A Mental Health First Aid Service in an Italian University Public Hospital during the Coronavirus Disease 2019 Outbreak

 , ,
, ,
Abstract
:1. Introduction
1.1. COVID-19 Outbreak and Mental Health
1.2. Psychological First Aid Interventions during Pandemics
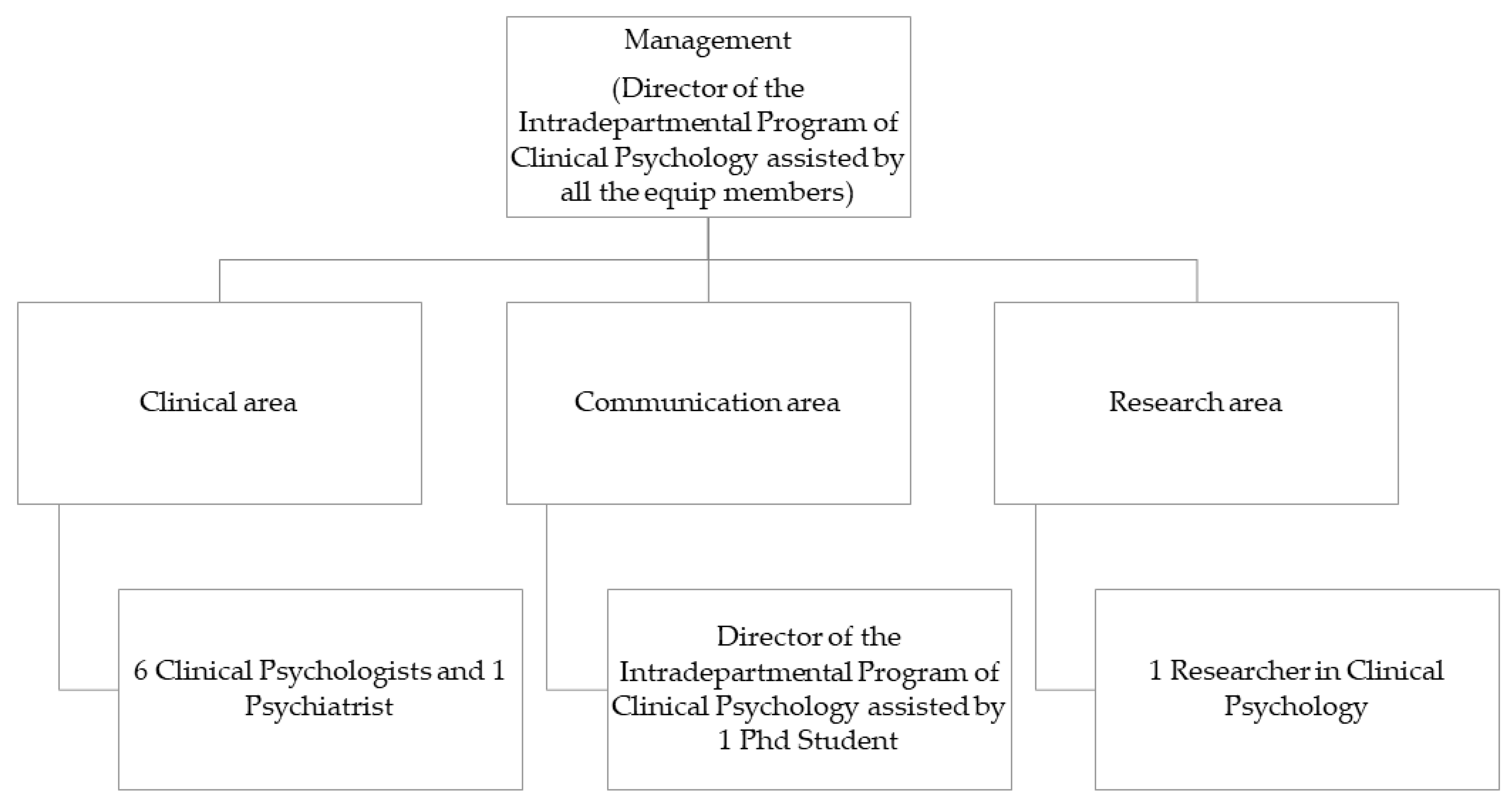
2. The Mental Health First Aid Service of the Federico II University Public Hospital: Architecture of the Service
2.1. Management
2.2. Clinical Area
2.3. Communication Area
2.4. Research Area
3. Current Overview of the Service
3.1. Characteristics of Users
3.2. Clinical Dimensions Detected
3.3. Past, Present, and Future Quality of Life
4. Discussion
5. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Situation Update Worldwide. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 12 May 2020).
