Sustainable Urban Mobility Policies as a Path to Healthy Cities—The Case Study of LMA, Portugal



Centre for Geographical Studies, Institute of Geography and Spatial Planning, Universidade de Lisboa, Rua Branca Edmée Marques, 1600-276 Lisboa, Portugal
*
Author to whom correspondence should be addressed.
Sustainability 2019, 11(10), 2929; https://0-doi-org.brum.beds.ac.uk/10.3390/su11102929
Submission received: 6 February 2019
/
Revised: 16 May 2019
/
Accepted: 17 May 2019
/
Published: 23 May 2019
(This article belongs to the Special Issue Accessibility and Transportation Equity)
Abstract
:Sustainable development has become the basis of several worldwide policies over the last few decades, and its role will continue to shape policies for decades to come, especially those that are focused on urban mobility. At the same time, urban mobility is included in the framework of the Healthy Cities movement. In this context, using the Lisbon Metropolitan Area (LMA), Portugal, as the study area, this article intends to answer the following research question: are sustainable urban mobility policies contributing to healthy cities? Urban mobility planning and public health instruments were compared with the discourses and practices of those responsible for the implementation of urban mobility policies and Healthy Cities projects. The results reveal that a large number of responses proposed in the mobility planning instruments are, to some extent, related to the principles of healthy cities. Also, while municipal agents tend not to consider the inclusion of those principles, they instead incorporate the concepts of sustainable development. Nevertheless, we found that both approaches overlap the policy directions of healthy cities. On the other hand, public health policies and Healthy Cities projects presented a scarce number of references to its interventions in the urban mobility domain and mainly focused on the promotion of soft modes. It is concluded that, in the case of the observed municipalities of the LMA, the healthy cities framework is greatly benefited by the inclusion of sustainable development principles in all policies, especially those for urban mobility.
1. Introduction
The concept of sustainable development has been a component of policies all around the world for some time. This has been systematically integrated into planning instruments, particularly in the field of urban mobility, generating instruments such as Sustainable Urban Mobility Plans (SUMPs). During the same period, the Healthy Cities movement emerged, extending the concept of health from the absence of disease to a complete physical, mental, and social status of well-being. So, this study intends to understand whether the sustainable urban mobility policies applied in the Lisbon Metropolitan Area (LMA), Portugal, are contributing to healthy cities and, simultaneously, whether the domain of urban mobility is already a concern within public health policies. The intention of this paper is to highlight the potential links between sustainable urban mobility plans and healthy cities while linking academic and political approaches. On one hand, there is already a solid conceptual discussion and empirical evidence of the relationship between urban mobility and transport and health, and it is often tied to sustainable development, which is at the heart of several policies of various sectors from the global to the local level. It is also very important that this relationship is translated into policies, also from the global to the local level, and its instruments, namely, SUMPs, so that these plans can promote real positive impacts and thus maximize their potential in all policies beyond those focused on urban mobility in accordance with intersectoral collaboration principles. This study, using the Lisbon Metropolitan Area (Portugal) as the study area, poses the following research question: are sustainable urban mobility policies contributing to healthy cities? This research question has generated several subsequent questions, such as the following:
- Q1. Are there consistent links between the principles of sustainable development and healthy cities?
- Q2. Could the intervention for sustainable urban mobility contribute to the principles of healthy cities?
- Q3. Are healthy cities principles already evident in the urban mobility planning instruments and in the discourses and practices of the municipal agents in LMA, and is urban mobility a concern in the public health instruments and in discourses and practices of Healthy Cities projects?
These issues have also led to a set of hypotheses to be proven. (h1) Since the principles of sustainable development and healthy cities are promoted by recognized global entities and both oriented toward the quality of life and environmental protection, such concepts present similar directions. (h2) On the one hand, urban mobility is widely accepted as a source of problems and solutions in the context of sustainable development, and on the other hand, its role in the context of healthy cities is also very important, but it is still less explored. (h3) Lastly, considering the two previous hypotheses and the membership of the majority of LMA municipalities in the Portuguese Network of Healthy Municipalities, the principles for healthy cities are already present in the urban mobility planning instruments as well as in the discourses and practices of autarchic agents, and urban mobility is already included in public health policies and Healthy Cities projects.
This paper is divided into six sections. Section 1 presents a brief introduction to the paper. Section 2 is related to the theoretical background of the links between sustainable development and healthy cities, given that they share a common history and that urban mobility plays a role in both paradigms; these commonalities are the foundation of the main research questions and the three hypotheses. Section 3 presents the research methods; this study’s approach is based on the content analysis of two sets of information: (1) urban mobility planning and (2) public health policies and the discourses and practices of competent agents in the urban mobility field and in Healthy Cities projects, particularly from an implementation perspective. Section 4 focuses on the results and discussion. This section distinguishes between two dimensions of the analysis: (1) planning instruments and (2) discourses and practices of municipal agents. The first dimension was studied by comparing instruments in the domain of urban mobility planning and instruments of public health planning, while the second dimension was examined by considering the discourses and practices of urban mobility department teams and Healthy Cities projects teams; both were considered at the municipal level. Section 5 describes the main conclusions. A notable presence of responses favor the integration of healthy cities principles with urban mobility policies and practices, but the presence of the urban mobility domain in public health policies and Healthy Cities projects interventions, although existent, is not so strong. The previous evidence contradicts the discourses of municipal agents; the partnerships between urban mobility departments and Healthy Cities projects and the recognition of the link between urban mobility and healthy cities by both teams are scarce or even non-existent. This reason for this contradiction is that the bottom–up approach proposed by the Healthy Cities movement is minimized by the top–down approach associated with sustainable development through the obligations of European and National entities (e.g., European Commission, national government) to include the respective guidelines in all policies. Lastly, Section 6 lists the main lessons for researchers and decision makers and highlights the need to reinforce the contribution of science to urban planning policies and practices.
2. Theoretical Background
The discussion on sustainability is not recent, and translational research has been extremely important in reinforcing the role of academia in planning policy and practice [1]. In this context, we highlight the study of the interaction between urban mobility and health and its contribution to sustainability. This relationship is complex because of its intersectoral nature [2,3,4,5], and it is relevant to the search for strategies and tools that enable monitoring sustainability practices in the short and long term, thus producing supporting information for more consistent decision making [5,6,7]. Within the framework of sustainability, particularly in an urban context, some concepts have emerged and triggered several planning movements that, in turn, have proposed frameworks for policies and monitoring tools.
2.1. Relationship between Sustainable Development and Healthy Cities
Several movements in the context of sustainability involve urban mobility and health issues, with particular emphasis on sustainable development and the Healthy Cities movements, which are further analyzed in this paper. For example, the movements of Smart Growth and New Urbanism, which present similar principles, promote compact urban forms and mixed land uses, strong neighborhood networks and a sense of community, soft modes for local travel, and the implementation of effective collective transport networks for extended journeys [7].
Other approaches with a city-level scope have also emerged. For example, the urban form and transport are the core of the “eco-city” model, in which high urban density is linked to a high-quality public transport system and walking and cycling infrastructures to minimize the dependence on cars [8]. Considering the key characteristics and driving factors of eco-cities, several assessment tools have been investigated on the basis of indicator systems [3,4].
Another example is the concept of “Resilient Cities”. This can be seen as “the ability to absorb, adapt, and respond to changes in an urban system” [5] (p. 89). Since resilience is an abstract concept, as sustainability is, it is necessary to define these cities’ main components—resources, processes, people, institutions, and activities, as well as the interactions among them—in order to evaluate them. In this case, monitoring these phenomena is very useful for urban planning but also a challenge to the decision support systems that exist today [9,10].
Locally, “sustainable communities” and “eco-neighborhoods” have arisen [2]; they are usually defined as “communities that meet the diverse needs of existing and future residents, their children, and other users, contribute to a high quality of life, and provide opportunity and choice. They achieve this in ways that make effective use of natural resources, enhance the environment, promote social cohesion and inclusion, and strengthen economic prosperity” [6] (p. 279). The approach to sustainable communities assumes the need for action in several fields, of which transportation and mobility and also health are fundamental pillars because of their inherent importance and their influence on the remaining pillars. In this context, the importance of monitoring the various phenomena that form a sustainable community has been debated by academics and politicians and underlies the purpose of many practices [2,6]. The two referenced urban movements—sustainable development and healthy cities—have a common history. Both originated at the United Nations Conference on the Human Environment of 1972, which was known as the Stockholm Conference, and recognized the importance of the balance between the environment and the economy. Thus, there is a great deal of similarity in the definitions and principles that guide them.
Following the Stockholm Conference (1972), the World Commission on Environment and Development (WCED) was set up in 1983. After four years, the Brundtland Report (1987) was drawn up as the new declaration for environmental protection; it was titled “Our Common Future”. It was in this report that the concept of sustainable development was used for the first time to describe a society “that meets the needs of the current generation without compromising the needs of future generations (...) balancing the binomial between local and global needs, between the present and the future, and between economic growth and social equity” [11] (p. 43). In this context, transport was already understood to be a source of environmental problems, a consumer of fossil fuels, and a source of air pollution that is harmful to the environment and health but, at the same time, the means of fulfilling the needs of the population, namely, the need to access goods and services and reinforce social inclusion [12]. Other important events followed, such as the United Nations Conference on Environment and Development (1992)—also known as the Rio de Janeiro Conference—from which Agenda 21 emerged as an action program to attend to environmental development, and the World Summit on Sustainable Development (2002). Despite the goals and targets defined so far at national, European, and global levels, Banister [13] emphasized that sustainable development is not intended to be only a goal, but rather a direction.
The Healthy Cities movement also emerged from a succession of events that occurred after the Stockholm Conference (1972), and its development was bolstered by the evolution of the framework for public health policies. These events include the Declaration of Alma-Ata that resulted from the International Conference on Primary Health Care (USSR, 1978), which emphasized a new perspective on health not only as the absence of disease, but also as the complete physical, mental, and social status of well-being, thus requiring the attention of various sectors beyond the health sector. In 1980, the “European Health for All Strategy” was published, and five years later, it was presented as the “European Targets for Health for All Strategy”, which included 38 targets organized by themes such as “Health for all in Europe by the year 2000”, “Lifestyles”, “Healthy environment”, “Appropriate care”, “Research for health for all”, and “Health development support”. The Ottawa Charter for Health Promotion was signed in 1986, which was an important moment in the debate on public health, as it related policies and agents, lifestyle, and the social environment of individuals. In this document, there was a paradigm shift related to health promotion from the hitherto focus on risk factors or individual behaviors to an approach that considers the various determinants of health. Health was also defined as “a resource for everyday life and not a life goal (...)”, while health promotion has emerged as “the process of empowering people to increase their control and improve their health” [14] (pp. 383–384). In 1987, the World Health Organization (WHO) launched one of the most popular initiatives, the Healthy Cities project, whose objective is to include health and health determinants in all policies. This should be implemented by the municipality members of Healthy Cities National Networks through innovative actions and principles, such as explicit political commitments, leadership, institutional change, and intersectoral partnerships [15]. This was followed by other documents, such as the “Jakarta Declaration on Leading Health Promotion into the 21st Century” from the Fourth International Conference on Health Promotion (1997) [16] and “Health 21: the health for all policy framework for the WHO European Region” (1998) [17]. Also, in this context, it is stressed that a healthy city is a process and not an outcome or a particular health status, which is a concept that aligns with the European policy framework Health 2020 and the 2030 Agenda for Sustainable Development [15]. Thus, we can assume that, in addition to their common historical roots, other factors of these two urban movements are deeply related.
The definitions of sustainable cities and healthy cities and the principles that drive them reveal common points that prove their symbiotic relationship (Table 1). Four key points stand out: (1) the multi-temporal perspective, which simultaneously considers interventions and results in the short term and the long term, the present and the future, and this generation and the next ones; (2) the multi-sectoral perspective, which highlights that sustainable cities require relationships among several sectors in the environmental, economic, and social domains, while the emphasis of healthy cities is the various determinants of health that arise from aspects such as individual behaviors and lifestyles, employment, housing, the social environment, and so on; (3) the multi-level perspective, which, similar to the context of sustainable development, raises the level of local initiatives, such as sustainable communities or neighborhoods, to the global scale, whereas the Healthy Cities movement intends to exert its effects starting from the individual level, then moving to the community level, until finally reaching the global or ecosystem level; and, lastly, (4) the common view that neither approach is focused on achieving specific goals but rather on the realization of a continuous improvement process applied to cities and the quality of life of their inhabitants.
2.2. The Complex Network of Problems of Sustainable Urban Mobility and Its Consequences for Healthy Cities
Urban mobility has been present in many urbanistic movements, namely in the context of sustainable development and Healthy Cities movements. At the same time, cities are at the center of the debate due to the high concentration of people and activities, the high resource consumption, and environmental degradation, among other problems [22,23], thus taking a prominent place toward sustainable and healthy cities.
Sustainable mobility is defined as “the ability to meet the needs of society to move freely, gain access, communicate, trade, and establish relationships without sacrificing other essential human or ecological values today or in the future” [24]. In other words, the concept of sustainable mobility assumes that all citizens can choose accessibility and mobility options that are safe, comfortable, timely, and affordable, and that simultaneously contribute to environmental protection by having high levels of energy efficiency and reduced environmental impacts [25].
The high importance of urban mobility for sustainability is proportional to the large number of problems that it entails. Its complexity is even greater when it is realized that the solution to one problem can cause new problems or amplify existing ones [12,26,27]. For example, the reduction in transport intensity should be achieved simultaneously with economic growth, thereby associating these trends of both components. On the other hand, Holden [12] pointed out the difficulty dissociating the positive and the negative impacts of transport, since the elimination of negative impacts may threaten the positive ones, as the author assumed that transport is probably the most problematic issue for sustainable development after poverty eradication.
In an attempt to systematize the main problems of sustainable urban mobility and its consequences for healthy cities, three sets of references were taken into account: (a) references about the link between transport and urban mobility and its sustainability or unsustainability [13,28,29,30,31,32,33]; (b) references that relate transport or urban planning and healthy cities and, more broadly, health, [34,35,36,37,38,39]; and (c) broad references about transport geography or urban geography [23,26,40,41]. The results of this review are depicted in Table 2 and led to the conclusions that (1) one problem can simultaneously participate in the environmental, economic, and/or social domains for sustainable development, and (2) the same problem can have several consequences for healthy cities.
Thus, the most cited problems in the literature were organized into four large groups. The first group brings together problems from individual behaviors, including road accidents [13,23,28,41], driving-related crime [42,43,44], the excessive motorization of transport due to individual modes [13,26], poor adherence to active transport modes [45,46], and, finally, the negative perception of transport, particularly the active modes [33,40,47,48,49]. The second set of problems refers to the infrastructural and investment constraints that cause problems such as inaccessibility to transport and goods and services [33,50], the high cost of transport and urban adaptations [26,28,33], and congestion [12,13,23,40]. The third group of problems is related to territorial occupation, which highlights problems associated with inappropriate urban forms at the local level [51,52] and land uses that have a single function and are dispersed at the regional/metropolitan level [26,40,53]. Finally, the fourth group includes mainly environmental problems, namely, increased soil sealing in urban areas [26], excessive fossil fuel consumption and energy dependence [13,28,54], extreme carbon emissions [13,34], and noise and air pollution [23,26,28].
