Understanding the Spatial-Related Abstraction of Public Health Impact Goals and Measures: Illustrated by the Example of the Austrian Action Plan on Women’s Health


Abstract
:1. Introduction
1.1. AAPWH in Brief
1.2. The Leading Role of Public Health and the Inclusion of the Author in the Circle of Public Health Experts
- The spatial-related reasons for health inequality (of women) and how they influence the future quality of ageing and being old in different spatial contexts or rather spatial archetypes, as well as to the negative consequences of an ongoing spatial polarization in structurally strong and structurally weak regions and
- Presenting spatial planning approaches to create equivalent living conditions.
2. The Purpose of the Paper
- The opportunities for and limitations of raising the awareness of public health experts about the relevance of the spatial dimension in defining impact goals and measures.
- The factors that determine the degree of spatial abstraction of target group-specific impact goals and measures.
- The frontiers of knowledge implementation in strategic policy papers.
- Recommendations for spatial planning scholars who are interested in, or rather already engaged in, inter-sectoral collaboration and issues of public health.
3. The Space–Health Nexus and the Relevance of Spatial Planning
4. The Expert Group on “Women in Old Age”
5. Materials and Methods
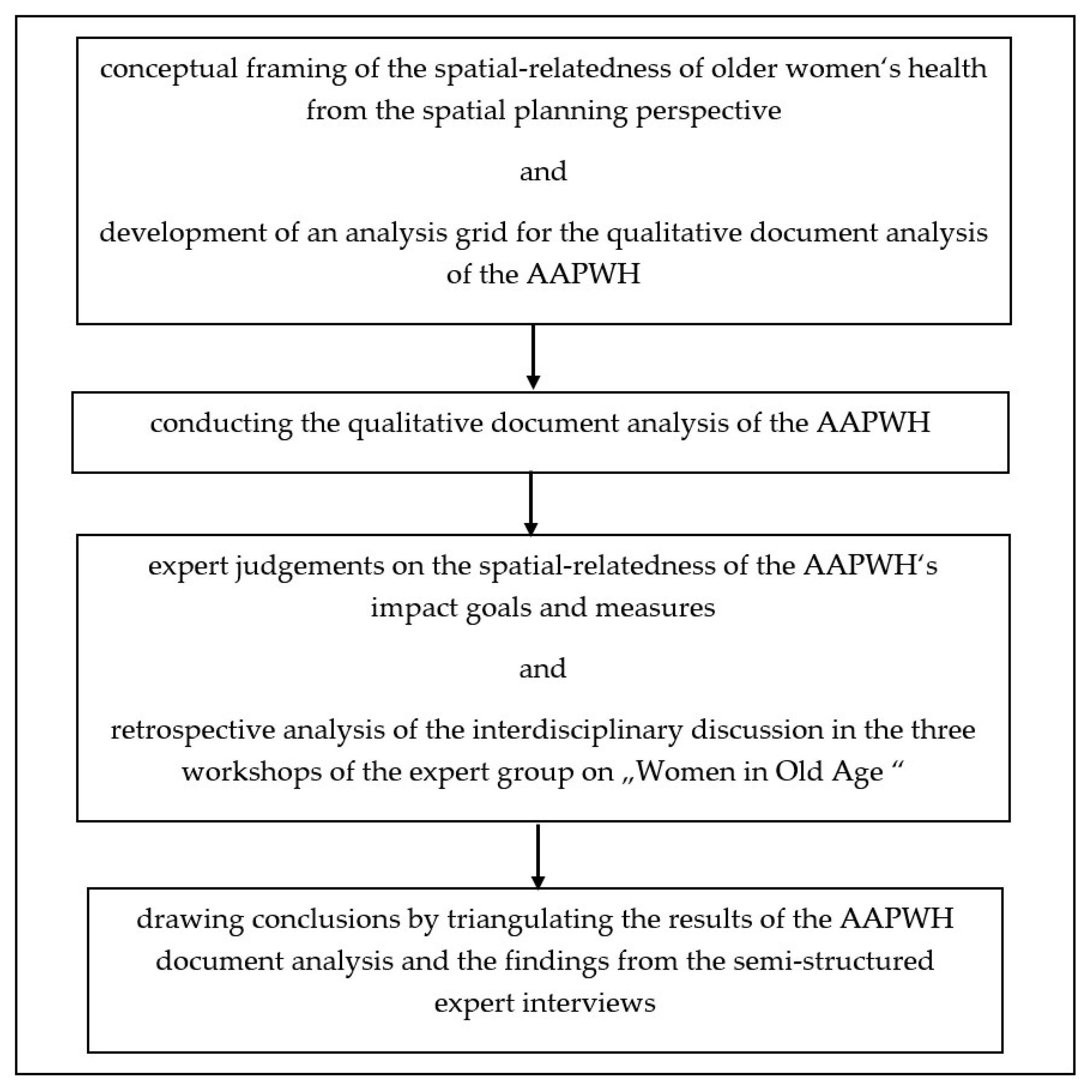
5.1. Research Design
5.2. Procedure
5.2.1. Development of an Analysis Grid for the Document Analysis of the AAPWH
- The challenges of organizing and coping with everyday life, including the accessibility of infrastructure and the social inclusion of physically impaired, or rather mobility-reduced, older people, taking into account topography (alpine rural areas), settlement structures, population density, infrastructural supply structures, (limited) freedom of choice related to goods and services and changes in family and other social networks, as well as considering the differences between urban and rural places of residence [22,35,43]
- The relevance of the region as the appropriate spatial reference of action with regard to the allocation of cost-intensive social infrastructures and the importance of regional centers or so-called central places as a result of the financially limited opportunities for action of low-income and/or ageing municipalities [12,44]
- Taking into account the stakeholder group of long-distance caregivers. This group is considered to be of great importance in quantitative terms in Austria [45] due to the ongoing polarization into prosperous and unfavorable regions on the one hand and thus, regions with continuing population loss and growing urban centers on the other hand.
