
Effects of Acute-Partial Sleep Deprivation on High-Intensity Exercise Performance and Cardiac Autonomic Activity in Healthy Adolescents








Abstract
:1. Introduction
2. Materials and Methods
2.1. Screening of Participants
2.2. Preliminary Testing
2.3. Experimental Conditions
2.3.1. Sleep Deprivation Protocol
2.3.2. High-Intensity Exercise Protocol
2.4. HRV Collection and Analysis
2.5. Statistical Analysis
3. Results
3.1. Pre-Experimental Data
3.2. Effects of Acute-Partial Sleep Deprivation on HIE Performance
3.3. Results for HRV Indices
3.3.1. Two-Way rmANOVA for Main Effect
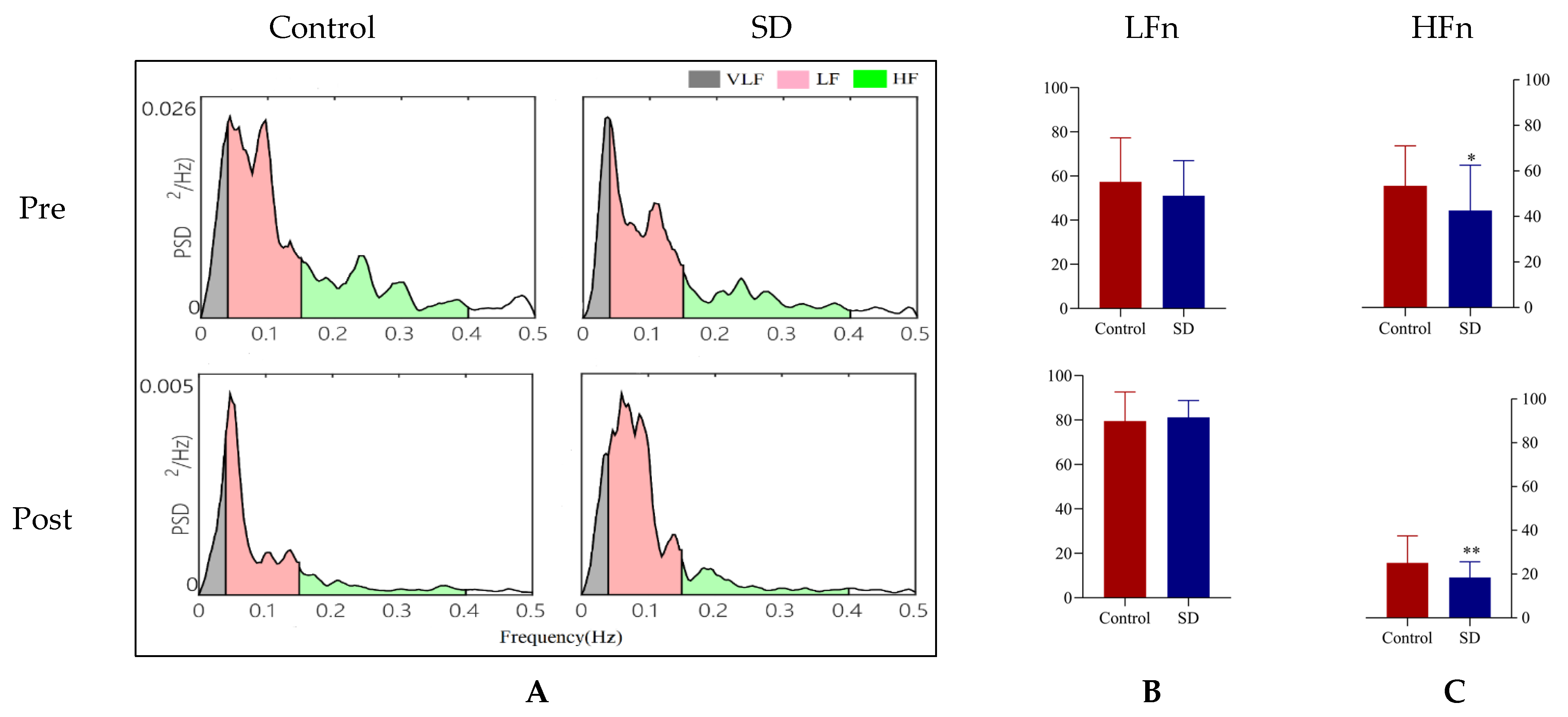
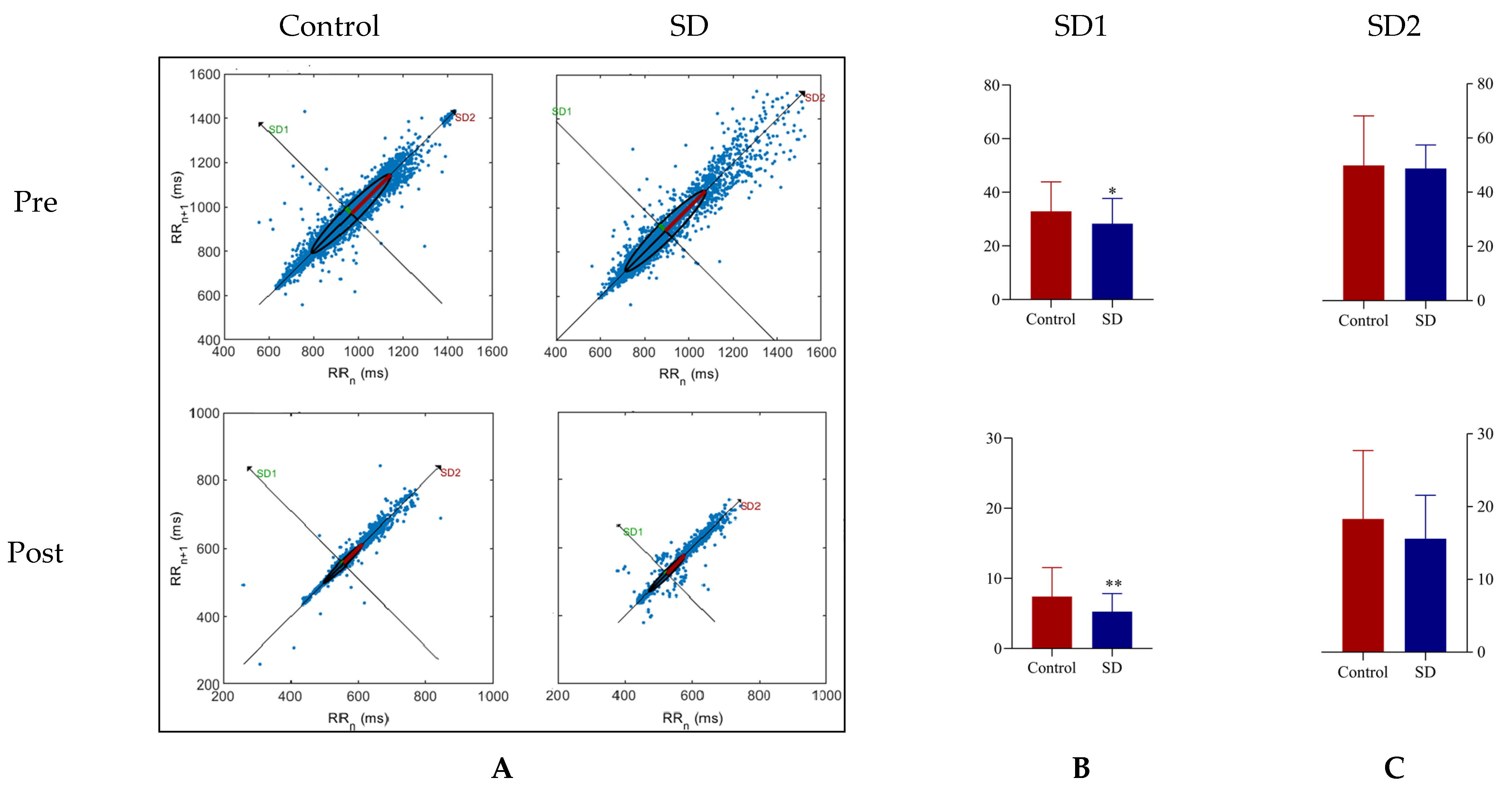
3.3.2. Effects of Acute-Partial Sleep Deprivation on HRV
3.3.3. Effects of Interaction of Acute-Partial Sleep Deprivation and HIE on HRV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meng, Q.; Zhang, J.; Kang, J.; Wu, Y. Effects of sound environment on the sleep of college students in China. Sci. Total Environ. 2020, 705, 135794. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Adams Hillard, P.J.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef]
- Toda, H.; Williams, J.A.; Gulledge, M.; Sehgal, A. A sleep-inducing gene, nemuri, links sleep and immune function in Drosophila. Science 2019, 363, 509–515. [Google Scholar] [CrossRef]
- da Costa Souza, A.; Ribeiro, S. Sleep deprivation and gene expression. Curr. Top. Behav. Neurosci. 2015, 25, 65–90. [Google Scholar]
- Morgan, D.; Tsai, S.C. Sleep and the Endocrine System. Sleep Med. Clin. 2016, 11, 115–126. [Google Scholar] [CrossRef]
- Huang, T.; Mariani, S.; Redline, S. Sleep Irregularity and Risk of Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis. J. Am. Coll. Cardiol. 2020, 75, 991–999. [Google Scholar] [CrossRef]
- Covassin, N.; Singh, P. Sleep Duration and Cardiovascular Disease Risk: Epidemiologic and Experimental Evidence. Sleep Med. Clin. 2016, 11, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiper, N.C.; Ridenour, T.A.; Fishbein, D.H. Characterizing psychiatric symptoms and neurocognitive functioning among substance-naïve early adolescents: Associations with sleep problems. Early Interv. Psychiatry 2020, 14, 439–449. [Google Scholar] [CrossRef]
- Yang, H.; Baltzis, D.; Bhatt, V.; Haack, M.; Meier-Ewert, H.K.; Gautam, S.; Veves, A.; Mullington, J.M. Macro- and microvascular reactivity during repetitive exposure to shortened sleep: Sex differences. Sleep 2021, 44, zsaa257. [Google Scholar] [CrossRef]
