
Do “Stay-at-Home Exercise” Videos Induce Behavioral Changes in College Students? A Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
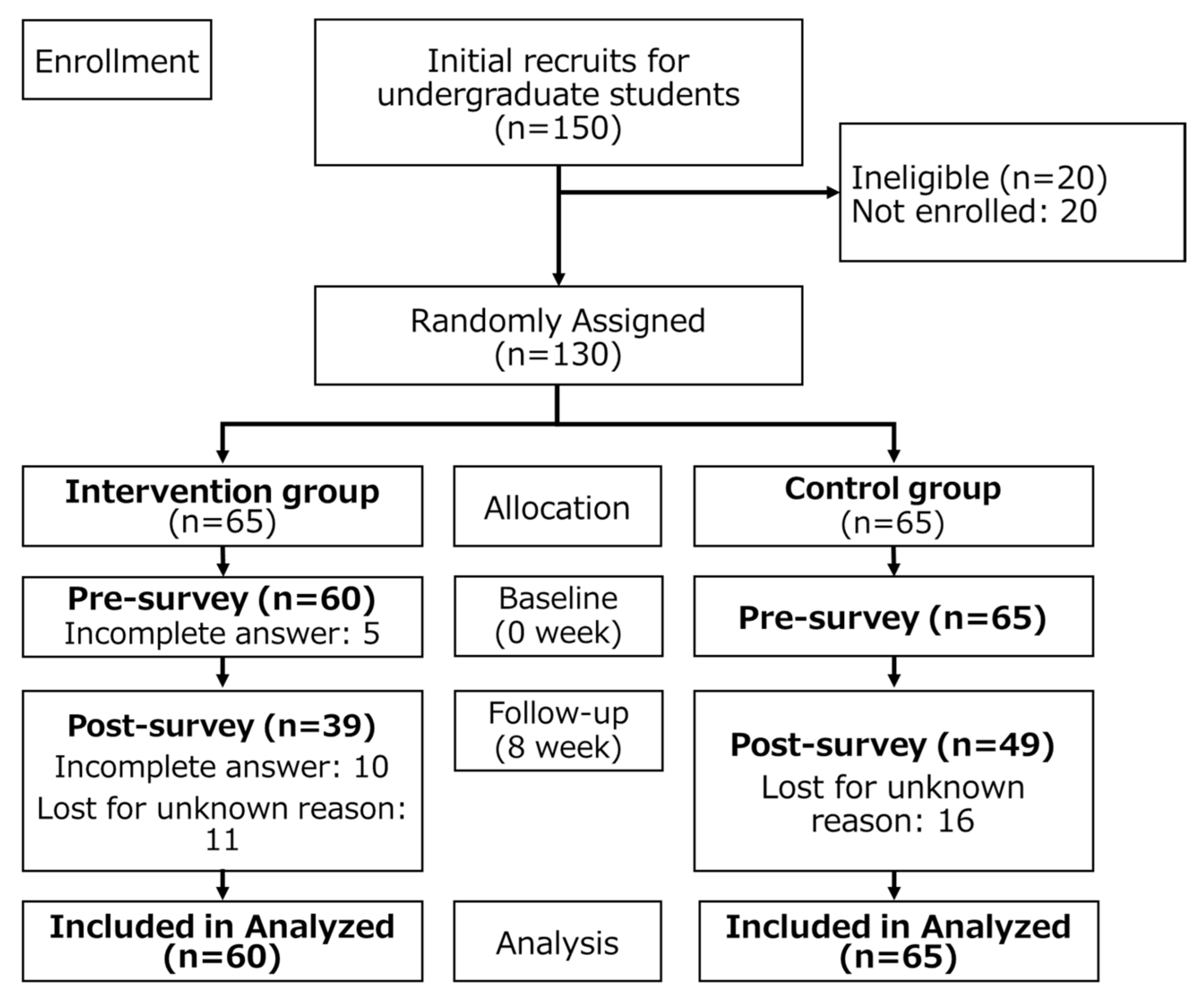
2.1. Participants and Study Design
2.2. Intervention
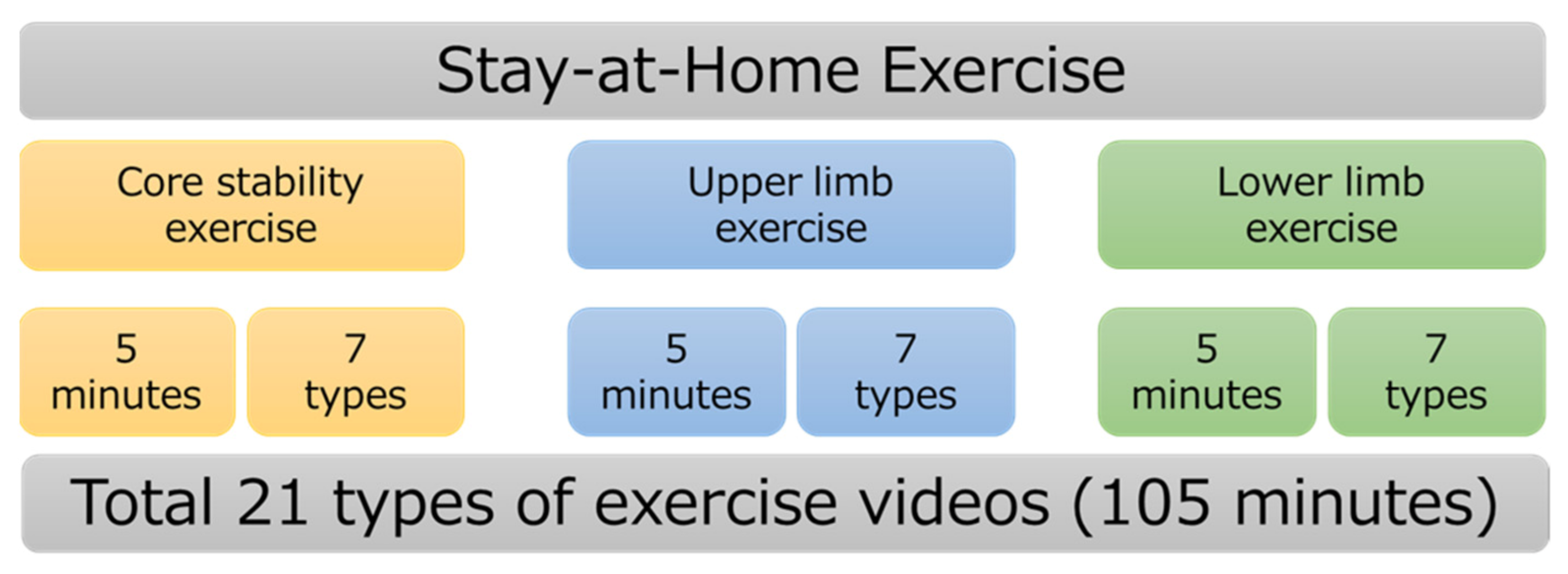
2.2.1. Intervention Group
2.2.2. Control Group
2.3. Outcome Measures of an Internet-Based Questionnaire
2.4. Demographic Characteristics
2.5. Primary Outcome: PA
2.6. Secondary Outcomes: HRQoL, SWB, and Psychological Distress
2.7. Statistical Analyses
3. Results
3.1. Participants
3.2. PA, HRQoL, SWB, and Psychological Distress at Baseline and Follow-Up
4. Discussion
4.1. Relationship between Video Streaming and Physical Activity
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Wegner, M.; Amatriain-Fernández, S.; Kaulitzky, A.; Murillo-Rodriguez, E.; Machado, S.; Budde, H. Systematic Review of Meta-Analyses: Exercise Effects on Depression in Children and Adolescents. Front. Psychiatry 2020, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: https://www.who.int/healthinfo/global_burden_disease/estimates/en/ (accessed on 22 June 2021).
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S.; Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2019, 4, 23–35. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. National Institute of Health and Nutrition. Japanese Official Physical Activity Guidelines for Health Promotion—ActiveGuide—2013. Available online: https://www.nibiohn.go.jp/eiken/english/research/pdf/active_guide2013.pdf (accessed on 23 May 2021).
