Immediate Impact of the COVID-19 Confinement on Physical Activity Levels in Spanish Adults

 ,
, 
 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Survey
2.2. Physical Activity
2.3. Demographic Characteristics
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 51. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 22 March 2020).
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 69. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200329-sitrep-69-covid-19.pdf?sfvrsn=8d6620fa_8 (accessed on 29 March 2020).
- Ministerio de Sanidad, Consumo y Bienestar Social. Enfermedad por Nuevo Coronavirus, COVID-19: Situación Actual. Actualización no 60; 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/situacionActual.htm (accessed on 30 March 2020).
- Gobierno de España. 2020. Available online: https://www.lamoncloa.gob.es/ (accessed on 22 March 2020).
- Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el Estado de Alarma para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. 2020. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-3692 (accessed on 22 March 2020).
- Consejo Superior de Deportes. 2020. Available online: https://www.csd.gob.es/es/la-campana-yomemuevoencasa-del-csd-y-el-consejo-colef-recuerda-la-importancia-de-mantener-un-estilo-de-vida-activo-durante (accessed on 24 March 2020).
- Schaefer, L.; Plotnikoff, R.C.; Majumdar, S.R.; Mollard, R.; Woo, M.; Sadman, R.; Rinaldi, R.L.; Boulé, N.; Torrance, B.; Ball, G.D.C.; et al. Outdoor time is associated with physical activity, sedentary time, and cardiorespiratory fitness in youth. J. Pediatr. 2014, 165, 516–521. [Google Scholar] [CrossRef]
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Inglés, E. Benefits of outdoor sports for society. A systematic literature review and reflections on evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar] [CrossRef] [Green Version]
- Wetmore, C.M.; Ulrich, C.M. Mechanisms associating physical activity with cancer incidence: Exercise and immune function. In Cancer Prevention And Management through Exercise and Weight Control; McTiernan, A., Ed.; CRC Press: Los Angeles, CA, USA, 2006; pp. 157–176. [Google Scholar]
- Gleeson, M. Immune function in sport and exercise. J. Appl. Physiol. 2007, 103, 693–699. [Google Scholar] [CrossRef] [Green Version]
- Mazzeo, R.S. Altitude, exercise and immune function. Exerc. Immunol. Rev. 2005, 11, 6–16. [Google Scholar] [PubMed]
- Woods, J.A.; Lowder, T.W.; Keylock, K.T. Can exercise training improve immune function in the aged? Ann. N. Y. Acad. Sci. 2002, 959, 117–127. [Google Scholar] [CrossRef]
- Woods, J.A.; Davis, J.M.; Smith, J.A.; Nieman, D.C. Exercise and cellular innate immune function. Med. Sci. Sports Exerc. 1999, 31, 5–66. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J.; Shek, P.N. Exercise, immunity, and susceptibility to infection: A J-shaped relationship? Phys. Sportsmed. 1999, 27, 47–71. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.M. Exercise, immunology and upper respiratory tract infections. Int. J. Sports Med. 1997, 18, S69–S77. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Heal. Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Hamer, M.; Donovan, G.O.; Stamatakis, E. Lifestyle risk factors, obesity and infectious disease mortality in the general population: Linkage study of 97,844 adults from England and Scotland. Prev. Med. Baltim. 2019, 123, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Vider, J.; Lehtmaa, J.; Kullisaar, T.; Vihalemm, T.; Zilmer, K.; Kairane, A.; Landõr, A.; Karu, T.; Zilmer, M. Acute immune response in respect to exercise-induced oxidative stress. Pathophysiology 2001, 7, 263–270. [Google Scholar] [CrossRef]
- Baik, I.; Curhan, G.C.; Rimm, E.B.; Bendich, A.; Willet, W.C.; Fawzi, W.W. A prospective study of age and lifestyle factors in relation to community-acquired pneumonia in US men and women. Arch. Intern. Med. 2000, 160, 3082–3088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo Clinic. Coronavirus Disease 2019 (COVID-19). Available online: https://www.mayoclinic.org/diseases-conditions/coronavirus/symptoms-causes/syc-20479963 (accessed on 22 March 2020).
