Healthy Diet Assistance for the Most Deprived in Post-Crisis Greece: An Evaluation of the State Food Provision Program

 , ,
, ,
Abstract
:1. Introduction
2. Methodology
2.1. Calculation of FEAD Food Provisions Delivered to Beneficiaries
2.1.1. Data Collection
2.1.2. Mapping of the Food Items Provided
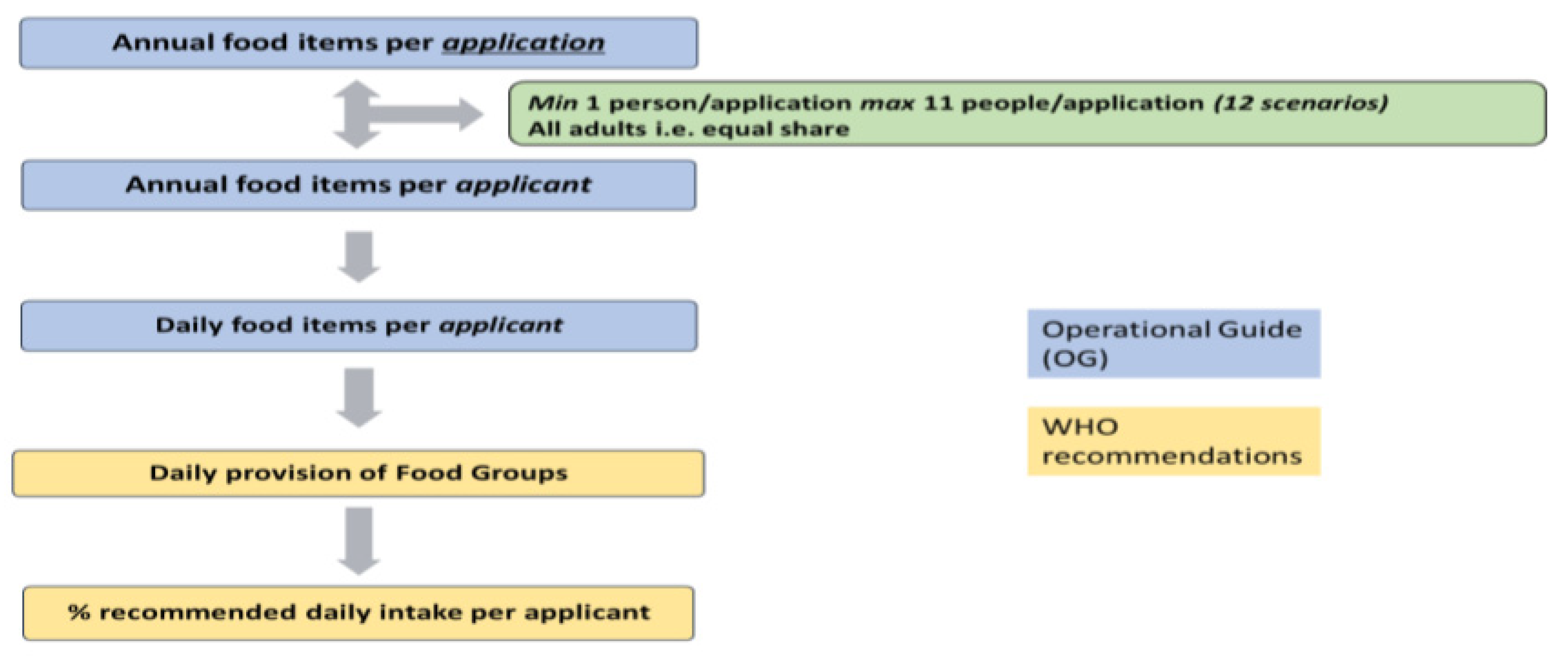
2.1.3. Calculation of FEAD’s Contribution toward the Achievement of a Healthy Diet
2.2. Beneficiaries’ Evaluation of the FEAD Program
Data Collection and Research Design
3. Statistical Analysis
4. Results
4.1. Calculation of FEAD Food Provisions Delivered to Beneficiaries
4.1.1. Mapping of Food Items Delivered by Each FEAD Supply Chain
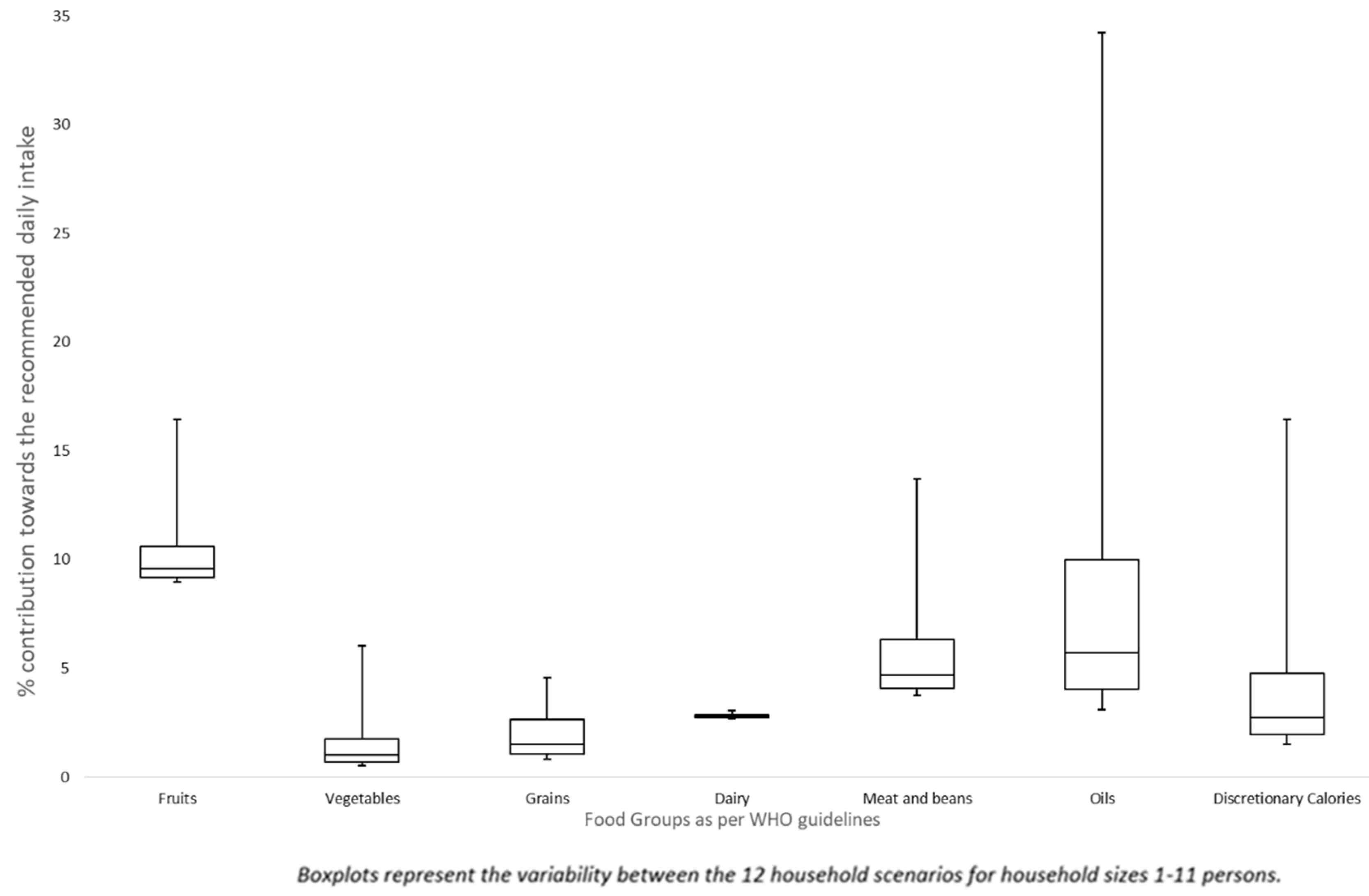
4.1.2. Contribution of Centralized Suppliers to Recommended Dietary Intake
4.1.3. Contribution of Decentralized Suppliers to Recommended Dietary Intake
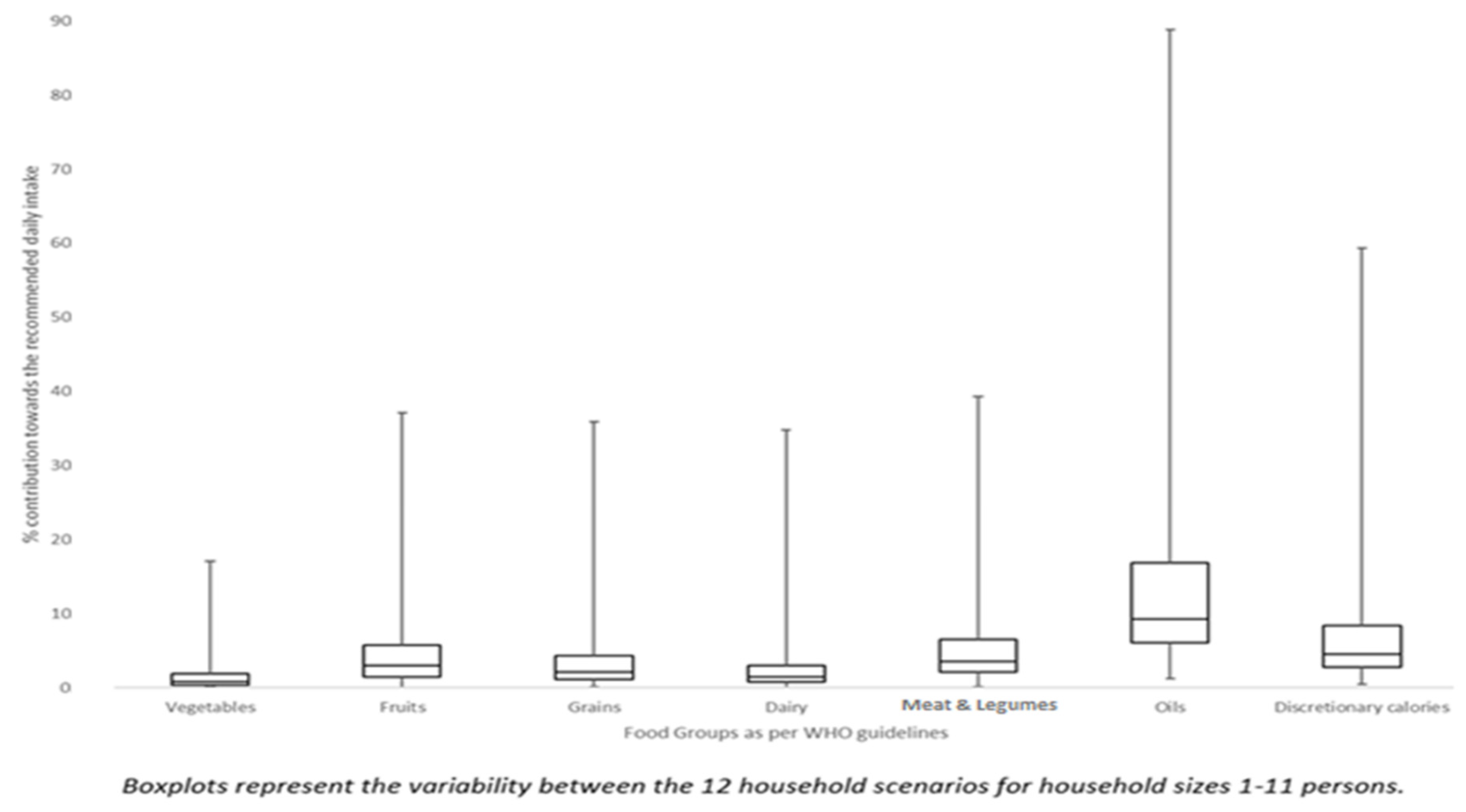
