1. Introduction
Medical education contributes significantly to the vision for Sustainability in Health. In our times, with the COVID-19 pandemic wide-spreading worldwide, the necessity to empower health experts with knowledge, skills, and competencies is a key priority for the management of healthcare. Furthermore, the increase in the positive motivation of health specialists and their willingness to promote their social role and the impact of their professional conduct is associated with various psychological factors like burnout or job satisfaction. The development of high-skilled experts with mental health and increased satisfaction from their work must be set as a key objective towards achieving Sustainable Health.
From a managerial point of view, Sustainable Health also requires the design, implementation, and continuous monitoring of benchmarks and Key Performance Indicators (KPIs) capable of offering a trusted, sustainable, and reliable set of measurements for performance monitoring.
Within this context, the assessment of medical Training Programs and the evaluation of their added value must be a strategic initiative for empowerment and sustainability. The development of medical competence through training and education is a bold action. Our research study is focusing on Residency Training Programs in the Kingdom of the Saudi Arabia supervised by the Saudi Commission for the Health Specialties.
Residency or postgraduate training is a stage of graduate medical education. Residents are trainees who are enrolled in programs recognized by the Saudi Commission for Health Sciences (SCFHS) and are fulfilling the requirements for primary discipline certification or a certification of special competence. A resident refers to a qualified physician, podiatrist, dentist, optometrist, veterinarian, or pharmacist who practices medicine, usually in a hospital or clinic, under the direct or indirect supervision of a senior clinician registered in that specialty such as an attending physician or consultant.
In
Section 2, we provide a thorough critical literature review on the concept of Job Satisfaction and we present various research studies that contribute to our research problem specification. The SCFHS has a main responsibility to deliver high quality Training Programs to approximately 18,000 health specialists in the Kingdom of Saudi Arabia. It also supervises numerous training centers and academic programs with a critical objective to deliver value to the Health System and to the Society of the Kingdom. This value-driven strategy of SCFHS has an impact on all the activities undertaken by the institution.
In total, 1200 programs are conducted across Saudi Arabia and other countries in the Gulf region covering 79 health specialties [
1]. One of the key strategic aims of the SCFHS is also to design, implement, and monitor a quality assurance system for the execution of all its Training Programs and also to access the efficiency of this system to enhance the update of strategies and policies. In this context, the SCFHS also supervises the quality of the implementation of residency medical Training Programs.
Trainees’ satisfaction is a multidimensional concept that has been associated with environmental factors and is predicted by intrinsic (personal growth and perceived ability to work) and extrinsic (perceived social support) forms of motivation. The objective of this study is to evaluate the trainees’ satisfaction level and to investigate its association with various features, including the quality of Training Programs.
The study of the trainees’ satisfaction is part of a multi-dimensional research strategy in the Saudi Commission of Health Specialties. The SCFHS is deploying a value-driven strategy for the integration of research-based evidence to the quality of its Training Programs. It also collects and processes significant data related to the various Training Programs and their evaluations towards enhanced decision making. Various data are related to key aspects of the residents’ perceptions related to the quality of the Training Program and institutions, as well as the self-assessments by the trainees of various psychological aspects of their educational and professional activities.
A continuous quality assurance strategy is in place focusing on different complementary aspects of medical training. In a recent study, we introduced the SCFHS Framework for Sustainable Medical Education and we introduced 23 integrated Key Performance Indicators for Implementing an Innovative Approach to Advance the Quality of Training Programs at the Saudi Commission for Health Specialties. Other strategic goals include the measurement of the effectiveness of online-training strategies, as well as the deep understanding and interpretation of human factors involved in medical education. For examples, recently we delivered research on the impact of the COVID-19 pandemic on the anxiety and depression of residents in medical Training Programs.
In
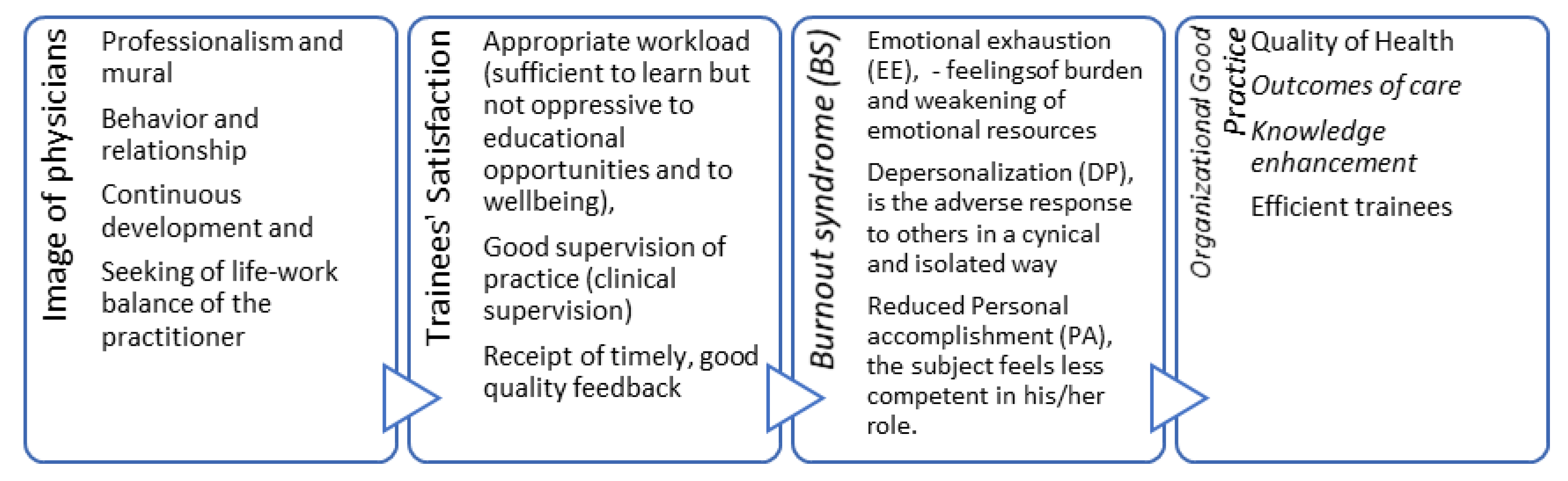
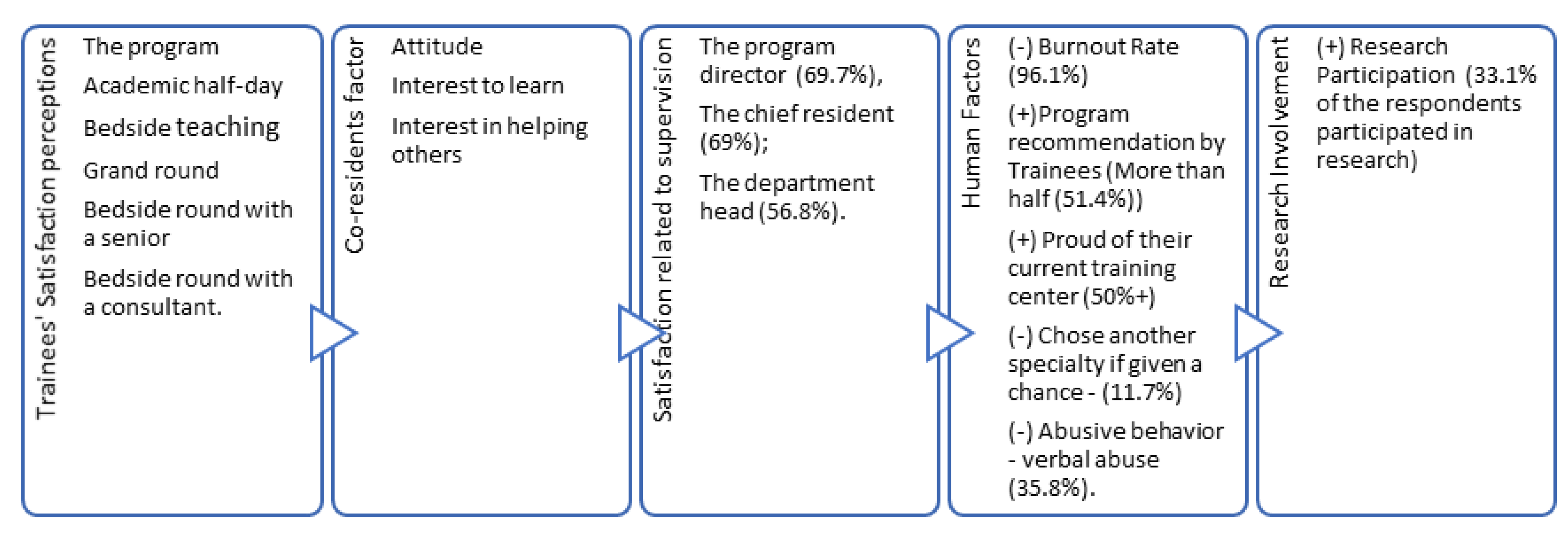
Figure 1 below, we summarize some of the key aspects of our research problem. The main motivation of our research is the direct association of four integrative pillars in training and professional life of residents. According to the literature that is presented below, the image of physicians has two critical components: the continuous development, and the seeking of life-work balance of the trainee/resident. Thus, the training satisfaction remains a core aspect of efficiency of Training Programs. The intention of our research is to analyze how specific aspects of trainee satisfaction lead to inefficiencies in medical Training Programs and their impact based on international benchmarks and our research approach.
Furthermore, we also focused on psychological factors, including the burnout syndrome of residents, as a key variable for the understanding of trainees’ satisfaction. Our ultimate objective is to analyze and to propose enhancements on organizational good practices, and to lead innovative plans and strategies for the beneficiaries of Training Programs of the SCFHS.
As the image of physicians has always been associated with high levels of professionalism, it is notable that values, behavior, and relationships are the main factors that sustain this image in the eyes of people. These factors can be maintained by continuous development and the seeking of a life-work balance of the practitioner. Maintenance of this balance can lead to satisfaction [
2].
Studies reported that trainee satisfaction has a major impact on their knowledge enhancement and outcomes of care. Also, this directly affects their education and maintenance of good organizational practices [
3].
In a study conducted to measure the satisfaction of UK junior doctors (medical post graduate students), factors of “appropriate workload (sufficient to learn but not oppressive to educational opportunities and to wellbeing), good supervision of practice (clinical supervision) and the receipt of timely, good quality feedback” were found to be correlated with trainee satisfaction. Moreover, assignment of an appropriate workload was found to the most crucial factor affecting the satisfaction of trainees, followed by the remaining factors prospectively. A high level of dissatisfaction was reported by junior doctors assigned to work in environments with a high workload and this led to the appearance of burnout symptoms in many cases [
3,
4]. According to [
5], burnout syndrome (BS) is a set of psychological symptoms resulting from the interaction between chronic occupational stress and individual factors. The syndrome is characterized by emotional exhaustion, depersonalization, and reduced personal achievement [
5]. Emotional exhaustion (EE) indicates the feelings of burden and the weakening of emotional resources; depersonalization (DP) entails responding to others, such as associates and patients, in a cynical and isolated way; reduced personal accomplishment (PA) occurs when the subject feels less competent in his/her role. These factors validate the importance of addressing the problem of burnout as fast as it occurs at all levels (training, education, and practice). As discussed in relevant literature, addressing of the problem can be defined into four main actions: distinguish its existence, address its prevalence and strength, and then perform the preventive and treatment strategy, this should then be followed by periodic measurement of all implemented strategies’ effectiveness [
6].
This article is organized as follows: In
Section 2, we provide an overview of our critical constructive review on the key aspects of our research phenomenon.
Then in
Section 3, we summarize our research methodology and we communicate our research objectives. In
Section 4, we provide analysis of the results and the key findings of our research. In
Section 5, we discuss the contribution and the implications of our work towards Sustainable Health. We also in parallel build our key theoretical contribution, the progressive model for Trainees’ Satisfaction in Medical Education for Sustainable Health. Finally, in
Section 6, we provide they key conclusions and future research directions.
2. Critical Literature Review on Trainee Satisfaction in Training Programs
The recent literature on medical training and healthcare workers research deals extensively with human and psychological factors of trainees, residents, and healthcare workers overall. Various recent studies explain the phenomenon and provide useful insights for our research. Trainee satisfaction appears to be a well discussed human soft factor in diverse studies on medical training. It is also a key variable in broader studies in other research and professional domains. According to literature, several integrated studies focus on the analysis of job satisfaction, professional burnout, the work environment, and health issues. Also, the recent pandemic of COVID-19 has led to new research on the further impact of the pandemic on the traditional human factors of healthcare workers, doctors, and residents. In
Table 1, below, we provide an overview of 13 recent studies on the phenomenon.
In
Table 2 below, we provide the overview of various research studies related to our research problem. A brief discussion and elaboration on the key aspects of our research problem that is anchored in the selected studies is provided in the next few paragraphs.
Alsubaiea and Isouard [
7] provide a meta-research analysis of four studies related to job satisfaction, and retention of Saudi nursing staff. The previous four studies involved 2362 nurses in Saudi Arabia, with a rather good rate of job satisfaction but limited job retention. In our research, we need to investigate the value adding components of residents in Training Programs supervised by the SCFHS. We also intend to develop a set of benchmarks for the relevant components of job satisfaction.
Chen et al. [
8] conducted a study on 39 doctors from five township hospitals in Guangxi Zhuang, China. The goal was to understand the level of job satisfaction of doctors and to make recommendations for improvements. The key findings of their research highlight that job satisfaction is associated with numerous factors including working conditions, financial rewards, and the doctor’s relationships with patients. As a key policy making proposition, the study suggests that the increasing of income and fringe benefits of healthcare workers will have a positive impact on job satisfaction. Additionally, enhanced training and more opportunities for continuous improvement are set as key reflective actions against unsatisfactory conditions. In our research study, we want to obtain a rich picture of the phenomenon in the large population of residents in Saudi Arabia and to reveal some key positive and negative relationships of job satisfaction with specific factors. As a responsive action, our research also aims to provide key recommendation for improvement. We are also very much interested in developing a trusted way and mechanism to monitor the evolution of job satisfaction on residency medical programs.
In another recent study in KSA (Kingdom of Saudi Arabia), Bawakid et al. [
9] conducted a study with 237 Family Physicians (FPs) working in primary healthcare centers under the Ministry of Health in two regions (Jeddah and the Eastern region). In the key findings of their research, it was evident that more than half of the FPs were satisfied in terms of their professional conduct. The majority though had a perception of being inferior to other specialties. As a bold recommendation, the relevant study proposed that the enhancement of self-esteem as well as the continuous support and improvement of the working environment, would limit stress and improve the health and psychological loads of physicians. In our research study, we need to understand the basic “cause and effect” relationships between job satisfaction and aspects of the psychological load of residents, including aspects of the Training Program and educational activities as well as the impact of burnout on satisfaction.
Zhang [
10] conducted a recent research study with a sample of 304 healthcare staff (doctors, nurses, radiologists, technicians, etc.) in China during COVID-19 with an emphasis on the revealing of psychological pressure on their professional conduct and job satisfaction including through stress, anxiety, and depression. In the key findings of this research, it was found that a significant portion of this staff faced high levels of anxiety (28.0%), depression (30.6%), and distress (20.1%). Several demographics and factors related to the provision of personal protection equipment were associated negatively with job satisfaction. In our research study, we are also interested in analyzing the psychological factors that affect job satisfaction. We also in parallel run a complimentary study that focuses on the analysis of depression and anxiety in the context of the professional and educational activities of the residents in training centers.