- Calati, R.; Ferrari, C.; Brittner, M.; Oasi, O.; Olié, E.; Carvalho, A.F.; Courtet, P. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. J. Affect. Disord. 2019, 245, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santini, Z.I.; Jose, P.E.; York Cornwell, E.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Heal. 2020, 5, e62–e70. [Google Scholar] [CrossRef] [Green Version]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1.2 million individuals in the USA between 2011 and 2015: A cross-sectional study. The Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef]
- Cao, C.; Liu, Q.; Yang, L.; Zheng, X.; Lan, P.; Koyanagi, A.; Vancampfort, D.; Soysal, P.; Veronese, N.; Stubbs, B.; et al. Handgrip strength is associated with suicidal thoughts in men: Cross-sectional analyses from NHANES. Scand. J. Med. Sci. Sports 2019, 30, 1–8. [Google Scholar] [CrossRef]
- Peluso, M.A.M.; Guerra de Andrade, L.H.S. Physical activity and mental health: The association between exercise and mood. Clinics 2005, 60, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Martinsen, E.W. Physical activity in the prevention and treatment of anxiety and depression. Nord. J. Psychiatry 2008, 62, 25–29. [Google Scholar] [CrossRef]
- Szabo, A. Acute psychological benefits of exercise performed at self-selected workloads: Implications for theory and practice. J. Sport Sci Med. 2003, 2, 77–87. [Google Scholar]
- Fleming, K.M.; Campbell, M.; Herring, M.P. Acute effects of Pilates on mood states among young adult males. Complement. Ther Med. 2020, 49, 102313. [Google Scholar] [CrossRef] [PubMed]
- Morgan, W.P.; Horstman, D.H. Anxiety reduction following acute physical activity. Psychiatr. Ann. 1979, 9, 36–45. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2014. Available online: https://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (accessed on 22 March 2020).
- López-Sánchez, G.F.; Pardhan, S.; Trott, M.; Sánchez-Castillo, S.; Jackson, S.E.; Tully, M.; Gorely, T.; López-Bueno, R.; Veronese, N.; Skalska, M.; et al. The Association Between Physical Activity and Cataracts Among 17,777 People Aged 15–69 Years Residing in Spain. Ophthalmic Epidemiol. 2020, 27, 272–277. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, 1628–1654. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, J.L.J.; Joy, E.A.; Stanford, J.B. The Physical Activity Vital Sign: A Primary Care Tool to Guide Counseling for Obesity. J. Phys. Act. Heal. 2010, 7, 571–576. [Google Scholar] [CrossRef]
- Schrempft, S.; Jackowska, M.; Hamer, M.; Steptoe, A. Associations between social isolation, loneliness, and objective physical activity in older men and women. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. On Behalf of the ECLB-COVID19 Consortium. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- European Commission. Special Eurobarometer 472 Report Sport and Physical Activity Fieldwork. 2018. Available online: http://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/survey (accessed on 23 March 2020).