4.1.4. Total Contribution
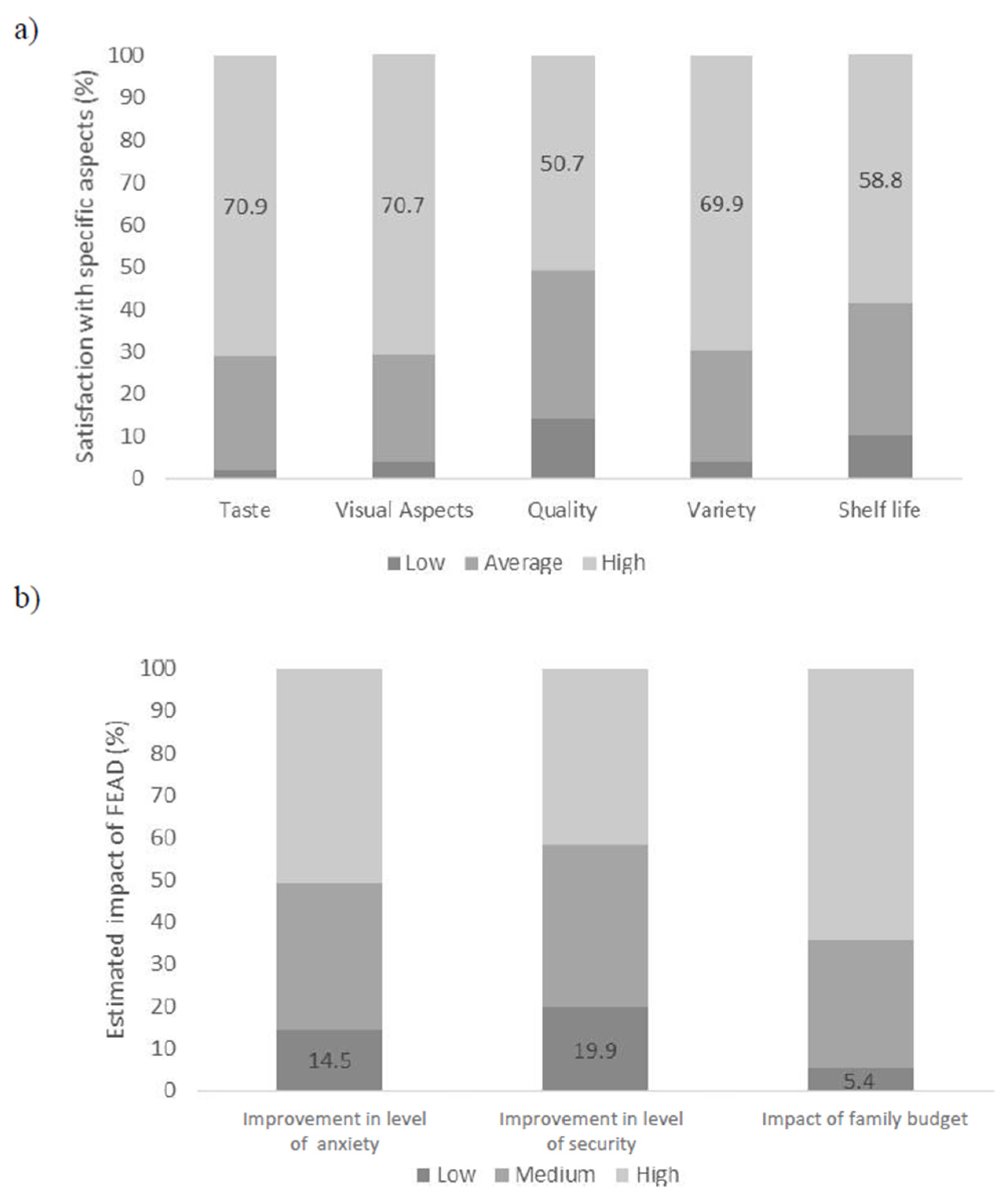
4.2. Beneficiaries’ Evaluation of the FEAD Program
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percentage of the Daily Recommended Intake Covered per Food Group per Person | |||||||
|---|---|---|---|---|---|---|---|
| Number of Members per Application | Fruits (%) | Vegetables (%) | Grains (%) | Dairy (%) | Meat and Legumes (%) | Oils (%) | Discretionary Calories (%) |
| 1 | 16.44 | 6.03 | 4.57 | 3.04 | 13.70 | 34.25 | 16.44 |
| 2 | 12.33 | 3.01 | 4.57 | 3.04 | 8.99 | 17.12 | 8.22 |
| 3 | 10.96 | 2.01 | 3.04 | 2.91 | 6.85 | 11.42 | 5.48 |
| 4 | 10.27 | 1.51 | 2.28 | 2.84 | 5.78 | 8.56 | 4.11 |
| 5 | 9.86 | 1.21 | 1.83 | 2.80 | 5.14 | 6.85 | 3.29 |
| 6 | 9.59 | 1.00 | 1.52 | 2.77 | 4.71 | 5.71 | 2.74 |
| 7 | 9.39 | 0.86 | 1.30 | 2.75 | 4.40 | 4.89 | 2.35 |
| 8 | 9.25 | 0.75 | 1.14 | 2.73 | 4.17 | 4.28 | 2.05 |