In their study that conducted in Spring 2013 (n = 556) and Spring 2020 at the peak of the pandemic in Eastern Europe (n = 781) in Slovenia, Leskovic et al. [
11] concluded that the COVID-19 pandemic significantly increased the burnout syndrome faced by nursing homes healthcare workers in Slovenian rural areas. In their study, they also dealt with job satisfaction and they proved that there is a direct association a predicting capability for the burnout syndrome. Additionally, they observed a negative correlation between job satisfaction in 2020 and feelings of emotional exhaustion and personal accomplishment in both 2013 and 2020. These findings also anchor our research in the relevant literature. As we explained, it is a key priority in our research to reveal hermeneutic factors for the job satisfaction of residents.
Soto–Rubio et al. [
12] delivers integrated research in Spain that involved 125 nurses. In their key findings, they emphasize that emotional intelligence serves as a positive favorable effect on job satisfaction. This is one more interesting anchor for our study. We are also interested in understanding which aspects of the mental capabilities and skills of residents can work against psychological pressure and dissatisfaction stemming from the professional and academic conduct of residents.
Aoyagi et al. [
13] performed a meta-analysis and narrative synthesis of available research and found out that respondents’ willingness to work ranged from 23.1% to 95.8%, depending on their work context. A variety of factors determine an increased willingness to work and these include full-time employment, perceived personal safety, awareness of pandemic risk and clinical knowledge of influenza pandemics, role-specific knowledge, pandemic response training, and confidence in personal skills. In our research, we need to understand the motivation of residents to perform effectively as trainees and to understand how job satisfaction is associated with specific motivational factors.
Liu et al. [
14]’s study of job satisfaction through a survey of 897 doctors from 11 tertiary public hospitals in Shanghai, China revealed that 64.8% of participants were dissatisfied with their jobs. A variety of factors were determined to have a direct relationship with dissatisfaction including professional title, the types of patients that doctors treated or expected to treat, as well as their work stress. In our research, the main interest is on the study of job satisfaction of residents and this differentiates our work from many other related works. Our survey is one of the first covering such a major population of residents.
Various other research studies contribute also to the domain of knowledge of job satisfaction and healthcare workers, nurses, physicians, licensed professionals, and social health activists of frontline nurses [
15,
16,
17,
18,
19]. For example, in [
15] a list of factors for the job satisfaction of nurses includes the following components: (satisfaction from the manager; satisfaction from the management administration; satisfaction with the ways of working; satisfaction of recognition; satisfactory working hours; satisfactory working security; self-satisfaction towards productivity; self-satisfaction of initiatives; self-satisfaction of working; self-satisfaction of quality improvements). Last but not least, a recent study during the COVID-19 pandemic [
19] proved that COVID-19 has an increased impact on the level of fear that is also associated with decreased job satisfaction and increased psychological distress, among other implications.
Some further aspects for the anchors of our study to the literature are discussed in the next paragraphs. These provide some more directions for the design of our research tools and the key objectives of our research.
In a global systematic review study focused on the correlation between residents’ burnout rate and their specialty, the highest prevalence of burnout was found to be among residents of radiology, neurology, and general surgery. In contrast, residents with the specialties of psychiatry, oncology, and family medicine were found to have the lowest level of burnout. Also, the same study reported the highest levels of burnout being experienced among males and older residents [
20].
The presence of life-work balance and meaning in work were found to be associated with lower levels or the absence of burnout and was associated with career satisfaction among residents [
21]. In a study of the prevalence of burnout among pediatric residents, burnout found to have a negative impact on the medical knowledge quality of care and professional conduct [
22].
Studies reported higher levels of depression among medical students when compared to the normal population; recommendations to focus on students’ psychological well-being and faculty support were raised. In the same vein, the advantages of including well-being as a curriculum area in addition to skills of stress management was highlighted [
23]. A systematic review focused on identifying factors affecting psychological well-being listed sleep, resilience, residents’ independence, building competence, and enhanced social relatedness as the main factors influencing residents’ well-being and requiring further focus and research [
24].
Psychological well-being featured in a study focused on measuring the burnout among 2nd year U.S. residents and regret towards career choices; the study found that a higher prevalence of burnout existed among the population associated with regret towards their career choices. Furthermore, the study recommended further research on this topic [
25].
The effect of burnout is not limited to the medical trainee only; it also affects patients under treatment and the community. It plays a role in medical error as well as patient dissatisfaction. Studies urge prompt intervention; such interventions might be as simple as the limitation of working hours and mindfulness training [
26].
In a national level study, physicians’ burnout, exhaustion, and work unit safety were found to be associated with major medical errors, and prompt intervention was requested to minimize the medical error through addressing physicians’ well-being and unit safety, as well by the assessment and modification of workload and alleviating the exhaustion of medical trainees and physicians [
27]. Some studies found that self-blame is higher in female residents, which leads to resident distress [
28].
A systematic review analysis conducted on the effect on different interventions on the level of trainees burnout and emotional exhaustion found that the limitation of working hours to the Accreditation Council for Graduate Medical Education (ACGME) work hour limits were associated with improvements in avoiding emotional exhaustion and burnout [
29].
Physician wellness has a great significant impact on patient satisfaction, long-term physician satisfaction, and increased physician productivity. Therefore, medical educators, academic leaders, and researchers are focusing on the initiative of ‘improving trainee well-being’ or on satisfaction and analyzing burnout [
26].
Management and dealing with the health professional practice requires stamina, good health, appropriate knowledge and skills, and the ability to respond positively to challenging experiences. Doctors needs to have good psychological and physical health to perform according to good practices and not to burn out. A recent study introduced the psychological concept of Resilience, which relates to the long-term ability of individuals to survive in and thrive on adversity; this concept is rarely used in medical practice but proved to increase the psychological stamina and interaction of individuals, which in turn showed significant impacts on the reduction of dissatisfaction and burnout. More research is highly recommended to be performed on this topic and the implementation of resilience assistance for medical trainees and practitioners [
2].
The performance of prospective observational studies is highly recommended by the literature; the conducting of such studies using validated international scales will provide a clear assessment of the affected population over time (trainees), which will measure the prevalence of the burnout syndrome and associated factors at each level (education, intern, resident, or practice). This will help in building both prevention and treatment strategies and increase their effectiveness [
30]. Within this context, our research study is timely and responds to a key requirement for resilient healthcare [
31,
32]. It is critical to monitor variations in trainees’ satisfaction and burnout rates in the short and long term in order to be capable of recognizing the effect of novel didactical approaches in Training Programs and in best practices [
33,
34,
35,
36].
Lastly, such investments in the wellness of physicians is an ethical responsibility that needs to be upheld by the medical community to assure good practices are conducted by future generations of practitioners [
37,
38,
39,
40,
41,
42,
43,
44,
45,
46,
47,
48,
49].
From this point of view, our research delivers this ethical responsibility and provides significant findings that can be exploited towards the enhancement of well-being, quality of life, and images of the residents in Training Programs. It is also a bold initiative for promoting the health specialties community’s involvement in the recognition of performance in all the aspects of health practices and training.
In summary, the contribution of the critical literature review to the specification of our research problem can be summarized as follows:
We are interested in setting up benchmarks to indicate the added value components of job satisfaction of residents in Training Programs supervised by the SCFHS.
We want to obtain a comprehensive picture of the burnout phenomenon in a large population of residents in Saudi Arabia and to reveal some key positive and negative relationships of job satisfaction with specific factors.
As a responsive action, our research also aims to provide key recommendations for improvement.
We intend to develop a trusted mechanism to monitor the evolution of job satisfaction during residency medical programs.
We want to understand the basic “cause and effect” relationships between job satisfaction and aspects of the psychological load of residents, including aspects of the Training Program and educational activities as well as the impact of burnout on satisfaction.
We focus on the analysis of the psychological factors that affect job satisfaction. We also in parallel run a complimentary study that studies the rates and impact of depression and anxiety in the context of the professional and educational activities of the residents in training centers.
We are also interested in understanding which aspects of mental capabilities and skills of residents can work against psychological pressure and dissatisfaction based on the professional and academic conduct of residents.
We do not intend to study the possible association of the job satisfaction of trainees with job performance. This can be a direction for future research.
We are interested in understanding how special aspects of the training institutions of trainees and special aspects of Training Programs affect the job satisfaction of residents.
In future research we would also like to investigate the income and rewards parameter and how it affects job satisfaction.
In the next section, we provide our research methodology strategy and we outline our research objectives.
3. Methods
The previous critical literature review revealed several complementary aspects of the research area in the wider literature. The focus of our research is on factors that enhance trainees’ satisfaction in post graduate medical Training Programs. We are very interested in analyzing, understanding, and interpreting perceptions from trainees of the quality of their residency programs. Our methodological approach is integrated into a greater research context. The SCFHS has launched the Quality Initiative, within which a multidimensional framework for quality assurance has been introduced. The core part of this framework is a set of 23 Key Performance Indicators (KPIs) that can be exploited as a significant managerial tool for enhanced decision making. In this research paper, we emphasize the perceptions of residents in postgraduate medical Training Programs as they refer to their job satisfaction. We also intend to add additional aspects for our Quality Assessment framework with an emphasis on KPIs related to job satisfaction.
Trainees’ satisfaction in residents Training Programs is a key factor for the measurement of efficiency. In our approach, we integrate several value components of the trainees’ satisfaction and we investigate the attitude of residents and fellows in the SCFHS’s medical Training Programs.
The seven components of trainees’ satisfaction under investigation in our research are summarized below (see
Table 3, below):
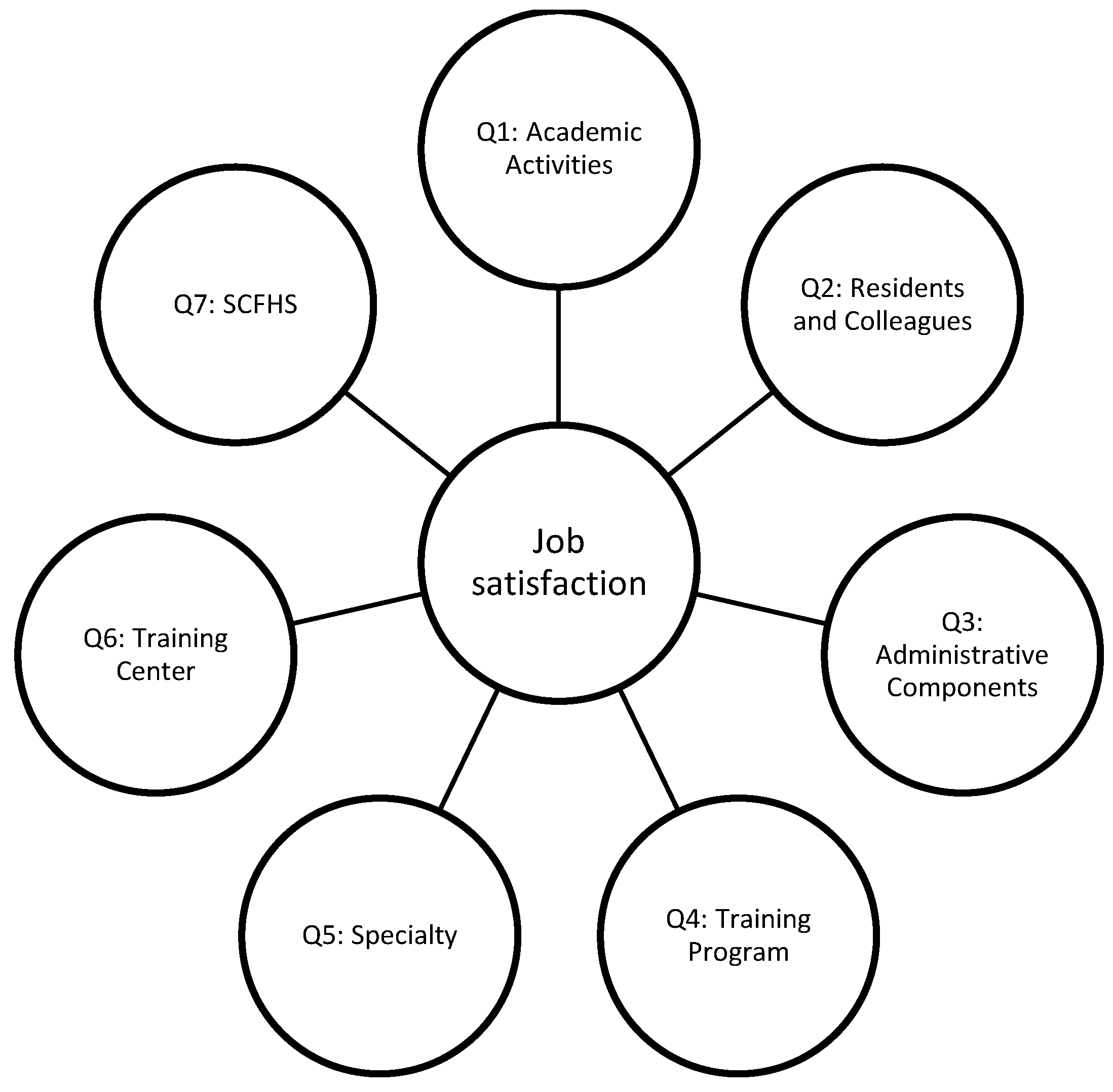
- Q1:
Satisfaction with Academic Activities in the Training Center. This is a critical aspect of our study on residents’ satisfaction. We are interested in analyzing and interpreting the degree of satisfaction of trainees related to the academic activities and learning strategies of their training center. The ultimate objective of our integrated research involving the SCFHS is to develop reflective strategies and actions towards improvement of the quality of Training Programs offered by the SCFHS.
- Q2:
Satisfaction with the Residents and Colleagues in the Training Center. This component is related to the collegiality and the professional social interaction of trainees with other parties in their training centers. It is important to investigate how trainees perceive the quality of their interaction with other residents and colleagues in the training center. We understand that several psychological and behavioral factors determine this relationship, but we intend to study its overall measure.
- Q3:
Satisfaction with the Administrative Components in the Training Center. We focus on the key aspects of interactions of residents with their administration and the execution of administrative tasks integrated in their training. We are interested in understanding the overall satisfaction and how to interpret it to provide significant and meaningful recommendations.
- Q4:
Satisfaction with the Training Program. The overall perception and evaluation of the Training Program by the trainees provides a holistic, subjective measure for the quality of education. We are interested in monitoring this rate over time and this study serves as a benchmark for future studies and initiatives related to the enhancement of the quality of Training Programs. It is also associated with our effort to update, and to enhance a compact set of Key Performance Indicators (KPIs) associated to the Quality Initiative in SCFHS. A full set of these KPIs can be found in our recent previous publication.
- Q5:
Satisfaction with the Specialty. The perception of residents and fellows towards their specialty and their internal association of different levels of satisfaction is another factor under investigation in our research study.