5.2.2. Document Analysis of the AAPWH
- In the first screening, the spatial references were checked. For this purpose, the text was searched for the following terms: “city/urban/urban space”, “land/rural/rural space”; “local/communal”; “region/regional”; “municipality/district/province”; “public space/social space”.
- In the second screening, the causalities between the state of health (or rather disadvantages and health inequalities) of women in old age and their housing and living environments were checked. To this end, all text paragraphs marked in the first screening as well as all impact goals and measures relevant to the target group on “Women in Old Age” were checked.
- In the third screening, interlinkages between the results of the first and the second screening were searched for. Moreover, the impact goals and measures were analyzed with a view to spatial-related differentiations of the theme-related recommendations for action.
- In the fourth screening, the AAPWH was checked for paragraphs which relate to a call for a more interdisciplinary (scientific) debate on the determinants of women’s health. For this, the search terms “interdisciplinary” and “interdisciplinarity” were chosen.
5.2.3. Expert Judgements
Aim of Expert Survey and Design of Questionnaire
Sampling and Data Collection
Data Extraction
6. Results
6.1. Findings from the Document Analysis
- Spatial-related challenges in organizing and coping with everyday life
- The region as spatial reference of action as an appropriate spatial reference level for infrastructure measures
- The subject of “long-distance caregiving”. Nonetheless, this issue is addressed by Impact Goal 15 “Creating framework conditions that enable the currently mainly female caregivers to maintain their own health, self-determination and dignity” [15] (p. 74), specified by short-term “Measure 36 Sensitizing companies to the situation of caregiving relatives and establishing counselling services” [15] (p. 77).
- The mention of spatial planning as a crucial discipline in the discussion of (older) women’s well-being and health. Nevertheless, the need for more interdisciplinarity was put in writing. This is shown by medium-term “Measure 31 Strengthening interdisciplinary research on health issues specific to women in the third and fourth phases of life” [15] (p. 72), which is related to Impact Goal 14 “Ensuring gender-appropriate, individualized medical, psychosocial and nursing care up to old age, regardless of setting” [15] (p. 71).
6.2. Findings from the Expert Interviews
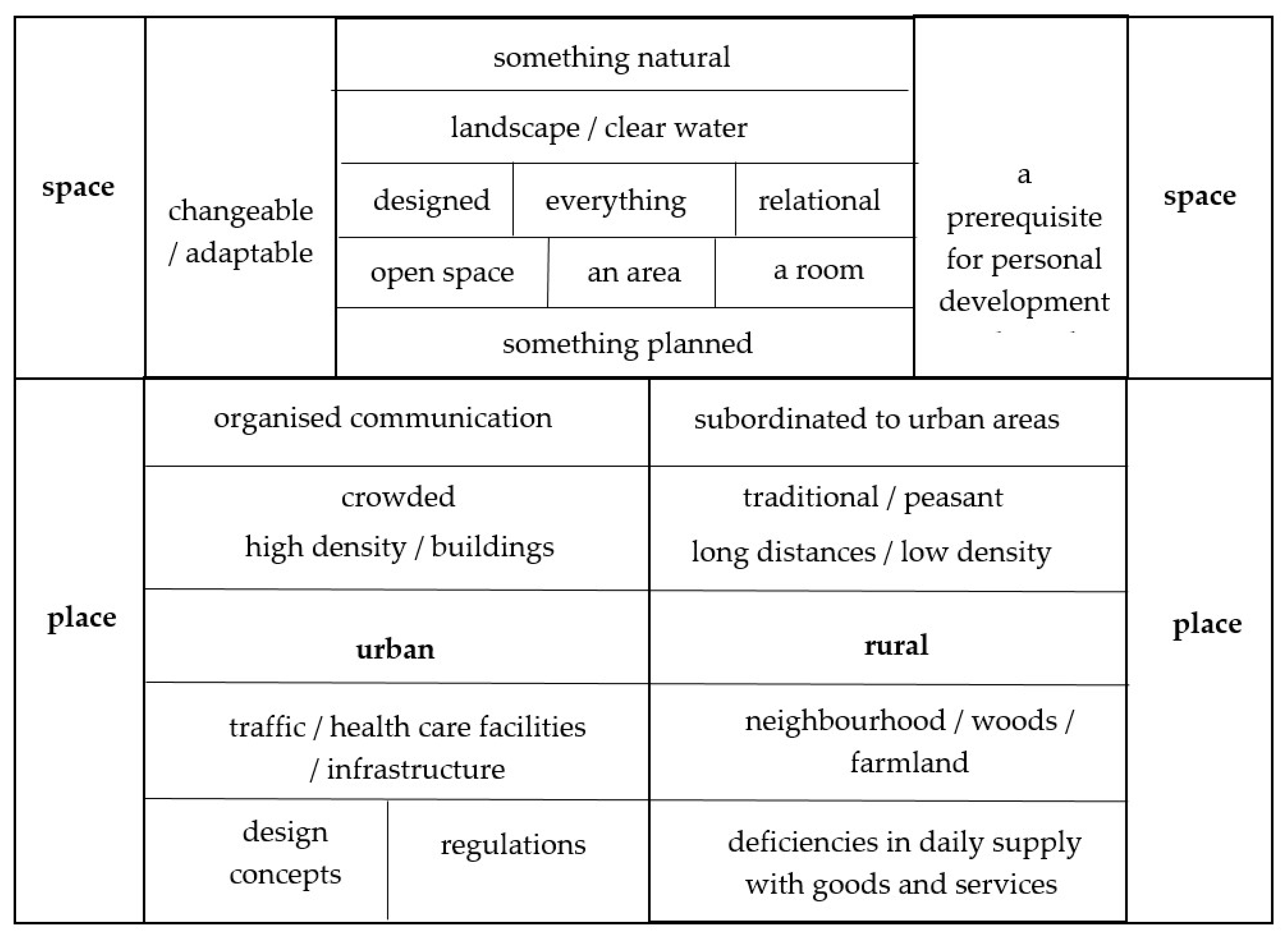
6.2.1. The Meaning of Space and Place for the Health of Older Women and the Urban–Rural Mindset