- Mellman, T.A.; Bell, K.A.; Abu-Bader, S.H.; Kobayashi, I. Neighborhood stress and autonomic nervous system activity during sleep. Sleep 2018, 41, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Yamanaka, Y.; Hashimoto, S.; Takasu, N.N.; Tanahashi, Y.; Nishide, S.Y.; Honma, S.; Honma, K. Morning and evening physical exercise differentially regulate the autonomic nervous system during nocturnal sleep in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R1112–R1121. [Google Scholar] [CrossRef] [Green Version]
- Kiss, O.; Sydó, N.; Vargha, P.; Vágó, H.; Czimbalmos, C.; Édes, E.; Zima, E.; Apponyi, G.; Merkely, G.; Sydó, T.; et al. Detailed heart rate variability analysis in athletes. Clin. Auton. Res. 2016, 26, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Hilton, H.J.; Gates, G.J.; Jelic, S.; Stern, Y.; Bartels, M.N.; Demeersman, R.E.; Basner, R.C. Increased sympathetic and decreased parasympathetic cardiovascular modulation in normal humans with acute sleep deprivation. J. Appl. Physiol. 2005, 98, 2024–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glos, M.; Fietze, I.; Blau, A.; Baumann, G.; Penzel, T. Cardiac autonomic modulation and sleepiness: Physiological consequences of sleep deprivation due to 40 h of prolonged wakefulness. Physiol. Behav. 2014, 125, 45–53. [Google Scholar] [CrossRef]
- Boutcher, Y.N.; Boutcher, S.H. Exercise intensity and hypertension: What’s new? J. Hum. Hypertens. 2017, 31, 157–164. [Google Scholar] [CrossRef]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil Clin. N. Am. 2017, 28, 659–669. [Google Scholar] [CrossRef] [PubMed]
- González-Gross, M.; Meléndez, A. Sedentarism, active lifestyle and sport: Impact on health and obesity prevention. Nutr. Hosp. 2013, 28 (Suppl. 5), 89–98. [Google Scholar]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Venn, D.; Strazdins, L. Your money or your time? How both types of scarcity matter to physical activity and healthy eating. Soc. Sci. Med. 2017, 172, 98–106. [Google Scholar] [CrossRef]