- Fernandez-Navarro, P.; Aragones, M.T.; Ley, V. Leisure-time physical activity and prevalence of non-communicable pathologies and prescription medication in Spain. PLoS ONE 2018, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäkinen, T.E.; Sippola, R.; Borodulin, K.; Rahkonen, O.; Kunst, A.; Klumbiene, J.; Regidor, E.; Ekholm, O.; MacKenbach, J.; Prättälä, R. Explaining educational differences in leisure-time physical activity in Europe: The contribution of work-related factors. Scand. J. Med. Sci. Sport 2012, 22, 439–447. [Google Scholar] [CrossRef]
- Mohammad Ali, S.; Lindström, M. Psychosocial work conditions, unemployment, and leisure-time physical activity: A population-based study. Scand. J. Public Health 2006, 34, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Seifert, A.; Schlomann, A.; Rietz, C.; Schelling, H.R. The use of mobile devices for physical activity tracking in older adults’ everyday life. Digit. Heal. 2017, 3, 205520761774008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ga, R.; May, A.M.; van Overmeeren, E.J.; Simons, M.; Monninkhof, E.M. The Effect of Physical Activity Interventions Comprising Wearables and Smartphone Applications on Physical Activity: A Systematic Review and Meta-analysis. Sport Med. Open 2018, 4, 42. [Google Scholar] [CrossRef]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Hämmig, O. Health risks associated with social isolation in general and in young, middle and old age. PLoS ONE 2019, 14, e0219663. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.; Steptoe, A.; Chen, L.J.; Chen, Y.H.; Lin, C.H.; Ku, P.W. Social Isolation, Loneliness, and All-Cause Mortality in Patients With Cardiovascular Disease: A 10-Year Follow-up Study. Psychosom. Med. 2020, 82, 208–214. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health—A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Lima, C.K.T.; de Medeiros Carvalho, P.M.; Lima, I.D.A.S.; de Oliveira Nunes, J.V.A.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| n | % | Weekly PA Minutes before Isolation Mean ± SD | Weekly PA Minutes during Isolation Mean ± SD | Difference of Weekly PA Minutes (before and during Isolation) ± SD | t | df | p Value a | db | p Value c | |
|---|---|---|---|---|---|---|---|---|---|---|
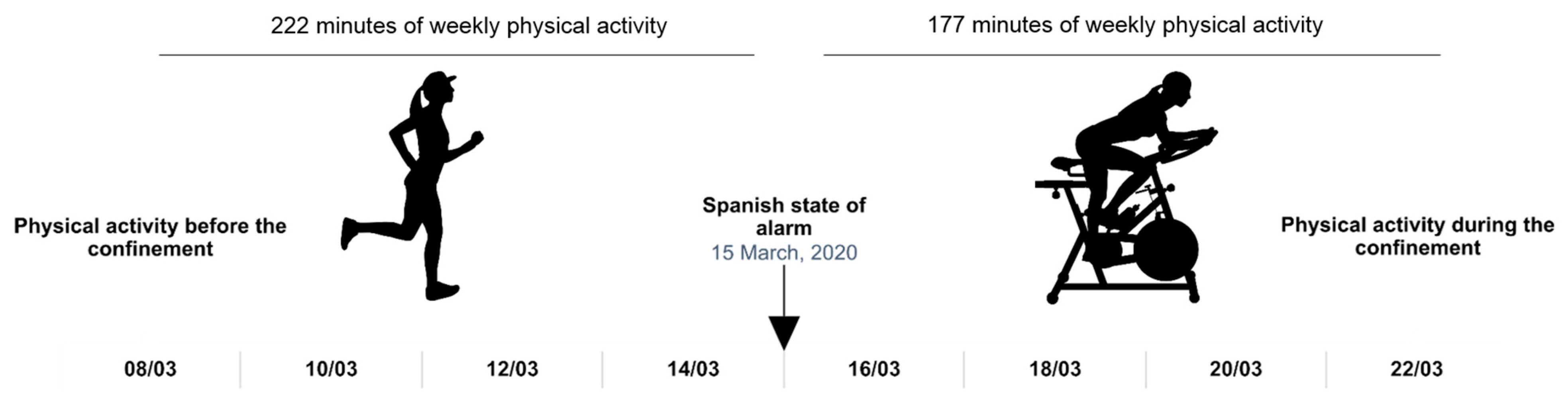
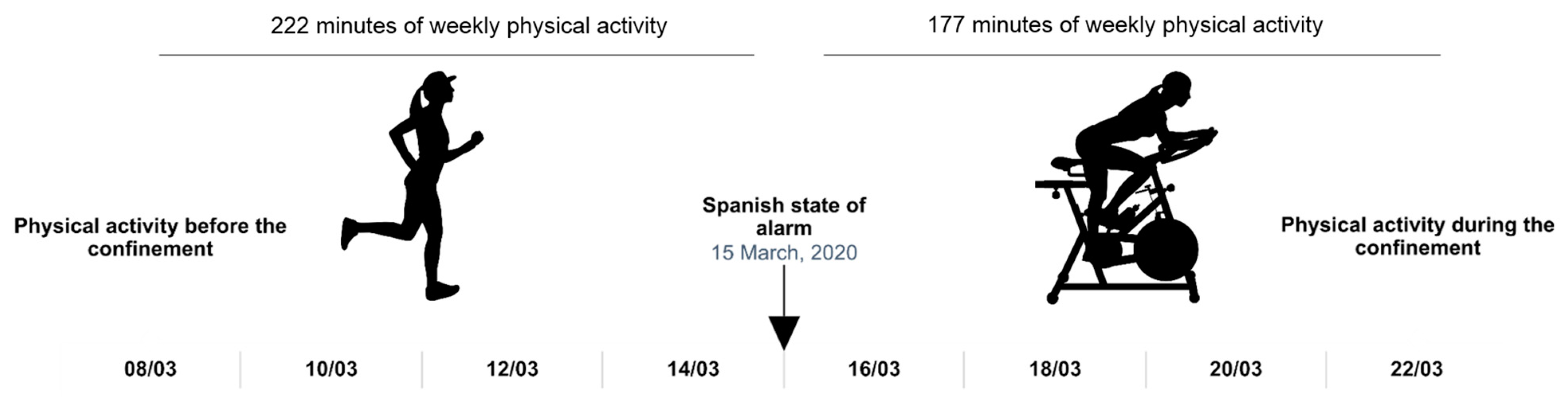
| Overall | 2042 | 221.9 ± 193.6 | 176.7 ± 178.9 | 45.2 ± 179.9 | 11.3486 | 2041 | <0.0001 | 0.2424 | ||
| Gender | <0.0001 | |||||||||
| Men | 938 | 45.9 | 268.8 ± 207.1 | 196.0 ± 185.0 | 72.9 ± 177.0 | 12.5392 | 937 | <0.0001 | 0.3703 | |
| Women | 1104 | 54.1 | 182.0 ± 171.7 | 160.4 ± 171.2 | 21.7 ± 178.3 | 4.0381 | 1103 | <0.0001 | 0.1264 | |
| Age | 0.1074 | |||||||||
| <43 years | 1441 | 70.6 | 238.4 ± 201.4 | 196.4 ± 181.9 | 42.0 ± 183.0 | 8.7093 | 1440 | <0.0001 | 0.2188 | |