- The basic importance of unspoiled nature and appropriate sanitary conditions
- Space as a basic prerequisite for personal development
- The importance of opportunities for social participation. Therefore, space is “a sphere where people are living together” (I 6).
6.2.2. Perceived Spatial-Related Challenges for Maintaining and Improving Quality of Life and Health of Women in Old Age in Urban and Rural Areas and the Tendency of Marginalization of Women Living in Rural Areas
6.2.3. The Significance of Spatial Planning for Public Health and the Merit of Integrating Spatial and Planning Sciences Scholars in the Debate on Older Women’s Health
- … is “a political issue” (I 2), which nevertheless “is not yet on the radar.” (I 1, I 5)
- … is “a societal means of power” (I 1), which organizes human coexistence.
- … is addressed to all and “being done by all” (I 3).
- … is about “allocating spatial resources taking into account the needs of the population as well as of different target groups” (I 4).
- … “must ensure that offers are maintained right down to the last corner” (I 7).
- …is an important task in which “a great deal is about social responsibility” (I 2).
6.2.4. Explanations for the Degree of Spatial-Related Abstraction of the Impact Goals and Measures and Its Determining Factors
- “There is hardly any understanding of how individual life is related to spatial conditions.” (I 6)
- “If it served the economy, this issue would carry more weight.” (I 1)
6.2.5. Recommendations for Spatial Planning Scholars
7. Discussion
7.1. Methodological Strengths, Challenges and Limitations
7.2. Considerations on the Validity of the Questionnaire and Reliability of the Findings from the Expert Survey
7.3. The Merit of the Interdisciplinary Discussion within the Expert Group on “Women in Old Age” Including the Spatial Planning Perspective
7.3.1. Identifying Health-Relevant Spatial Aspects and Dealing with Spatial-Relatedness of (Older) Women’s Health: Similarities of and Differences between the Two Professions
7.3.2. Explanations for the Level of Spatial-Related Abstraction in the Impact Goals and Measures of the AAPWH
7.4. Some Considerations on the Fit of Findings into an International Perspective
8. Conclusions and Outlook
- Describe complex and abstract issues in a low-threshold manner, depicting them visually and, for this purpose, explain the space–health nexus for example by means of storytelling, in order to convey the key messages appropriately [26].
- Discuss the impact goals and measures of the AAPWH in the light of the sound empirical evidence of spatial planning research together with public health experts, in order to bring these findings closer to policy makers [28].