In turn, as Table 1 shows, there are many consequences that are contrary to the principles of healthy cities, and they can be organized into four main areas: (a) the social area, with consequences such as social exclusion [12,13,23,28], lack of social interaction [55,56], a reduced sense of community [46,56,57], difficulties of physical mobility [28,46,58], and the lack of moderate and strong physical activity [34,35,37,38,59]; (b) the health area encompasses consequences in the form of a great variety of diseases, such as respiratory diseases [26,60,61], cardiovascular diseases [26,60,61], neurological diseases [26,28,61], oncological diseases [34,43], behavioral and psychological disorders [28,34], obesity and being overweight [34,35,37,59], physical and psychological damages [34], and, finally, effects on mortality rates [60]; (c) from the economic area emerges the loss of local amenities, infrastructure, and material costs [28,34], fuel costs [13,28], time costs [28,33], and medical and insurance costs [28,34,37]; (d) finally, in the environmental area, the apparent consequences include the decline in green spaces and open spaces [23], floods [28,31], water and soil contamination [26], islands of urban heat [60,61], and global warming [13,23,28,62].
2.3. Main Intervention Axes in Sustainable Urban Mobility for Healthy Cities
Beyond the previous references addressing the main problems of sustainable urban mobility and the wide range of consequences for healthy cities, since the late 1980s, many academic and policy documents have highlighted the importance of acting in this context. One main source is the World Health Organization, European Region Office for Europe (WHO-Europe), and its various reports that directly address issues such as urban planning for health and healthy cities [39,63] or the relationship between health, transport, and physical activity [64,65,66,67,68,69]. Many others have worked on this subject as well, with focuses such as the healthy city concept as it relates to European policy orientations [57], the links between health and the urban environment [70,71,72], or the relationship between health and urban mobility and transport, with special attention to active travel [73,74,75,76,77,78].
The previous literature review resulted in the identification of 13 intervention axes in sustainable urban mobility for healthy cities, as presented in Table 3. Intervention axis 1, “Healthy and clean behaviors in transport”, promotes, for instance, safe driving behaviors by individuals free from the harmful effects of tobacco, alcohol, and drugs. Axis 2, “Integrated transport information supported by Information and Communication Technology (ICT)”, includes initiatives that provide real-time information about routes and schedules or about support infrastructures such as parking, electric vehicle loading, or bikesharing. Axis 3, “Inclusive, safe, and barrier-free transport systems”, highlights initiatives to make the system more inclusive (e.g., level crossing and walking), safer (e.g., lane separation, protection of bicycle lanes), and free of barriers (e.g., intervention in route junctions). Axis 4, “Transport speed”, is linked to the creation of public transport lines (priority or exclusive routes) or areas of reduced flow and the speed of motorized modes. Axis 5, “Networks, intermodality, and connectivity” includes the promotion of transit-oriented development (TOD), the improvement or extension of public transport networks, and the improvement of stations and stops by developing better sidewalks, parking, taxi points, bicycle parking, and public toilets, among other amenities. Axis 6, “Infrastructures for active modes”, considers measures to promote bicycle-friendly cities (e.g., the creation of bicycle lanes and support infrastructures), pedestrian-friendly city (e.g., safe and accessible routes and support equipment), attractive and comfortable environments for active mobility (e.g., shade areas, shelters), and good connectivity with the public transport network. Axis 7, “Transport electrification”, arises from the need for energy independence in transport. Axis 8, “Land-use planning”, brings together actions related to sustainable urban models anchored in the principles of mixed land use, higher population densities, and the activities and optimal locations of transport. Axis 9, “Data collection”, refers to the identification and/or creation of indicators to support diagnosis and evaluations by considering, for example, real-time and open-access information using digital tools (Global Positioning System (GPS), apps), in which case, the transport user is also the information producer. Axis 10, “Legislation”, frames the legislative measures that cover all users and all transportation modes. Axis 11, “Agents and Competencies”, reflects the initiatives that promote partnerships between funders, managers, and beneficiaries; multi-level, multi-agent, and multi-sector partnerships; and urban mobility in all policies. Axis 12, “Instruments and studies”, includes initiatives related to sustainable urban mobility plans or similar, school or business mobility plans, road safety plans, and other tools, such as the Health Impact Assessment (HIA) and Health Economic Assessment Tool (HEAT). Finally, axis 13, “Awareness of benefits for health, environment, and economy sectors”, combines actions associated with active mobility, road safety education, and initiatives to communicate strategies and plans related to this subject to the whole community.
3. Research Methods
The present study covers the Lisbon Metropolitan Area, Portugal, and its municipalities (Figure 1). The intention of this paper is to understand if sustainable urban mobility policies at the municipal and metropolitan levels contribute to healthy cities while combining the analysis of two dimensions—“Planning instruments” and “Discourses and practices”—using the perspectives of municipal competent agents in the fields of urban mobility and public health (where the Healthy Cities projects take place) at municipal level (Figure 2).
In this context, the research methods are organized into the following stages:
- 1.
- Definition of the aim of the research and associated research questions;
- 2.
- Literature review that focuses on sustainable urban mobility and respective links to the principles for healthy cities using a wide variety of sources: academic papers and theses, policy documents at various levels, technical reports, and case studies;
- 3.
- Dimension 1, “Planning instruments”—Inventory and content analysis of urban mobility and public health planning instruments, using the software NVivo 11 (more information about the software in Appendix C) for the following steps:
- First step: Qualitative data upload in the analysis context software;
- Second step: Content coding using node or descriptor systems (funded by stage two and iteratively tested);
- Third step: Analysis of the outcomes by descriptor.
Content analysis in the urban mobility domain included reviewing documents with several territorial levels: metropolitan (LMA), intermunicipal (South LMA, a document that covers the municipalities of Barreiro, Moita, Palmela, Seixal, and Sesimbra), municipal (cases of Almada, Cascais, Lisbon, Loures, Oeiras, and Setúbal), and local, which involved the parishes of the municipalities Mafra and V.F. Xira. In the public health domain, similar to the urban mobility analysis, a multi-level approach was considered for document selection: the National Health Plan and Priority health programs at the national level, the Regional Health Plan and Regional Health Profile at the regional level, and Local Health Plans, the Municipal Health Profile, and the Health Development Plan at the municipal/local level.
- 4.
- Dimension 2, “Discourses and practices of municipal agents”—Interviews with municipal agents with competencies in urban mobility and Healthy Cities projects were conducted through a structured interview script (Appendix A and Appendix B) and analyzed using NVivo 11 with the following steps:
- First step: Interview transcription upload to the analysis context software (one Microsoft Word file per interview);
- Second step: Content coding using node or descriptor systems, where each descriptor is a discussed topic (e.g., major urban changes, municipal resources, etc.);
- Third step: Analysis of the outcomes by descriptor.
The interviews with urban mobility agents were carried out in eight of the 18 LMA municipalities—Cascais, Lisbon, Loures, Moita, Odivelas, Oeiras, Seixal, and Setúbal—during the spring of 2017. The eight municipalities represent 57% of the LMA’s resident population and 27% of the LMA’s surface area [79]. The interviews with Healthy Cities project agents were carried out in six of the 18 LMA municipalities—Amadora, Cascais, Loures, Odivelas, Oeiras, and Seixal—during the spring of 2017. The six municipalities represent 38% of the LMA’s resident population and 15% of the LMA’s surface area [79].
In each studied municipality, a unique and collective interview was carried out with a group of political and/or technical experts with competencies in each theme. The interviewees were appointed by the president of each city hall.
- 5.
- Discussion of the results following the presented dimensions in Figure 2: (1) “Urban mobility for healthy cities: An approach to planning instruments in LMA” is composed of two subdimensions—urban mobility planning instruments and public health planning instruments; (2) “Practices and discourses about urban mobility for healthy cities in LMA” also comprises two subdimensions—the perspective of municipal agents who are competent in urban mobility, and municipal agents related to Healthy Cities projects;
- 6.
- Identification of the main conclusions drawn from this case study and a summary of the main lessons that can be used in the future by researchers and decision makers.
4. Results and Discussion
4.1. Urban Mobility for Healthy Cities: An Approach to Planning Instruments in LMA
4.1.1. Urban Mobility Planning and Management Instruments in LMA
Highlighting again the importance of urban mobility planning tools [80], the team carried out an exhaustive search of the existing documents in the context of the LMA and its municipalities, especially documents that have been developed since the beginning of the 2000s. This review culminated in the categorization of these documents into three main groups: urban mobility plans and similar, studies and technical documents, and chapters of other urban planning documents. In this context, 10 documents were selected for deeper analysis using two criteria: a multi-level criterion that considers documents focused on local, municipal, inter-municipal, and metropolitan levels; and a diversity criterion that is based on the typology of documents (Table 4).
Several methodological steps were followed to systematize the information for content analysis (Section 3). Thus, all the items from the intervention component of each document were listed. In this context, because of the variety of documents, the items also presented several typologies: measures or projects (LMA, South LMA, Oeiras, Almada, Mafra), actions (Lisbon, Loures), and intervention lines (Setúbal, VF Xira, and Cascais) (each measure, action, or intervention line was considered an item). This led to the identification of a total of 1041 items to be introduced into the NVivo 11 software for later coding. The applied coding system was based on Table 3, i.e., the various intervention axes in sustainable urban mobility for healthy cities, with each intervention axis regarded as a coding descriptor. Each item could be encoded by one or more descriptors. In this sense, counting was done on the basis of the simple frequency of the descriptors for each analyzed document. From this process arose Figure 3, which reflects the different patterns of the main intervention axes among the documents, with each document influenced by its typology and the needs of the respective territory and community.
Thus, while some intervention axes have a significant presence (such as axis 3, “Inclusive, safe and barrier-free transport system”, and axis 6, “Infrastructures for active modes”), others show little or no presence in the studied documents (e.g., axis 1, “Healthy and clean behaviors in transport”; axis 7, “Transport electrification”; and axis 9, “Data collection”).
Axis 2, “Integrated transport information supported by ICT”, is present in most of the analyzed documents, albeit in small proportions. However, it registers a wide range of measures or initiatives, including the availability of the public transport system and its characteristics through the online Transporlis Platform (LMA, South LMA, Cascais), the dissemination of network diagrams, schedules, prices, and real-time changes in the network (LMA, South LMA, Setúbal, Oeiras, V.F. Xira, Cascais), advertising campaigns about the service offered (Setúbal), the provision of the enclosures of the interfaces (South LMA), information about transport by bicycles on trains (Setúbal), the creation of mobility stores (LMA, South LMA, Setúbal, Cascais), brand development for public transport companies (Mafra), and the creation of parking management tools (LMA).
Axis 3, “Inclusive, safe, and barrier-free transport system”, is present in almost all the documents as well, being relevant for three of the documents (Lisboa, Loures, and V.F. Xira) and representing more than one-third of the total codifications. Some initiatives are highlighted: the creation of reserved parking (Setúbal, V.F. Xira, Cascais, Lisboa, and Loures), intervention in stops and its surroundings (LMA, South LMA, Lisboa, Loures, V.F. Xira), the creation of accessible pedestrian routes (LMA, South LMA, Lisboa, V.F. Xira), the promotion of adapted vehicles and adapted taxis (Cascais, Loures, Lisboa, V.F. Xira), pavement repair and the elimination of architectural and urban barriers (Lisboa, V.F. Xira), the adaptation of walkways for greater visibility (Lisboa, V.F. Xira, Mafra), the development of an intermodal system at tariff, ticketing, and interface levels (LMA, South LMA, Setúbal), and the management of illegal parking (South LMA, Setúbal, Oeiras, Lisboa, V.F. Xira).
Axis 4, “Transport speed”, is especially present in Oeiras and Cascais documents (and present to a lesser degree in five more documents), and is materialized in actions that include studies and the implementation of fast lines or priority routes in new or existing public transport systems (LMA, South LMA, Oeiras, Cascais), the implementation of traffic-calming measures (LMA, South LMA, Oeiras, Cascais, Lisboa, Almada, Mafra), and the management of heavy vehicle flows (Setúbal, Cascais).
Axis 5, “Networks, intermodality, and connectivity”, is quite relevant in three of the seven documents that have one or more actions in this axis. Here, the highlighted initiatives are those that promote transit-oriented development, increase and qualify transport networks and flexible transport through studies and posterior implementations (LMA, South LMA, Setúbal, Cascais, Oeiras, Mafra), actions to improve connectivity to transport stations, stops, and respective amenities for transport sharing or soft modes of transport (LMA, South LMA, Setúbal), and the creation of parking lots at interfaces and stations (LMA, Cascais).
Axis 6, “Infrastructures for active modes”, is present in almost all the documents (nine of 10), representing more than two-thirds of the total codifications in some cases (LMA, South LMA, Almada, Mafra) and about one-third in other documents (Setúbal, Oeiras, and Cascais). Although a large proportion of these initiatives fall within the qualification of the road network action, several other initiatives are mentioned: the improvement of bicycle lanes (LMA, South LMA, Setúbal, Oeiras, Cascais, Lisboa, Almada, Mafra) and support for bicycle infrastructure (parking, workshops, drinking fountains, and air pumps) (LMA, South LMA, Setúbal, Cascais, Mafra), the implementation of bikesharing systems (LMA, South LMA, Setúbal, Cascais), information availability about bicycle use, infrastructure, and services (South LMA, Cascais), the qualification and expansion of the pedestrian network through reprofiling, extension or new construction (LMA, South LMA, Setúbal, V.F. Xira, Cascais, Lisboa), implementation of the Pedibus Project (South LMA, Cascais), studies about pedestrian crossings and their quality (Lisboa), road network qualification (LMA, South LMA, Setúbal, Oeiras, Cascais, Almada, Mafra), and, finally, the resolution of small road constraints (LMA, Setúbal, Oeiras, Lisboa, V.F. Xira, and Almada).
Axis 8, “Land-use planning”, is found in seven documents (LMA, South LMA, Oeiras, Cascais, Lisboa, Setúbal, and Mafra), particularly aiming to consolidate the urban network, contain the urban perimeter (Setúbal, Oeiras, Cascais and Mafra), and choose the location of collective equipment pieces (Setúbal and Oeiras).
Axis 11, “Agents and competencies”, is present in seven documents and is quite relevant in Oeiras, Cascais, and Setúbal, with references to partnerships between the private and public sector through training actions, including specific training for technicians on accessibility and inclusive urban design (Lisboa), or the involvement between local government and external agents through, for example, inter-municipal mobility agreements or municipal mobility councils (Setúbal, Lisboa).