- Q6:
Satisfaction with the Training Center. The perception of trainees towards their training center is also an important area for understanding possible barriers, difficulties, and quality evaluations for residents. This quantifiable measure can also be used for strategic actions towards improvements.
- Q7:
Satisfaction with the SCFHS. Trainees in their daily interaction with the Training Program in the training center also indirectly interact with the SCFHS as a supervising and accreditation body. It is extremely important to reveal how this relationship is valued by the residents and also how it informs reflective actions for the enhancement of the overall quality.
In
Figure 2, below we summarize the core components of the job satisfaction as we approached them with our methodological tool. Namely, seven core components of job satisfaction were set in the center of our focus.
Our research has four critical key objectives:
- Research Question 1:
Which are the core components of job satisfaction in residency medical Training Programs as perceived by the trainees?
- Research Question 2:
Which are the current benchmarks of job satisfaction in the residency program supervised by the Saudi Commission for the Health Specialties?
- Research Question 3:
Which are the key recommendations for the enhancement of residency Training Programs for enhanced trainee satisfaction?
- Research Question 4:
How can we interpret the main perceptions of trainees’ job satisfaction in terms of measurable, trusted, and reliable Key Performance Indicators for promoting the quality of post graduate medical Training Programs?
The key aspects of our research approach are summarized as follows:
This is an analytical, prospective, cross-sectional study design that represents the trainees’ job satisfaction towards Training Programs supervised by the SCFHS in 2018. A self-administered, semi-structured questionnaire survey with both open and close ended questions was distributed to trainees through an online link.
The validation process of the questionnaire included assessing its content validity, which was performed by content experts, after its face validity was assessed by a medical educationist who found that the survey fulfilled the objectives of the study and that the flow of questions followed a logical sequence. To test the reliability of the questionnaire, a pilot study was conducted on 40 participants.
The survey questionnaires for residents were developed by the PGMT Quality Indicator Committee (QIC) to produce an error-free measure of the quality of care, based on characteristics of best practice such as validity, reliability, and transparency. The questionnaire comprised items and included domains pertaining to the training center evaluation, research and simulation training, personal issues, residency program evaluation, and recommendations.
In total, there were 13,688 residents working in different specialties throughout Saudi Arabia, of which only 3442 (25.14%) agreed to participate in the online survey. The trainers were excluded from the survey owing to time constraints. A total of 41 questions represented the indicators of the quality of Training Programs, which were validated by experts and QIC panels for clarity and content relevance.
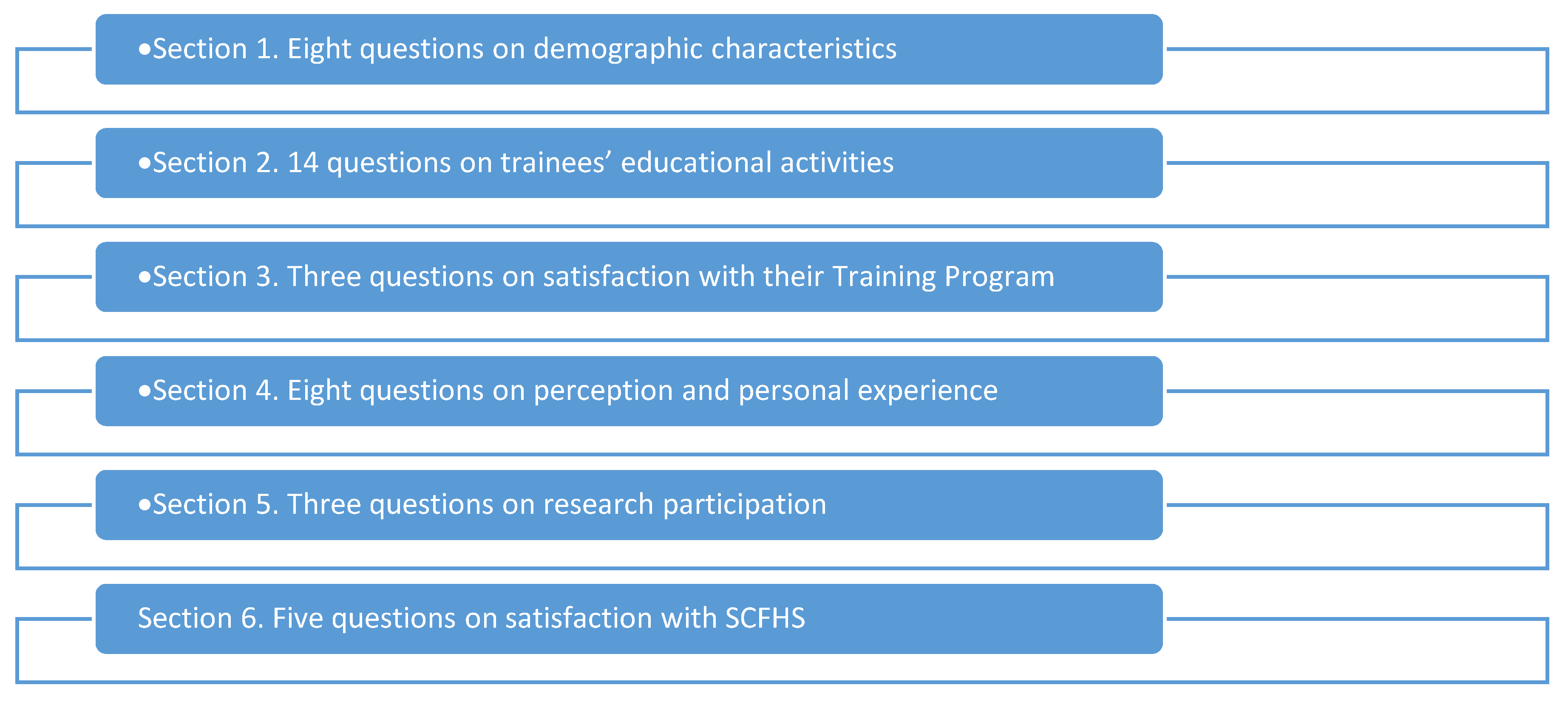
The questionnaire comprised six sections (see
Figure 3):
The first section comprised eight questions on demographic characteristics
The second section comprised 14 questions on trainees’ educational activities
The third section comprised three questions on satisfaction with the Training Program
The fourth section comprised eight questions on perceptions and personal experience
The fifth and sixth sections comprised three and five questions on research participation and satisfaction with SCFHS, respectively.
The Key Performance Indicators Working Group is responsible for collecting and analyzing data annually and ensuring that the indicators remain precise and appropriate. This goes against Toussaint et al.’s suggestion of releasing quarterly reports [
22]. After respondents’ data were collected and entered into Microsoft Excel, they were rechecked to ensure there were no typos or blank/empty data cells. The statistical program SPSS version 24 was used for online data analysis. A test was considered significant if the
p-value < 0.05.
In the next section, we provide a systematic overview of key findings organized into five distinct areas of interest:
In
Section 4.1, we present the key demographics of our study
In
Section 4.2, we present the key findings related to the Overall Job Satisfaction of trainees in residency programs
In
Section 4.3, we summarize the key aspects of core components of trainees’ satisfaction per their discipline and gender
In
Section 4.4, we discuss the findings related to job satisfaction associated to the Training Center of the residents
In
Section 4.5, we elaborate on the key perceptions of residents for their job satisfaction associated to the Training Program they participated in
Last but not least, in
Section 4.6 we present some key aspects of the impact of burnout and sexual harassment on trainees’ satisfaction.
In
Section 5, we provide a thorough discussion of key findings and their implications. We also discuss the limitations of our study, as well as key recommendations related to sustainable health.
4. Results
The trainees’ response rate to the online survey was 27% (3696/13,688) which is satisfactory and represents a significant sample for our interpretations and key findings. This section is organized as follows. First, we present the key demographics of our research. Then we emphasize the presentation of the overall job satisfaction of residents per their discipline, residency type, and gender. After this overall analysis, we emphasize key aspects affecting the perceptions of trainees towards the Training Program and the training institution. Finally, we discuss the important factors affecting burnout and other psychological aspects of trainees’ satisfaction.
4.1. Demographics of Our Survey
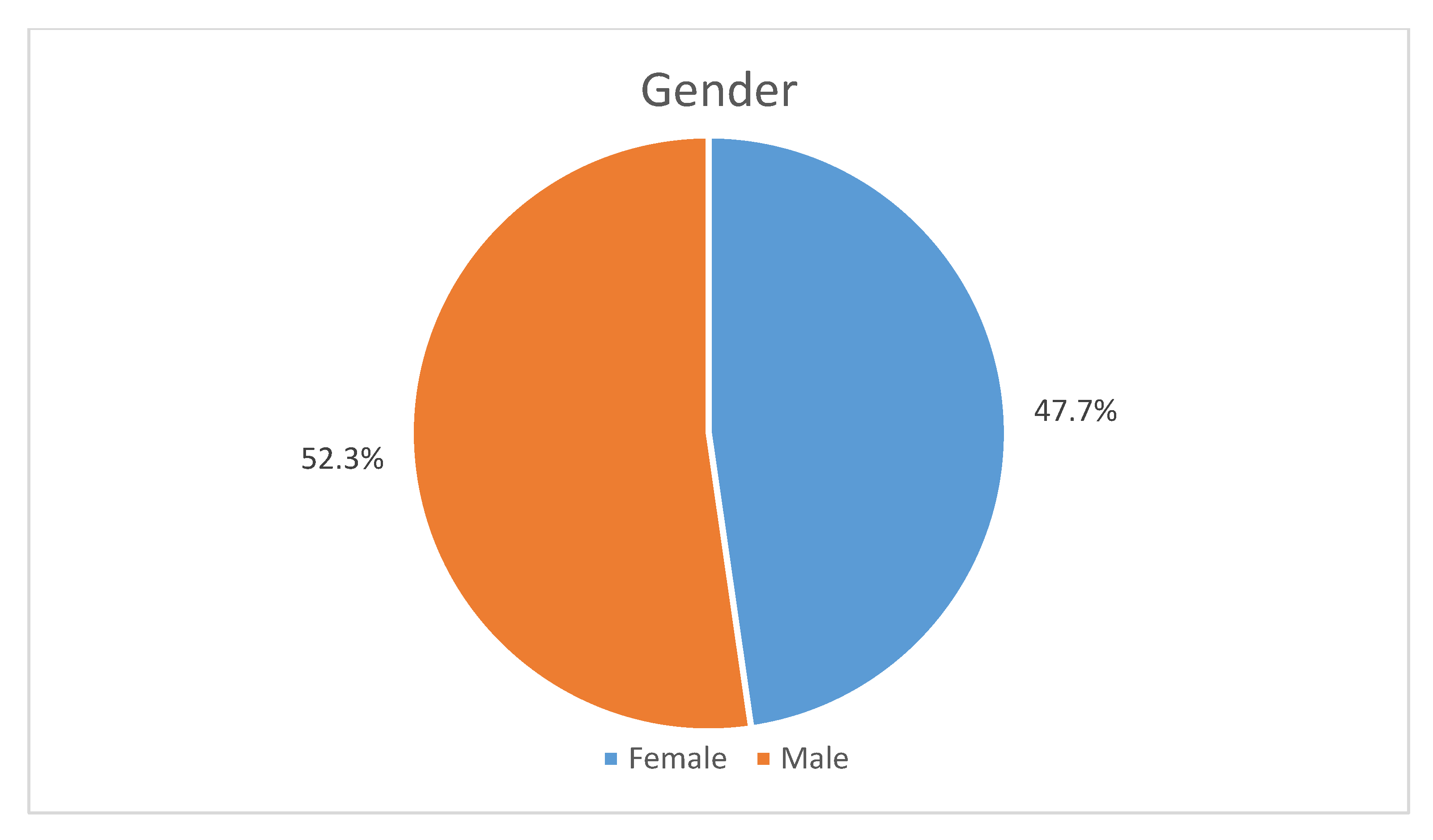
There were 1932 (52.3%) male respondents (see
Figure 4, below), and the majority (91.9%) were Saudi nationals.
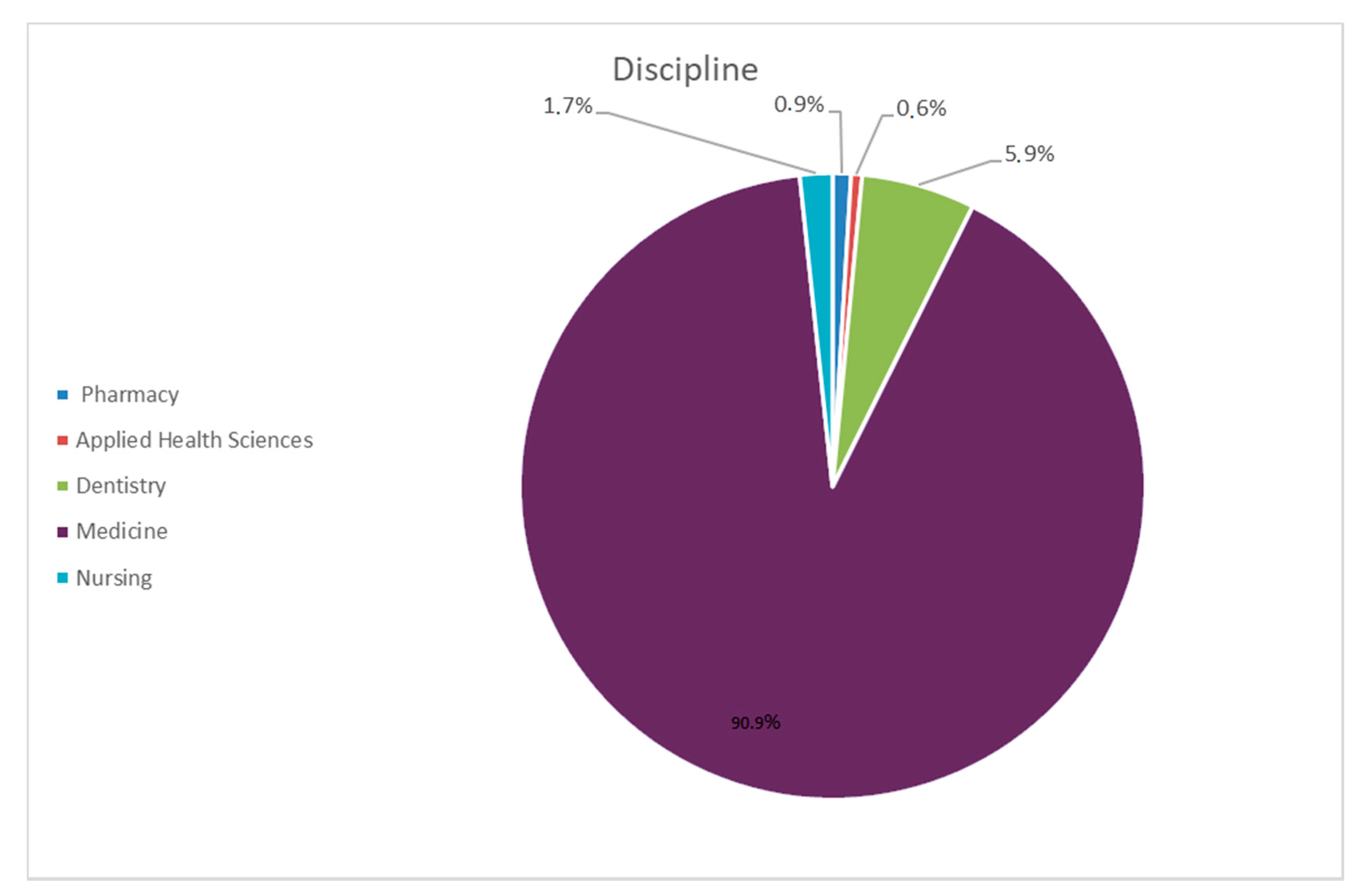
Concerning the discipline, as seen in
Figure 5 below, the vast majority, almost 9 out of 10 respondents belong to the Medicine discipline (90.9%) while the second largest representative discipline is Dentistry with 5.9% (see
Table 4 and
Table 5 below).