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nour, N.M. Global women’s health—A global perspective. Scand. J. Clin. Lab. Investig. Suppl. 2014, 244, 8–12; discussion 11–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.A.E.; Woodward, M.; Jha, V.; Kennedy, S.; Norton, R. Women’s health: A new global agenda. BMJ Glob. Health 2016, 1, e000080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manandhar, M.; Hawkes, S.; Buse, K.; Nosrati, E.; Magar, V. Gender, health and the 2030 agenda for sustainable development. Bull. World Health Organ. 2018, 96, 644–653. [Google Scholar] [CrossRef]
- Rudolph, L.; Caplan, J.; Ben-Moshe, K.; Dillon, L. Health in All Policies: A Guide for State and Local Governments; American Public Health Association and Public Health Institute: Washington, DC, USA; Oakland, CA, USA, 2013. [Google Scholar]
- World Bank, W. Atlas of Sustainable Development Goals 2018. From World Development Indicators; World Bank Publications: Washington, DC, USA, 2018; ISBN 978-1-4648-1250-7. [Google Scholar]
- Rásky, É. Women’s Health Network: State of Affairs, Concepts, Approaches, Organizations in the Women’s Health Movement. Country Report Austria. Available online: https://www.gesundheit-nds.de/ewhnet/Country%20Reports/AustriaE.PDF (accessed on 1 October 2020).
- Habimana, K.; Bachner, F.; Bobek, J.; Ladurner, J.; Ostermann, H. Das Österreichische Gesundheitswesen im Internationalen Vergleich. Wissenschaftlicher Ergebnisbericht.: Im Auftrag des Bundesministeriums für Gesundheit. Available online: https://www.sozialministerium.at/dam/jcr:32d88746-dd2b-4e38-bd6b-a7622200da71/das_oesterreichische_gesundheitswesen_im_internationalen_vergleich.pdf (accessed on 1 October 2020).
- Barber, R.M.; Fullman, N.; Sorensen, R.J.D.; Bollyky, T.; McKee, M.; Nolte, E.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; et al. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the Global Burden of Disease Study 2015. Lancet 2017, 390, 231–266. [Google Scholar] [CrossRef] [Green Version]
- OECD. Health at a Glance 2017: OECD Indicators. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/social-issues-migration-health/health-at-a-glance-2017_health_glance-2017-en (accessed on 1 October 2020).
- World Health Organization. World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals. Available online: https://www.who.int/data/gho/publications/world-health-statistics (accessed on 1 October 2020).
- Simon, G.; Benischke, C. FRAUEN (60+) IN ÖSTERREICH. FAKTEN, FRAGEN, FORSCHUNGSLÜCKEN: GRUNDLAGEN ZUM EMPOWERMENT. Available online: https://www.sozialministerium.at/dam/jcr:a37b8996-5183-4e8e-af82-9712926ccef2/Frauen%2060+.%202019.pdf (accessed on 1 October 2020).
- Fischer, T. Versorgung mit sozialer Infrastruktur. In Stöglehner, Gernot (Hrsg.): Grundlagen der Raumplanung 2. Strategien, Themen, Konzepte.; Facultas: Wien, Austria, 2020; pp. 235–267. ISBN 978-3-7089-1755-9. [Google Scholar]
- Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz. Demographischer Wandel—Geänderte Rahmenbedingungen für den Sozialstaat? Available online: https://www.sozialministerium.at/dam/jcr:6375bc0a-d6a7-4c93-879e-b2e7acb13668/dokument_demographischer_wandel_22_11_2019_barrierefrei.pdf (accessed on 1 October 2020).
- Mayrhuber, C. Erwerbsunterbrechungen, Teilzeitarbeit und ihre Bedeutung für das FrauenLebenseinkommen. Available online: http://www.forschungsnetzwerk.at/downloadpub/Studie_Lebenseinkommen%202017_end.pdf (accessed on 1 October 2020).
- Bundesministerium für Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz. In Aktionsplan Frauengesundheit. 40 Maßnahmen für Die Gesundheit von Frauen in Österreich; Sozialministerium: Wien, Auatria, 2018.
- Austrian Presidency of the Council of the European Union, Federal Chancellery of Austria, Federal Minister for Women, Families and Youth, Division III—Women and Equality. Gender Equality in Austria. Milestones, Successes and Challenges. Available online: https://www.frauen-familien-jugend.bka.gv.at/dam/jcr:67b5975f-358e-474e-9b3c-5c81b3167fca/Gleichstellung_Broschuere_Ratsvorsitz_EN_RZ16.pdf (accessed on 5 January 2021).
- World Health Organization (WHO). Regional Office for Europe. Health 2020. A European Policy Framework and Strategy for the 21st Century. Available online: https://www.euro.who.int/en/publications/abstracts/health-2020.-a-european-policy-framework-and-strategy-for-the-21st-century-2013 (accessed on 1 October 2020).