Axis 12, “Instruments and studies”, is highlighted in documents for South LMA, Cascais, and Lisboa and expressed to a lesser extent in another four documents; it aggregates initiatives related to the elaboration of municipal and metropolitan sustainable mobility plans (LMA, South LMA), mobility plans for companies and schools (South LMA, Setúbal, Oeiras, Cascais), municipal and inter-municipal road safety plans (LMA, South LMA, Setúbal, Oeiras, Cascais, and Lisbon), plans and studies for the implementation or adaptation of soft transport modes, accessibility plans, and accessibility for all plans (Cascais and Lisboa), and pedestrian and cycling plans (South LMA). Some measures that were referred to in the literature, such as the Health Impact Assessment and the Health Economic Assessment Tool (HEAT), are non-existent in all the documents studied.
Finally, intervention axis 13, “Awareness of benefits for health, environment, and economy”, is substantially highlighted in the Loures document, in which it represents about 40% of the total codifications, and the Setúbal, Oeiras, and Cascais documents, in which it accounts for around 10% (being present to a smaller extent in three more documents). In this context, some actions are highlighted such as campaigns to promote the benefits of an active and non-motorized mobility (LMA, South LMA, Setúbal, Oeiras, Cascais, Lisboa, Loures), educational campaigns about road safety (Setúbal, Oeiras, Cascais), and the communication of strategies and plans about soft mobility (Cascais and Loures).
As previously mentioned, some intervention axes in the context of sustainable urban mobility for healthy cities are rare or absent in the context of the intervention defined in the 10 documents previously analyzed. This is the case for axis 1, “Healthy and clean behaviors in transport”; axis 7, “Transport electrification”; and axis 9, “Data collection”. Thus, these points were deeply studied in order to confirm the existence of any performance by local authorities or other entities.
In the case of axis 1, “Healthy and clean behaviors in transport”, the lack of proposed actions in the studied documents contrasts with the existence of prevention and inspection actions and adequate national legislation. In the area of smoking, there is a legal framework that promotes the health protection of nonsmokers in public transport e.g., Decree-Law no. 200/91 of May 29 [81] and Law no. 22/82 of 27 August, which creates the Prevention of Smoking Council [82]; Law no. 37/2007 of 14 August [83], which approved norms for citizen protection against involuntary exposure to tobacco smoke; and Law no. 63/2017 of 3 August [84], which established a smoking ban in various places, including public transportation. Such legislation is in line with Article 8 of the WHO Framework Convention on Tobacco Control (2005) [85]. At the prevention level, there are initiatives such as the campaigns “I smoke, you smoke” coordinated by the National Health Service and the National Directorate-General of Health, “Cigarettes Zero” in the Seixal municipality, and “Cars without smoke” coordinated by the Portuguese League against Cancer and the Automobile Club of Portugal. Alcohol dependence and driving is also a constant theme that is implemented. For example, Law no. 18/2007 of 17 May approved the Supervisory Regulation on Driving Control under the Influence of Alcohol or Psychotropic Substances, which assigns the supervision of this situation to traffic police divisions. The literature also references awareness campaigns, such as “Enjoy driving without alcohol” coordinated by Brisa (a transport infrastructure operator), Sagres (a beverage company), Galp (an energy company), and Portuguese Road Prevention (a nonprofit association) (2017), in response to the high level of blood alcohol content found in drivers and pedestrians involved in road accidents.
There are several municipal initiatives that fall under axis 7, “Transport electrification”. The first one is the modernization of municipal fleets. For example, the Lisbon municipality reduced the light passenger fleet and replaced fossil fuel vehicles with electric or natural gas vehicles. The municipalities of Cascais and Seixal modernized the fleet of urban cleaning vehicles by opting for electric vehicles, with the intention of reducing fuel consumption and carbon emissions. Also, the modernization of public transport fleets has been evident. For example, a protocol signed by the Lisbon municipality, Antral (National Association of Road Transport in Light Automobiles), and the Portuguese Taxi Federation (2013) promoted the renewal of Lisbon’s taxi fleet because of the aging of the vehicles. Some public passenger transport companies have renewed their fleet with vehicles powered by natural gas or electricity (Lisbon, Barreiro, and Cascais). Also, in this context, carsharing initiatives have been supported using electric vehicles (Lisbon and Cascais).
Axis 9, “Data collection”, although not explicitly stated as an action in the documents under study, exists in the form of the component “Monitoring and evaluation indicators system” in most documents related to this question. From this axis emerges the need to construct a common framework of urban mobility indicators for healthy cities using a diachronic and multi-level approach [86,87]. On the other hand, there are already several online applications that could act as sources of information for understanding the dynamics of real-time mobility; for example, users can be regarded as producers of information about their mobility (e.g., Google Maps). Other information sources include public transport ticketing systems, tolls, online pay-as-you-go parking, or GPS systems in public transport or municipal fleets. In the Portuguese academic context, there are several research projects focused on this subject, namely, the GENMOB project, “Gender and Mobility: Inequality in Space-Time” (IGOT, University of Lisbon, 2015/2016) [88]; the URBY-SENSE project, “Urban mobility analysis and prediction for non-routine scenarios using digital footprints” (CISUC, University of Coimbra, 2016–2018) [89], and the CISMOB project, “Cooperative Information Platform for low carbon and sustainable mobility” (University of Aveiro, 2016–2020) [90]. However, this area still raises legal issues associated with data privacy and the ability to manage and process large amounts of data (big data).
4.1.2. Public Health Planning Instruments in LMA
In the context of public health, there is also a wide range of planning instruments that guide the priorities in the LMA. A multi-level approach is evident by the existence of guidelines from the European level to the level of national, regional, and municipal policies [79]. Therefore, it is necessary to verify whether there are concrete concerns about the role of urban mobility in health and whether it is incorporated into the proposed measures in a set of plans and programs (Table 5).
The National Health Plan 2012–2016 (NHP), revised in 2015 and leading to the National Health Plan: Revision and extension to 2020 [91,92], is a strategic document that presents guidelines and actions for the promotion of the health system and the maximization of health gains. The document presents four objectives: “Gaining health benefits”, “Promoting favorable contexts for health throughout the life cycle”, “Strengthening social and economic support in health and disease”, and “Strengthening Portugal’s participation in global health”. It also has four strategic axes: “Citizenship in health”, “Equity and adequate access to healthcare”, “Quality in health”, and “Healthy policies”. The fourth strategic axis, healthy policies, is based on the concepts of the World Health Organization and the model of health determinants and combines the dual perspectives of public health and health in all policies. The participation of Portugal in international networks that promote healthy policies, such as the Portuguese Network of Healthy Municipalities, is underlined. In this document, despite the promotion of the intersectoral collaboration for health, urban mobility policies are never explicitly referenced.
In the context of the NHP, 12 priority health programs (smoking, healthy eating, physical activity, diabetes, cerebrovascular diseases, oncological diseases, respiratory diseases, hepatitis, HIV/AIDS, infections, mental health, and tuberculosis) have been established. Urban mobility is only referenced in the context of physical activity, namely, in the National Program for the Promotion of Physical Activity, guided by the National Strategy for the Promotion of Physical Activity, Health, and Welfare [93]. Part of this document promotes increased physical activity practices for a physically active lifestyle as a sign of health and well-being. Thus, it is underlined, although briefly, that among the strategies to increase the levels of physical activity of the populations, the development of environments and policies that promote active transport (cycle paths, pedestrian walkways, and public transport organization) is very important. In this line, whether or not it is treated as a transport mode or a leisure activity, active mobility promotes the physical activity of citizens of all ages.
At the regional level of the Lisbon and Tagus Valley Region (LTVR), in which the LMA is located, there is the Regional Health Plan 2018–2020 (RHPLTV) [94]. The RHPLTV 2018–2020 is the instrument for implementing the NHP, the WHO-Europe 2020 Strategy, and the Sustainable Development Objectives 2030. This document is framed by four strategic axes: citizenship, affections, sustainable health, and quality. Here, we emphasize the third axis, sustainable health, which relates the concepts of healthy policies and public health, with a value placed on the holistic approach of individuals: their contexts and lifestyles. The recommendations reinforce the importance of intersectoral strategies and policies for health, the strengthening of partnerships, and the enhancement of environmental health as a determinant of individuals’ health.
The Regional Health Profile of the LTVR [95] is a tool to support technical, political, strategic, and organizational decision making. It presents the evolution of a set of indicators by major themes at the level of the Health Centers Groups (ACES), with a brief set of transport and urban mobility indicators related to commuting and road accidents.
Local health plans (LHPs) at the ACES level are in line with national and regional strategies. They highlight the main problems and strategies according to the specificities of the community. Among the various LHPs, there are few references to the role of urban mobility in health (Table 6); some references related to commuting and road accidents in the diagnoses are present in the Almada-Seixal LHP and the Loures-Odivelas LHP, and a unique reference to the kilometers of cycling and pedestrian paths in the monitoring system is documented in the Arco Ribeirinho LHP. In 2017, the LTV Region created local health profiles for all ACES; these local health profiles are in line with the Regional Health Profile of the LTVR and includes a system of monitoring indicators that are highly focused on the characteristics of the population and their health conditions, with a more restricted number of indicators compared with the Regional Health Profile.
Lastly, health development plans (HDPs) are underlined as the instruments that are associated with municipal competencies for health promotion and municipal health strategies. In the few documents available in the LMA, some references to urban mobility’s contribution to health arise. In the Social and Health Development Plan 2007–2009 of Montijo, there exists a specific objective to increase the cycleway extension by 20% by 2009, along with the respective monitoring indicator [97]. In the Social and Health Development Plan 2018–2025 of Amadora, this issue is present in one of the strategic objectives: “promote mobility, transport and accessibility considering personal comfort and security”. This is formalized in two strategic initiatives:
- Initiatives that promote accessibility on the public road, such as obstacle removal, the widening of traffic lights, downsizing, tactile floors, and footpaths. These initiatives are framed by pilot projects of urban regeneration;
- Improvements to the public transport network in order to ensure the accessibility of transport and the mobility of elderly citizens, especially the most economically vulnerable. This initiative has the following goals: (1) implementing door-to-door transportation services at the parish level for disabled citizens to travel to public services, health centers, and hospitals; developing a diagnosis of traffic flows in public transport; and creating awareness of public transport operators of the need to create or improve internal circuits in the municipality [98].
A final example is the Health, Quality of Life and Welfare Development Plan of the City of Lisbon 2017–2020 [99]. In this document, several projects are related to the health–urban mobility binomial, such as
- Noise Action Plan in conjunction with the management entities of road, rail, and air traffic;
- Pave Lisboa by restoring roads, replacing infrastructure, reconstructing sidewalks, altering signaling or removing architectural barriers, lowering or elevating walkways, introducing tactile floors and guides for people with reduced mobility, creating parking spaces for disabled people, and constructing bicycle lanes;
- Reduced emission areas that restrict the car circulation of older vehicles;
- Zonas 30, which limits the maximum circulation speed of 30 km per hour in certain areas to reduce road accidents, noise, and environmental pollution;
- Life project, which aims to eliminate the physical barriers that impede mobility while promoting the comfort and safety of people who are permanently limited in municipal housing;
- Neighborhood Network, which was established in order to generate greater proximity to the most important infrastructures in the neighborhoods, such as health centers, schools, kindergartens, markets, pharmacies, services, and subway stations, by complementing the transport network already in operation.
4.2. Practices and Discourses about Urban Mobility for Healthy Cities in LMA
4.2.1. The Perspective of Responsible Municipal Agents on Urban Mobility
According to the interviews with the autarchic responsible agents (politicians and technicians) in the domain of urban mobility in the eight municipalities in this study [44], the main concerns that have arisen over the last few years are underlined. Firstly, major urban changes have been identified that, combined with strong fluctuations in fuel and public transport prices, have greatly boosted the use of the car, leading to infrastructure and transport inadequacies (e.g., roads, parking, service reduction). Secondly, the financial and economic national and European crisis impacted families and their transportation options. Companies were forced to restructure through strategies involving employee dismissals or relocation to peripheral areas that were cheaper but unprepared to receive larger flows of people, which involved decreasing the number of registered transport operators, and thus decreasing the number of users. As a result, the restructuring of their services was required. Finally, the municipal councils resented the resource cutbacks, which affected the ability to raise new funding for infrastructures and planning instruments, such as the SUMP. The final concern refers to the conditions of the autarchies that faced some limitations to their performance, specifically, insufficient human resources and time for all tasks, a lack of financial resources, and a lack of political competencies. However, financial constraints have been circumvented by seeking external and diversified funds, reducing the number of infrastructure interventions, or turning to internal human resources.
The interviewed agents evaluated “Parking”, “Accessibility by transportation”, “Appropriate traffic lights and walkways”, and “Surrounding of public facilities” as domains that are extremely important, while the domains “Noise”, “Carbon emissions from motorized transport”, and “Accessibility to commercial areas” were considered less important. On the other hand, there were different positions regarding the domain “Accessibility by bike path”: it was evaluated as less important in Odivelas and extremely important in the municipalities of Moita, Setúbal, and Loures.
The partnership networks were also analyzed in light of their relevance, with the assumption that in a partnership with a high level of intensity, one of the partners will occur more frequently or prove to be decisive in the fulfillment of the municipal objectives. Summarizing the various responses, the closest circle of partners to these offices comprises the municipal presidency and parish councils (the lowest power level of the Portuguese governance structure), transport operators, and municipality departments associated with green spaces and public spaces. By contrast, there has been little or no relationship with the coordination of the Portuguese Network of Healthy Cities, the department in which the Healthy Cities project has been inserted, or social departments and social entities.
The main limitations and potentialities of these offices were reported during the interviews. Financial limitation was the first to be referenced, and it was considered a constraint to planning and intervention in the domain of urban mobility, as well as to capturing new financing. In this context, it was emphasized that collaboration between municipalities leveraged more financing for joint interventions (Moita). The absence or lack of interaction with human resources was the second limitation identified. This issue was judged to sometimes generate more time-consuming interventions or require the use of external resources to fill technical areas that did not exist in the autarchy (Loures, Moita, and Setúbal). The third and final limitation was associated with the lack of legal competencies that are necessary: for example, for joint planning strategies between municipalities or at a metropolitan level to solve major problems such as excessive traffic (Oeiras, Odivelas). On the other hand, the first potentiality was related to the multiple capacities of the autarchies: the high quality of technical teams and deep knowledge of the territory, the capacity to develop instruments and execute their actions in a manner that was better adapted to each municipal reality, and the fast adaptation to the context of crisis through low-resource solutions with great impacts (Loures, Moita, Oeiras, and Setúbal). A second potentiality was the political will to promote sustainable and healthy territories, as reflected by the good acceptance of technical suggestions offered by the presidencies, who acted as a catalyst, moderator, and conciliator in the autarchies on several fronts and represented an element of balance between top–down and bottom–up approaches (Odivelas and Moita). In this context, the use of the “sustainable urban mobility” slogan has enabled the attainment of financing for studies and interventions inserted into the European Structural and Investment Funds 2014–2020, with the fostering of strategies and partnerships between nearby municipalities that share the same concerns and between municipalities and transport operators (Loures, Odivelas, and Moita). The last potentiality was linked to the high expectations for the results of planning instruments, particularly the SUMP, and there were positive expectations about the inclusion of urban mobility policies in all planning documents and other sectoral instruments (Setúbal, Moita). Other expectations included a stronger change in the mentalities and behaviors of people, a greater understanding of urban mobility issues, and greater confidence in the work of the municipality councils.