- Andersen, L.B.; Mota, J.; Di Pietro, L. Update on the global pandemic of physical inactivity. Lancet 2016, 388, 1255–1256. [Google Scholar] [CrossRef]
- Yunusova, A.; Lai, J.; Rivera, A.P.; Hu, S.; Labbaf, S.; Rahmani, A.M.; Dutt, N.; Jain, R.C.; Borelli, J.L. Assessing the Mental Health of Emerging Adults Through a Mental Health App: Protocol for a Prospective Pilot Study. JMIR Res. Protoc. 2021, 10, e25775. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical Activity Changes and Its Risk Factors among Community-Dwelling Japanese Older Adults during the COVID-19 Epidemic: Associations with Subjective Well-Being and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Maeda, N.; Urabe, Y.; Suzuki, Y.; Hirado, D.; Morikawa, M.; Komiya, M.; Mizuta, R.; Naito, K.; Shirakawa, T. Cross-Sectional Study of the Prevalence and Symptoms of Urinary Incontinence among Japanese Older Adults: Associations with Physical Activity, Health-Related Quality of Life, and Well-Being. Int. J. Environ. Res. Public Health 2021, 18, 360. [Google Scholar] [CrossRef]
- Kaneda, K.; Maeda, N.; Suzuki, Y.; Fukui, K.; Urabe, Y. Impact of the COVID-19 Pandemic on Life Space Extent and Apathy: A Comparison of Competitive Japanese Swimmers with and without Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 5106. [Google Scholar] [CrossRef]
- Government of Japan. Basic Policies for Novel Coronavirus Disease Control by the Government of Japan (Summary). Available online: https://www.mhlw.go.jp/content/10900000/000634753.pdf (accessed on 18 June 2021).
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.D.C.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Japan Sports Agency. 2021. 04. Sport in Life. Available online: https://sportinlife.go.jp/news/20210428_1.html (accessed on 22 June 2021).
- Sebire, K. The Coronavirus Lockdown is Forcing Us to View “Screen Time” Differently. That’s a Good Thing. The Conversation. Available online: https://theconversation.com/the-coronavirus-lockdown-is-forcing-us-to-view-screen-time-differentlythats-a-good-thing-135641 (accessed on 22 June 2021).
- Amatriain-Fernández, S.; Murillo-Rodríguez, E.S.; Gronwald, T.; Machado, S.; Budde, H. Benefits of physical activity and physical exercise in the time of pandemic. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S264–S266. [Google Scholar] [CrossRef]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Can Smartphone Apps Increase Physical Activity? Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef]
- Stockwell, S.; Schofield, P.; Fisher, A.; Firth, J.; Jackson, S.; Stubbs, B.; Smith, L. Digital behavior change interventions to promote physical activity and/or reduce sedentary behavior in older adults: A systematic review and meta-analysis. Exp. Gerontol. 2019, 120, 68–87. [Google Scholar] [CrossRef]
- Baranowski, T. Exergaming: Hope for future physical activity? or blight on mankind? J. Sport Health. Sci. 2017, 6, 44–46. [Google Scholar] [CrossRef]
- Parker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The Use of Digital Platforms for Adults’ and Adolescents’ Physical Activity During the COVID-19 Pandemic (Our Life at Home): Survey Study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef]
- G*Power 3.1. Available online: http://www.gpower.hhu.de/en.html (accessed on 13 January 2021).
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Kosinski, M.; Dewey, J.E.; Gandek, B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8 Health Survey; QualityMetric Incorporated: Lincoln, NE, USA, 2001. [Google Scholar]
- Fukuhara, S.; Suzukamo, Y. Manual of the SF-8 Japanese Version; Institute for Health Outcomes and Process Evaluation Research: Kyoto, Japan, 2004. [Google Scholar]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Fukui, T. Assessing items on the SF-8 Japanese version for health-related quality of life: A psychometric analysis based on the nominal categories model of item response theory. Value Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Lucas-Carrasco, R.; Allerup, P.; Bech, P. The Validity of the WHO-5 as an Early Screening for Apathy in an Elderly Population. Curr. Gerontol. Geriatr. Res. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Haapasalo, V.; de Vries, H.; Vandelanotte, C.; Rosenkranz, R.R.; Duncan, M.J. Cross-sectional associations between multiple lifestyle behaviours and excellent well-being in Australian adults. Prev. Med. 2018, 116, 119–125. [Google Scholar] [CrossRef]