- Buzeti, T.; Madureira Lima, J.; Yang, L.; Brown, C. Leaving no one behind: Health equity as a catalyst for the sustainable development goals. Eur. J. Public Health 2020, 30, i24–i27. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Regional Office for Europe. Intersectoral Action between Health, Social Protection and Labour Market Policy. Available online: https://www.euro.who.int/__data/assets/pdf_file/0017/413018/Intersectoral-action-between-health,-social-protection-and-labour-market-policy.pdf (accessed on 1 October 2020).
- Federal Ministry of Social Affairs, Health, Care and Consumer Protection. Available online: https://broschuerenservice.sozialministerium.at/Home/Download?publicationId=480 (accessed on 13 January 2021).
- Baumgart, S. Räumliche Planung und öffentliche Gesundheit—eine historische Verknüpfung. In Planung für Gesundheitsfördernde Städte. Forschungsberichte der ARL 08; Baumgart, S., Köckler, H., Ritzinger, A., Rüdiger, A., Eds.; ARL: Hannover, Germany, 2018; pp. 20–36. ISBN 978-3-88838-085-3. Available online: https://webcache.googleusercontent.com/search?q=cache:BjWo1P517gIJ:https://shop.arl-net.de/planung-fuer-gesundheitsfoerdernde-staedte.html+&cd=2&hl=de&ct=clnk&gl=at&client=firefox-b-d (accessed on 13 January 2021).
- Fischer, T.; Stöglehner, G. Gesundheitsbezogene Lebensqualität im Alter als Thema der Raumplanung. Zusammenhänge und Handlungsoptionen. In Gesundheitliche Lebensqualität im Alter. Ein Interdisziplinäres Handbuch für Health Professionals; Kolland, F., Dorner, T.E., Eds.; MANZ Verlag: Wien, Austria, 2020; pp. 27–41. ISBN 978-3-214-13158-6. [Google Scholar]
- UN-HABITAT & World Health Organization. Integrating Health in Urban and Territorial Planning: A Sourcebook. Available online: https://apps.who.int/iris/handle/10665/331678 (accessed on 4 January 2021).
- Storm, I.; den Hertog, F.; van Oers, H.; Schuit, A.J. How to improve collaboration between the public health sector and other policy sectors to reduce health inequalities?—A study in sixteen municipalities in the Netherlands. Int. J. Equity Health 2016, 15, 97. [Google Scholar] [CrossRef] [Green Version]
- Barton, H.; Tsourou, C. Healthy Urban Planning. A WHO Guide to Planning for People; Published on Behalf of the World Health Organization Regional Office for Europe by Spon: London, UK, 2000; ISBN 0-415-24327-0. [Google Scholar]
- Sisnowski, J.; Street, J.M. Evidence-Informed Public Health Policy. In International Encyclopedia of Public Health; Elsevier: Amsterdam, The Netherlands, 2017; pp. 57–65. ISBN 9780128037089. [Google Scholar]
- Storm, I.; Aarts, M.-J.; Harting, J.; Schuit, A.J. Opportunities to reduce health inequalities by ‘Health in All Policies’ in the Netherlands: An explorative study on the national level. Health Policy 2011, 103, 130–140. [Google Scholar] [CrossRef]
- Ige-Elegbede, J.; Pilkington, P.; Bird, E.L.; Gray, S.; Mindell, J.S.; Chang, M.; Stimpson, A.; Gallagher, D.; Petrokofsky, C. Exploring the views of planners and public health practitioners on integrating health evidence into spatial planning in England: A mixed-methods study. J. Public Health 2020. [Google Scholar] [CrossRef]
- Baumgart, S.; Köckler, H.; Ritzinger, A.; Rüdiger, A. (Eds.) Planung für Gesundheitsfördernde Städte. Forschungsberichte der ARL 08; Hannover, Germany, 2018; ISBN 978-3-88838-085-3. Available online: https://webcache.googleusercontent.com/search?q=cache:BjWo1P517gIJ:https://shop.arl-net.de/planung-fuer-gesundheitsfoerdernde-staedte.html+&cd=2&hl=de&ct=clnk&gl=at&client=firefox-b-d (accessed on 13 January 2021).