- Zouhal, H.; Saeidi, A.; Salhi, A.; Li, H.; Essop, M.F.; Laher, I.; Rhibi, F.; Amani-Shalamzari, S.; Ben Abderrahman, A. Exercise Training and Fasting: Current Insights. Open Access J. Sports Med. 2020, 11, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallis, G.A.; Gonzalez, J.T. Is exercise best served on an empty stomach? Proc. Nutr. Soc. 2019, 78, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Aird, T.P.; Davies, R.W.; Carson, B.P. Effects of fasted vs. fed-state exercise on performance and post-exercise metabolism: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2018, 28, 1476–1493. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.F.; Costa, R.R.; Macedo, R.C.; Coconcelli, L.; Kruel, L.F. Effects of aerobic exercise performed in fasted v. fed state on fat and carbohydrate metabolism in adults: A systematic review and meta-analysis. Br. J. Nutr. 2016, 116, 1153–1164. [Google Scholar] [CrossRef] [Green Version]
- De Bock, K.; Richter, E.A.; Russell, A.P.; Eijnde, B.O.; Derave, W.; Ramaekers, M.; Koninckx, E.; Léger, B.; Verhaeghe, J.; Hespel, P. Exercise in the fasted state facilitates fibre type-specific intramyocellular lipid breakdown and stimulates glycogen resynthesis in humans. J. Physiol. 2005, 564 Pt 2, 649–660. [Google Scholar] [CrossRef]
- Venables, M.C.; Jeukendrup, A.E. Endurance training and obesity: Effect on substrate metabolism and insulin sensitivity. Med. Sci. Sports Exerc. 2008, 40, 495–502. [Google Scholar] [CrossRef]
- Abedelmalek, S.; Chtourou, H.; Aloui, A.; Aouichaoui, C.; Souissi, N.; Tabka, Z. Effect of time of day and partial sleep deprivation on plasma concentrations of IL-6 during a short-term maximal performance. Eur. J. Appl. Physiol. 2013, 113, 241–248. [Google Scholar] [CrossRef]
- Roberson, P.A.; Chase, J.D.; Bigman, M.B.; Saunders, M.J.; Luden, N.D.; Womack, C.J. Time of day, but not sleep restriction, affects markers of hemostasis following heavy exercise. Appl. Physiol. Nutr. Metab. 2019, 44, 148–152. [Google Scholar] [CrossRef]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Julian, R.; Bartlett, J.; Meyer, T. Impaired sleep and recovery after night matches in elite football players. J. Sports Sci. 2016, 34, 1333–1339. [Google Scholar] [CrossRef]
- Mejri, M.A.; Yousfi, N.; Mhenni, T.; Tayech, A.; Hammouda, O.; Driss, T.; Chaouachi, A.; Souissi, N. Does one night of partial sleep deprivation affect the evening performance during intermittent exercise in Taekwondo players? J. Exerc. Rehabil. 2016, 12, 47–53. [Google Scholar] [CrossRef]