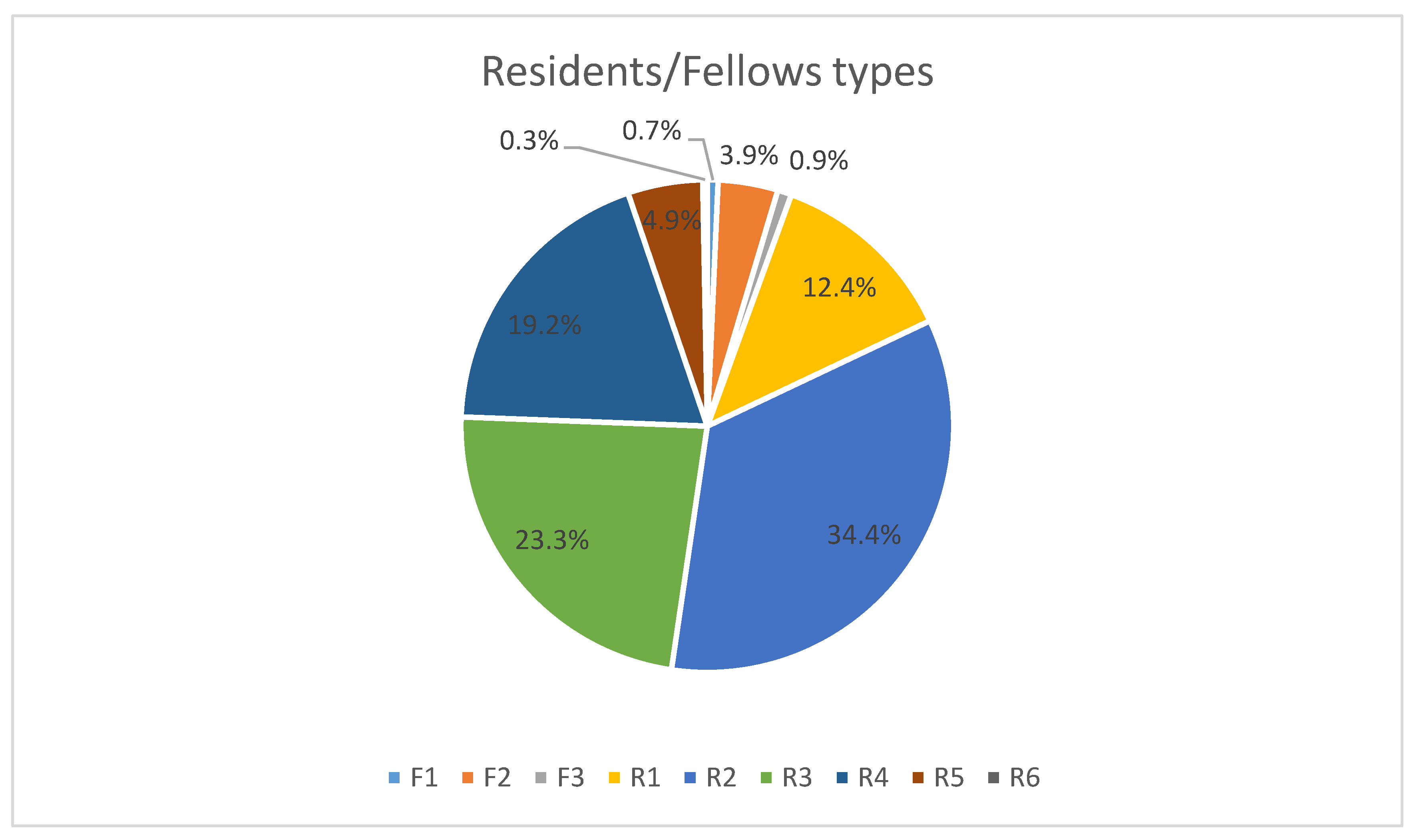
Almost third of the residents (1270 or 34.4%) were working in the R2 level, while 860 (23.3%) were working in the R3 level (see
Figure 6 below).
More than one-third (40.4%) of the trainees were in the Central Region of Saudi Arabia and approximately one-third (34.5%) were in the Western Region. The highest proportion of trainees (39.6%) were working in Riyadh City and 20.1% were working in Jeddah.
4.2. Analysis of Overall Job Satisfaction
One of the key objectives of our research was to develop a benchmark for the measurement of the job satisfaction of trainees in residency programs in the Kingdom of the Saudi Arabia. From this point of view, our work is novel and provides a snapshot for the measurement of trainees’ satisfaction in this given period. This metric is significant and allows further developments related to its constitutional factors.
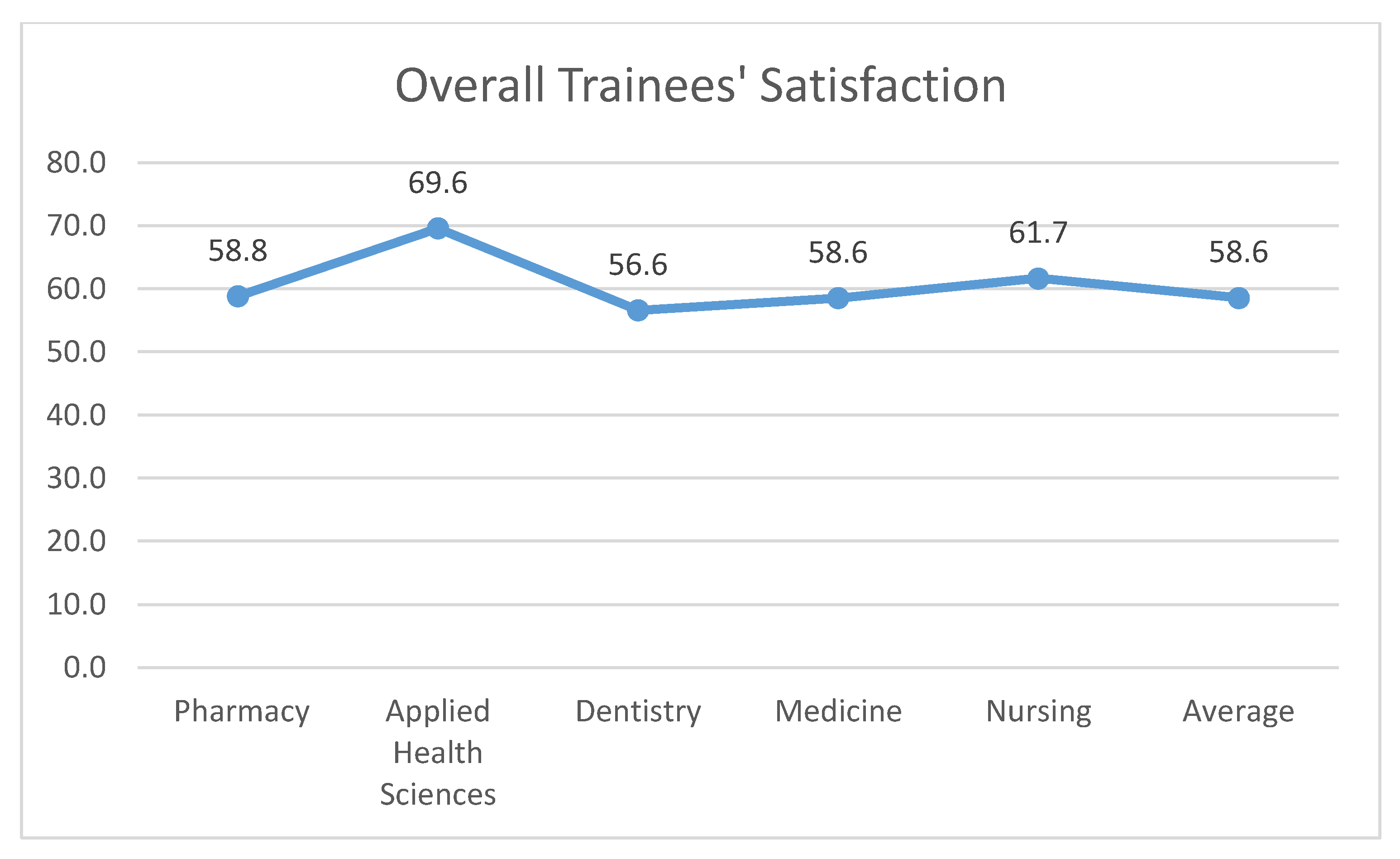
In
Figure 7 below, we provide the overall trainees’ satisfaction per discipline. The absolute rate for Medicine is 58.6%, a number which allows for significant improvement and sets an initial benchmark for the Training Programs of the SCFHS. From a decision-making point of view, an update of the integrate strategy for the integration of quality in residency programs is required. We intend to discuss this first significant finding of our research further in the Discussion and Implications of our research study section. The overall satisfaction for Pharmacy, is quite like the one related to Medicine and it equals 58.8% (see
Table 6, below).
The highest satisfaction rate is for the Applied Health Science trainees, at almost 70%, while the lowest is related to Dentistry at 56.6%. The first interpretation for this finding is that it can be used as a benchmark for the ongoing and future monitoring of trainees’ satisfaction in the near future and also that the especially for the Medicine specialty, there is significant space for improvement. In the Discussion section, we provide our key recommendations.
Another interesting finding of our research is summarized in
Figure 8 below, which is related to the overall satisfaction per residency type. It seems that fellows in residency programs have 8% greater satisfaction than junior and senior residents.
4.3. Analysis Trainees’ Satisfaction Core Components
As discussed in the Research methodology section, one the key objectives of our survey is to understand the perception of trainees in residency medical programs related to seven core aspects of satisfaction including:
In
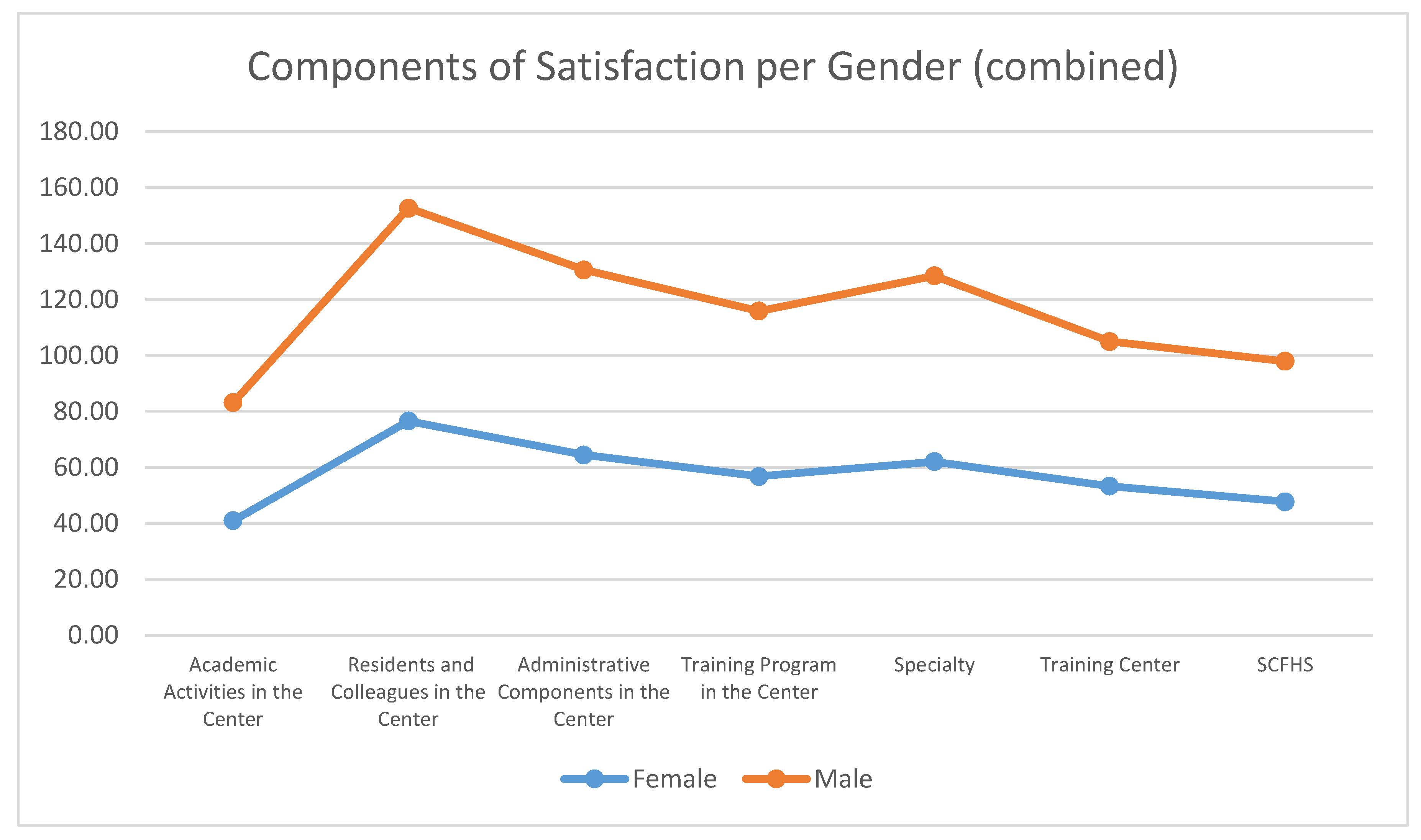
Figure 9 and
Figure 10 below, we provide the key findings per Gender. The female participants rate showed high satisfaction gained from their interaction and co-existence with other residents and colleagues in the center (76.6%). They also appreciate the administrative components in the center at a fairly high rate (64.5%) and they are satisfied with their specialty at a good rate (62.1%). Their perceptions of their Training Center and the Training Program at the center are also rather fair (53.3% and 56.8%, respectively). It seems that there is lots of room for improvement for their academic activities in the center, as well as their interactions and integration with the SCFHS (41% and 47.8%) ((see
Table 7, below).