| 9 | 9.13 | 0.67 | 1.01 | 2.72 | 4.00 | 3.81 | 1.83 |
| 10 | 9.04 | 0.60 | 0.91 | 2.71 | 3.85 | 3.42 | 1.64 |
| 11 | 8.97 | 0.55 | 0.83 | 2.71 | 3.74 | 3.11 | 1.49 |

References
- Food and Agriculture Organization of the United Nations. Declaration of the World Summit on Food Security. World Food Summit. 2009. Available online: www.fao.org (accessed on 22 December 2020).
- Vilar-Compte, M.; Sandoval-Olascoaga, S.; Bernal-Stuart, A.; Shimoga, S.; Vargas-Bustamante, A. The impact of the 2008 financial crisis on food security and food expenditures in Mexico: A disproportionate effect on the vulnerable. Public Health Nutr. 2015, 18, 2934. [Google Scholar] [CrossRef] [Green Version]
- Von Braun, J. Food and Financial Crises: Implications for Agriculture and the Poor; International Food Policy Research Institute: Washington, DC, USA, 2008. [Google Scholar]
- Nawrotzki, R.J.; Robson, K.; Gutilla, M.J.; Hunter, L.M.; Twine, W.; Norlund, P. Exploring the impact of the 2008 global food crisis on food security among vulnerable households in rural South Africa. Food Secur. 2014, 6, 283–297. [Google Scholar] [CrossRef] [Green Version]
- Metis, G. FEAD Mid-Term Evaluation, Interim Report; European Commision, Directorate General for Employment, Social Affairs and Inclusion: Brussels, Belgium, 2018. [Google Scholar]
- Loopstra, R.; Reeves, A.; Stuckler, D. Rising food insecurity in Europe. Lancet 2015, 385, 2041. [Google Scholar] [CrossRef]
- Swinnen, J.; van Herck, K. Food Security: Challenges and Opportunities for Eastern Europe and Central Asia. Asian J. Agric. Dev. 2012, 9, 1–16. [Google Scholar]
- Food and Agriculture Organization of the United Nations; International Fund for Agricultural Development; UNICEF; World Food Program; World Health Organization. The State of Food Security and Nutrition in the World 2018; FAO: Rome, Italy, 2018. [Google Scholar]
- Food and Agriculture Organization of the United Nations; International Fund for Agricultural Development; UNICEF; World Food Program; World Health Organization. The State of Food Security and Nutrition in the World 2019; Safeguarding against Economic Slowdowns and Downturns; FAO: Rome, Italy, 2019. [Google Scholar]
- Gundersen, C. Food Insecurity Is an Ongoing National Concern. Adv Nutr. 2013, 4, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Garratt, E. Food insecurity in Europe: Who is at risk, and how successful are social benefits in protecting against food insecurity? J. Soc. Policy 2019, 49, 1–25. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Healthy Diet. Media Cent [Internet]. 2015, pp. 1–6. Available online: http://www.who.int/mediacentre/factsheets/fs394/en/ (accessed on 22 December 2020).