- Souissi, N.; Souissi, M.; Souissi, H.; Chamari, K.; Tabka, Z.; Dogui, M.; Davenne, D. Effect of time of day and partial sleep deprivation on short-term, high-power output. Chronobiol. Int. 2008, 25, 1062–1076. [Google Scholar] [CrossRef]
- Vitale, K.C.; Owens, R.; Hopkins, S.R.; Malhotra, A. Sleep Hygiene for Optimizing Recovery in Athletes: Review and Recommendations. Int. J. Sports Med. 2019, 40, 535–543. [Google Scholar] [CrossRef]
- Antunes, B.M.; Campos, E.Z.; Parmezzani, S.S.; Santos, R.V.; Franchini, E.; Lira, F.S. Sleep quality and duration are associated with performance in maximal incremental test. Physiol. Behav. 2017, 177, 252–256. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A.; Hale, L.; Moore, M.; Patel, N.P. Mortality associated with short sleep duration: The evidence, the possible mechanisms, and the future. Sleep Med. Rev. 2010, 14, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Chase, J.D.; Roberson, P.A.; Saunders, M.J.; Hargens, T.A.; Womack, C.J.; Luden, N.D. One night of sleep restriction following heavy exercise impairs 3-km cycling time-trial performance in the morning. Appl. Physiol. Nutr. Metab. 2017, 42, 909–915. [Google Scholar] [CrossRef]
- Khan, A.A.; Lip, G.Y.H.; Shantsila, A. Heart rate variability in atrial fibrillation: The balance between sympathetic and parasympathetic nervous system. Eur. J. Clin. Investig. 2019, 49, e13174. [Google Scholar] [CrossRef] [Green Version]
- Kaltsatou, A.; Hadjigeorgiou, G.M.; Grigoriou, S.S.; Karatzaferi, C.; Giannaki, C.D.; Lavdas, E.; Fotiou, D.; Kouidi, E.; Patramani, G.; Vogiatzi, C.; et al. Cardiac autonomic function during intradialytic exercise training. Postgrad. Med. 2019, 131, 539–545. [Google Scholar] [CrossRef]
- Tan, J.P.H.; Beilharz, J.E.; Vollmer-Conna, U.; Cvejic, E. Heart rate variability as a marker of healthy ageing. Int. J. Cardiol. 2019, 275, 101–103. [Google Scholar] [CrossRef]
- Zhang, L.; Wu, H.; Zhang, X.; Wei, X.; Hou, F.; Ma, Y. Sleep heart rate variability assists the automatic prediction of long-term cardiovascular outcomes. Sleep Med. 2020, 67, 217–224. [Google Scholar] [CrossRef]
- Lee, H.J.; Hwang, S.H.; Yoon, H.N.; Lee, W.K.; Park, K.S. Heart Rate Variability Monitoring during Sleep Based on Capacitively Coupled Textile Electrodes on a Bed. Sensors 2015, 15, 11295–11311. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.N.; Tian, H.; Chen, P.; Wang, D.; Ren, J.; Zhang, Y. Physical Exercise and Selective Autophagy: Benefit and Risk on Cardiovascular Health. Cells 2019, 8, 1436. [Google Scholar] [CrossRef] [Green Version]