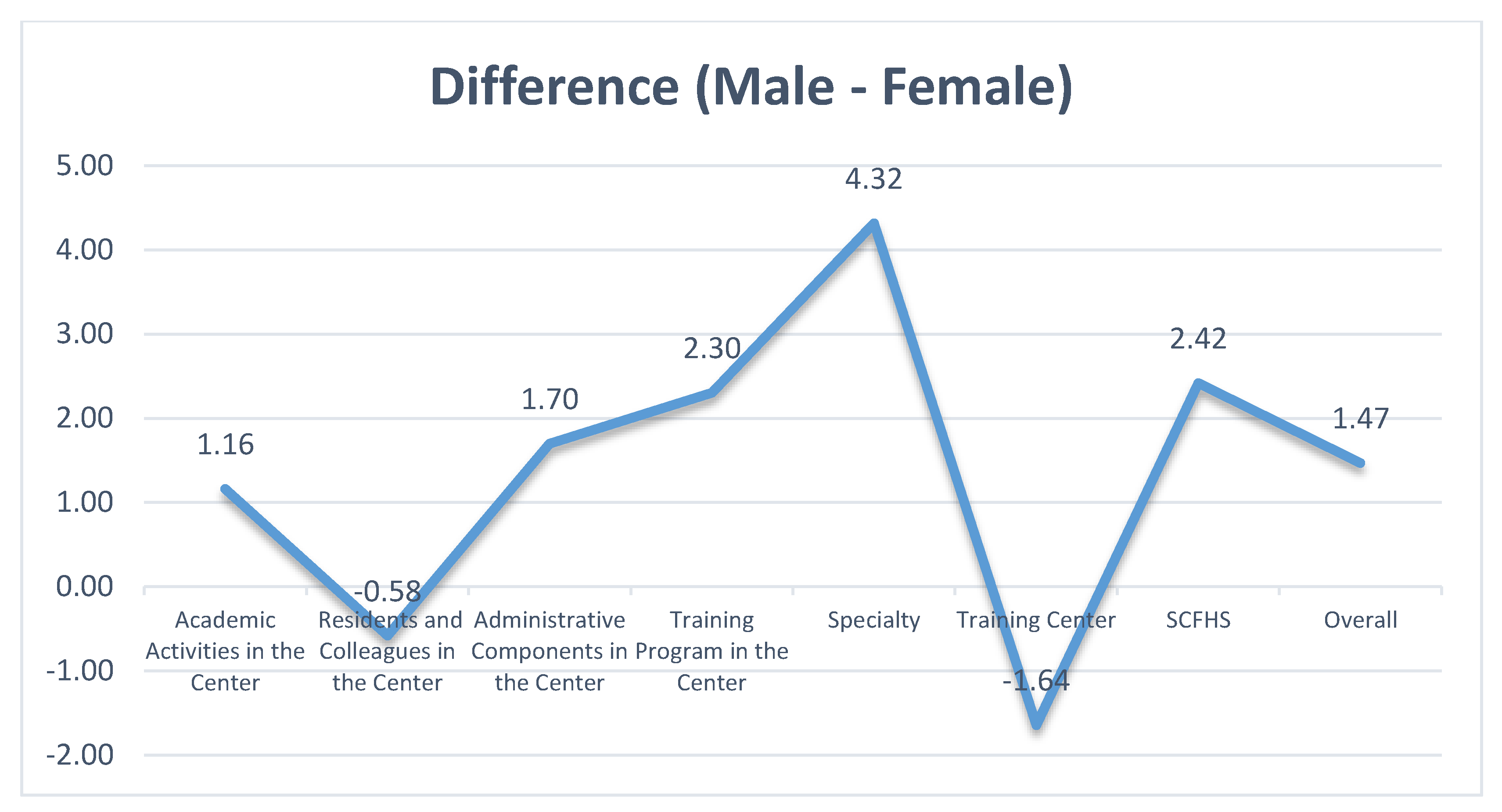
Male participants in our survey have similar attitudes to the seven components with some minor differentiations. They rate their overall satisfaction (+1.5%), their satisfaction related to administration in the Training Center (+1.7%), and to academic activities in the center (+1.2%) a bit higher. They are happier with their specialty (+4.3%) and also they value their relation with the SCFHS (+2.4%) more highly. Similarly to females, males seem to need further developments and enhancement in their academic activities in the center.
The rather low degree of satisfaction of residents related to the academic activities in the training institution must initiate a debate on a strategic plan for quality enhancement. Various ideas and approaches can be integrated. Some ideas are related to:
Access to trusted online academic content
Teamwork and active learning strategies
Extensive use of robotics, Artificial intelligence tools, virtual and augmented reality labs, and simulation labs
Extensive research enhancement initiatives for the support of residents in the research domain
Applied research-based training and learning
Technology enhanced learning interventions
Integration of academic activities with the healthcare industry
Enhancement of the relation of residents with academic supervisors
Psychological support and relief of burnout rates. A more balanced work-life-study approach
In the discussion section, we elaborate further on this key finding of our research. We also comment on our future research for a more sophisticated analysis of these core components of satisfaction.
In
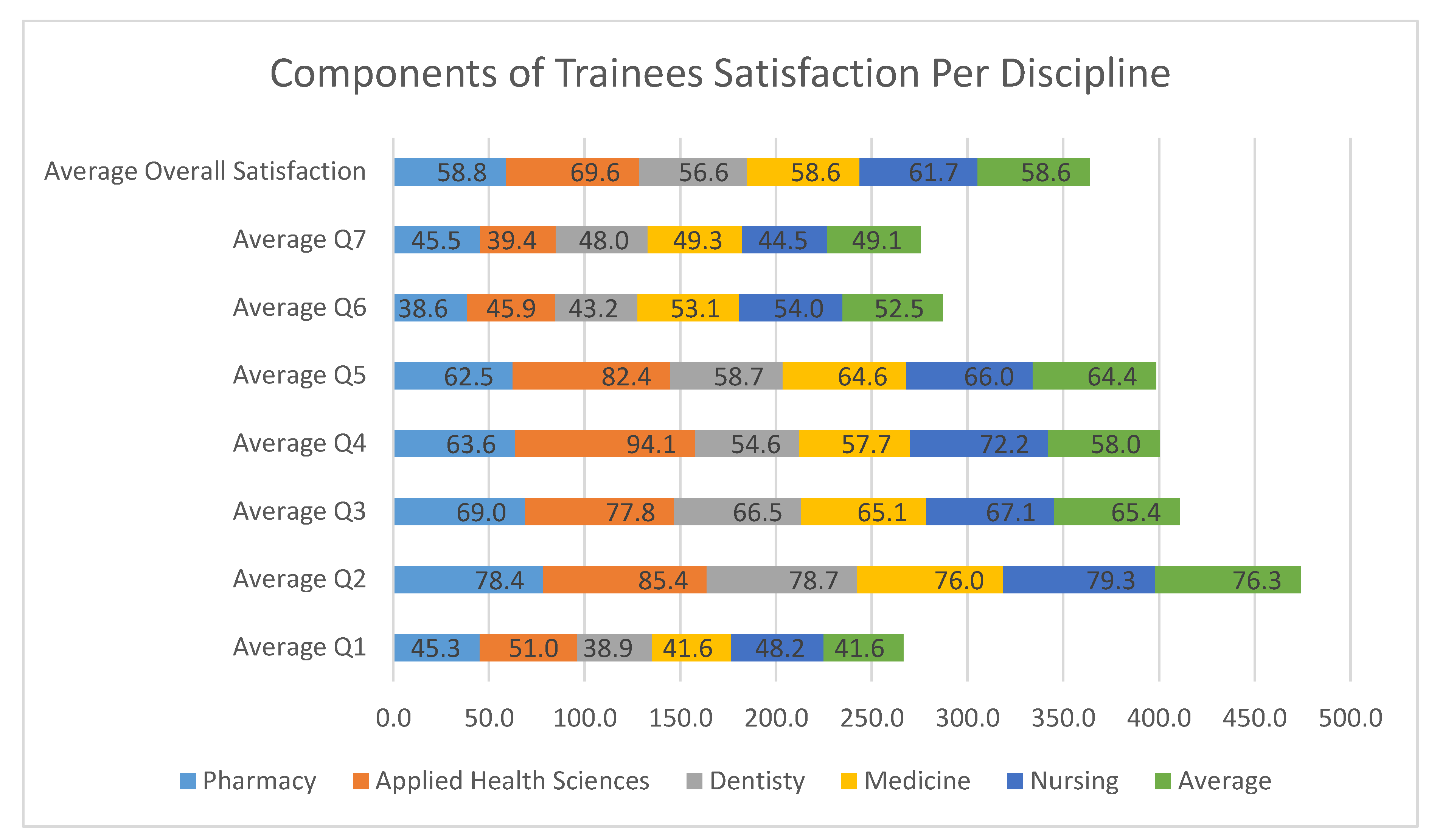
Figure 11 below, we add one more level of analysis concerning the core components of trainees’ satisfaction. We summarize the values for the seven core components of residents’ satisfaction per different discipline. In the attached table, we also highlight some significant findings for further discussion.
In the Pharmacy and Dentistry disciplines, there is a rather low satisfaction of residents towards their Training Center. The absolute rates (38.6% and 43.2%, respectively) require further study and investigation. Obviously, some aspects of the training centers do not satisfy residents.
As the key finding for most of our sample, the Medicine discipline residents are not satisfied with their academic activities in the Training Center. Their rate of 41.6% is a bit higher from the relevant rate for the Dentistry specialty, which is 38.9%. One of the key propositions of our study is that the Academic activities should be reconsidered and we should also initiate this satisfaction component as an absolute KPI for the quality of the Training Programs offered by the SCFHS.
Residents in Applied Health Sciences seem to be enthusiastic towards their Training Program in the center, with an extremely high rate of 94.1%. They also seem the happiest in terms of their specialty (94.1%) (see
Table 8, below).
All the other findings follow the same trends and patterns of male and female participant averages. It seems from all the different disciplines that there is a need for focused strategic actions targeted towards:
The multidimensional enhancement of the academic activities in the training center. For this purpose, we intend to initiate a new survey of the required actions and the suggestions of administrators and trainees.
The cultivation of a trusted relationship between the residents and the SCFHS. It is necessary to update communication channels and to increase the awareness of residents to provide added value and increase its contribution to their careers.
The enhancement of the Training Centers and a continuous improvement process and strategy over time. It is a recommendation to use the benchmarks of this study as a managerial tool for enhancing satisfaction rates over time for the next 5 years by 5–10% per year. This is a bold requirement that needs further investigation, planning, and implementation.
The development of an institution-wide initiative for the enhancement of the Training Centers in all their aspects. In the next section of our survey, we provide numerous additional qualitative features of the perceptions of the residents towards their Training Center. We do believe that one of the bold findings of our research is related to the average perceptions of respondents towards the Training Center and the academic activities. These two aspects jointly summarize the core components for the residents’ experiences and behavior.
4.4. Special Analysis of Trainees’ Satisfaction Related to Training Center
Our research study is one of the first efforts worldwide to identify, measure, and interpret the satisfaction of trainees in residency medical programs for the enhancement in their quality and their impacts. It is linked to the Sustainability and Health debate because it promotes a scientific debate for the constitutional value adding components in medical training. In the discussion section, we provide thorough case for the connection and the implications of our research for the Sustainable Health domain.
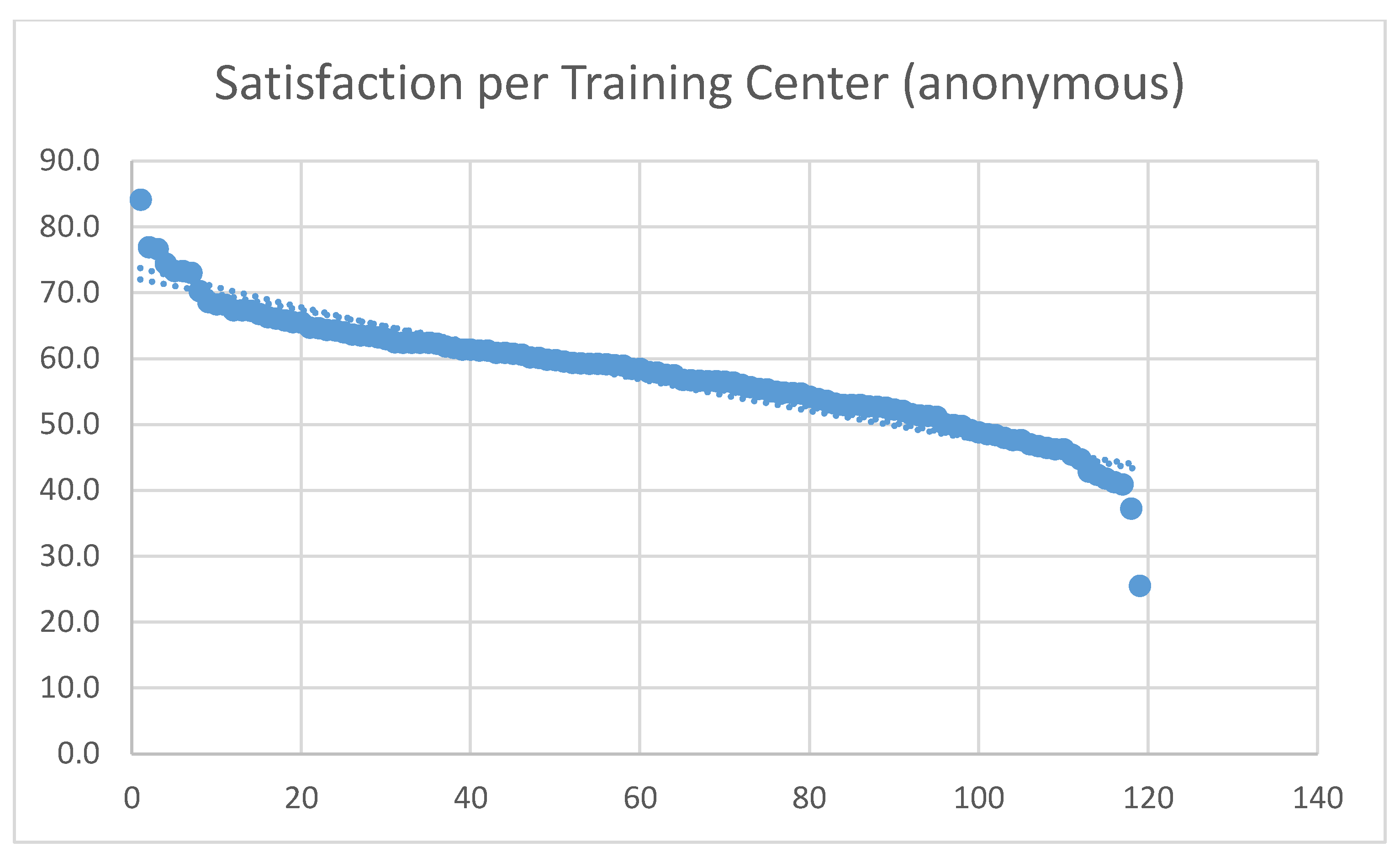
In this section, we elaborate further in the perceptions of our respondents for their satisfaction towards the Training Program and the Training Center. In
Figure 12, we provide a high-level abstraction for the satisfaction rate of residents for 120 different Training Centers without uncovering the identity of each center. The picture provided in this figure is interesting. There are Training Centers that are perceived highly by residents, which provide high satisfaction and happiness. From the other side, residents also provide rather low satisfaction rates for numerous other Training Centers. The overall rate of satisfaction of trainees for all the Training Centers is approximately 55%. This is another interesting benchmark that our research study reveals.
