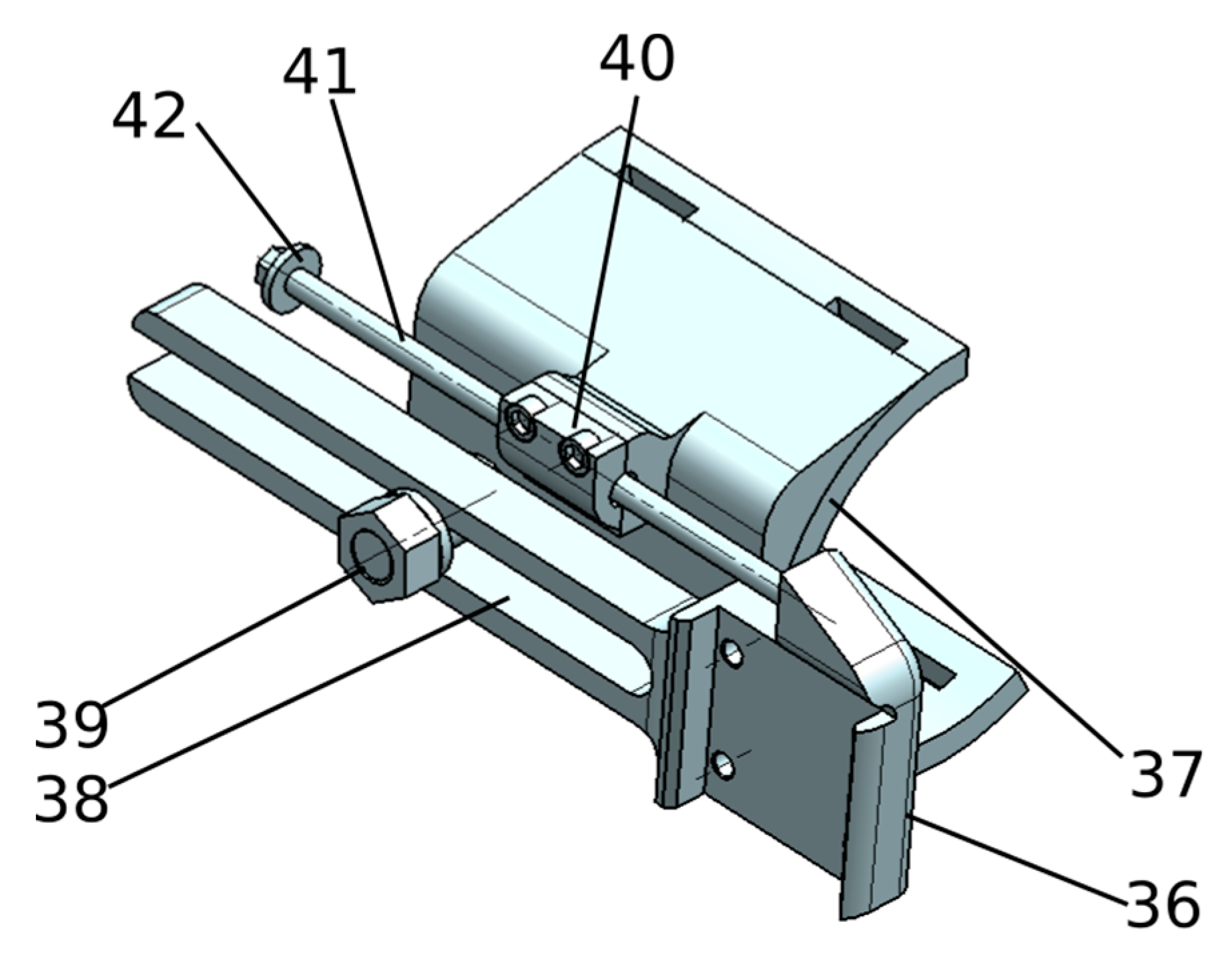
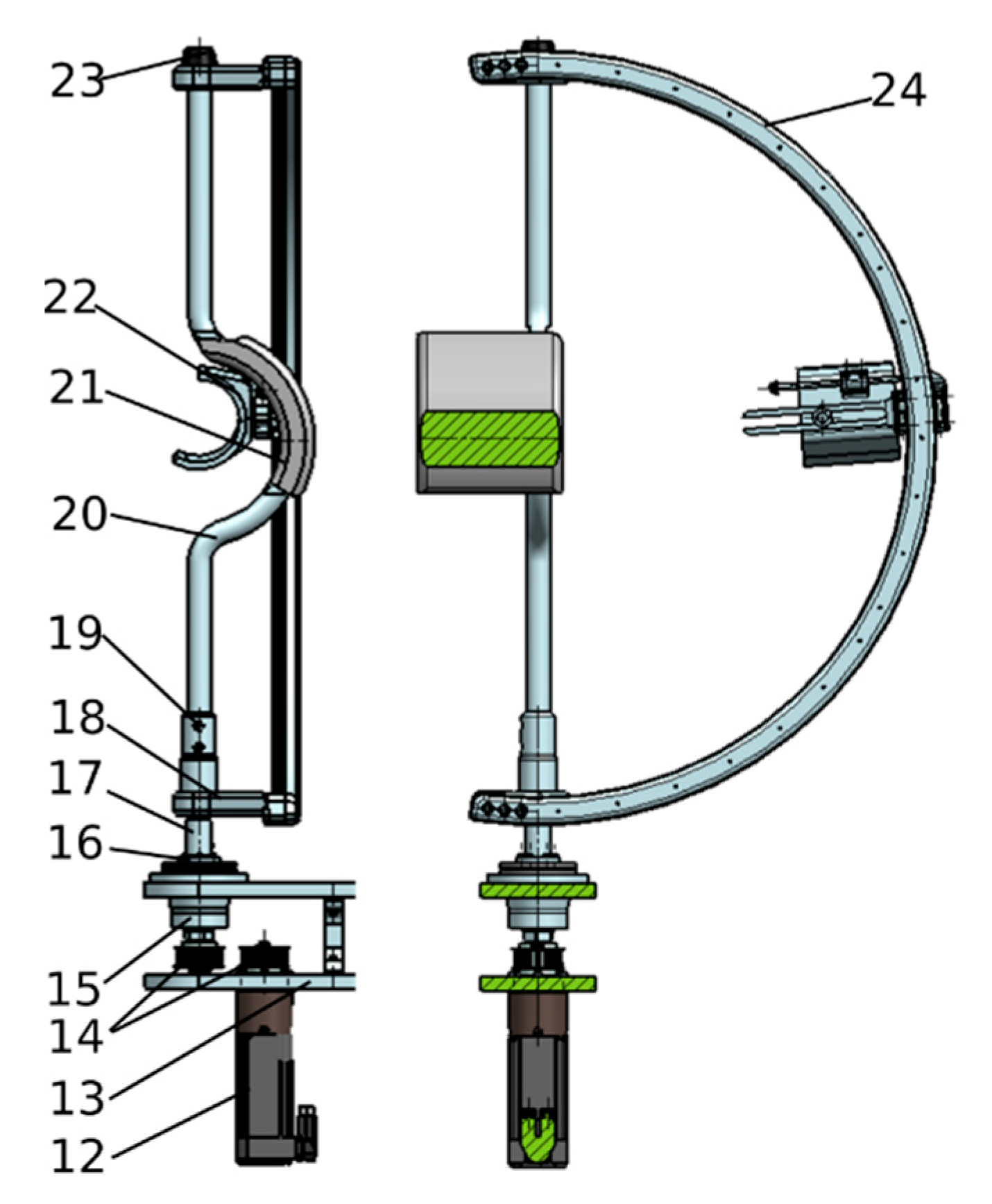
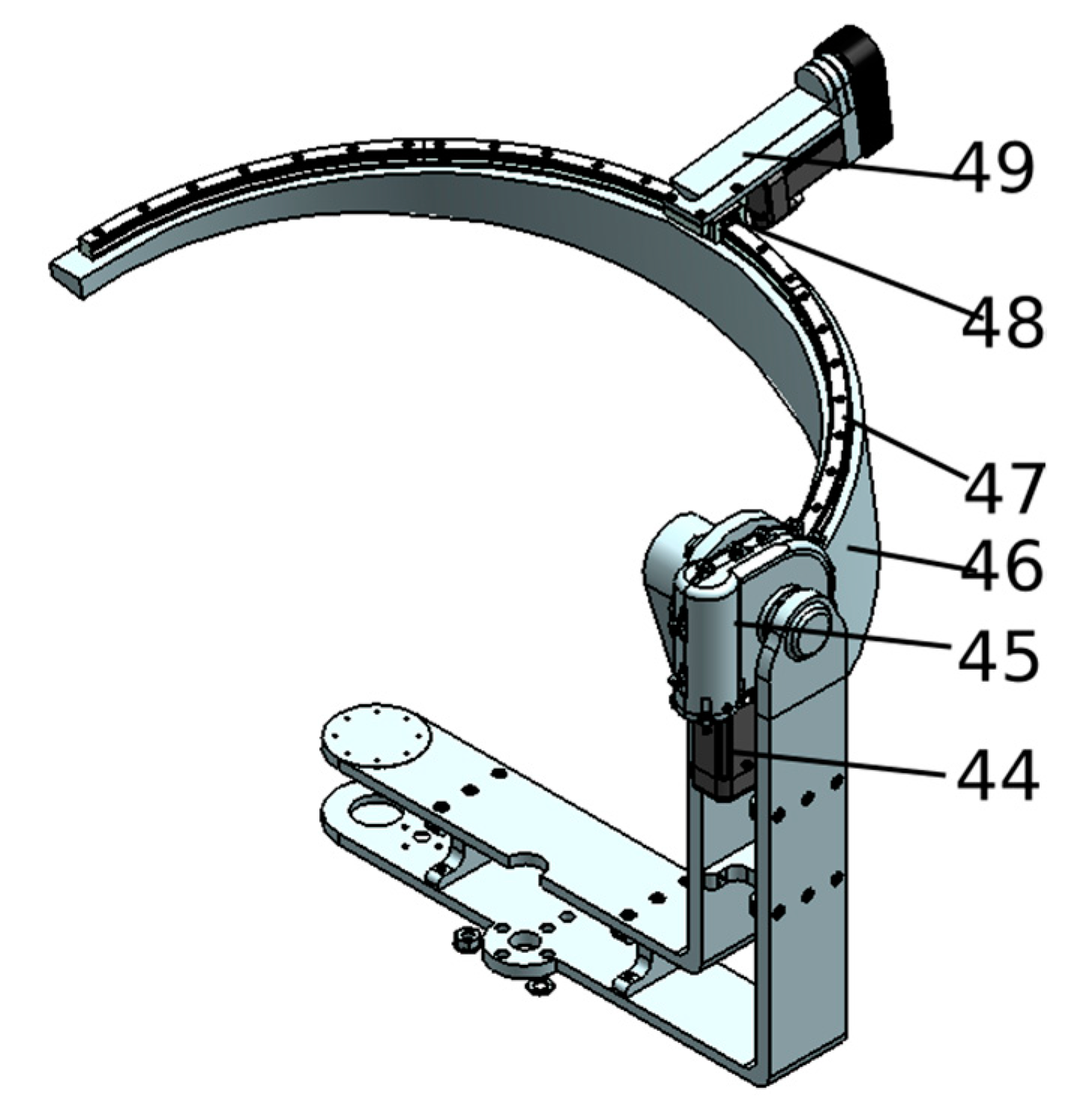
Table 6. To provide a reliable solution for the rehabilitation system all the above failure modes have to be analyzed and embedded in the robotic system during the design stage. To overcome F1, F2, F3, and F4 failure modes, physical end-range limiters should be embedded in the constructive design of the robot to stop the mechanism when the maximum stroke is reached. To prevent F1 and F2 simple screw nut assembly buffers have to be mounted on both circular slides. To prevent F3 and F4, adjustable buffers may be used to modify the stroke of each mechanism based on the patient body type (height, weight, etc.). Each stroke limit should have a double check-up, once by proximity sensors mounted to detect a possible collision, and second by the control system that gives the possibility to impose discreet limits of kinematic axis, making the buffer mechanism to be a supplementary solution in case of F1, F2, F3, or F4 malfunctions.