- European Centre for Disease Prevention and Control. Situation Update for the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 12 May 2020).
- European Centre for Disease Prevention and Control. Rapid Risk Assessment: Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK–Seventh Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-seventh-update-Outbreak-of-coronavirus-disease-COVID-19.pdf (accessed on 18 April 2020).
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (accessed on 18 April 2020).
- Li, W.; Yang, Y.; Liu, Z.H.; Zhao, Y.J.; Zhang, Q.; Zhang, L.; Cheung5, T.; Xiang, Y.T. Progression of mental health services during the COVID-19 outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 21. [Google Scholar] [CrossRef]
- Brooks, S.H.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiat. Clin. Neuros. 2020, 74, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19 and its impact on HCWs outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Yeager, K.R.; Roberts, A.R. Crisis Intervention Handbook. Assessment, Treatment, and Research, 4th ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Everly, G.S.; Flynn, B.W. Principles and practical procedures for acute psychological first aid training for personnel without mental health experience. Int. J. Emerg. Ment. Health 2006, 8, 93–100. [Google Scholar]
- Shah, K.; Kamrai, D.; Mekala, H.; Mann, B.; Desai, K.; Patel, R.S. Focus on mental health during the Coronavirus (COVID-19) pandemic: Applying learnings from the past outbreaks. Cureus 2020, 12, e7405. [Google Scholar] [CrossRef] [Green Version]
- Everly, G.S.; Barnett, D.J.; Links, J.M. The Johns Hopkins model of psychological first aid (RAPID-PFA): Curriculum development and content validation. Int. J. Emerg. Ment. Health 2012, 14, 95–103. [Google Scholar]
- National Center for Child Traumatic Stress Network and National Center for PTSD, U.S. Department of Veterans Affairs. Psychological First Aid: Field Operations Guide, 2nd ed.; 2006. Available online: http://www.ncptsd.va.gov/ncmain/index.jsp (accessed on 6 May 2020).
- McCabe, O.L.; Everly, G.S., Jr.; Brown, L.M.; Wendelboe, A.M.; Abd Hamid, N.H.; Tallchief, V.L.; Links, J.M. Psychological first aid: A consensus-derived, empirically supported, competency-based training model. Am. J. Public Health 2014, 104, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wu, W.; Zhao, X.; Zhang, W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: A model of West China Hospital. Precis. Clin. Med. 2020, 3, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Corliss, J. Six Relaxation Techniques to Reduce Stress. Harvard Health Publishing, 2019. Available online: https://www.health.harvard.edu/mind-and-mood/six-relaxation-techniques-to-reduce-stress (accessed on 18 April 2020).
- Liu, S.; Yang, L.L.; Zhang, C.X.; Xiang, Y.T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- de Boer, A.G.E.M.; van Lanschot, J.J.B.; Stalmeier, P.F.M.; van Sandick, J.W.; Hulscher, J.B.F.; de Haes, J.C.J.M.; Sprangers, M.A.G. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. 2004, 13, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Irvine, A.; Drew, P.; Bower, P.; Brooks, H.; Gellatly, J.; Armitage, C.J.; Barkham, M.; McMillan, D.; Bee, P. Are there interactional differences between telephone and face-to-face psychological therapy? A systematic review of comparative studies. J. Affect. Disord. 2020, 26, 120–131. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Mason, D.J.; Friese, C.R. Protecting health care workers against COVID-19—And being prepared for future pandemics. JAMA Health Forum 2020, 1, e200353. Available online: https://jamanetwork.com/channels/health-forum/fullarticle/2763478 (accessed on 18 April 2020).
- International Council of Nurses. High Proportion of Healthcare Workers with COVID-19 in Italy Is a Stark Warning to the World: Protecting Nurses and Their Colleagues Must Be the Number One Priority. Available online: https://www.icn.ch/news/high-proportion-healthcare-workers-covid-19-italy-stark-warning-world-protecting-nurses-and (accessed on 18 April 2020).