- Michael, S.; Jay, O.; Halaki, M.; Graham, K.; Davis, G.M. Submaximal exercise intensity modulates acute post-exercise heart rate variability. Eur. J. Appl. Physiol. 2016, 116, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Alansare, A.; Alford, K.; Lee, S.; Church, T.; Jung, H.C. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. Int. J. Environ. Res. Public Health 2018, 15, 1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itagi, A.B.H.; Patil, N.A.; Kotian, R.K.; Reddy, S.K.; Abhyankar, S.; Parveen, R.S. Physical Exhaustion Induced Variations in Event-Related Potentials and Cognitive Task Performance in Young Adults. Ann. Neurosci. 2018, 25, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Karageorghis, C.I.; Wang, C.C.; Chu, C.H.; Kao, S.C.; Hung, T.M.; Chang, Y.K. Effects of acute aerobic and resistance exercise on executive function: An ERP study. J. Sci. Med. Sport 2019, 22, 1367–1372. [Google Scholar] [CrossRef] [Green Version]
- Heathers, J.A. Everything Hertz: Methodological issues in short-term frequency-domain HRV. Front. Physiol. 2014, 5, 177–191. [Google Scholar] [CrossRef] [Green Version]
- Burr, R.L. Interpretation of normalized spectral heart rate variability indices in sleep research: A critical review. Sleep 2007, 30, 913–919. [Google Scholar] [CrossRef] [Green Version]
- Brennan, M.; Palaniswami, M.; Kamen, P. Do existing measures of Poincaré plot geometry reflect nonlinear features of heart rate variability? IEEE Trans. Biomed. Eng. 2001, 48, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Q.; Ji, L.L.; Fretwell, V.S.; Nunez, G. Effect of exercise on postprandial lipemia in men with hypertriglyceridemia. Eur. J. Appl. Physiol. 2006, 98, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Milz, P.; Faber, P.L.; Lehmann, D.; Koenig, T.; Kochi, K.; Pascual-Marqui, R.D. The functional significance of EEG microstates—Associations with modalities of thinking. Neuroimage 2016, 125, 643–656. [Google Scholar] [CrossRef]
- Azboy, O.; Kaygisiz, Z. Effects of sleep deprivation on cardiorespiratory functions of the runners and volleyball players during rest and exercise. Acta Physiol. Hung. 2009, 96, 29–36. [Google Scholar] [CrossRef]