- Phillips, J.; Walford, N.; Hockey, A.; Foreman, N.; Lewis, M. Older people and outdoor environments: Pedestrian anxieties and barriers in the use of familiar and unfamiliar spaces. Geoforum 2013, 47, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Mehrabi, F.; Béland, F. Effects of social isolation, loneliness and frailty on health outcomes and their possible mediators and moderators in community-dwelling older adults: A scoping review. Arch. Gerontol. Geriatr. 2020, 90, 104119. [Google Scholar] [CrossRef]
- Morrisby, C.; Joosten, A.; Ciccarelli, M. Do services meet the needs of people with dementia and carers living in the community? A scoping review of the international literature. Int. Psychogeriatr. 2018, 30, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Harper, S. The Convergence of Population Ageing with Climate Change. Popul. Ageing 2019, 12, 401–403. [Google Scholar] [CrossRef] [Green Version]
- Haq, G.; Whitelegg, J.; Kohler, M. Growing Old in a Changing Climate: Meeting the Challenges of an Ageing Population and Climate Change; Stockholm Environment Institute: Stockholm, Sweden, 2008. [Google Scholar] [CrossRef]
- Fischer, T. Aging in rural areas in Austria—On the interrelations of spatial aspects and the quality of life of today’s older generation. Eur. Countrys. 2009, 1. [Google Scholar] [CrossRef] [Green Version]
- Rechel, B.; Džakula, A.; Duran, A.; Fattore, G.; Edwards, N.; Grignon, M.; Haas, M.; Habicht, T.; Marchildon, G.P.; Moreno, A.; et al. Hospitals in rural or remote areas: An exploratory review of policies in 8 high-income countries. Health Policy 2016, 120, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Allen, P.; May, J.; Pegram, R.; Shires, L. ‘It’s mostly about the job’—Putting the lens on specialist rural retention. Rural Remote Health 2020, 20, 5299. [Google Scholar] [CrossRef] [PubMed]
- ARL—Akademie für Raumentwicklung in der Leibniz-Gemeinschaft. Raumordnung: Anwalt für Gleichwertige Lebensverhältnisse und Regionale Entwicklung—Eine Positionsbestimmung. = Positionspapier aus der ARL 115. Available online: https://www.arl-net.de/de/blog/raumordnung-anwalt-f%C3%BCr-gleichwertige-lebensverh%C3%A4ltnisse-und-regionale-entwicklung-eine (accessed on 5 October 2020).
- Akademie für Raumforschung und Landesplanung. Daseinsvorsorge und Gleichwertige Lebensverhältnisse neu Denken—Perspektiven und Handlungsfelder. Hannover. = Positionspapier aus der ARL 108. Available online: https://shop.arl-net.de/daseinsvorsorg-und-gleichwertige-lebensverhaeltnisse-neu-denken.html (accessed on 5 October 2020).
- Austrian National Public Health Institute. Minute of Workshop No. 1 of the expert group "Women in Old Age" Title of document: Minute_28_04_2015.pdf, Document not available to the public.
- Austrian National Public Health Institute. Minute of Workshop No. 2 of the expert group "Women in Old Age". Title of document: Minute_26_05_2015.pdf, Document not available to the public.
- Hofmarcher, M.M.; Rack Herta, M. Gesundheitssysteme im Wandel: Österreich; WHO Regionalbüro für Europa im Auftrag des Europäischen Observatoriums für Gesundheitssysteme und Gesundheitspolitik: Kopenhagen, Denmark, 2006. [Google Scholar]
- Fischer, T. Raumrelevante Aspekte des Altseins und Älterwerdens im ländlichen Raum Österreichs und in der Metropolregion Wien. In Europäische Raumentwicklung: Metropolen und Periphere Regionen; Güldenberg, E., Ed.; Lang: Frankfurt am Main, Germany, 2009; pp. 93–108. ISBN 3631588771. [Google Scholar]
- Fischer, T. Räumliche Disparitäten und gleichwertige Lebensverhältnisse. In Stöglehner, Gernot (Hrsg.): Grundlagen der Raumplanung 2. Strategien, Themen, Konzepte.; Facultas: Wien, Austria, 2020; pp. 303–324. ISBN 978-3-7089-1755-9. [Google Scholar]
- Fischer, T.; Jobst, M. Capturing the Spatial Relatedness of Long-Distance Caregiving: A Mixed-Methods Approach. Int. J. Environ. Res. Public Health 2020, 17, 6406. [Google Scholar] [CrossRef] [PubMed]
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development, 1st ed.; Sage Publications: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Fischer, T. Zur Verankerung raum-und planungswissenschaftlicher Anliegen im Aktionsplan Frauengesundheit—Ein Erfahrungsbericht [Poster]. In Forum Geriatrie und Gerontologie Bad Hofgastein. Altern Multiprofessionell: Praxis und Forschung, 8.–10.; Kongresszentrum Bad Hofgastein: Bad Hofgastein, Österreich, 2018. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. Grounded Theory. Strategien Qualitativer Forschung, 1st ed.; Huber: Bern, Switzerland, 1998. [Google Scholar]