Finally, there were several initiatives identified by the various interviewed agents that are related to the assumptions of healthy cities, although the relationship is informal; that is, none of the initiatives are officially associated with the municipal intervention for healthy cities [78,79]. In this context, we highlight the following:
- In axis 3, “Inclusive, safe, and barrier-free transport system”, there is emphasis on the implementation of flexible urban transportation systems (e.g., “Loures Rodinhas” in Loures, “ROTAS” in Oeiras, “Voltas” in Odivelas), the promotion of soft mobility in the education community (e.g., project “On foot to school”, usually known as Pedibus, in Loures (2010–2011)), and the promotion of road safety (e.g., “Be safe for better mobility: Road safety education in Basic Education” in Odivelas);
- In axis 11, “Agents and competencies”, the municipality of Cascais stands out because of two innovative initiatives: (1) the creation of the horizontal autarchic service “Accessibility for all” in 2011, with competencies in the planning and execution of transversal projects; and (2) the creation of the MobiCascais System (2017), which manages the municipal public transport system, bikesharing service, and parking;
- In axis 13, “Awareness of benefits for health, environment, and economy”, two items were noteworthy: (1) the implementation of Local Agenda 21, which is oriented toward sustainable development (Seixal), and (2) the participation of almost all of the LMA municipalities in European Mobility Weeks (except in Sesimbra), which has promoted local interventions for soft mobility and awareness campaigns.
4.2.2. The perspective of municipal responsible agents for the Healthy Cities projects
In the Portuguese case, Healthy Cities projects (HCP) are dynamized by the member municipalities of the Portuguese Network of Healthy Cities (PNHC). Six municipalities of LMA—Amadora, Cascais, Loures, Oeiras, Odivelas, and Seixal—were taken into account in order to understand the contribution of HCP to urban mobility based on the interviews with the technicians assigned to HCP [44].
The main initiatives framed by the HCP in the LMA were grouped into five areas: “Access to health”, “Social inclusion”, “Literacy and health education”, “Building and public space”, and “Urban mobility” [78,79]. Only one initiative was directly framed by the “Urban Mobility” area: the “Municipal Road Safety project”, which was the result of a partnership between Seixal City Hall, the security forces, and schools, with the aim of promoting safe behaviors to reduce road accidents. In the other areas, some initiatives were intended to promote greater and better mobility for all or specific community groups. For example, the area of “Social inclusion” included several adapted transport services (e.g., “Regular adapted transport” for disabled people in Oeiras); the area of “Building and public space” had initiatives to remove or adapt architectural barriers in buildings and public spaces (e.g., “Oeiras without barriers project“); finally, in the area of “Literacy and health education”, several initiatives to promote healthy behaviors were highlighted that focused, for example, on the importance of physical activity and the respective contribution of soft mobility to that goal (e.g., “Club in Movement “(Odivelas) and “Move More” (Oeiras)).
Partnerships are fundamental within the HCP because they minimize the existing limitations of human and financial resources and maximize the impact of their initiatives. A clear hierarchy of partners was identified by the interviewed agents according to the level of intensity (frequency and importance of the interactions). Political–administrative entities—the municipal council presidency, parish councils, and social departments of the autarchies—appeared as the most important. Second in importance were entities of a social nature, such as those with education, health, and social inclusion competencies. The good relations in the coordination between PNHC and other municipality members of the network are also noteworthy. In contrast, interactions with economic and environmental entities were, in general, strongly limited.
The main limitations and potentialities of HCP were identified, too. The most outstanding potential corresponded to the innovative methodology of the HCP, which is based on knowledge sharing at various levels (theoretical, methodological, political, and practical). The promotion of training and knowledge recycling for decision makers, technicians, and partners, the multi-sectoral approach to land planning, and the development of formal and informal re-partnerships were referred to as having the potential for more concerted action between actors at various scales. As the main constraints, human, technical, and financial resource shortages emerged primarily for the current workload and the capability of expanding the range of initiatives. This limitation was minimized by the shared work among partners and the good management of local authorities. Another limitation that was highlighted was the ability to realize the incorporation of HCP into all policies and the limited understanding and diffusion of the Healthy City movement philosophy among decision makers, technicians, partners, and the community.
In summary, the comparison of discourses and practices between urban mobility departments and Healthy Cities projects revealed some limitations to the potential participation of urban mobility in healthy cities initiatives (Figure 4). On the basis of the remarks made by those who were interviewed, the importance of partnerships is well known. On the one hand, the municipal councils, parish councils, and security forces are very important for both urban mobility and Healthy Cities projects. On the other hand, while urban mobility departments often work in partnership with transport operators and departments that manage green spaces and open spaces, HCP teams are more often related to social entities in the areas of education, health, and social inclusion. Finally, the evidence of little or no relationship between the agents under study—urban mobility departments and HCP teams—is bilaterally underlined. Regarding the practices, there are several initiatives in the area of urban mobility (regarding the number and variety of intervention axes) carried out by the urban mobility departments in favor of healthy cities, although they are informally associated; that is, such initiatives are not carried out with the clear objective of promoting healthy cities. On the other hand, within the Healthy Cities projects, initiatives in the area of urban mobility are scarce, partially because they are minimized by initiatives to improve urban mobility in other areas (“Social inclusion”, “Literacy and health education”, and “Building and public space”). In this context, the initiatives are highly concentrated in intervention axis 3: “Inclusive, safe and barrier-free transport system”.
5. Conclusions
The conclusions of this work provide the answer to the question being investigated. Firstly, it is confirmed that a strong link exists between the framework of sustainable development and healthy cities, both historically and conceptually, with four key points in common: they are multi-temporal, multi-sectoral, multiscalar, and considered to be a continuous process rather than just a final goal to be completed. The domain of urban mobility, which is widely considered in the context of sustainable development, also proves to be important in the context of healthy cities. Issues related to sustainable development generate a multiplicity of problems that lead to diverse social, environmental, and economic consequences, but they also serve as triggers to take action, as evidenced by the various intervention axes in sustainable urban mobility for Healthy Cities identified by the team.
However, a contradiction emerges from the main results. In the analysis of urban mobility planning instruments, there was a strong relationship between the various actions proposed in the intervention component of these documents and the axes of intervention in sustainable urban mobility for healthy cities, despite the diversity in the instrument typologies, territorial levels, the characteristics of the territory for which it is intended, and the publication years. However, it is noteworthy that in all documents, there is no explicit reference to “healthy cities”, but a reference to “sustainable development” is relatively frequent.
Regarding the municipal agent approach, on the one hand, it was frequently indicated that healthy cities principles were rarely or never considered in their daily practice, even though the majority of the LMA municipalities are members of the Portuguese Network of Healthy Municipalities. This contradicts the evident consistency between the concerns and actions of these same agents and the principles and framework of healthy cities. Thus, we can conclude that the healthy cities intervention is effective in the framework of the analyzed instruments and the framework of the interviewed teams, although its success is implicit and informal.
In conclusion, the answer to the research question (are sustainable urban mobility policies contributing to healthy cities?) is clearly affirmative as it is proven that sustainable development principles are an umbrella of all policies and diffuse in a top–down way, especially through the policies directed by the European Commission and Portuguese government. This fact translates to the policy instruments and practices being consistent with the principles of healthy cities, which is a movement characterized by its bottom–up nature and anchored in a local, innovative, multi-sectoral, and multiscalar governance strategy. These principles are not implemented explicitly or consciously by the technicians and politicians who work in the field of urban mobility in the LMA; nevertheless, the findings of this study indicate that they are being carried out.
6. Lessons for the Future
The intention of this research is to reinforce the contribution of science to urban planning policies and practices, particularly in the domains of sustainable urban mobility and healthy cities, as the communication of academic findings to decision makers is extremely important, and it works through the concept known as “research translation” or “knowledge transfer” [100]. The main conclusions of this research enable the identification of some lessons for the future to reinforce the common values regarding the policies and interventions for sustainable urban mobility and healthy cities: that is, both approaches are multi-temporal, multi-sectoral, and multi-level perspectives, and do not have a specific goal to achieve, but are instead a continuous process that can always be improved.
The promotion of cross-sectoral and multi-sectoral policies is one of the key factors in this study, although it proves to be scarce in both the analyzed instruments and agent discourses and practices [101,102,103]. In this sense, the following is suggested:
- The inclusion of Healthy Cities projects teams and/or their feedback in the elaboration, discussion, and evaluation phases of sustainable urban mobility planning instruments or other instruments;
- The inclusion of representatives of the urban mobility domain in a broad team of Healthy Cities projects (along with representatives of other areas, such as education, green spaces, or sanitation);
- Clear dissemination of the main concepts that shape the policies of each municipality (e.g., sustainable cities, healthy cities, eco-cities, inclusive cities, etc.) in all autarchic departments, as well as their reinforcement by the strong political influence of the presidency of the autarchies.
The knowledge of each reality and its monitoring serves as a support for political action that is more adapted to the problems and realities of the territory and community [1,104,105]. In this context, academia could take part by considering the following:
- The existence of national and international benchmarking studies can enrich the performance of municipalities and improve and/or expand their performance more efficiently, perhaps through creating new partnerships;
- The existence of community-based diagnostic studies based on surveys or interviews may also be relevant to policies and interventions that are more in line with local needs;
- The existence of up-to-date and independent monitoring systems that can be used simultaneously by the various agents from a multiscale perspective (from the local to the metropolitan/regional) enables the assessment of the dynamics in the long term, especially if the common objectives of the various departments are in tune with one another. This system could be used for urban modeling and simulation techniques to support policy decisions.
Partnerships have proved to be important within municipal actions [106,107]. The existence of several networks of partners is already a reality. However, sometimes, certain networks are confined to a single department (e.g., social department). Thus, the following actions are suggested:
- Encouraging the inclusion of the sustainable urban mobility approach and its influence on healthy cities not only in the network of partners of Healthy Cities projects but also in other existing networks (e.g., Social Network, Educational Network, Local Agenda 21). This promotes access to a greater diversity of funding sources and awareness initiatives.
Finally, the importance of the awareness of the community and local agents is highlighted, since it is only with their acceptance that significant changes can be expected [108,109,110,111]. Some of the main agents are as follows:
- The school community can become more involved by including this subject in educational programs, school mobility plans, and projects such as Pedibus, as well as the participation of the school community in initiatives to identify local problems and possible solutions;
- Companies, especially those with a large number of workers, are considered to be major centers of attraction/generation, so the deployment of the initiatives related to urban mobility and healthy cities can be enhanced by elaborating company mobility plans, employee awareness, initiatives with regard to policy transport in the company (e.g., fleet management, service cars), or boosting car-sharing initiatives;
- The transport operators, in order to promote better levels of quality of the transport system, can also become involved in campaigns to raise awareness of the factors leading to the unsustainability of individual transport and promote a modal shift to soft modes or collective transportation;
- The community in general can be engaged by discussing future political choices and sensitizing residents to the present and future problems of transport and its consequences, especially those that affect health;
- It is necessary to continue this specific research. If the implicit presence of the healthy city principles in the context of urban mobility planning has been proven, the next approach should be centered on the evaluation of the implementation of the instruments and their results. A more demanding study would be the evaluation of their impacts, especially on health. Only then can we assess the real changes that have been made in favor of healthier territories.
Thus, there is a need for future research, especially by the methodological replication of this study, which is anchored in sustainable urban mobility and focuses on various autarchic departments related to the “environment”, “social inclusion”, and “employment and local economy”, among other domains. This awareness will promote the more effective integration of urban mobility concerns with all policies, maximize the positive effects of the planning instruments and municipal interventions, increase the partnership network, and generate greater positive impacts.
Author Contributions
Conceptualization, A.L. and N.M.d.C.; Formal analysis, A.L., N.M.d.C. and E.M.d.C.; Investigation, A.L. and N.M.d.C.; Methodology, A.L. and N.M.d.C.; Writing—original draft, A.L.; Writing—review & editing, N.M.d.C. and E.M.d.C.
Funding
The fieldwork of this research was funded by the research project “Local Development and Strategies to Built Healthy Cities” (4.4.1.00 CAPES Agreement) (2014–2016) in a bilateral consortia CAPES Brazil—FCT Portugal (coord. by Nuno Marques da Costa, IGOT-ULisboa) and by the individual PhD research project of Louro “Contributions of Urban Mobility Planning and Management for the construction of a ‘Healthy City’” (SFRH/BD/85150/2012) (2013–2017) financed by FCT Portugal. The output publication was funded by national funding through FCT—Fundação para a Ciência e a Tecnologia, I.P., in the framework of CEG multi-year financing 2019, reference number UID/GEO/00295/2019.
Acknowledgments
The authors would like to thank all the interviewees who made this work viable, validating the team results and presenting their specific perspectives as technicians and politicians. The authors would also like to thank to the editor and the three anonymous reviewers the very useful comments.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Interview Script to Urban Mobility Department Teams
- 1.
- Municipality characteristics (previous to the meeting)
- 1.1.
- Municipality
- 1.2.
- Department
- 1.3.
- Resident population and area (km2)
- 1.4.
- Interviewed (name, position)
- 2.
- Department framework
- 2.1.
- What are the main concerns of this department about the served territory and community?
- 2.2.
- Those main concerns are part of the overall strategy of this municipality; are they shared between the various municipal departments or are they exclusively from this department?
- 2.3.
- Is this department called upon to discuss the main policy guidelines of the municipality?
- 2.4.
- Is there any relationship between this department and the other city council departments? Which departments do you have the most interaction with? What are the main motivations?
- 3.
- Projects, initiatives, and planning and management instruments
- 3.1.
- What are the main projects or initiatives carried out in the domain of transport and urban mobility? Please identify its main characteristics (e.g., starting date, territorial coverage, target population, etc.).
- 3.2.
- What are your main planning and management instruments and/or studies about urban mobility and transport? Please identify its main characteristics (e.g., starting date, territorial coverage, target population, etc.).
- 3.3.