It is necessary to study the findings of
Figure 12 further. The SCFHS must have a continuous improvement process to understand in depth the causal factors for the low evaluation of specific training centers indicated by the respondents of our survey. We do understand that the current survey provides a snapshot of a given moment, but the overall findings have validity and require interpretation and revision of policies, as well as actions for enhanced decision making. In the next section, we try to provide more data and facts indicating the perceptions and attitudes of trainees towards their Training Center and program. We recommend a new run of a similar surveys in due time to understand how some reflective actions and recommendations had an impact on overall quality and satisfaction levels.
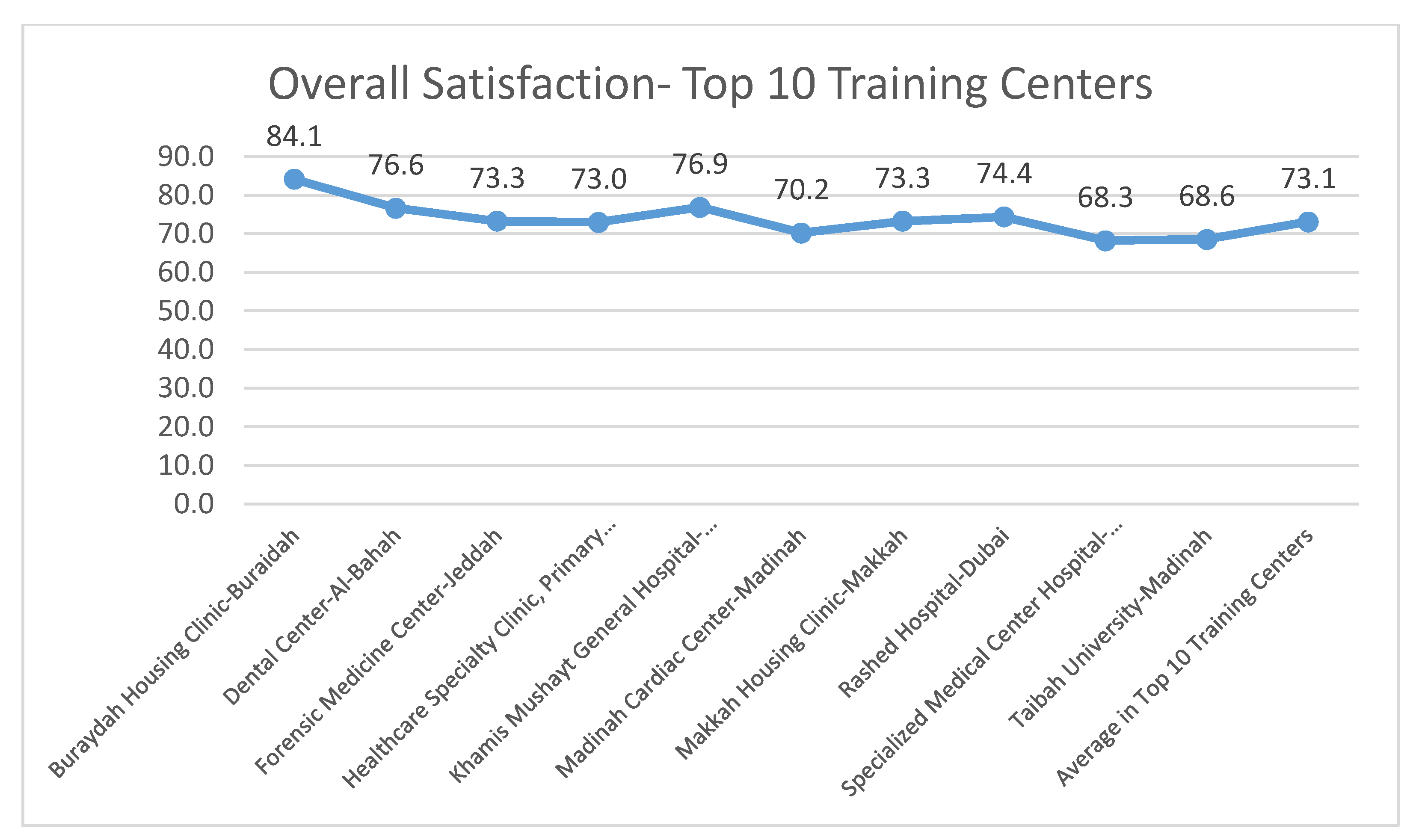
In
Figure 13, we also provide the top Training Centers in terms of residents’ satisfaction. We understand the limitations of our study, which will also be discussed in
Section 5 of this paper, but we also consider that the ratings of such a large sample in our study provide trustworthy approximations of quality and satisfaction.
The concluding comment for the attitudes of residents related to the Training Centers is that overall residents feel that more value can be delivered in the academic program, as well as in the integration with the services and supervision of the SCFHS. In the next section, we provide additional key data and facts related to the disposition of trainees with the Training Program. Last but not least, we also provide some sensitive data related to burnout rates and sexual harassment figures.
4.5. Special Analysis of Trainees’ Satisfaction Related to the Training Program
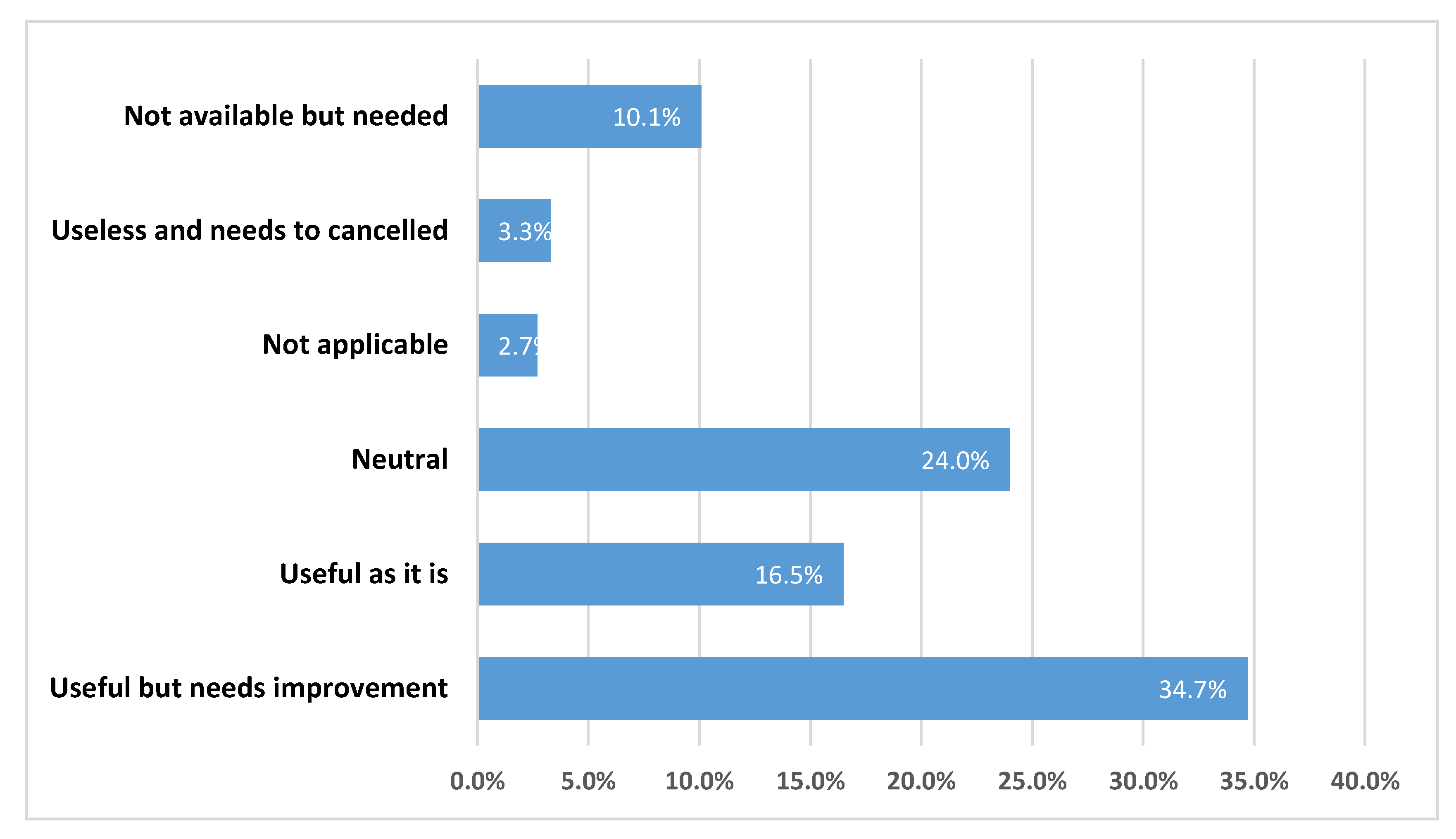
The fourth value component and interpretive factor for the overall job satisfaction of trainees in our methodological approach is related to the training program. The analysis of the key findings is presented in this section. Overall, there is some appreciation from the residents for their Training Programs. According to our collected data, 16.5% of trainees are satisfied with their current Training Programs, while almost 50% request improvements or have neutral attitudes. This is a significant finding. We do believe that a thorough strategic initiative for the enhancement of Training Programs must be undertaken by the SCFHS and the other bodies that are involved in these programs. Some additional facts that are presented below provide directions for this enhancement.
Regarding the satisfaction rate of the trainees, 34.7% believe the programs are good, 16.5% believe that they can be improved, and 2.7% think they are useless (see
Figure 14 below). One fourth of respondents also provided neutral perceptions, which highlights that currently there is a lot of space for enhancements in the Training Programs for residents. From this short overview of the satisfaction with Training Programs, it is highly recommended to use the current benchmarks the Useful as it is and the Useful but needs improvement rates as initial points for improving the satisfaction rate over the next two years by 20%.
In the same direction, we also tried to understand some key factors with a significant impact on trainees’ perception towards the quality of the Training Programs.
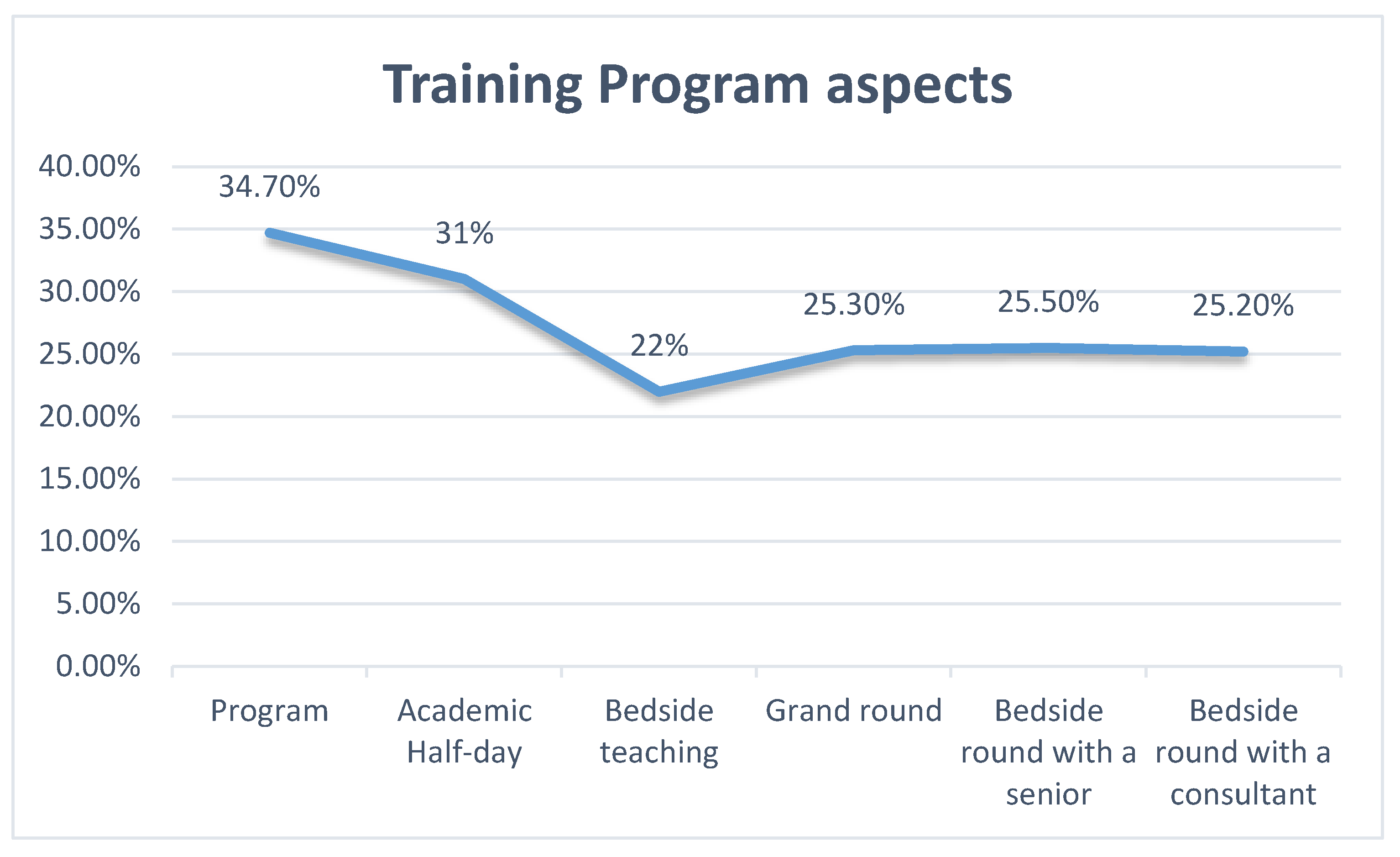
With regard to the satisfaction rate of the trainees, 34.7%, 31%, 22%, 25.3%, 25.5%, and 25.3% considered the program, academic half-day, bedside teaching, grand round, bedside round with a senior, and bedside round with a consultant to be good, respectively (see
Table 9, below).
It is important to emphasize that residents commented that academic half-day is a key aspect of satisfaction, which implies that research and training beyond professional service are recognized as top priorities by trainees. This is a key finding that needs to be exploited further through strategic consultation by enhancing the research and academic life and practice of residents. Trainees selected attitude, interest in learning, and interest in helping others as top priorities while rating features of other residents working in the program.