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; MacKenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Eurostat. Regional Yearbook 2017 Edition; Eurostat: Luxembourg, 2017. [Google Scholar]
- Tyrovolas, S.; Kassebaum, N.J.; Stergachis, A.; Abraha, H.N.; Alla, F.; Androudi, S.; Car, M.; Chrepa, V.; Fullman, N.; Fürst, T.; et al. The burden of disease in Greece, health loss, risk factors, and health financing, 2000–2016: An analysis of the Global Burden of Disease Study 2016. Lancet Public Health 2018, 3, e395–e406. [Google Scholar] [CrossRef] [Green Version]
- Kleanthous, K.; Dermitzaki, E.; Papadimitriou, D.T.; Papaevangelou, V.; Papadimitriou, A. Overweight and obesity decreased in Greek schoolchildren from 2009 to 2012 during the early phase of the economic crisis. Acta Paediatr. 2016, 105, 200–205. [Google Scholar] [CrossRef]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Current data in Greek children indicate decreasing trends of obesity in the transition from childhood to adolescence; Results from the National Action for Children’s Health (EYZHN) program. J. Prev. Med. Hyg. 2018, 59, E36–E47. [Google Scholar]
- Chatzivagia, E.; Pepa, A.; Vlassopoulos, A.; Kapsokefalou, M.; Malisova, O.; Filippou, K. Nutrition transition in the post-economic crisis of Greece: Assessing the nutritional gap of food-insecure individuals. A cross-sectional study. Nutrients 2019, 11, 2914. [Google Scholar] [CrossRef] [Green Version]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef]
- United Nations General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015, pp. 1–5. Available online: https://sustainabledevelopment.un.org/content/documents/7891Transforming (accessed on 22 December 2020).
- FEAD Greece Managing Authority. Implementation Guide for the Operational Programme I Food and Basic Material Assistance from FEAD, 2nd ed.; FEAD Greece Managing Authority, 2015; Available online: http://teba.eiead.gr/?lang=en (accessed on 9 December 2020).
- WHO Regional Office for Europe. Better Food and Nutrition in Europe: Progress Report. 2018. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/publications/2018/better-food-and-nutrition-in-europe-progress-report-2018 (accessed on 22 December 2020).
- European Commission. Regulation (EU) No 223/2014 of the European Parliament and of the Council of 11 March 2014 on the Fund for European Aid to the Most Deprived. Off. J. Eur. Union. 2012, 57, 10. [Google Scholar]
- Lawson, L.; Quick, V.; Taylor, M.; Kapsokefalou, M.; Kotsiow, P.; Rao, S.; Schoolman, E. Food Aid and the Emergency Food System in Greece. June 2017. Available online: http://agriurban.rutgers.edu/Documents/Greek_report.pdf (accessed on 3 April 2020).
- World Health Organisation. Promoting a healthy diet for the WHO Eastern Mediterranean Region: User-friendly guide; World Health Organisation: Geneva, Switzerland, 2012; 41p. [Google Scholar]
- Cotugna, N.; Vickery, C.E.; Glick, M. An outcome evaluation of a food bank program. J. Am. Diet. Assoc. 1994, 94, 888–890. [Google Scholar] [CrossRef]
- Wang, K.Y.-T.; Lyu, L.-C. The emergence of food bank/voucher programs in Taiwan: A new measure for combating poverty and food insecurity? Asia Pac. J. Soc. Work Dev. 2013, 23, 48–58. [Google Scholar] [CrossRef]
- Whiteman, E.D.; Chrisinger, B.W.; Hillier, A. Diet Quality Over the Monthly Supplemental Nutrition Assistance Program Cycle. Am. J. Prev. Med. 2018, 55, 205–212. [Google Scholar] [CrossRef]