- Wiles, J. Conceptualizing place in the care of older people: The contributions of geographical gerontology. J. Clin. Nurs. 2005, 14, 100–108. [Google Scholar] [CrossRef]
- Harris, P.; Kent, J.; Sainsbury, P.; Thow, A.M. Framing health for land-use planning legislation: A qualitative descriptive content analysis. Soc. Sci. Med. 2016, 148, 42–51. [Google Scholar] [CrossRef]
- Hult, M.; Lennung, S.-Å. Towards a definition of action research: A note and bibliography. J. Manag. Stud. 1980, 17, 241–250. [Google Scholar] [CrossRef]
- Walt, G.; Shiffman, J.; Schneider, H.; Murray, S.F.; Brugha, R.; Gilson, L. ‘Doing’ health policy analysis: Methodological and conceptual reflections and challenges. Health Policy Plan. 2008, 23, 308–317. [Google Scholar] [CrossRef] [Green Version]
- Huber, A. Die Angst des Wissenschaftlers vor der Ästhetik. Forum Qual. Soz. 2001. [Google Scholar] [CrossRef]
- Schmitt, P.; Wiechmann, T. Unpacking Spatial Planning as the Governance of Place. Disp. Plan. Rev. 2018, 54, 21–33. [Google Scholar] [CrossRef] [Green Version]
- Freedman, D.A.; Bess, K.D.; Tucker, H.A.; Boyd, D.L.; Tuchman, A.M.; Wallston, K.A. Public health literacy defined. Am. J. Prev. Med. 2009, 36, 446–451. [Google Scholar] [CrossRef]
- Danielzyk, R.; Dittrich-Wesbuer, A.; Hilti, N.; Tippel, C. (Eds.) Multilokale Lebensführungen und Räumliche Entwicklungen—Ein Kompendium; Print-on-Demand; ARL—Akademie für Raumentwicklung in der Leibniz-Gemeinschaft: Hannover, Austria, 2020; ISBN 978-3-88838-098-3. [Google Scholar]
- Levy, C. Gender and the environment: The challenge of cross-cutting issues in development policy and planning. Environ. Urban. 1992, 4, 134–149. [Google Scholar] [CrossRef]
- Mirzoev, T.N.; Green, A.T. Planning, for Public Health Policy. In International Encyclopedia of Public Health; Elsevier: Amsterdam, The Netherlands, 2017; pp. 489–499. ISBN 9780128037089. [Google Scholar]
- Peters, D.T.J.M.; Raab, J.; Grêaux, K.M.; Stronks, K.; Harting, J. Structural integration and performance of inter-sectoral public health-related policy networks: An analysis across policy phases. Health Policy 2017, 121, 1296–1302. [Google Scholar] [CrossRef]
- McKinnon, G.; Pineo, H.; Chang, M.; Taylor-Green, L.; Strategy, A.J.; Toms, R. Strengthening the links between planning and health in England. BMJ 2020, 369, m795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, Q.H.; Napier, N.K. Acculturation and global mindsponge: An emerging market perspective. Int. J. Intercult. Relat. 2015, 49, 354–367. [Google Scholar] [CrossRef]
- Albrechts, L. Strategic (Spatial) Planning Reexamined. Environ. Plan B Plan Des. 2004, 31, 743–758. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, P.; Hewitt, S.; Blackshaw, N. Joining up health and planning: How Joint Strategic Needs Assessment (JSNA) can inform health and wellbeing strategies and spatial planning. Perspect. Public Health 2013, 133, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, A.-M.; Habraken, J.; Jansen, M.W.J.; Gubbels, J.S.; de Vries, N.K.; van Oers, H.; Michie, S.; Atkins, L.; Kremers, S.P.J. ‘Are we there yet?’—Operationalizing the concept of Integrated Public Health Policies. Health Policy 2014, 114, 174–182. [Google Scholar] [CrossRef]
- Lowe, M.; Whitzman, C.; Giles-Corti, B. Health-Promoting Spatial Planning: Approaches for Strengthening Urban Policy Integration. Plan. Theory Pract. 2018, 19, 180–197. [Google Scholar] [CrossRef]
- Fischer, T.; Jobst, M. On the Suitability and Potential of Nursing Care Discussion Forums as a Health Promotion Measure for Long-Distance Caregiving Relatives: Evidence from Upper Austria. Healthcare 2019, 7, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, G. Intertextuality, 2nd ed.; Routledge: London, UK, 2011; ISBN 9780203829455. [Google Scholar]
- Clark, H.; Taplin, D. Theory of Change Basics: A Primer on Theory of Change. Available online: https://www.theoryofchange.org/wp-content/uploads/toco_library/pdf/ToCBasics.pdf (accessed on 15 October 2020).
- Smith, M.K.; Argyris, C. Chris Argyris: Theories of Action, Double-Loop Learning and Organizational Learning. The Encyclopedia of Informal Education. Available online: www.infed.org/thinkers/argyris.htm (accessed on 15 October 2020).