- Please assess the importance of the following themes in your daily work (1 = Not important, 2 = Slightly important, 3 = Moderately important, 4 = Important, 5 = Very important):
| Theme | Assessment(1–5) |
| Traffic | |
| Road accidents | |
| CO2 emissions from motorized transport | |
| Noise from transport | |
| Land use for accessibility infrastructures—roads, streets | |
| Land use for parking | |
| Footpaths | |
| Bike paths | |
| Public transportation | |
| Traffic lights and walkways | |
| Surrounding areas of public facilities (schools, health services, etc.) | |
| Special transport for the elderly, children and people with reduced mobility | |
| Accessibility to commercial areas | |
| Others: |
- 4.
- Partnerships
- 4.1.
- What are the main partners of this department?
- 4.2.
- Does the municipality/department belong to any national or international network with the purpose of exchanging experiences, technical training, knowledge of financing, or other?
- 4.3.
- We kindly ask you to evaluate the frequency of partnerships between your department and various agents (1 = Never, 2 = Rarely, 3 = Occasionally, 4 = Frequently, 5 = Very frequently):
| Agents | Partners | Partnership Frequency |
| Political and management agents | Presidency of the municipal council | |
| Health department/Health promotion department | ||
| Departments related to public facilities | ||
| Departments related to social action | ||
| Departments related to public spaces/green spaces | ||
| Parish councils | ||
| Healthy Cities Network | Coordination of the Portuguese Network of Healthy Cities | |
| Healthy Cities project within the municipality | ||
| Social agents | Hospitals and health centers | |
| Schools and kindergartens | ||
| Nursing homes and day care centers | ||
| Non-governmental organizations/Residents Associations/local development associations | ||
| Police | ||
| Fire brigades and civil defense | ||
| Universities and polytechnics | ||
| Economic agents | Transport operators | |
| Companies | ||
| Local businesses | ||
| Consultancy companies | ||
| Environmental agents | Environmental non-governmental organizations |
- 5.
- Constraints and potentialities
- 5.1.
- What are the main constraints of the department’s work?
- 5.2.
- What are the main potentialities of the department’s work?
Appendix B. Interview Script to Healthy Cities Project Teams
- 1.
- Municipality characteristics (previous to the meeting)
- 1.1.
- Municipality
- 1.2.
- Department
- 1.3.
- Resident population and area (km2)
- 1.4.
- Interviewed (name, position)
- 2.
- HCP framework
- 2.1.
- When did the municipality integrate with the Portuguese Network of Healthy Cities?
- 2.2.
- What is your current framework within the municipal council? (own office, integrated in a department—which? own human and technical resources?)
- 2.3.
- Is the Healthy Cities Project called upon to discuss the main policy guidelines of the municipality?
- 2.4.
- Are there any relationships between this department and the other city council departments? Which departments do you have the most interaction with? What are the main motivations?
- 3.
- Projects and initiatives
- 3.1.
- Does this Healthy Cities Project include the area of urban mobility in your daily work?
- 3.2.
- What are the main projects or initiatives carried out in this Healthy Cities Project? Please identify its main characteristics (e.g., starting date, territorial coverage, target population, etc.).
- 4.
- Partnerships
- 4.1.
- What are the main partners of this department?
- 4.2.
- Does this Healthy Cities Project (or the department where it is inserted) belong to any national or international network with the purpose of exchanging experiences, technical training, knowledge of financing, or other?
- 4.3.
- We kindly ask you to evaluate the frequency of partnerships between your department and various agents (1 = Never, 2 = Rarely, 3 = Occasionally, 4 = Frequently, 5 = Very frequently):
| Agents | Partners | Partnership Frequency |
| Political and management agents | Presidency of the municipal council | |
| Departments related to urban mobility | ||
| Departments related to public facilities | ||
| Departments related to social action | ||
| Departments related to public spaces/green spaces | ||
| Parish councils | ||
| Healthy Cities Network | Coordination of the European Network of Healthy Cities | |
| Other municipalities members of European Network of Healthy Cities | ||
| Coordination of the Portuguese Network of Healthy Cities | ||
| Other municipalities members of Portuguese Network of Healthy Cities | ||
| Social agents | Hospitals and health centers | |
| Schools and kindergartens | ||
| Nursing homes and day care centers | ||
| Non-governmental organizations/residents Associations/local development associations | ||
| Police | ||
| Fire brigades and civil defense | ||
| Universities and polytechnics | ||
| Economic agents | Transport operators | |
| Companies | ||
| Local businesses | ||
| Consultancy companies | ||
| Environmental agents | Environmental non-governmental organizations |
- 5.
- Constraints and potentialities
- 5.1.
- What are the main constraints of the Healthy Cities Project s work?
- 5.2.
- What are the main potentialities of the Healthy Cities Project ’s work?
Appendix C. NVivo11 Software
This appendix intends to synthetically describe the NVivo 11 software [112,113]. NVIVO is a qualitative data analysis software that enables the organization and analysis of information from unstructured or semi-structured data (e.g., interviews, reports, etc.), allowing its comparison by sources and their attributes. Ultimately, this approach generates quantitative analyses of, for example, the frequency of nodes in each source. NVivo software uses specific terminology, namely:
- (a)
- sources as the term referring to the research material (e.g., documents, transcripts, etc.);
- (b)
- nodes as a virtual container (a code, category, or topic) that will support the act of coding the source content;
- (c)
- coding as the action of identifying the topic(s) associated with a portion of the source content;
- (d)
- cases and their attributes as characteristics or metadata about the sources.
NVivo software offers a generic step sequence (Figure A1), with the coding process dependent on the objectives, methodology, and sources of each study.
Figure A1.
Proposed path for codification. Source: Adapted from [112].
Figure A1.
Proposed path for codification. Source: Adapted from [112].

In this context, coding is, perhaps, the most important step, because the results are totally dependent on the researcher’s decisions. This requires an iterative process, as the node structure could change during the coding process. There are different types of coding: (1) topic coding considering the discussed topic (e.g., real estate development); and (2) analytical coding considering the meaning of data (e.g., overvalued housing market). The same content (for example, a phrase or a paragraph) could be coded by multiple nodes.
After coding, the researcher is allowed to create queries in order to explore the data. The flexibility of NVivo software is reflected by the numerous types of queries, such as:
- (a)
- Text search, identifying all the occurrences of a word or phrase in one or more sources;
- (b)
- Word frequency, listing the most frequent words in one or more sources;
- (c)
- Coding, highlighting all the content coded in one or more nodes.
Lastly, NVivo software also allows for the visualization of the queries through:
- (a)
- Maps, such as “mind maps”, especially used for brainstorm, “concept maps” based on concepts and their connections, and “project maps” that display all project information (sources, cases, attributes, etc.) and their links;
- (b)
- Charts, with several chart types available according to the data (e.g., bar chart, column chart, pie chart, bubble chart, heat maps, and radar charts) to represent coding information about one or more sources or nodes;
- (c)
- Hierarchy charts, allowing the visualization of a hierarchical structure through two types of charts: tree maps, as a set of nested rectangles of varying sizes, where size indicates the number of nodes coded or the number of coding references and relationships, and radial tree maps (sunburst), where each ring represents the hierarchy level of data (the innermost ring is the top level), allowing the identification of the contribution of each segment in the big picture;
- (d)
- Diagrams, namely:
- (d1)
- Cluster analysis, which groups sources and/or nodes based on words, coding, or attribute value similarities, where the greater the proximity of the sources or nodes in the diagram, the greater their similarities. There are several types of cluster analysis diagrams—2D cluster map, 3D cluster map, horizontal dendrogram, vertical dendrogram, circle graph—and three similarity metrics: Pearson correlation coefficient, Jaccard’s coefficient, and Sørensen’s coefficient.
- (d2)
- Explore diagrams, focused on all the linked items of one source or node;
- (d3)
- Comparison diagrams, allowing the comparison of all linked items of two sources or nodes, emerging what items are common or unique.
References
- May, A.; Page, M.; Hull, A. Developing a set of decision-support tools for sustainable urban transport in the UK. Transport Policy 2008, 15, 328–340. [Google Scholar] [CrossRef]
- Barton, H. Sustainable Communities—The Potential for Eco-Neighbourhoods, 1st ed.; Routledge: London, UK, 1999; ISBN 9781853835131. [Google Scholar]
- Wang, Y.; Sun, M.; Wang, R.; Lou, F. Promoting regional sustainability by eco-province construction in China: A critical assessment. Ecol. Indic. 2015, 51, 127–138. [Google Scholar] [CrossRef]
- Joss, S. Eco-Cities: The mainstreaming of urban sustainability—Key characteristics and driving factors. Int. J. Sustain. Dev. Plan. 2011, 6, 268–285. [Google Scholar] [CrossRef]
- Desouza, K.; Flanery, T. Designing, planning, and managing resilient cities: A conceptual framework. Cities 2013, 35, 89–99. [Google Scholar] [CrossRef]
- Marques da Costa, E.; Fumega, J.; Louro, A. Defining sustainable communities: The development of a toolkit for urban policy. J. Urban. Regen. Renew. 2012, 6, 278–292. [Google Scholar]
- Ouellet, M. Le smart growth et le nouvel urbanisme. Cah. Géogr. Qué. 2006, 50, 175–193. [Google Scholar] [CrossRef] [Green Version]
- Kenworthy, J. The eco-city: Ten key transport and planning dimensions for sustainable city development. Environ. Urban 2006, 18, 67–85. [Google Scholar] [CrossRef]
- Vale, L. The politics of resilient cities: Whose resilience and whose city? Build. Res. Inf. 2014, 42, 191–201. [Google Scholar] [CrossRef]
- Deal, B.; Pan, H.; Pallathucheril, V.; Fulton, G. Urban Resilience and Planning Support Systems: The Need for Sentience. J. Urban Technol. 2017, 24, 29–45. [Google Scholar] [CrossRef]
- World Commission on Environment and Development (WCED). Our Common Future (The Brundtland Report); Oxford University Press: Oxford, UK, 1987; ISBN 978-0192820808. [Google Scholar]
- Holden, E. Achieving Sustainable Mobility—Everyday and Leisure-Time Travel in the EU, 1st ed.; Ashgate: Hampshire, UK, 2007; ISBN 978-1138254954. [Google Scholar]
- Banister, D. Unsustainable Transport: City Transport. in the New Century; Routledge—Taylor & Francis Group: London, UK, 2005; ISBN 978-0415357906. [Google Scholar]
- Kickbusch, I. The contribution of the World Health Organization to a new public health and health promotion. Am. J. Public Health 2003, 93, 383–388. [Google Scholar] [CrossRef]
- What Is a Healthy City. Available online: WHO http://www.euro.who.int/en/health-topics/environment -and-health/urban-health/who-european-healthy-cities-network/what-is-a-healthy-city (accessed on 15 November 2018).
- Jakarta Declaration on Leading Health Promotion into the 21st Century. Available online: https://www.who.int/healthpromotion/conferences/previous/jakarta/declaration/en/ (accessed on 3 November 2018).
- HEALTH21: The Health for all Policy Framework for the WHO European Region. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/98398/wa540ga199heeng.pdf (accessed on 3 November 2018).
- Clos, J.; Surinach, R. Integrating Human Health into Urban. and Transport. Planning—A Framework; Springer: Cham, Switzerland, 2019; ISBN 978-3319749822. [Google Scholar]
- The Melbourne Principles for Sustainable Cities. Available online: http://archive.iclei.org/documents/ANZ/WhatWeDo/ISS/ISS_InfoSheet3_SustainabilityPrinciples.pdf (accessed on 7 October 2018).
- WHO. Health Promotion Glossary; WHO/HPR/HEP/98.1; WHO: Geneva, Switzerland, 1998. [Google Scholar]
- WHO. Healthy City Checklist. Available online: http://www.euro.who.int/en/health-topics/environment-and-health/urban-health/who-european-healthy-cities-network/what-is-a-healthy-city/healthy-city-checklist (accessed on 15 November 2018).
- Turcu, C. Re-thinking sustainability indicators: Local perspectives of urban sustainability. J. Environ. Plan. Mant. 2013, 56, 695–719. [Google Scholar] [CrossRef]
- Pacione, M. Urban. Geography: A Global Perspective. Routledge, 3rd ed.; Routledge—Taylor & Francis Group: London, UK, 2009; ISBN 978-0415462020. [Google Scholar]
- WBCSD. Mobility 2001—World Mobility at the end of the Twentieth Century and Its Sustainability; WBCSD: Conches-Geneva, Switzerland, 2001. [Google Scholar]
- Pacote da Mobilidade. Available online: http://www.imt-ip.pt/sites/IMTT/Portugues/Planeamento/ DocumentosdeReferencia/PacotedaMobilidade/Paginas/QuadrodeReferenciaparaPlanosdeMobilidadeAcessibilidadeeTransportes.aspx (accessed on 2 March 2017).