To overcome F5 and F6 a worm gear is a possible solution. The height adjustment mechanism may be actuated by a servomotor attached to a worm gear reduction box, mechanism that slides along a screw nut assembly. For this mechanism, buffers have to be mounted to avoid end-range collision between the robot’s links (or patient). Proximity sensors are the primary safety system along with the discrete limit of the kinematic axis. To prevent F6 a worm gear reduction could also be used, this time to overcome the possible forces that can occur in the mechanism during the rehabilitation process.
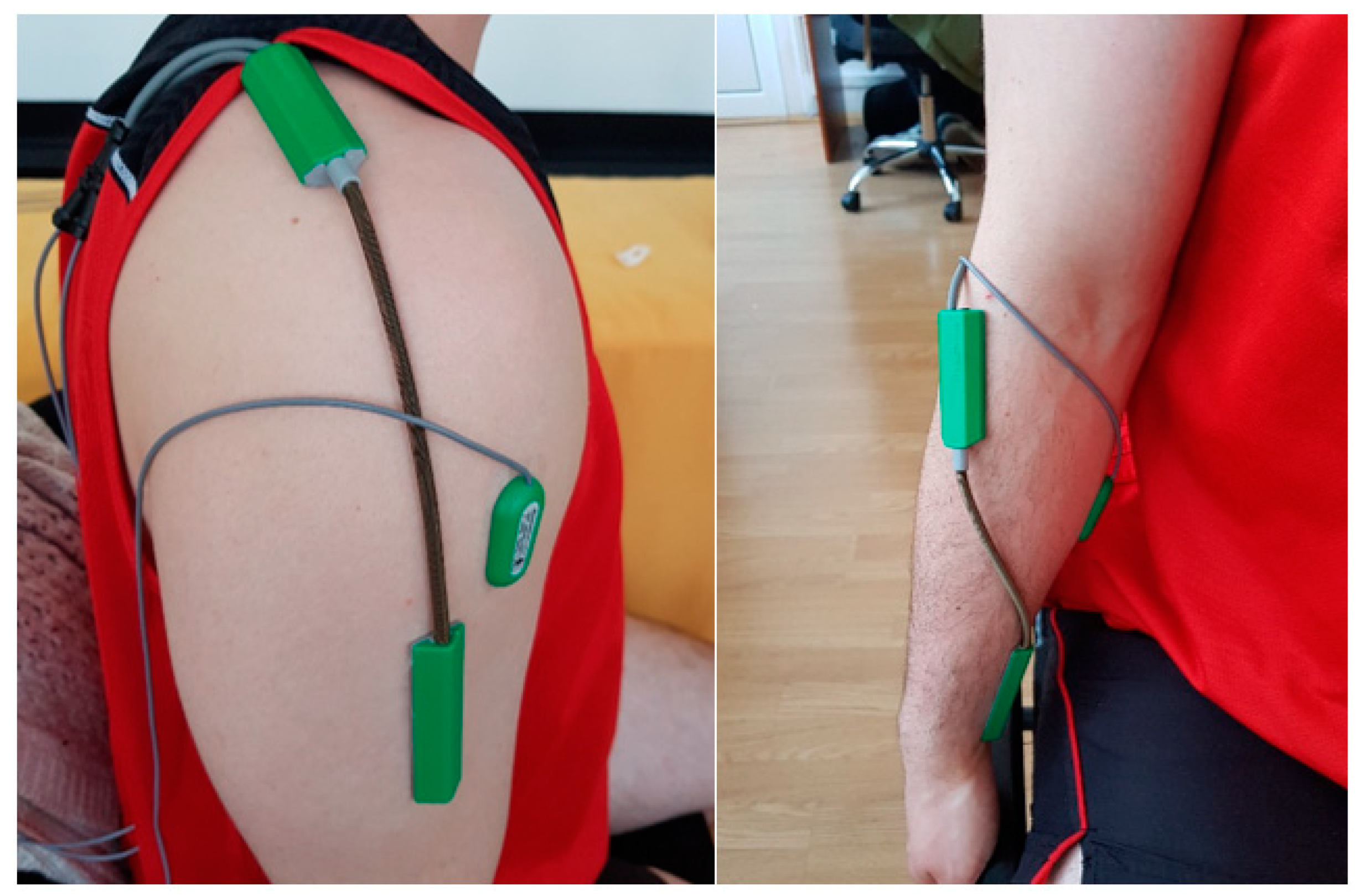
To overcome F7, F8, and F9 an external sensor system may be embedded in the rehabilitation system. Failure F7 can occur when the encoder of the motor is not functioning properly, for this a double check sensor system could be implemented. This sensor system consists of mounting and monitoring goniometers placed on the impaired limb of the patient. Before performing the rehabilitation procedure, the patient is measured by a kinetotherapist and a rehabilitation chart is defined with the maximum range of the patient articulations. Based on these measurements the setup of the robotic structure is defined (end-range buffers and inductive sensors are set to detect the maximum range of each rehabilitated articulation); using the goniometers the joint angular displacement is measured, preventing the system to go over the reachable limit of the patient and in the same time giving the possibility to monitor, register and compare the progress of the patient. To prevent failure F8 a special subprogram could be implemented into the control system to monitor and prevent processor failure.