- Cullen, T.; Thomas, G.; Wadley, A.J.; Myers, T. The effects of a single night of complete and partial sleep deprivation on physical and cognitive performance: A Bayesian analysis. J. Sports Sci. 2019, 37, 2726–2734. [Google Scholar] [CrossRef]
- Roberts, S.S.H.; Teo, W.P.; Aisbett, B.; Warmington, S.A. Extended Sleep Maintains Endurance Performance Better than Normal or Restricted Sleep. Med. Sci. Sports Exerc. 2019, 51, 2516–2523. [Google Scholar] [CrossRef]
- Oliver, S.J.; Costa, R.J.; Laing, S.J.; Bilzon, J.L.; Walsh, N.P. One night of sleep deprivation decreases treadmill endurance performance. Eur. J. Appl. Physiol. 2009, 107, 155–161. [Google Scholar] [CrossRef]
- Mejri, M.A.; Hammouda, O.; Zouaoui, K.; Chaouachi, A.; Chamari, K.; Rayana, M.C.B.; Souissi, N. Effect of two types of partial sleep deprivation on Taekwondo players’ performance during intermittent exercise. Biol. Rhythm. Res. 2013, 45, 17–26. [Google Scholar] [CrossRef]
- Papadakis, Z.; Forsse, J.S.; Stamatis, A. High-Intensity Interval Exercise Performance and Short-Term Metabolic Responses to Overnight-Fasted Acute-Partial Sleep Deprivation. Int. J. Environ. Res. Public Health 2021, 18, 3655. [Google Scholar] [CrossRef]
- Meier-Ewert, H.K.; Ridker, P.M.; Rifai, N.; Regan, M.M.; Price, N.J.; Dinges, D.F.; Mullington, J.M. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J. Am. Coll. Cardiol. 2004, 43, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Kato, M.; Phillips, B.G.; Sigurdsson, G.; Narkiewicz, K.; Pesek, C.A.; Somers, V.K. Effects of sleep deprivation on neural circulatory control. Hypertension 2000, 35, 1173–1175. [Google Scholar] [CrossRef] [Green Version]
- Sarma, S.; Levine, B.D. Beyond the Bruce Protocol: Advanced Exercise Testing for the Sports Cardiologist. Cardiol. Clin. 2016, 34, 603–608. [Google Scholar] [CrossRef]
- Tekieh, T.; Lockley, S.W.; Robinson, P.A.; McCloskey, S.; Zobaer, M.S.; Postnova, S. Modeling melanopsin-mediated effects of light on circadian phase, melatonin suppression, and subjective sleepiness. J. Pineal Res. 2020, 69, e12681. [Google Scholar] [CrossRef] [PubMed]
- Zobaer, M.S. Physiology-Based Modeling of Sleep and Wake Phenomena in the Human Brain. Ph.D. Thesis, The University of Sydney, Sydney, Australia, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Parameters | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Level 6 | Level 7 |