- Rodrigue, J.; Comtois, C.; Slack, B. The Geography of Transport. Systems, 1st ed.; Routledge—Taylor & Francis Group: London, UK, 2006; ISBN 978-041582253. [Google Scholar]
- CE. Roteiro do espaço único europeu dos transportes—Rumo a um sistema de transportes competitivo e económico em recursos; COM(2011)144; CE: Bruxelas, Bélgica, 2011. [Google Scholar]
- Black, W.R. Sustainable Transportation—Problems and Solutions, 1st ed.; The Guilford Press: New York, NY, USA, 2010; ISBN 978-1606234853. [Google Scholar]
- Burns, L.D. A vision of our transport future. Nature 2013, 497, 181–182. [Google Scholar] [CrossRef] [PubMed]
- DG Energy and Transport. A Sustainable Future for Transport; EU: Luxembourg City, Luxembourg, 2009. [Google Scholar] [CrossRef]
- Gilbert, R.; Perl, A. Transport. Revolution: Moving People and Freight Without Oil; Earthscan: London, UK, 2008; ISBN 978-1844072484. [Google Scholar]
- Newman, P.; Kenworthy, J. Sustainability and Cities: Overcoming Automobile Dependence; Island Press: Washington, DC, USA, 1999; ISBN 978-1559636605. [Google Scholar]
- Marques da Costa, N. Mobilidade e Transporte em Áreas Urbanas. O caso da Área Metropolitana de Lisboa. Doctoral Thesis, Universidade de Lisboa, Lisboa, Portugal, 2007. [Google Scholar]
- Milner, J.; Davies, M.; Wilkinson, P. Urban energy, carbon management (low carbon cities) and co-benefits for human health. Curr. Opin. Environ. Sustain. 2012, 4, 398–404. [Google Scholar] [CrossRef] [Green Version]
- Barton, H.; Grant, M. Urban Planning for Healthy Cities: A Review of the Progress of the European Healthy Cities Programme. J. Urban Health 2011, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Barton, H.; Mitcham, C.; Tsourou, C. Healthy urban planning and transport. In Proceedings of the WHO workshop on Sustainable and Healthy Urban Transport and Planning, Nicosia, Cyprus, 2003; UNECE: Nicosia, Cyprus, 2003; pp. 1–13. [Google Scholar]
- Frumkin, H.; Frank, L.; Jackson, R. Urban. Sprawl and Public Health—Designing, Planning and Building for Healthy Communities; Island Press: Washington, DC, USA, 2004; ISBN 978-1559633055. [Google Scholar]
- Semenza, J.C. Building Healthy Cities—A Focus on Interventions. In Handbook of Urban Health: Populations, Methods, and Practice; Galea, S., Vlahov, D., Eds.; Springer: New York, NY, USA, 2005; pp. 459–478. ISBN 978-0-387-23994-1. [Google Scholar]
- Duhl, L.J.; Sanchez, A.K. Healthy Cities and the City Planning Process: A Background Document on Links between Health and Urban Planning; EUR/ICP/CHDV 03-04-03; WHO-Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Simpson, B.J. Urban. Public Transport Today, 1st ed.; E & FN SPON: London, UK, 2003; ISBN 0-203362233. [Google Scholar]
- Newman, P. Global Cities, Transport, Energy and the Future: Will Ecosocialization Reverse the Historic Trends? In Making Urban Transport Sustainable; Low, N., Gleeson, B., Eds.; Palgrave Macmillan: New York, NY, USA, 2003; pp. 25–41. ISBN 978-0230523838. [Google Scholar]
- ECMT. Vandalism, Terrorism and Security in Urban. Public Passenger Transport; Economic Research Centre: Paris, France, 2003. [Google Scholar]
- Bai, X.; Nath, I.; Capon, A.; Hasan, N.; Jaron, D. Health and wellbeing in the changing urban environment: Complex challenges, scientific responses, and the way forward. Curr. Opin. Environ. Sustain. 2012, 4, 465–472. [Google Scholar] [CrossRef]
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. Projetos Cidades Saudáveis na Área Metropolitana de Lisboa—Exemplo da “Mobilidade urbana” como área de intervenção. Confins 2018, 38, 1–22. [Google Scholar] [CrossRef]
- Vale, D.S.; Saraiva, M.; Pereira, M. Active accessibility: A review of operational measures of walking and cycling accessibility. J. Transp. Land Use 2016, 9, 1–27. [Google Scholar] [CrossRef]
- Muhlbach, J.D. Building Healthy Communities: Integrating Walkability Concepts into Local Land Use Planning. Master thesis in Community and Regional Planning Program: Student Projects and Theses, University of Nebraska, Lincoln, NE, USA, 2012. nº 16. 81 p. [Google Scholar]
- Napier, M.A.; Brown, B.B.; Werner, C.M.; Gallimore, J. Walking to school: Community design and child and parent barriers. J. Environ. Psychol. 2011, 31, 45–51. [Google Scholar] [CrossRef]
- Pooley, C.G.; Horton, D.; Scheldeman, G.; Mullen, C.; Jones, T.; Tight, M.; Jopson, A.; Chisholm, A. Policies for promoting walking and cycling in England: A view from the street. Transp. Policy 2013, 27, 66–72. [Google Scholar] [CrossRef]
- White, P. Public Transport—Its Planning, Management and Operation, 4th ed.; Spon Press—Taylor & Francis Group: London, UK, 2004; ISBN 978-0415257718. [Google Scholar]
- Daniels, R.; Mulley, C. Explaining walking distance to public transport: The dominance of public transport supply. J. Transp. Land Use 2011, 6, 5–20. [Google Scholar] [CrossRef]
- Morar, T.; Bertolini, L. Planning for Pedestrians: A Way Out of Traffic Congestion. Proc. Soc. Behav. 2013, 81, 600–608. [Google Scholar] [CrossRef] [Green Version]
- Dombois, O.T.; Kahlmeier, S.; Martin, B.; Racioppi, F.; Braun-Fahrländer, C. Collaboration between the Health and Transport. Sectors in Promoting Physical Activity: Examples from European Countries; WHO-Europe: Copenhagen, Denmark, 2006; ISBN 92-89021918. [Google Scholar]
- Leountidou, L.; Couch, G. Urban Sprawl and Hybrid Cityscapes in Europe: Comparisons, Theory Construction and Conclusions. In Urban Sprawl in Europe—Landscapes, Land-Use Change & Policy; Couch, G., Leontidou, C., Petschel-Held, L., Eds.; Blackwell Publishing: Oxford, UK, 2007; pp. 242–268. ISBN 978-1405139175. [Google Scholar]
- Litman, T.; Burwell, D. Issues in sustainable transportation. Int. J. Glob. Environ. Issues 2006, 6, 331–347. [Google Scholar] [CrossRef]
- Macário, R. What is Strategy in Urban Mobility Systems? In Proceedings of the 10th Conference on Competition and Ownership in Land Passenger Transport, Sydney, Australia, 2007; University of Sydney: Sydney, Australia, 2007; Volume 01094956, pp. 107–126. [Google Scholar]
- Jenks, M.; Jones, C. Dimensions of the Sustainable City; Springer: Dordrecht, The Netherlands; Heidelberg, Germany; London, UK, 2010; ISBN 978-1402086465. [Google Scholar]
- Are We Developing Battery-Reared or Free-Range Children? Available online: https://mayerhillman.com/2002/03/14/are-we-developing-battery-reared-or-free-range-children/ (accessed on 7 October 2018).
- Hass-Klau, C. Walking and its relationship to public transport. In Sustainable Transport—Planning for Walking and Cycling in Urban Environments; Tolley, R., Ed.; CRC Press: Cambridge, UK, 2003; pp. 189–199. ISBN 978-0849317835. [Google Scholar]
- Vlahov, D.; Freudenberg, N.; Proietti, F.; Ompad, D.; Quinn, A.; Nandi, V.; Galea, S. Urban as a Determinant of Health. J. Urban. Health 2007, 84 (Suppl. 3), i16–i26. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.J. Urban health challenges in Europe. J. Urban Health 2013, 90 (Suppl. 1), 23–36. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Khreis, H. Car free cities: Pathway to healthy urban living. Environ. Int. 2016, 94, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Younger, M.; Morrow-Almeida, H.R.; Vindigni, S.M.; Dannenberg, A.L. The Built Environment, Climate Change, and Health. Opportunities for Co-Benefits. Am. J. Prev. Med. 2008, 35, 517–526. [Google Scholar] [CrossRef]
- Barton, H.; Mitcham, C.; Tsourou, C. Healthy Urban Planning in Practice: Experience of European Cities; WHO-Europe: Copenhagen, Denmark, 2003; ISBN 92-89010886. [Google Scholar]
- Dora, C.; Phillips, M. Transport., Environment and Health; WHO-Europe: Copenhagen, Denmark, 2000; ISBN 92-89013567. [Google Scholar]
- Marques da Costa, E. Desconstruir utopias e construir novas práticas para um Planejamento urbano saudável. Presented at the VI Simpósio Internacional Saúde Ambiental para Cidades Saudáveis, Uberlândia, Brazil, 30 August 2017. [Google Scholar] [CrossRef]
- Edwards, P.; Tsouros, A.D. Promoting Physical Activity and Active Living in Urban Environments: The Role of Local Governments; WHO-Europe: Copenhagen, Denmark, 2006; ISBN 92-89021810. [Google Scholar]
- Cavill, N.; Kahlmeier, S.; Racioppi, F. Physical Activity and Health in Europe: Evidence for Action; WHO-Europe: Copenhagen, Denmark, 2006; ISBN 92-89013877. [Google Scholar]
- Edwards, P.; Tsouros, A.D. A Healthy City Is an Active City: A Physical Activity Planning Guide; WHO-Europe: Copenhagen, Denmark, 2008; ISBN 978-9289042918. [Google Scholar]
- Marques da Costa, E. Cidades saudáveis, saúde e sustentabilidade: Dos conceitos às orientações de política na União Europeia. In Construindo cidades saudáveis; Lima, S.C., Marques da Costa, E., Eds.; Assis Editora: Uberlândia, Brasil, 2013; pp. 45–64. ISBN 78-8562192999. [Google Scholar]
- Perdue, W.C. Building Healthy Cities. Legal framework and considerations. In Handbook of Urban Healthy: Population, Methods, and Practice; Galea, S., Vlahov, D., Eds.; Springer Science: New York, NY, USA, 2005; pp. 503–519. ISBN 978-0387857701. [Google Scholar]
- Promoting Healthy Cities. Available online: http://www.rtpi.org.uk/briefing-room/rtpi-blog/why-planning-is-critical-to-a-healthy-urban-future/ (accessed on 7 October 2018).
- Colman, J. (Ed.) Urban Planning and Human Health in the European City—Report to the World Health Organisation by the International Society of City and Regional Planners; ISOCARP: Hague, The Netherlands, 2009; Available online: https://isocarp.org/app/uploads/2014/08/WHO_report_final_version.pdf (accessed on 3 September 2018).
- Dora, C. A different route to health: Implications of transport policies. BMJ Clin. Res. Ed. 1999, 318, 1686–1689. [Google Scholar] [CrossRef]
- Boschetti, F.; Davies, C.; Curtis, P.; Frost, M.; Haon, S.; Insall, P.; Meschik, M.; Nussio, F.; Panis, L.; Racioppi, F. Securing the Benefits of Active Travel in Europe; Conclusions from the Roundtable on Transport & Health Polis Conference, Polis: Brussels, Belgium, 2011; Available online: https://www.polisnetwork.eu/uploads/Modules/PublicDocuments/polis-paper-securing-the-health-benefits-of-active-travel-in-europe.pdf (accessed on 4 October 2018).
- Braubach, M. Healthy Cities—Challenges and Ways Forward. In Proceedings of the 8th European Conference on Sustainable Cities & Towns, Bilbao, Spain, 2016; ICLEI: Bilbao, Spain, 2016; Available online: http://conferences.sustainablecities.eu/fileadmin/user_upload/_imported/uploads/DOCUMENTS/PPT/Healthy_Cities/Healthy_cities_Matthias_Braubach.pdf (accessed on 31 September 2018).
- GIZ; BMZ; WHO. Urban. Transport. and Health. Urban. Transport. and Health. Module 5g—Sustainable Transport: Sourcebook for Policy Makers in Developing Cities; BMZ: Geneva, Switzerland, 2011; ISBN 978-9241502443. [Google Scholar]
- IUTP. Policy Brief—Desvendando os benefícios da mobilidade para a saúde; IUTP: São Paulo, Brasil, 2016; Available online: https://www.uitp.org/sites/default/files/cck-focus-papers-files/UITP_Policy_Brief_Health_POR_LQ.pdf (accessed on 29 August 2018).
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. A Cidade Saudável no planeamento municipal: Exemplos de atuação na AML, Portugal. In Construindo cidades saudáveis: Utopias e práticas; Ribeiro Soares, B., v. II, Marques da Costa, N., Lima, S.C., Marques da Costa, E., Eds.; Assis Editora: Uberlândia, Brasil, 2017; pp. 35–72. ISBN 978-8562191999. [Google Scholar]
- Instituto Nacional de Estatística—Principais Indicadores. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_princindic&menuBOUI=13707095&contexto=pi&selTab=tab0 (accessed on 29 December 2018).
- Louro, A.; Marques da Costa, N. Indicadores de Transporte e Mobilidade Urbana para as Cidades Saudáveis—Caso da Área Metropolitana de Lisboa, Portugal. Geo Uerj 2017, 30, 99–121. [Google Scholar] [CrossRef]
- Diários da República—Decreto-lei 200/91, de 29 de Maio. Available online: https://dre.tretas.org/dre/25993/decreto-lei-200-91-de-29-de-maio (accessed on 13 November 2018).
- Diários da República—Lei 22/82, de 17 de Agosto. Available online: https://dre.tretas.org/dre/34408/lei-22-82-de-17-de-agosto (accessed on 13 November 2018).
- Diário da República Electrónico—Lei 37/2007, de 14 de Agosto. Available online: https://dre.pt/pesquisa/-/search/636938/details/maximized (accessed on 13 November 2018).
- Diário da República Electrónico—Lei 63/2017, de 3 de Agosto. Available online: https://dre.pt/pesquisa/-/search/107805893/details/maximized (accessed on 13 November 2018).
- World Health Organization’s Framework Convention for Tobacco Control. Available online: https://apps.who.int/iris/bitstream/handle/10665/42811/9241591013.pdf;jsessionid=292555C309F907E9A5445E8659B7F6D7?sequence=1 (accessed on 3 November 2018).
- Marques da Costa, E. Da Ação em Saúde à Ação para a Saúde. In Geografia da Saúde—Ambientes e sujeitos sociais no mundo globalizado; Valdemir de Oliveira, J., Alves de Souza, G., Eds.; EDUA: Manaus, Brasil, 2016; pp. 71–93. ISBN 978-8574018140. [Google Scholar]
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. Transporte e Mobilidade urbana para as Cidades Saudáveis. Presented at the XVI Colóquio Ibérico da Geografia, Lisboa, Portugal, 5–7 November 2018. [Google Scholar]
- Gender and Mobility. Inequality in Space-Time–Policy Brief. Available online: http://genmob.ceg.ulisboa.pt/gender-and-mobility-inequaity-in-space-time-policy-briefgenero-e-mobilidade-desigualdade-no-espaco-tempo-informacao-para-as-politicas/ (accessed on 24 September 2018).
- URBY.SENSE—Urban Mobility Analysis and Prediction for Non-Routine Scenarios Using Digital Footprints. Available online: https://www.cisuc.uc.pt/publication/show/4880 (accessed on 24 September 2018).
- CISMOB Project—Cooperative Information Platform for Low Carbon and Sustainable Mobility–Project Summary. Available online: https://www.interregeurope.eu/cismob/ (accessed on 24 September 2018).
- Plano Nacional de Saúde 2012–2016—Versão Resumo. Available online: http://pns.dgs.pt/files/2013/05/PNS2012_2016_versaoresumo_maio20133.pdf (accessed on 14 March 2019).
- Plano Nacional de Saúde—Revisão e extensão a 2020. Available online: https://www.dgs.pt/em-destaque/plano-nacional-de-saude-revisao-e-extensao-a-2020-aprovada-pelo-governo.aspx (accessed on 14 March 2019).
- Programa Nacional para a Promoção da Atividade Física. Available online: https://www.dgs.pt/pns-e-programas/programas-de-saude-prioritarios/atividade-fisica.aspx (accessed on 14 March 2019).
- Plano Regional de Saúde Lisboa e Vale do Tejo. Available online: http://www.arslvt.min-saude.pt/uploads/writer_file/document/6792/PRSLVT_-_Plano_Regional_Sa_de_LVT.pdf (accessed on 14 March 2019).
- ARSLVT—Perfil Regional de Saúde 2017. Available online: http://www.arslvt.min-saude.pt/pages/197 (accessed on 14 March 2019).
- Planos Locais de Saúde. Available online: https://pns.dgs.pt/planos-locais-de-saude/ (accessed on 14 March 2019).