- Teron, A.C.; Tarasuk, V.S. Charitable Food Assistance: What are Food Bank Users Receiving? Can. J. Public Health 1999, 90, 382–384. Available online: http://0-www-jstor-org.brum.beds.ac.uk/stable/41994160 (accessed on 22 December 2020). [CrossRef]
- Kang, S.; Hong, M.; Yang, I.; Jo, M.; Kim, C. Analysis on the Characteristics of Government-dominant and Non-governmental Food Bank Programs from the Users’ Perspective. Korean J. Community Nutr. 2005, 10, 224–233. [Google Scholar]
- Kang, S.; Yang, I.; Lee, Y. Investigation of the Conditions and Evaluation of the Benefits of the Foodbank Program from the Recipients’ Perspective. Korean J. Community Nutr. 2003, 8, 231–239. [Google Scholar]
- Simmet, A.; Depa, J.; Tinnemann, P.; Stroebele-Benschop, N. The Dietary Quality of Food Pantry Users: A Systematic Review of Existing Literature. J. Acad. Nutr. Diet. 2017, 117, 563–576. [Google Scholar] [CrossRef]
- Bazerghi, C.; McKay, F.H.; Dunn, M. The Role of Food Banks in Addressing Food Insecurity: A Systematic Review. J. Community Health 2016, 41, 732–740. [Google Scholar] [CrossRef]
- Castetbon, K.; Méjean, C.; Deschamps, V.; Bellin-Lestienne, C.; Oleko, A.; Darmon, N.; Hercberg, S. Dietary behaviour and nutritional status in underprivileged people using food aid (ABENA study, 2004–2005). J. Hum. Nutr. Diet. 2011, 24, 560–571. [Google Scholar] [CrossRef]
- Robaina, K.A.; Martin, K.S. Food Insecurity, Poor Diet Quality, and Obesity among Food Pantry Participants in Hartford, CT. J. Nutr. Educ. Behav. 2013, 45, 159–164. [Google Scholar] [CrossRef]
- Depa, J.; Hilzendegen, C.; Tinnemann, P.; Stroebele-Benschop, N. An explorative cross-sectional study examining self-reported health and nutritional status of disadvantaged people using food banks in Germany. Int. J. Equity Health 2015, 14, 141. [Google Scholar] [CrossRef] [Green Version]
- Neter, J.E.; Dijkstra, S.C.; Visser, M.; Brouwer, I.A. Dutch food bank parcels do not meet nutritional guidelines for a healthy diet. Br. J. Nutr. 2016, 116, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, T.; Sun, B.; Dixit-Joshi, S. Nutrient and Food Group Analysis of USDA Foods in Five of Its Food and Nutrition Programs—2014; USDA-FNS: Washington, DC, USA, 2016. [Google Scholar]
- Verpy, H.; Smith, C.; Riecks, M. Attitudes and behaviors of food donors and perceived needs and wants of food shelf clients. J. Nutr. Educ. Behav. 2003, 35, 6–15. [Google Scholar] [CrossRef]
- Azurdia, A.X.; Lecompte, E.; Sibbald, E. Bon Appétit! A Process Evaluation of a Campus-Based Food Bank. J. Hunger. Environ. Nutr. 2011, 6, 324–342. Available online: http://0-www-tandfonline-com.brum.beds.ac.uk/doi/abs/10.1080/19320248.2011.597834 (accessed on 1 March 2020). [CrossRef]
- Tarasuk, V.; Eakin, J.M. Food assistance through “surplus” food: Insights from an ethnographic study of food bank work. Agric. Hum. Values 2005, 22, 177–186. [Google Scholar] [CrossRef]
- Seidel, M.; Laquatra, I.; Woods, M.; Sharrard, J. Applying a Nutrient-Rich Foods Index Algorithm to Address Nutrient Content of Food Bank Food. J. Acad. Nutr. Diet. 2015, 115, 695–700. [Google Scholar] [CrossRef]
- Campbell, E.C.; Ross, M.; Webb, K.L. Improving the Nutritional Quality of Emergency Food: A Study of Food Bank Organizational Culture, Capacity, and Practices. J. Hunger. Environ. Nutr. 2013, 8, 261–280. Available online: http://0-www-tandfonline-com.brum.beds.ac.uk/doi/abs/10.1080/19320248.2013.816991 (accessed on 1 March 2020). [CrossRef]