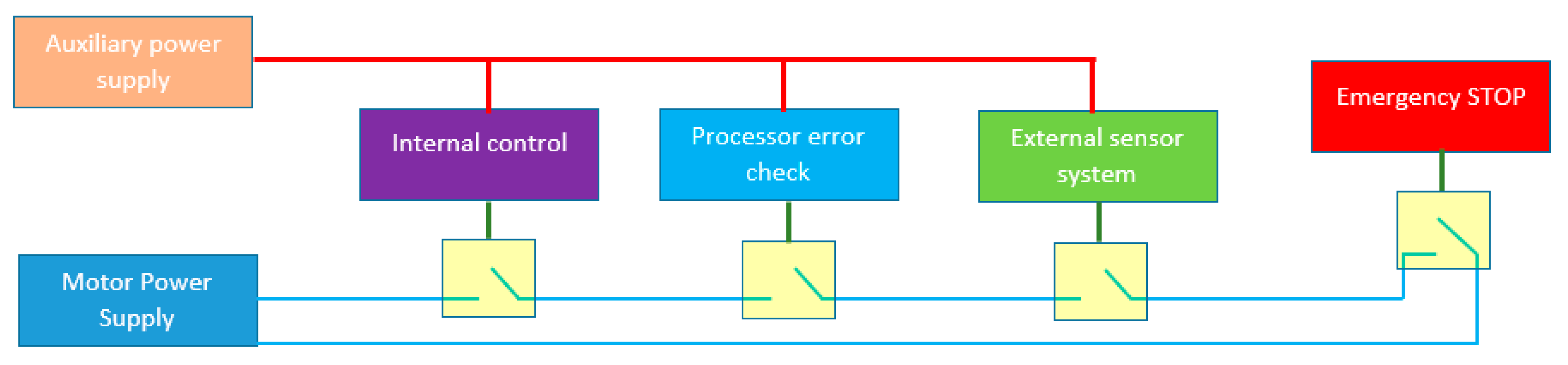
Figure 5 represents a safety loop in the ASPIRE’s controller. The robotic system can be forced to a sudden stop through either one of the following four systems.
ES1: Emergency stop system, manually actuated by the supervising personnel or by the patient (if possible) and gives the possibility to stop the rehabilitation procedure at any time if the supervisor observes some incorrect functioning of the system; following an emergency stop the system has to be reinitialized after the errors in functioning have been identified and eliminated. Correlated with the emergency stop a special procedure to detach the patient from the robotic system should be implemented.
ES2: External sensor system represents the goniometers system mounted on the patient’s arm, monitored by a special, individual processor that communicates with the main controller of the robotic system; any abnormal values or the lack of communication will induce an emergency stop of the system.
ES3: Processor error check system is the subroutine implemented to monitor the errors that can be created by the faulty functioning of the processor.
ES4: Internal control system is the main control module of the robot that can stop the system if some uncontrolled forces are identified, or if the mathematical model of the structure identifies some unreachable zones embedded in the rehabilitation chart.
All these safety systems are able to individually stop the procedure at any time without any confirmation; the safety and health of the patient at risk can be seen in
Table 4.


 and
and 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





