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Jiang, X.; Deng, L.; Zhu, Y.; Ji, H.; Tao, L.; Liu, L.; Yang, D.; Ji, W. Psychological crisis intervention during the outbreak period of new coronavirus pneumonia from experience in Shanghai. Psychiatry Res. 2020, 286, 112903. [Google Scholar] [CrossRef]
- WHO and the International Labour Organization. Occupational Safety and Health in Public Health Emergencies: A Manual for Protecting Health Workers and Responders. Available online: https://www.who.int/occupational_health/Web_OSH_manual.pdf (accessed on 18 April 2020).
- International Federation of Red Cross and Red Crescent Societies. Mental Health and Psychosocial Support for Staff, Volunteers and Communities in an Outbreak of Novel Coronavirus. 2020. Available online: https://pscentre.org/wp-content/uploads/2020/02/MHPSS-in-nCoV-2020_ENG-1.pdf (accessed on 18 April 2020).
- Yeager, K.R. Trauma support services for healthcare workers: The Stress, Trauma and Resilience (STAR) program. In Crisis Intervention Handbook. Assessment, Treatment, and Research, 4th ed.; Yeager, K.R., Roberts, A.R., Eds.; Oxford University Press: New York, NY, USA, 2015; pp. 609–633. [Google Scholar]
- Dewey, C.; Hingle, S.; Goelz, E.; Linzer, M. Supporting clinicians during the COVID-19 pandemic. Ann. Intern. Med. 2020. Epub ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Sultana, A.; Sharma, R.; Hossain, M.D.M.; Bhattacharya, S.; Purohit, N. Burnout among healthcare providers during COVID-19 pandemic: Challenges and evidence-based interventions. SocArXiv 2020. Available online: https://ideas.repec.org/p/osf/socarx/4hxga.html (accessed on 7 May 2020). [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinical Reasons | Health-Care Professionals | General Population | χ2 |
|---|---|---|---|
| n(%) | n(%) | ||
| Anxiety symptoms | 13(43.3) | 56(53.3) | 0.95 |
| Loneliness | 4(13.3) | 31(23.5) | 2.78 * |
| Depressive symptoms | — | 28(26.6) | — |
| Fear of contagion | 15(50) | 8(7.6) | 20.25 *** |
| Stress symptoms | 3(10) | 19(18.1) | 1.65 |
| Sleep disorders | 1(3.3) | 18(17.1) | 2.63 |
| Trauma | — | 16(15.2) | — |
| Social disease | — | 11(10.5) | — |
| Suicidal ideation | — | 7(6.6) | — |
| Psychomotor agitation | 2(6.6) | 3(2.8) | 0.86 |
| Total | General Population | Health-Care Professionals | |
|---|---|---|---|
| QoL | M(SD) | M(SD) | M(SD) |
| Past QoL | 6.62(2.32) | 6.60(2.38) | 6.71(2.14) |
| Present QoL | 4.02(2.51) | 4.01(2.59) | 4.05(2.28) |
| Future QoL | 7.29(2.15) | 7.64(1.28) | 6.12(1.32) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maldonato, N.M.; Bottone, M.; Chiodi, A.; Continisio, G.I.; De Falco, R.; Duval, M.; Muzii, B.; Siani, G.; Valerio, P.; Vitelli, R.; et al. A Mental Health First Aid Service in an Italian University Public Hospital during the Coronavirus Disease 2019 Outbreak. Sustainability 2020, 12, 4244. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104244
Maldonato NM, Bottone M, Chiodi A, Continisio GI, De Falco R, Duval M, Muzii B, Siani G, Valerio P, Vitelli R, et al. A Mental Health First Aid Service in an Italian University Public Hospital during the Coronavirus Disease 2019 Outbreak. Sustainability. 2020; 12(10):4244. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104244
Chicago/Turabian StyleMaldonato, Nelson Mauro, Mario Bottone, Alessandro Chiodi, Grazia Isabella Continisio, Raffaella De Falco, Marzia Duval, Benedetta Muzii, Gerarda Siani, Paolo Valerio, Roberto Vitelli, and et al. 2020. "A Mental Health First Aid Service in an Italian University Public Hospital during the Coronavirus Disease 2019 Outbreak" Sustainability 12, no. 10: 4244. https://0-doi-org.brum.beds.ac.uk/10.3390/su12104244