|---|---|---|---|---|---|---|---|
| Speed (km/h) | 2.7 | 4.0 | 5.4 | 6.7 | 8.0 | 8.8 | 9.6 |
| Slope (%) | 10 | 12 | 14 | 16 | 18 | 20 | 22 |
| Duration (min) | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Body Condition | Results |
|---|---|
| Age (years) | 20.74 ± 3.68 |
| Gender | Male |
| Height (cm) | 178.50 ± 5.03 |
| BMI (kg/m2) | 21.88 ± 2.02 |
| Weight (kg) | 70.05 ± 7.14 |
| Basal metabolism/d (kcal) | 1759.00 ± 160.02 |
| Resting heart rate (bpm) | 65.73 ± 10.43 |
| Resting SBP (mmHg) | 119.60 ± 14.74 |
| Resting DBP (mmHg) | 65.15 ± 10.00 |
| VO2 max (mL/kg/min) | 52.79 ± 18.49 |
| Condition | Sleep Duration (h) | Condition of Exercise Termination | Exercise Duration (min) | ||||
|---|---|---|---|---|---|---|---|
| Difficulty Breathing | SBP (Number of >150 mmHg) | DBP (Number of >75 mmHg) | HRmax (Number of >180 bpm) | RPE > 18 | |||
| Control | 7.63 ± 0.52 | all | 155.47 ± 17.56 (21) | 75.95 ± 13.71 (24) | 180.25 ± 5.36 (all) | all | 17.15 ± 1.15 |
| SD | 3.78 ± 0.69 *** | all | 157.78 ± 24.54 (25) | 86.28 ± 24.62 (26) | 188.78 ± 6.12 (all) * | all | 16.55 ± 1.07 * |
| Index | Pre- | Post- | ||
|---|---|---|---|---|
| Control | SD | Control | SD | |
| SDNN (ms) | 39.82 ± 12.40 | 36.43 ± 6.71 | 13.42 ± 7.29 | 9.76 ± 4.13 * |
| RMSSD (ms) | 47.28 ± 11.93 | 38.49 ± 13.93 * | 9.86 ± 5.34 | 7.44 ± 3.65 ** |
| pNN50 (%) | 24.61 ± 6.20 | 21.78 ± 5.85 * | 2.68 ± 1.71 | 0.25 ± 0.23 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Liang, A.; Song, J.; Zhang, Y.; Niu, X.; Xiao, T.; Chi, A. Effects of Acute-Partial Sleep Deprivation on High-Intensity Exercise Performance and Cardiac Autonomic Activity in Healthy Adolescents. Sustainability 2021, 13, 8769. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168769
Zhang Y, Liang A, Song J, Zhang Y, Niu X, Xiao T, Chi A. Effects of Acute-Partial Sleep Deprivation on High-Intensity Exercise Performance and Cardiac Autonomic Activity in Healthy Adolescents. Sustainability. 2021; 13(16):8769. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168769
Chicago/Turabian StyleZhang, Yue, Andi Liang, Jing Song, Yan Zhang, Xiaodan Niu, Tao Xiao, and Aiping Chi. 2021. "Effects of Acute-Partial Sleep Deprivation on High-Intensity Exercise Performance and Cardiac Autonomic Activity in Healthy Adolescents" Sustainability 13, no. 16: 8769. https://0-doi-org.brum.beds.ac.uk/10.3390/su13168769