- Plano de Desenvolvimento Social e de Saúde 2007–2009. Available online: https://www.mun-montijo.pt/cmmontijo/uploads/writer_file/document/3026/2007-09_-_II_PDSS.pdf (accessed on 14 March 2019).
- Plano de Desenvolvimento Social e de Saúde 2018–2025. Available online: http://www.cm-amadora.pt/images/INTERVENCAO_SOCIAL/REDE_SOCIAL/PDF/plano_desenvlvmnt_social_saude_2018_2025.pdf (accessed on 14 March 2019).
- Plano de Desenvolvimento de Saúde, Qualidade de Vida e Bem-estar da Cidade de Lisboa. Available online: http://observatorio-lisboa.eapn.pt/wp-content/uploads/PDSQVBEL_Vol_III_PLANO_DE_ACCAO 2017-2020_07-08-2017.pdf (accessed on 14 March 2019).
- Sallis, J.; Bull, F.; Burdett, R.; Frank, L.; Giffihs, P.; Giles-Corti, B.; Stevenson, M. Use of science to guide city planning policy and practice: How to achieve healthy and sustainable future cities. Lancet 2016, 388, 2936–2947. [Google Scholar] [CrossRef]
- Stead. Institutional aspects of integrating transport, environment and health policies. Transp. Policy 2008, 15, 139–148. [Google Scholar] [CrossRef]
- Lin, V.; Carter, B. From Healthy Public Policy to Intersectoral Action and Health-in-All Policies. In Global Handbook on Noncommunicable Diseases and Health Promotion; McQueen, D., Ed.; Springer: New York, NY, USA, 2013; pp. 189–201. ISBN 978-1-4614-7593-4. [Google Scholar]
- Guell, C.; Mackett, R.; Ogilvie, D. Negotiating multisectoral evidence: A qualitative Study of knowledge Exchange at the intersection of transport and public health. BMC Public Health 2017, 17, 1–17. [Google Scholar] [CrossRef]
- Deal, B.; Pan, H.; Timm, S.; Pallathucheril, V. The role of multidirectional temporal Analysis in scenario planning exercises and Planning Support Systems. Comput. Environ. Urban. Syst. 2017, 64, 91–102. [Google Scholar] [CrossRef]
- Miranda, H.; Rodrigues da Silva, A. Benchmarking sustainable urban mobility: The case of Curitiba, Brazil. Transp. Policy 2012, 21, 141–151. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Whitzman, C. Active living research: Partnerships that count. Health Place 2012, 18, 118–120. [Google Scholar] [CrossRef] [Green Version]
- Dirgahayani, P.; Nakamura, F. Fostering partnerships towards sustainable urban mobility from the National to local level: Matsuyama, Japan and Yogyakarta, Indonesia. Iatss Res. 2012, 36, 48–55. [Google Scholar] [CrossRef]
- Curtis, C.; Headicar, P. Targeting travel awareness campaigns: Which individuals are more likely to switch from car to other transport for the journey to work? Transp. Policy 1997, 4, 57–65. [Google Scholar] [CrossRef]
- Macário, R.; Marques, C. Transferability of sustainable urban mobility measures. Res. Transp. Econ. 2008, 22, 146–156. [Google Scholar] [CrossRef]
- Bamberg, S.; Fujii, S.; Friman, M.; Gärling, T. Behaviour theory and soft transport policy measures. Transp. Policy 2011, 18, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Cruz, I.; Katz-Gerro, T. Urban public transport companies and srategies to promote sustainable consumption Practices. J. Clean. Prod. 2016, 123, 28–33. [Google Scholar] [CrossRef]
- NVivo 11 for Windows—Concepts, Strategies and Techniques. Available online: http://help-nv11. qsrinternational.com/desktop/concepts/Understand_product_editions.htm (accessed on 16 September 2017).
- Using NVivo for Qualitative Research. Available online: http://help-nv11. qsrinternational.com/desktop/concepts/using_nvivo_for_qualitative_research.htm (accessed on 16 September 2017).
Figure 1.
(A) Nomenclature of Territorial Units for Statistics (NUTS) III—Lisbon Metropolitan Area (LMA), Mainland Portugal, (B) LMA municipalities.
Figure 1.
(A) Nomenclature of Territorial Units for Statistics (NUTS) III—Lisbon Metropolitan Area (LMA), Mainland Portugal, (B) LMA municipalities.

Figure 2.
Dimensions of analysis of sustainable urban mobility and public health/healthy cities policies and practices and respective methodological steps. Source: Own source.
Figure 2.
Dimensions of analysis of sustainable urban mobility and public health/healthy cities policies and practices and respective methodological steps. Source: Own source.

Figure 3.
Distribution of descriptors per document. Note: “N” represents the total number of codifications per document, considering that each item can be encoded by one or more descriptors. Source: Own source.
Figure 3.
Distribution of descriptors per document. Note: “N” represents the total number of codifications per document, considering that each item can be encoded by one or more descriptors. Source: Own source.

Figure 4.
Practices and discourses about urban mobility for healthy cities in LMA—Synthesis. Source: Own source.
Figure 4.
Practices and discourses about urban mobility for healthy cities in LMA—Synthesis. Source: Own source.


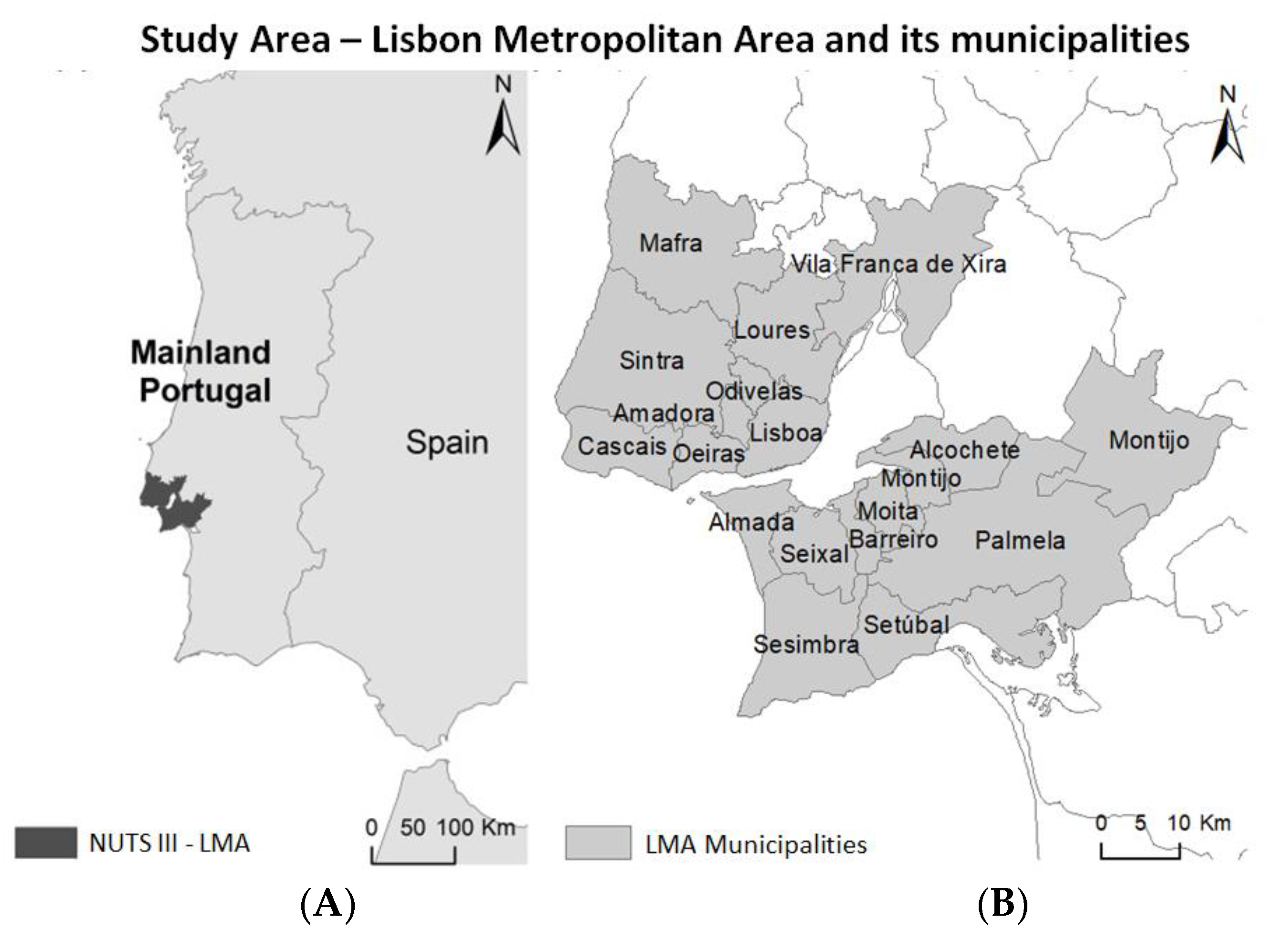{kind=link}
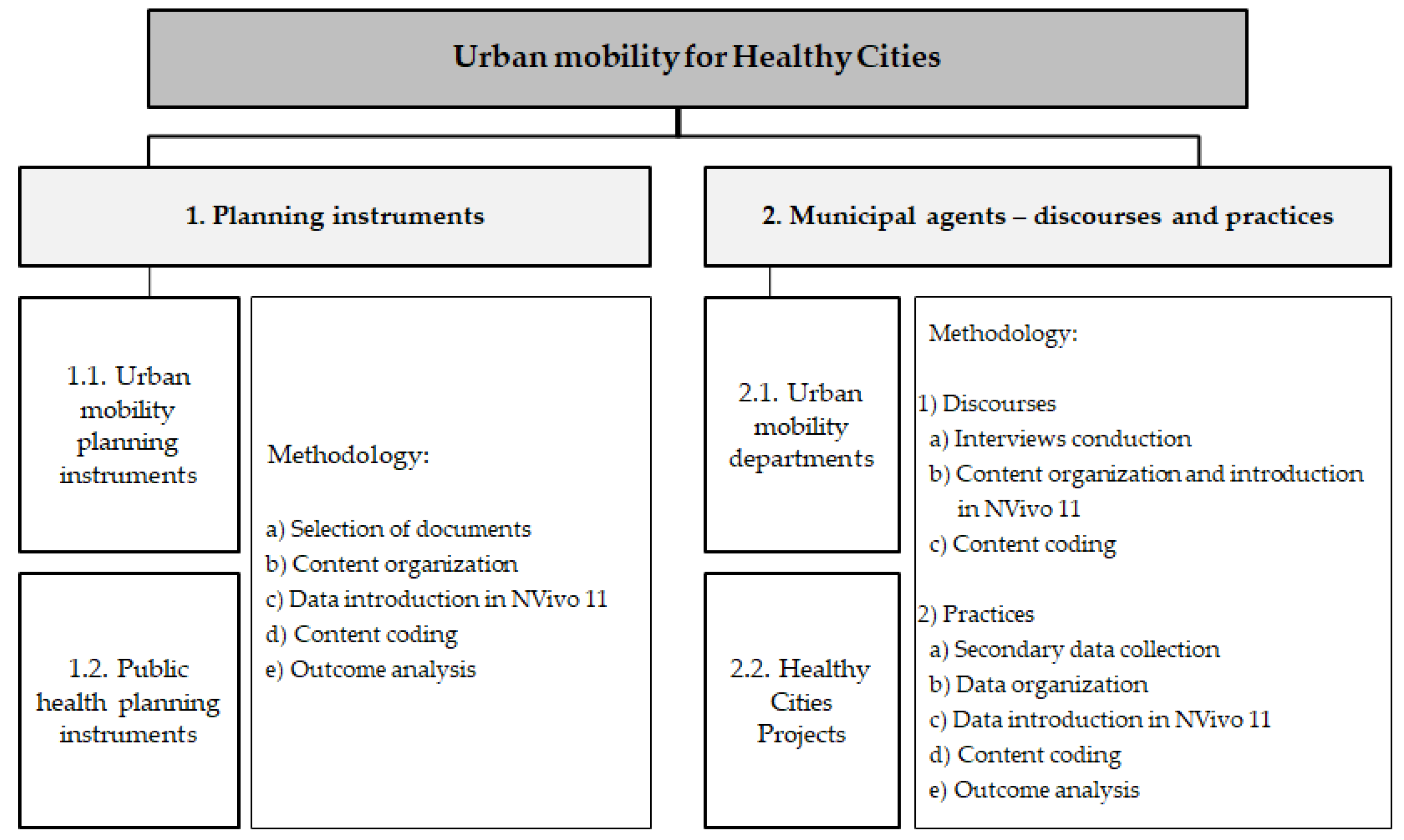{kind=link}
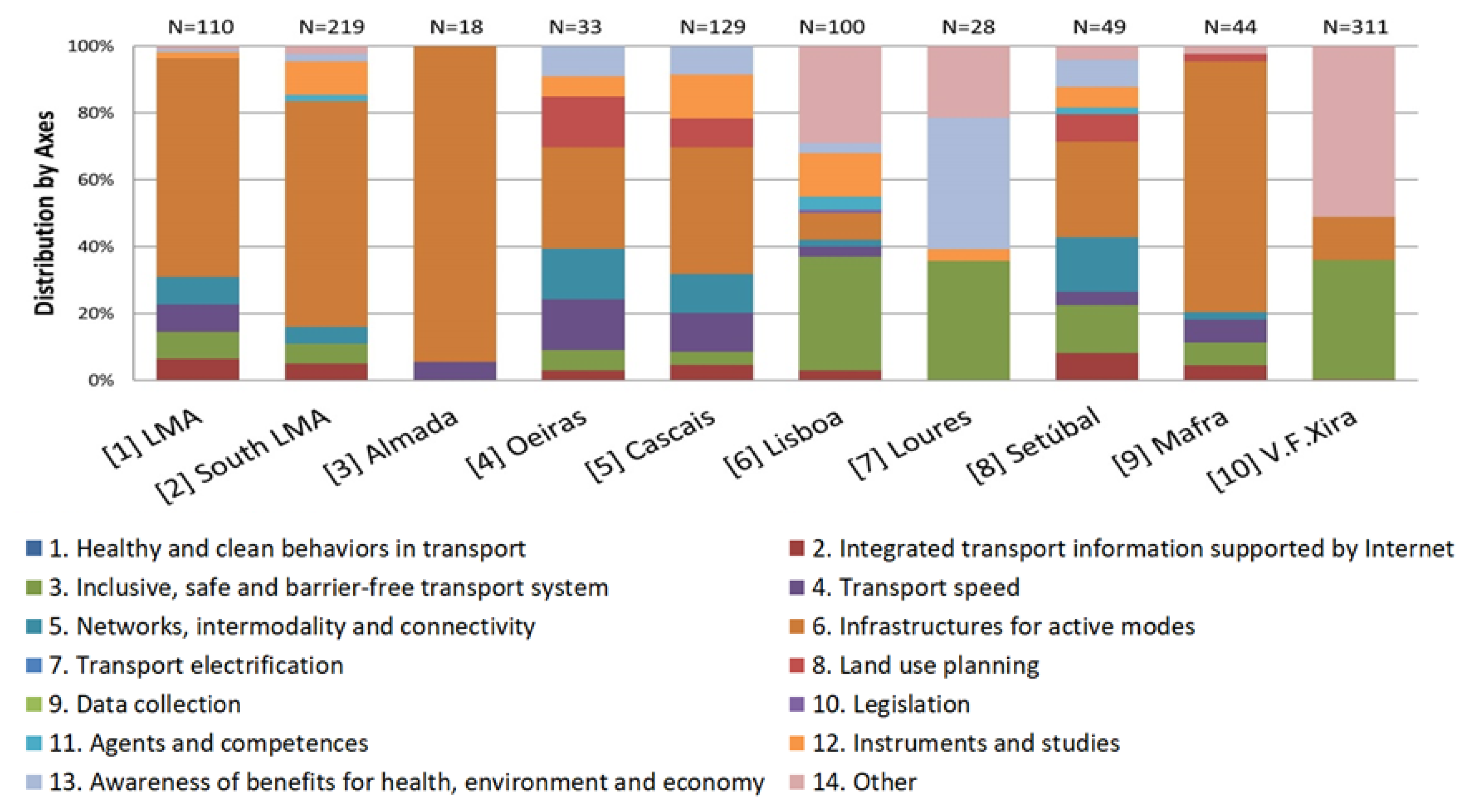{kind=link}
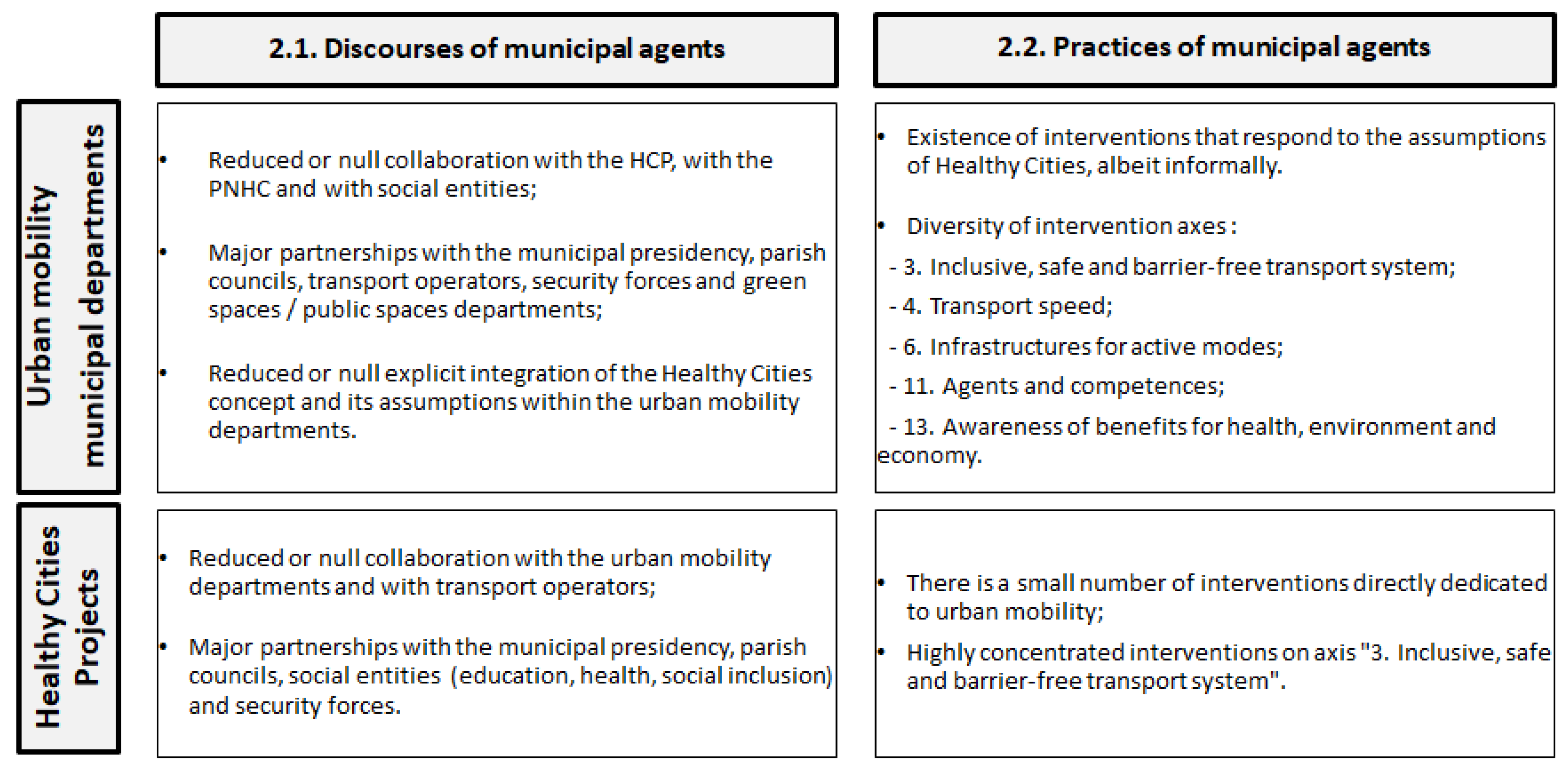{kind=link}
{kind=link}
Table 1.
Definitions and principles of sustainable cities and healthy cities.
| Definition | Principles | |
|---|---|---|
| Sustainable cities | “A sustainable city is often defined as a city designed with consideration of local and global environmental impact, guided by urban sustainability visions and targets. People in a sustainable city try to minimize their required inputs of energy, water, and food, and waste output of heat, air, and water pollution and greenhouse gas emissions. (…) [a] sustainable city should meet the needs of the present without compromising the ability of future generations to meet their own needs.” Source: [18] (p. 9) | “The Melbourne principles for sustainable cities 1: Provide a long-term vision for cities based on sustainability; intergenerational, social, economic, and political equity; and their individuality. 2: Achieve long-term economic and social security. 3: Recognize the intrinsic value of biodiversity and natural ecosystems, and protect and restore them. 4: Enable communities to minimize their ecological footprint. 5: Build on the characteristics of ecosystems in the development and nurturing of healthy and sustainable cities. 6: Recognize and build on the distinctive characteristics of cities, including their human and cultural values, history, and natural systems. 7: Empower people and foster participation. 8: Expand and enable cooperative networks to work toward a common sustainable future. 9: Promote sustainable production and consumption through the appropriate use of environmentally sound technologies and effective demand management. 10: Enable continual improvement, based on accountability, transparency, and good governance.” Source: [19] (p. 2) |