{kind=link}
{kind=link}
| Number of Workshop | Date, Location and Duration | Agenda 1 | Working Methods |
|---|---|---|---|
| Workshop No. 1 | 28 April 2015, Federal Ministry of Social Affairs, Health and Consumer Protection, 10.00 a.m. to 5 p.m. | Presentation of the project “Austrian Action Plan on Women’s Health”, Keynote speech given by the expert group leader Stocktaking of initiatives, and projects: focus on “Women in Old Age” and Development of 3 to 4 key topics Impact goals for the prioritized key topics | PowerPoint-presentation in plenary working in small groups/World Café (guided by key questions, result documentation using flipcharts) plenary discussion |
| Workshop No. 2 | 26 May 2015, Austrian National Public Health Institute, 10.00 a.m. to 5 p.m. | Retrospection on the project activities and results so far Feedback on the impact goals from the organizations involved in the making of AAPWH Completion of impact goals Compilation of good practices, agreements, Laws, regulations, concepts related to the impact goals Description of measures related to the impact goals and collection of ideas for cross-age topics Suggestions for the AAPWH’s monitoring prioritization of measures | PowerPoint-presentation discussions in small groups and plenary discussion |
| Workshop No. 3 | 10 November 2015, Austrian National Public Health Institute, 10.00 a.m. to 5 p.m. | Discussion of the results of the online consultation and Project finalization 2 | PowerPoint-presentation and plenary discussion |
| Theme | Questions (Verbatim) |
|---|---|
| General questions on the three workshops of the expert group on “Women in old age” | Q 1: How did you experience the interdisciplinary debate on the topic of “women in old age and health”? What challenges—in your opinion—were associated with the comprehensibility of the argumentation of experts from other disciplines? |
| Interrelations between health and space | Q 2: What do you associate with the terms “space” and “place”?” Q 3: What do you associate with the term “urban”? Q 4: What do you associate with the term “rural”? Q 5: If you interlink the three terms “rural”, “older women” and “health”, what will come to your mind? Q 6: How do you define quality of life? Q 7: What spatial aspects do you associate with “good” or “bad” quality of life in old age? |
| Perception of spatial planning as a professional discipline and retrospection on the discussions during the workshops | Q 8: What do you associate with the term “spatial planning”? Q 9: Did you deal with “spatial planning” as a discipline before the workshops? Q 10: What competences or fields of expertise do you ascribe to spatial planning? Q 11: What, in your opinion, constitutes “good spatial planning”, and who do you think is responsible for that? Q 12: How did you experience the introduction of spatial planning arguments during the discussions in the workshops? Do you remember something special of it? If so, why and what? If not, why not? Q 13: Has “acquaintance with spatial planning” changed a) your perception of the discipline of spatial planning, b) your awareness of the relevance of spatial aspects to the quality of getting old (as a women), c) your way of thinking and reasoning? (Please explain.) Q 14: How do you deal with the fact that the target group-specific impact goals and measures are characterized by a high level of abstraction in spatial terms? |
| Outlook | Q 15: How, in your opinion, could it succeed in future to anchor spatial aspects more firmly in health and care-related policy papers as well as in public health recommendations for action? Q 16: May I ask you for your further thoughts. |
| Identifier of the Interview Partners | Gender | Educational Background/Place of Work | Interview Method/Date of Interview |
|---|---|---|---|
| Interviewee 1 | female | nursing and health care, humanities/ public health institution | live one-to-one interview, 19 January 2018 |
| Interviewee 2 | female | medical sciences/ health care facility | live one-to-one interview, 22 January 2018 |
| Interviewee 3 | female | nursing and health care/ professional association | live one-to-one interview, 23 January 2018 |
| Interviewee 4 | female | public health, nursing, social sciences/ interest group | live one-to-one interview, 30 January 2018 |
| Interviewee 5 | female | journalism and communication sciences/ interest group | phone interview, 27 February 2018 |
| Interviewee 6 | female | nursing and health care, humanities, public health/ blue-light organization | live one-to-one interview, 4 May 2018 |
| Interviewee 7 | female | natural sciences/ federal authority | live one-to-one interview, 4 May 2018 |
| Interviewee 8 1 | female | social work/ professional association | live one-to-one interview, 5 March 2018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischer, T. Understanding the Spatial-Related Abstraction of Public Health Impact Goals and Measures: Illustrated by the Example of the Austrian Action Plan on Women’s Health. Sustainability 2021, 13, 773. https://0-doi-org.brum.beds.ac.uk/10.3390/su13020773
Fischer T. Understanding the Spatial-Related Abstraction of Public Health Impact Goals and Measures: Illustrated by the Example of the Austrian Action Plan on Women’s Health. Sustainability. 2021; 13(2):773. https://0-doi-org.brum.beds.ac.uk/10.3390/su13020773
Chicago/Turabian StyleFischer, Tatjana. 2021. "Understanding the Spatial-Related Abstraction of Public Health Impact Goals and Measures: Illustrated by the Example of the Austrian Action Plan on Women’s Health" Sustainability 13, no. 2: 773. https://0-doi-org.brum.beds.ac.uk/10.3390/su13020773