| ≥43 years | 601 | 29.4 | 182.4 ± 167.3 | 129.6 ± 162.4 | 52.8 ± 172.1 | 7.5255 | 600 | <0.0001 | 0.3205 | |
| Civil status | 0.1951 | |||||||||
| Married | 1001 | 49.0 | 210.1 ± 187.6 | 161.4 ± 170.6 | 48.7 ± 173.7 | 8.8637 | 1000 | <0.0001 | 0.2715 | |
| Not married | 1041 | 51.0 | 233.2 ± 198.8 | 191.4 ± 185.5 | 41.8 ± 185.7 | 7.2681 | 1040 | <0.0001 | 0.2176 | |
| Education | 0.0011 | |||||||||
| University degree | 1293 | 63.3 | 217.2 ± 180.7 | 181.3 ± 174.4 | 36.0 ± 174.2 | 7.4155 | 1292 | <0.0001 | 0.2023 | |
| No University degree | 749 | 36.7 | 221.9 ± 180.7 | 168.8 ± 186.4 | 61.2 ± 188.4 | 8.8845 | 748 | <0.0001 | 0.3048 | |
| Occupation | 0.0249 | |||||||||
| Employed | 1287 | 63.0 | 205.0 ± 180.0 | 165.6 ± 168.7 | 39.2 ± 175.2 | 8.0281 | 1286 | <0.0001 | 0.2247 | |
| Not employed | 755 | 37.0 | 251.0 ± 212.0 | 195.6 ± 193.7 | 55.4 ± 187.4 | 8.1205 | 754 | <0.0001 | 0.2728 |
| WHO before | WHO isolated | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | Difference | χ2 | df | p Value a | db | |
| Overall | 1238 | 60.6 | 999 | 48.9 | 11.7 | 16.67 | 1 | <0.0001 | 0.2367 |
| Gender | |||||||||
| Men | 662 | 70.6 | 502 | 53.5 | 17.1 | 94.12 | 1 | <0.0001 | 0.3569 |
| Women | 576 | 52.2 | 497 | 45.0 | 7.2 | 17.19 | 1 | <0.0001 | 0.1435 |
| Age | |||||||||
| <43 years | 928 | 64.4 | 792 | 55.0 | 9.4 | 43.42 | 1 | <0.0001 | 0.1932 |
| ≥43 years | 310 | 51.6 | 207 | 34.4 | 17.2 | 50.76 | 1 | <0.0001 | 0.3512 |
| Civil status | |||||||||
| Married | 593 | 59.2 | 461 | 46.1 | 13.1 | 52.80 | 1 | <0.0001 | 0.2663 |
| Not married | 645 | 61.0 | 538 | 51.7 | 9.3 | 37.54 | 1 | <0.0001 | 0.2085 |
| Education | |||||||||
| University degree | 798 | 61.7 | 667 | 51.6 | 10.1 | 42.37 | 1 | <0.0001 | 0.2054 |
| No University degree | 440 | 58.7 | 332 | 44.3 | 14.4 | 50.71 | 1 | <0.0001 | 0.2914 |
| Occupation | |||||||||
| Employed | 750 | 58.3 | 606 | 47.1 | 11.2 | 52.36 | 1 | <0.0001 | 0.2254 |
| Not employed | 488 | 64.6 | 393 | 52.1 | 12.5 | 37.76 | 1 | <0.0001 | 0.2572 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Balsalobre-Fernández, C.; Casaña, J.; Casajús, J.A.; Smith, L.; López-Sánchez, G.F. Immediate Impact of the COVID-19 Confinement on Physical Activity Levels in Spanish Adults. Sustainability 2020, 12, 5708. https://0-doi-org.brum.beds.ac.uk/10.3390/su12145708
López-Bueno R, Calatayud J, Andersen LL, Balsalobre-Fernández C, Casaña J, Casajús JA, Smith L, López-Sánchez GF. Immediate Impact of the COVID-19 Confinement on Physical Activity Levels in Spanish Adults. Sustainability. 2020; 12(14):5708. https://0-doi-org.brum.beds.ac.uk/10.3390/su12145708
Chicago/Turabian StyleLópez-Bueno, Rubén, Joaquín Calatayud, Lars L. Andersen, Carlos Balsalobre-Fernández, José Casaña, José A. Casajús, Lee Smith, and Guillermo F. López-Sánchez. 2020. "Immediate Impact of the COVID-19 Confinement on Physical Activity Levels in Spanish Adults" Sustainability 12, no. 14: 5708. https://0-doi-org.brum.beds.ac.uk/10.3390/su12145708