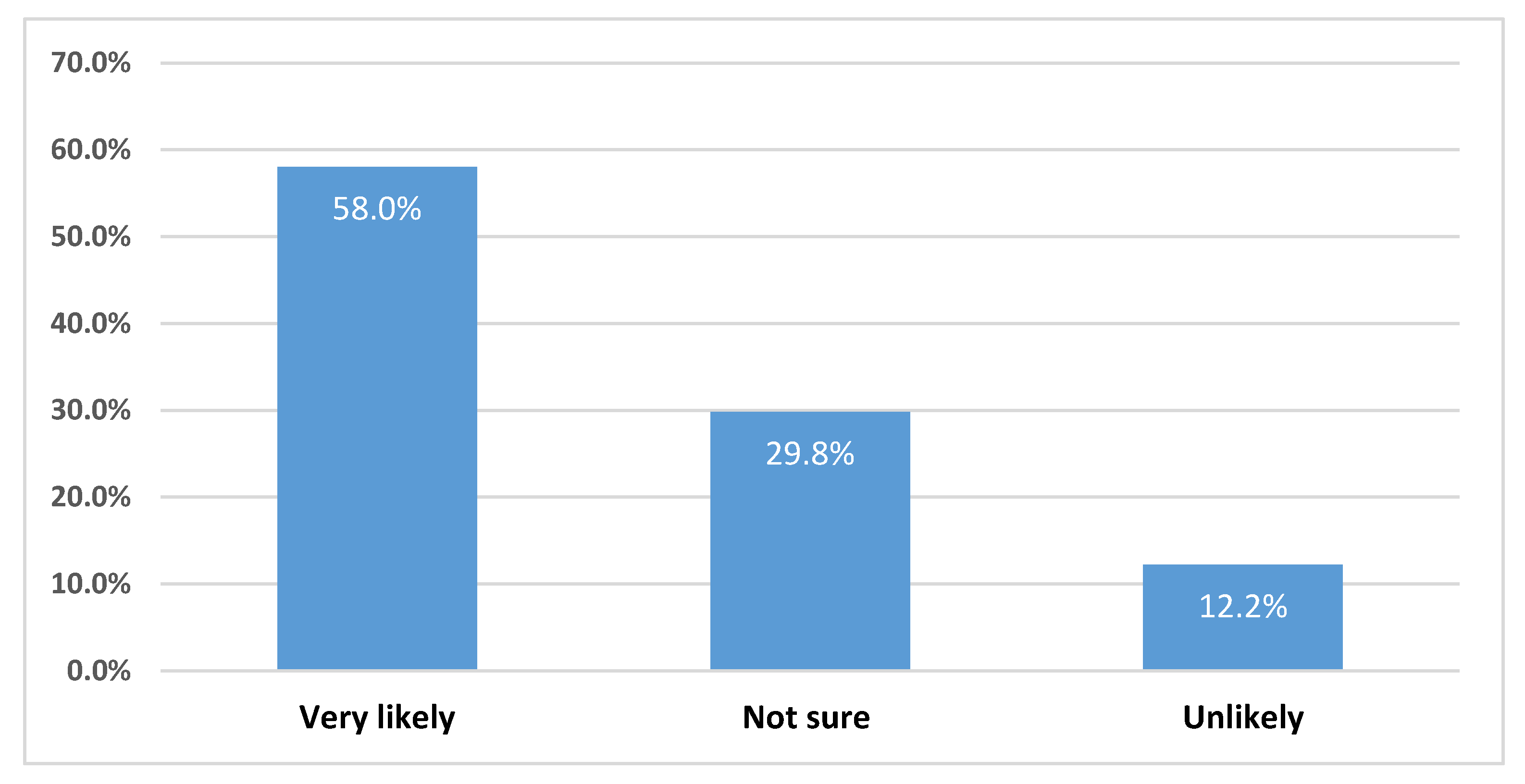
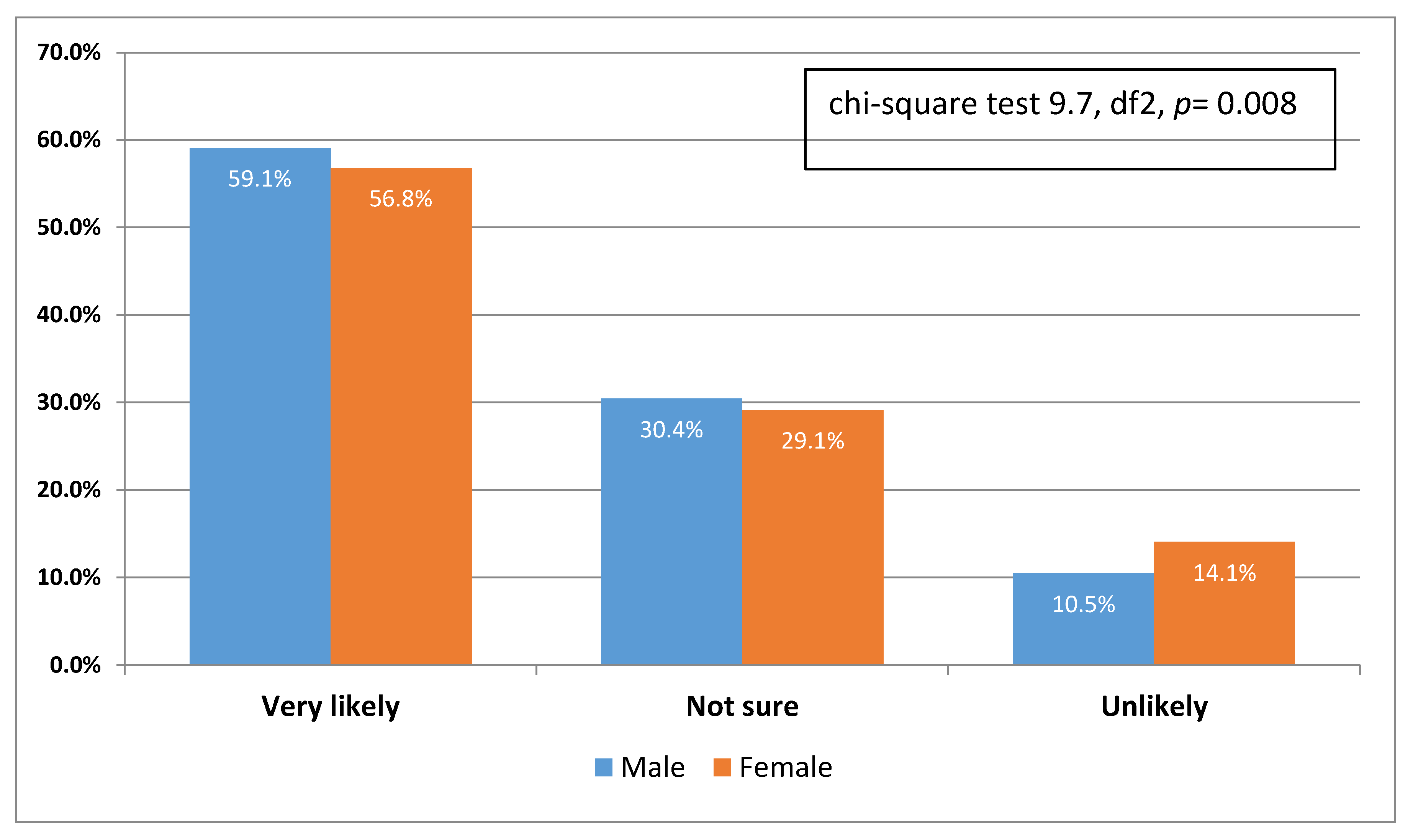
More than half (58%) were very likely to recommend the program in which they work to others, while 12.2% were unlikely to do so (see
Figure 15 and
Figure 16 below). This seems to be a strong core component of trainees’ satisfaction. In future research, we plan to study the value components for his likelihood behavior for recommendation using a Structural Equation Modeling research tool. In the
Section 5, we also provide our constructive interpretation of the key findings of our research towards a progressive model for Trainees’ Satisfaction in Medical Education.
These absolute numbers can also be used for future benchmarking research. They can serve as managerial tools for enhancement and also for monitoring and control of the value proposition of the medical Training Programs supervised by the SCFHS.
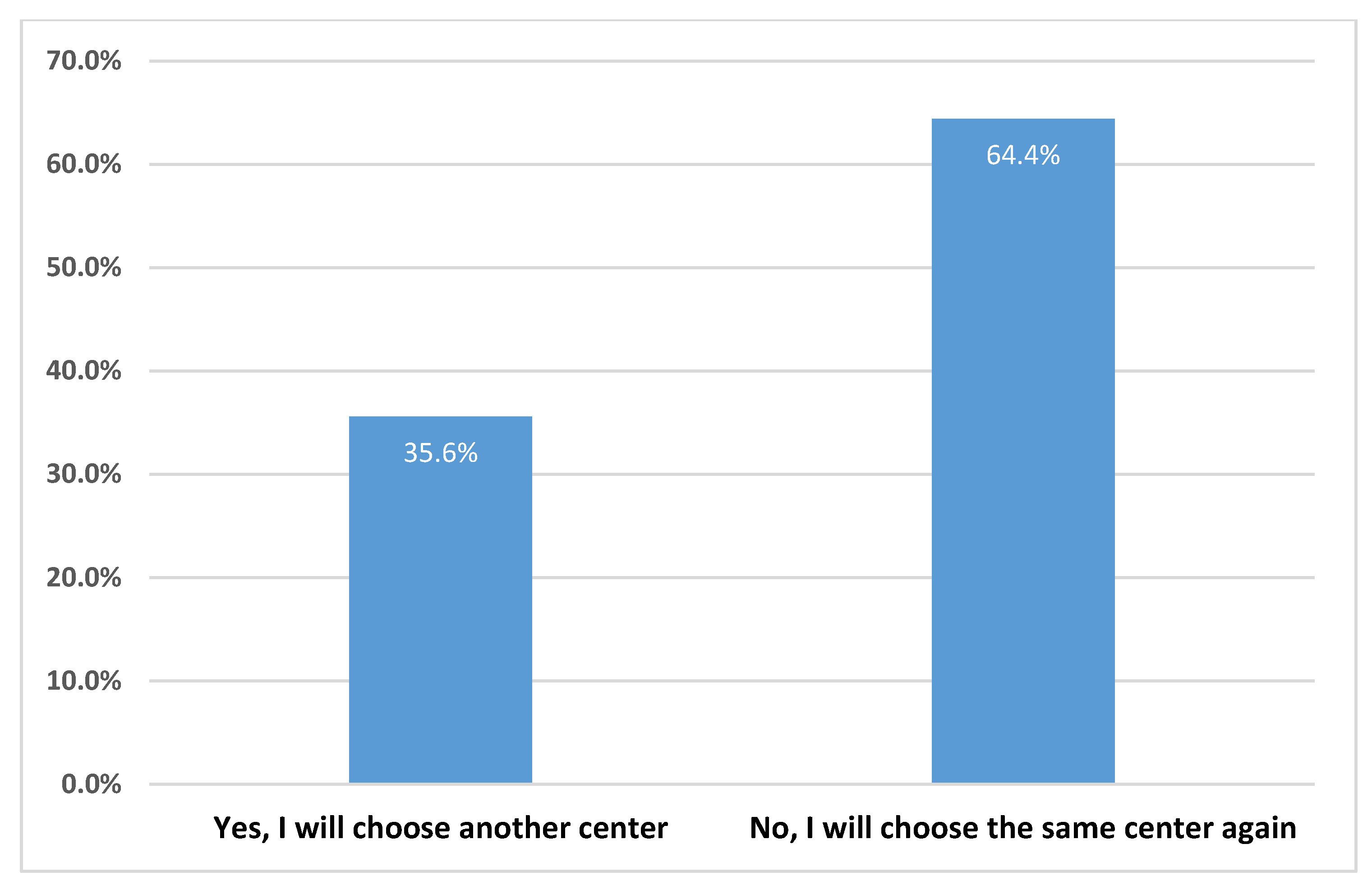
In response to the question on whether they would choose another center for residency training after joining the residency program, nearly one third of the trainees (30.5%) agreed they would (see
Figure 17 below). This is potentially another factor that links the satisfaction rate of trainees to their perceptions towards their Training Center. It seems that one third of respondents do not build a strong bond with their selected Training Center. This finding requires further investigation. We must reveal the factors behind this attitude held by residents. The absolute rate of almost one third is rather high and means that several residents are not satisfied with their current Training Center.
More males than females consider it “very likely” that they will recommend their program to other trainees, while more females consider it “unlikely” that they will do so (see
Figure 18,
Figure 19 and
Figure 20 below).
Female residents seem to be more likely to switch Training Centers than males. In
Figure 19 below, there is a graphical representation of this finding.
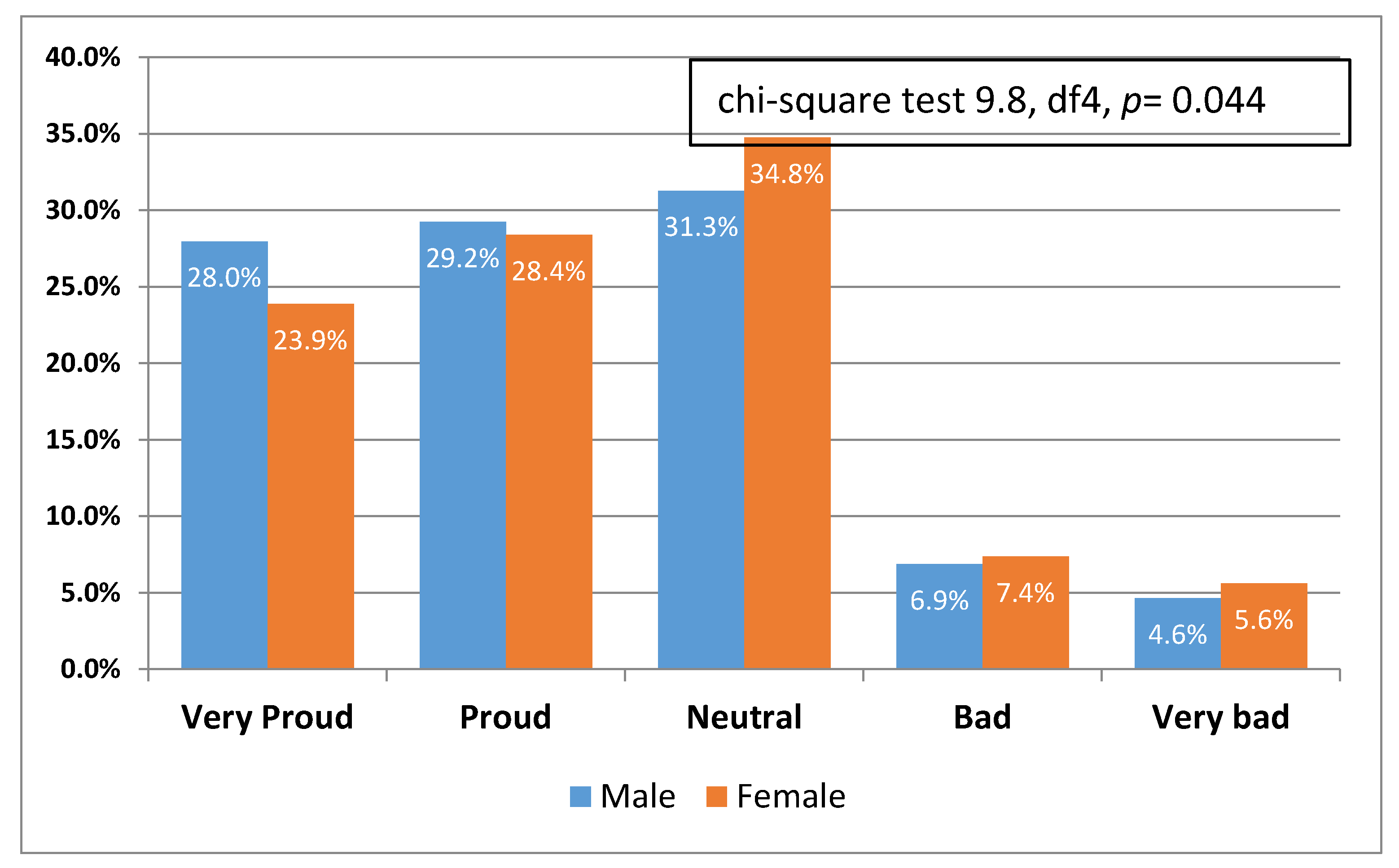
Overall, residents feel proud to have been members of their current Training Center. There were no huge gender-based differences found. It is also important in our future research to understand the reasons why about 10% of residents are unhappy in their current Training Centers. It is a key priority of our future research to identify unhappy residents and to provide flexible mechanisms for their support and psychological enhancement (see
Figure 20 below).