- Grieger, J.A.; Johnson, B.J.; Wycherley, T.P.; Golley, R.K. Evaluation of Simulation Models that Estimate the Effect of Dietary Strategies on Nutritional Intake: A Systematic Review. J. Nutr. 2017, 147, 908–931. [Google Scholar] [CrossRef] [Green Version]
- Pearson-Stuttard, J.; Bandosz, P.; Rehm, C.D.; Penalvo, J.; Whitsel, L.; Gaziano, T.; Conrad, Z.; Wilde, P.; Micha, R.; Lloyd-Williams, F.; et al. Reducing US cardiovascular disease burden and disparities through national and targeted dietary policies: A modelling study. PLoS Med. 2017, 14, e1002311. [Google Scholar] [CrossRef]
- Ibok, O.W.; Osbahr, H.; Srinivasan, C. Advancing a new index for measuring household vulnerability to food insecurity. Food Policy 2019, 84, 10–20. [Google Scholar] [CrossRef]




| Foods Procured by the Centralized Suppliers | Social Partnerships That Distributed These Foods (%) | Foods Procured by the Decentralized Suppliers | Social Partnerships That Distributed These Foods (%) | |
|---|---|---|---|---|
| Fruits | Oranges | 35% | Kiwi | 4% |
| Peach | 4% | |||
| Apples | 39% | Canned Fruit | 30% | |
| Marmalade | 30% | |||
| Vegetables | Cabbage | 17% | Carrot | 4% |
| Zucchini | 9% | |||
| Tomato Juice Concentrate | 56% | Tomato | 4% | |
| Eggplant | 4% | |||
| Onion | 4% | |||
| Cereals & Starch | Spaghetti | 83% | Rice | 39% |
| Flour | 40% | |||
| Cornflakes | 26% | |||
| Potato | 17% | |||
| Melba Toast | 4% | |||
| Dairy | Feta Cheese | 70% | Hard Cheese | 39% |
| Condensed Milk | 70% | |||
| Meat & Legumes | Fresh Chicken | 43% | Fresh Turkey | 4% |
| Fresh Boneless Pork | 70% | Chicken Soup | 26% | |
| Fresh Boneless Beef | 78% | |||
| White Dry Beans | 70% | |||
| Lentils | 65% | |||
| Fats & Oils | Olive Oil | 48% | Margarine | 4% |
| Sunflower Oil | 26% | |||
| Olives | 26% | |||
| Free Sugars | Sugar | 52% | Honey | 30% |
| Total (n = 1891) | |
|---|---|
| Female (%) | 52.2 |
| Age (years) | 48.1 ± 12.7 |
| Education (years) | 9.90 ± 6.0 |
| Children (#) | 2.02 ± 1.9 |
| Household size (# people) | 2.87 ± 1.6 |
| Currently married (%) | 47.7 |
| Currently employed (%) | 13.4 |
| Duration of FEAD enrollment (months) | 12.74 ± 8.4 |
| Beneficiaries per application (#) | 2.55 ± 1.6 |
| Food deliveries received (#) | 3.54 ± 4.3 |
| Personal hygiene item deliveries received (#) | 2.30 ± 9.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlassopoulos, A.; Filippou, K.; Pepa, A.; Malisova, O.; Xenaki, D.; Kapsokefalou, M. Healthy Diet Assistance for the Most Deprived in Post-Crisis Greece: An Evaluation of the State Food Provision Program. Sustainability 2021, 13, 99. https://0-doi-org.brum.beds.ac.uk/10.3390/su13010099
Vlassopoulos A, Filippou K, Pepa A, Malisova O, Xenaki D, Kapsokefalou M. Healthy Diet Assistance for the Most Deprived in Post-Crisis Greece: An Evaluation of the State Food Provision Program. Sustainability. 2021; 13(1):99. https://0-doi-org.brum.beds.ac.uk/10.3390/su13010099
Chicago/Turabian StyleVlassopoulos, Antonis, Konstantina Filippou, Aleks Pepa, Olga Malisova, Dimitra Xenaki, and Maria Kapsokefalou. 2021. "Healthy Diet Assistance for the Most Deprived in Post-Crisis Greece: An Evaluation of the State Food Provision Program" Sustainability 13, no. 1: 99. https://0-doi-org.brum.beds.ac.uk/10.3390/su13010099