| Healthy cities | “A healthy city is one that is continually creating and improving those physical and social environments and expanding those community resources which enable people to mutually support each other in performing all the functions of life and in developing to their maximum potential.” Source: [20] (p. 13) | “A Healthy City aims to provide: 1. a clean, safe physical environment of high quality (including housing quality); 2. an ecosystem that is stable now and sustainable in the long term; 3. a strong, mutually supportive, and non-exploitative community; 4. a high degree of participation in and control by the citizens over the decisions affecting their lives, health, and well-being; 5. the meeting of basic needs (food, water, shelter, income, safety, and work) for all the city’s people; 6. access by the people to a wide variety of experiences and resources, with the chance for a wide variety of contact, interaction, and communication; 7. a diverse, vital, and innovative economy; connectedness with the past, with the cultural and biological heritage of city dwellers, and with other groups and individuals; 8. a form that is compatible with and enhances the preceding characteristics; an optimum level of appropriate public health and sickness care services, accessible to all; 9. high health status (high levels of positive health and low levels of disease).” Source: [21] |
Table 2.
Influence matrix of sustainable urban mobility problems and consequences for healthy cities (x = strong or moderate influence). Source: Own source developed from literature review.
Table 2.
Influence matrix of sustainable urban mobility problems and consequences for healthy cities (x = strong or moderate influence). Source: Own source developed from literature review.
| Sustainable Urban Mobility Problems | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Consequences for Healthy Cities | Road Accident Claims | Driving Crime | Inaccessibility to Transport and Other | Costs of Transport Adaptation | Low Adherence to Active Transport | Excessive Motorized Transport | Congestion | Illegal Occupation | Inappropriate Urban Form | Negative Transport Perceptions | Monofunctional and Disperse Land Use | Increased Waterproof Surface | Fossil Fuels & Energy Dependence | Excessive Carbon Emissions | Atmospheric and Noise Pollution |
| Social exclusion | x | x | x | ||||||||||||
| Difficulty of mobility | x | x | x | x | X | x | x | x | |||||||
| Lack of moderate to strong physical activity | x | x | x | X | x | x | x | x | |||||||
| Respiratory diseases | x | x | x | x | x | x | x | ||||||||
| Cardiovascular diseases | x | x | x | x | x | x | x | ||||||||
| Neurological diseases | x | x | x | x | |||||||||||
| Oncologic diseases | x | x | x | ||||||||||||
| Chronic diseases | x | x | x | x | |||||||||||
| Behavioral and physiological disorders | x | x | x | x | x | x | |||||||||
| Obesity and overweight | x | x | X | x | x | x | |||||||||
| Physical and psychological damages | x | x | x | X | x | x | x | ||||||||
| Mortality rate | x | x | x | x | |||||||||||
| Small sense of community | x | x | x | x | x | x | |||||||||
| Lack of social interaction | x | x | x | X | x | x | x | x | |||||||
| Loss of local amenities | X | x | x | ||||||||||||
| Material and infrastructural costs | X | x | x | x | x | ||||||||||
| Medical and insurance costs | x | x | x | x | |||||||||||
| Time costs | x | x | x | x | |||||||||||
| Fuel costs | x | x | x | x | x | ||||||||||
| Shortage of green spaces and open spaces | x | x | X | x | x | x | x | ||||||||
| Floods | X | x | x | x | |||||||||||
| Water and soil contamination | x | x | x | x | |||||||||||
| Urban heat islands | x | x | X | x | x | x | x | x | x | ||||||
| Global warming | x | x | x | x | x | x | x | x | |||||||
Table 3.
Main intervention axes in sustainable urban mobility for healthy cities. Source: Own source.
Table 3.
Main intervention axes in sustainable urban mobility for healthy cities. Source: Own source.
| Intervention Axes | |
|---|---|
| 1. Healthy and clean behaviors in transport | 8. Land-use planning |
| 2. Integrated transport information supported by Information and Communication Technology (ICT) | 9. Data collection |
| 3. Inclusive, safe, and barrier-free transport system | 10. Legislation |
| 4. Transport speed | 11. Agents and competences |
| 5. Networks, intermodality, and connectivity | 12. Instruments and studies |
| 6. Infrastructures for active modes | 13. Awareness of benefits for health, environment, and economy sectors |
| 7. Transport electrification | |
Table 4.
Selected urban mobility planning instruments according to spatial level and publication year. Source: Own source.
Table 4.
Selected urban mobility planning instruments according to spatial level and publication year. Source: Own source.
| Publication Year | ||||||
|---|---|---|---|---|---|---|
| Level | Before 2010 | 2010 | 2013 | 2015 | 2016 | 2017 |
| Metropolitan | . | . | . | . | LMA 1 | . |
| Inter-municipal | . | . | South LMA 2 | |||
| Municipal | Almada 3 Oeiras 4 | Cascais 5 | Lisboa 6 | Loures 7 | Setúbal 8 | . |
| Local | Mafra 9 | V.F. Xira 10 | . | . | . | . |
1 LMA—Action Plan for Sustainable Urban Mobility in the Lisbon Metropolitan Area (2016); 2 South LMA—Intermunicipal Mobility and Transport Plan of the Area of Influence of the Third Crossing of the Tagus (2013–2017) (this covers the municipalities of Barreiro, Moita, Palmela, Seixal, and Sesimbra); 3 Almada—Accessibilities 21: Almada/Laranjeiro Travel Plan (2002); 4 Oeiras—Study of Mobility and Accessibility in the Municipality of Oeiras (2008); 5 Cascais—Municipal Traffic Study of Cascais (2010–2011); 6 Lisbon—Lisbon’s Pedestrian Accessibility Plan (2013); 7 Loures—Accessibility and Mobility Action Plan—Loures Accessible to All (2015); 8 Setúbal—SUMP Setúbal (2016); 9 Mafra—Mafra Strategic Mobility Plan (2008); 10 V.F. Xira—Municipal Plan for the Promotion of Accessibility in Vila Franca de Xira (2010).
Table 5.
Public health planning instruments according to spatial level. Source: Adapted of [79] (p. 85).
Table 5.
Public health planning instruments according to spatial level. Source: Adapted of [79] (p. 85).
| Level | Public Health Sector |
|---|---|
| National | National Health Plan Priority health programs |
| Regional | Regional health plans Regional health profiles |
| Municipal/Local | Local health plans Health Development Plan Municipal Health Profile |
Table 6.
Local Health Plans in LMA—a synthesis. Source: [96]. ACES: Health Centers Groups.
Table 6.
Local Health Plans in LMA—a synthesis. Source: [96]. ACES: Health Centers Groups.
| ACES | Local Health Plans—References to Urban Mobility |
|---|---|
| Almada-Seixal | Diagnosis—road accidents |
| Amadora | Without any reference |
| Arco Ribeirinho | Indicator system—reference to kilometers of cycling and pedestrian paths |
| Arrábida | Not available |
| Cascais | Without any reference |
| Estuário do Tejo | Not available |
| Lisboa Central | Without any reference |
| Lisboa Norte | Without any reference |
| Lisboa Ocidental—Oeiras | Without any reference |
| Loures—Odivelas | Diagnosis—commuting |
| Sintra | Without any reference |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Louro, A.; Marques da Costa, N.; Marques da Costa, E. Sustainable Urban Mobility Policies as a Path to Healthy Cities—The Case Study of LMA, Portugal. Sustainability 2019, 11, 2929. https://0-doi-org.brum.beds.ac.uk/10.3390/su11102929
AMA Style
Louro A, Marques da Costa N, Marques da Costa E. Sustainable Urban Mobility Policies as a Path to Healthy Cities—The Case Study of LMA, Portugal. Sustainability. 2019; 11(10):2929. https://0-doi-org.brum.beds.ac.uk/10.3390/su11102929
Chicago/Turabian StyleLouro, Ana, Nuno Marques da Costa, and Eduarda Marques da Costa. 2019. "Sustainable Urban Mobility Policies as a Path to Healthy Cities—The Case Study of LMA, Portugal" Sustainability 11, no. 10: 2929. https://0-doi-org.brum.beds.ac.uk/10.3390/su11102929
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.