In this section, we provided some initial assessments of the attitudes of residents relating to their Training Program. It seemed that there is a rather fair satisfaction level of residents towards their Training Programs, and a lot of space for improvements. We also suggest that we should use the various rates of the relevant questions as benchmarks for future analysis, monitoring, and control. They can also serve as strategic objectives from improvements. We do believe it is feasible to set the increase of relevant satisfaction components for the Training Programs by 5–10% for the next two years as an objective through reflective strategic actions carried out by the SCFHS.
In the next section, we focus on one more key objective of our research study, which is to investigate the degree of burnout of residents as expressed by themselves in our survey. We intend to interpret the key facts of this situation and to make significant recommendations in the Discussion section.
4.6. Special Analysis of Trainees’ Satisfaction Related to Burnout
Burnout is always referred to the literature as a key component of residents’ dissatisfaction in their medical Training Programs. It is a factor with diverse direct and indirect psychological effects, and also linked with depression and anxiety. In this section, we provide our key findings related to various aspects of burnout (see
Table 10, below).
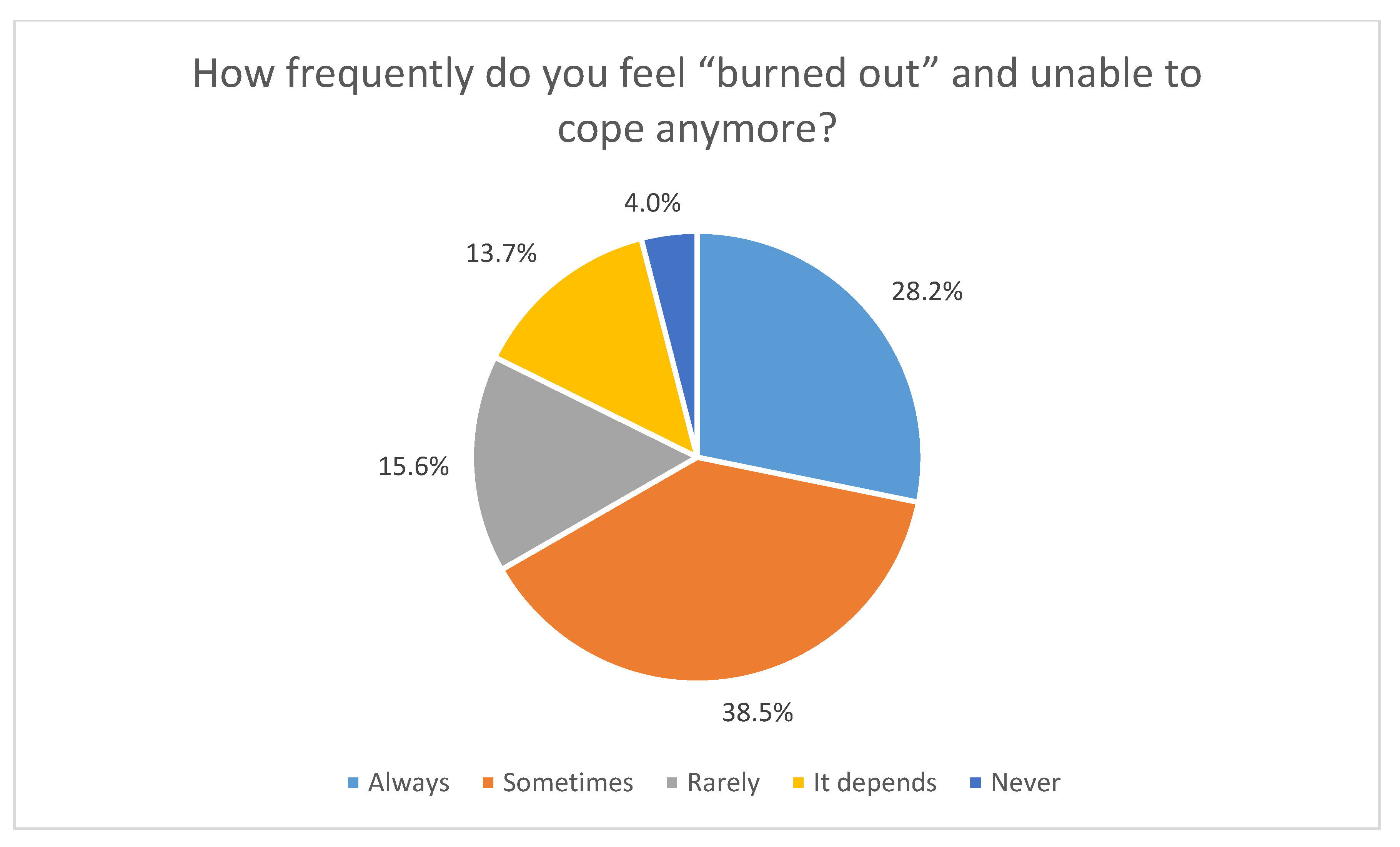
In response to the question “How frequently do you feel “burned out” and unable to cope anymore?”, 28.2% of trainees believe they “always” feel this way, 38.5% “sometimes” have this feeling, 15.6% feel it rarely, 13.7% said it depends, while approximately 4% “never” feel burned out (see
Figure 21 below). This is a major finding of our research that poses critical questions for managerial decisions and key responsive actions. The too high rate of burnout seems to be one of the negative catalysts for the snapshot of the trainees’ satisfaction in residents’ Training Programs. Almost two third of residents feel that they experience a significant rate of burnout in their lives that has a key impact on their professional conduct and their lives. We intend in the near future to run a survey based on structural equation modeling in order to understand the cause and effect relations of burnout and also to measure the impact of the high level of burnout to different aspects of residents’ personal and professional lives. We also present some key recommendations in the Discussion section.
Concerning the burnout rate of residents, there is not a gender-based uniform pattern. In
Figure 22, there is a detailed overview of gender differences related to burnout. Once again, the high rate of burnout for males and females alike is a major finding of our survey and needs further study. It seems to be one of the core components of trainees’ dissatisfaction. The SCFHS must focus on this finding and initiate actions and plans to provide residents with psychological relief and increase their courage and physical capabilities.
In
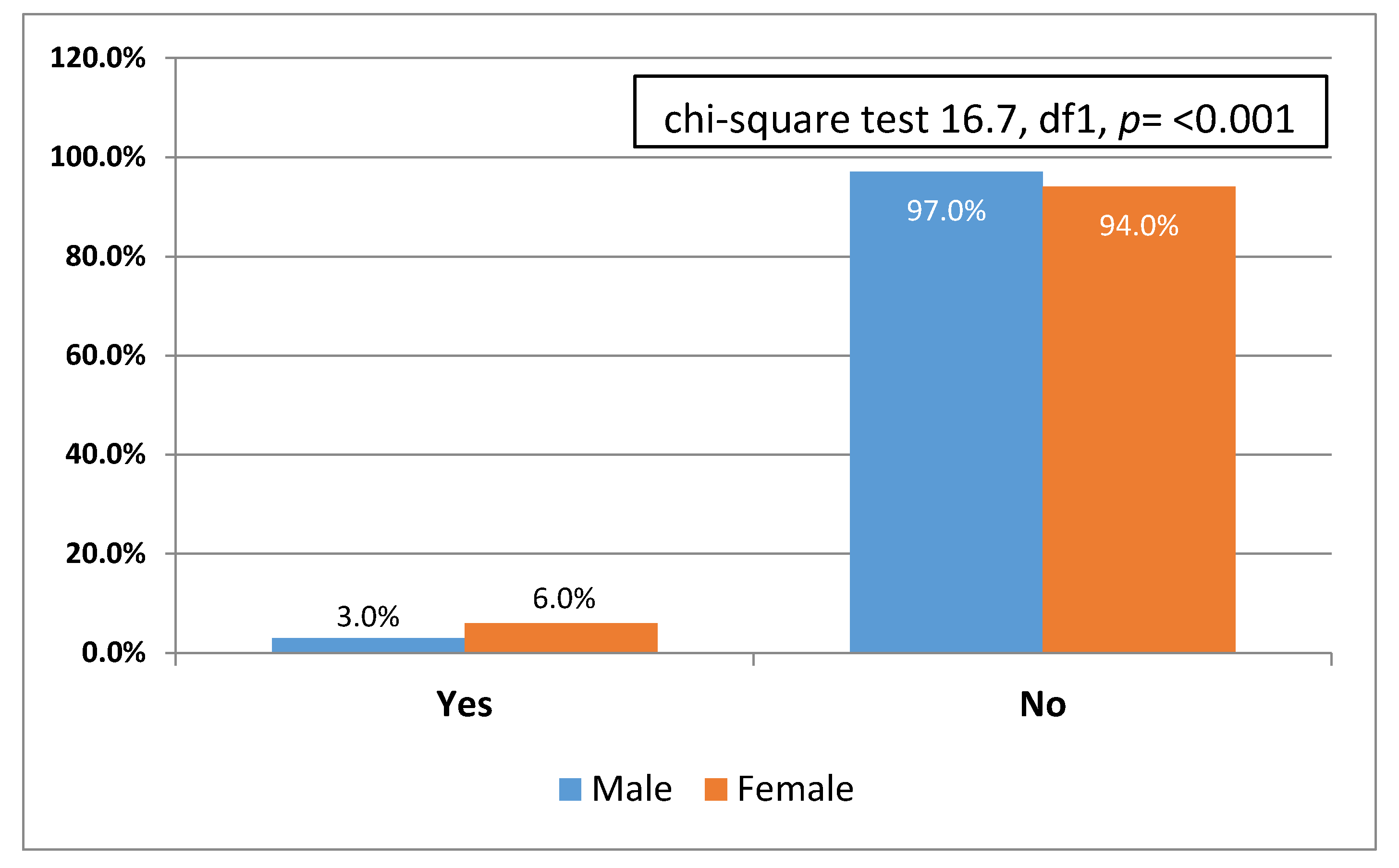
Figure 23, we also summarize a very delicate factor of trainees’ satisfaction related to sexual harassment. The percentage is low related to international benchmarks but it seems that females experience verbal sexual harassment twice as frequently as males. This is also another significant key direction for future research.
In the next section, we provide our key interpretations of the findings and we also contribute theoretically with a progressive model for Trainees’ Satisfaction. We must provide the following significant statements for the end of this Analysis of findings section:
Some of the collected data and their relevant analysis are only for internal use in the SCFHS. In this research paper, we focus on data and findings that can be shared publicly to promote knowledge in the domain of Sustainable Health
Our intention in this research is to build a systematic, trusted set of benchmarks for the study of residents’ satisfaction in their medical Training Programs. In future research, we intend to further study the cause and effect relationships for the key findings of this research. This seems to be a limitation factor for the current study but our current contribution remains unique, bold, and significant. Our study is one of the first to analyze resident population issues related to satisfaction at such a large scale.
6. Conclusions, Limitations, and Future Research
Our research study is a systematic effort to understand residents’ attitudes related to job satisfaction. In such a complicated research environment, we tried at a first stage to obtain a comprehensive picture of the phenomenon.
Our research study is one of the first in KSA as well as worldwide, with a special emphasis on a thorough understanding of issues affecting the job satisfaction of residents at a major scale. In comparison to other studies, we have obtained a significant achievement by obtaining almost 4000 questionnaire results from a major portion of the whole population of residents in the KSA. A key limitation of our research is that all findings and key interpretations refer to the current snapshot of the professional and academic conduct of trainees. Thus, the generalization of findings must be made while taking into consideration that we only studied residents from the Kingdom of the Saudi Arabia.
One more limitation of this survey is that we intended to develop a thorough trusted initial benchmark for various components of trainees’ satisfaction. We do believe that the outcome of our intellectual effort and research methodology enabled summarizing a clear overview of trainees’ satisfaction benchmarks at present. We have to admit though that especially in this study, we did not provide the same effort towards analyzing the cause and effect relations of the trainee satisfaction phenomenon. We plan to shortly run a new survey based on structural equation modeling to further inform our key findings. The ultimate objective is also to update our recently published set of Key Performance Indicators (KPIs) for the Quality of Residents Training with an additional set of KPIs related to residents’ satisfaction.
One additional limitation of our study is the disclosure of significant information. Some of the aspects and findings of our survey must be used only for internal use of the Saudi Commission of the Health Specialties, since they refer to indirect evaluation and assessment of various training centers supervised by the SCFHS. Finally, we have also to communicate that this research study refers to a certain period, and thus all the findings and conclusions must be interpreted within the given time. Any effort to extend the validity of the findings for the future must be made with special care and conditions. We do believe though that all the key findings have direct implications on the launching of revised policies for the enhancement of the Training Programs and trainee satisfaction.
We also contributed significantly by summarizing key hermeneutic factors for the job satisfaction of trainees and we also introduced some key benchmarks for the measurement of its rate. Our work contributes to the literature of job satisfaction in medical training by introducing new measurable benchmarks.
It also serves as a key methodological approach for the introduction of reflective actions in different areas of residency including the academic activities, the Training Program, the Training Center, the collegiality, the psychological load of residents, and their interactions with the administration and the residency supervising bodies.
It is also a bold contribution to Sustainable Health literature, since it promotes a vision for enhanced skills and competencies of health specialists with a balance of life and work. It is also linked to the discussion and the debate on Sustainable Development Goals as introduced by the United Nations. The Sustainable Development Goal #3—Establish Good Health and Well-Being—must also extend to health specialists. The promotion of good mental health and wellbeing of health experts must be a priority of modern societies. Within this context, our work is also directly related to the Sustainable Development Goal #4—Provide Quality Education. Our main interest in this study is to understand the conditions and requirements that make residents happy and efficient in their training and professional conduct. Last but not least, our work also contributed to the Sustainable Health Vision through the SDG #8 Create Decent Work and Economic Growth. It is a key responsibility of the SCFHS to promote the professional capacity of residents so that the Future Saudi Society will enjoy having high-skilled health experts with a strong sense of social responsibility and high efficiency.
In the near future, we intend to further extend our theoretical model in the following directions: (i) Delivery of a research study based on Structural Equation Modeling to understand the contribution of each of the factors to the Quality of Residents’ Training and the effectiveness of knowledge creation [
50]; (ii) the design and implementation of an innovative Artificial Intelligence enabled ecosystem for personalized training based on key assumptions of our model [
51]; (iii) focused research on the key determinants and hermeneutic variables of Human Factors affecting residents’ education; [iv] the integration of smart cities research and smart healthcare strategies [
52,
53] under the vision of the Kingdom 2030 Digital Transformation of Healthcare.

 ,
, 
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}