- Molenberghs, G.; Verbeke, G. A review on linear mixed models for longitudinal data, possibly subject to dropout. Stat. Model. 2001, 1, 235–269. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; del Pozo Cruz, B.; Green, M.A.; Bauman, A.E. Is the COVID-19 lockdown nudging people to be more active: A big data analysis. Br. J. Sports Med. 2020, 54, 1183–1184. [Google Scholar] [CrossRef]
- Alley, S.; Jennings, C.; Plotnikoff, R.C.; Vandelanotte, C. Web-Based Video-Coaching to Assist an Automated Computer-Tailored Physical Activity Intervention for Inactive Adults: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e223. [Google Scholar] [CrossRef] [Green Version]
- Vandelanotte, C.; Duncan, M.J.; Maher, C.A.; Schoeppe, S.; Rebar, A.L.; Power, D.A.; Short, C.E.; Doran, C.M.; Hayman, M.J.; Alley, S.J. The Effectiveness of a Web-Based Computer-Tailored Physical Activity Intervention Using Fitbit Activity Trackers: Randomized Trial. J. Med. Internet Res. 2018, 20, e11321. [Google Scholar] [CrossRef]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Rayward, A.T.; Vandelanotte, C.; Van Itallie, A.; Duncan, M.J. The Association Between Logging Steps Using a Website, App, or Fitbit and Engaging With the 10,000 Steps Physical Activity Program: Observational Study. J. Med. Internet Res. 2021, 23, e22151. [Google Scholar] [CrossRef]
- Mandic, D.; Bjegovic-Mikanovic, V.; Vukovic, D.; Djikanovic, B.; Stamenkovic, Z.; Lalic, N.M. Successful promotion of physical activity among students of medicine through motivational interview and Web-based intervention. PeerJ 2020, 8, e9495. [Google Scholar] [CrossRef]
- Nomura, K.; Minamizono, S.; Maeda, E.; Kim, R.; Iwata, T.; Hirayama, J.; Ono, K.; Fushimi, M.; Goto, T.; Mishima, K.; et al. Cross-sectional survey of depressive symptoms and suicide-related ideation at a Japanese national university during the COVID-19 stay-home order. Environ. Health Prev. Med. 2021, 26, 1–9. [Google Scholar] [CrossRef]
- El Morr, C.; Ritvo, P.; Ahmad, F.; Moineddin, R.; Team, M. Effectiveness of an 8-Week Web-Based Mindfulness Virtual Community Intervention for University Students on Symptoms of Stress, Anxiety, and Depression: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e18595. [Google Scholar] [CrossRef] [PubMed]
- Wiljer, D.; Shi, J.; Lo, B.; Sanches, M.; Hollenberg, E.; Johnson, A.; Abi-Jaoudé, A.; Chaim, G.; Cleverley, K.; Henderson, J.; et al. Effects of a Mobile and Web App (Thought Spot) on Mental Health Help-Seeking Among College and University Students: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e20790. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, S.; Rizzi, S.; Bassi, G.; Carbone, S.; Maimone, R.; Marchesoni, M.; Forti, S. Engagement and Effectiveness of a Healthy Coping Intervention via Chatbot for university students: Proof-of-concept study during the COVID-19 pandemic. JMIR mHealth uHealth 2021, 9, e27965. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health Literacy: What Is It? J. Health Commun. 2010, 15, 9–19. [Google Scholar] [CrossRef]
- Diviani, N.; Putte, B.V.D.; Giani, S.; Van Weert, J.C. Low Health Literacy and Evaluation of Online Health Information: A Systematic Review of the Literature. J. Med. Internet Res. 2015, 17, e112. [Google Scholar] [CrossRef] [Green Version]
- Levin-Zamir, D.; Baron-Epel, O.; Cohen, V.; Elhayany, A. The Association of Health Literacy with Health Behavior, Socioeconomic Indicators, and Self-Assessed Health from a National Adult Survey in Israel. J. Health Commun. 2016, 21, 61–68. [Google Scholar] [CrossRef]
- Sentell, T.L.; Tsoh, J.; Davis, T.; Davis, J.; Braun, K.L. Low health literacy and cancer screening among Chinese Americans in California: A cross-sectional analysis. BMJ Open 2015, 5, e006104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 125) | Intervention (n = 60) | Control (n = 65) | |
|---|---|---|---|
| Age (years), mean ± SD | 21.6 ± 2.9 | 21.6 ± 2.7 | 21.5 ± 1.4 |
| Height (cm), mean ± SD | 164.6 ± 9.8 | 164.7 ± 8.8 | 164.5 ± 8.8 |
| Weight (kg), mean ± SD | 57.0 ± 11.1 | 56.5 ± 11.5 | 57.3 ± 9.9 |
| BMI (kg/m2), mean ± SD | 21.2 ± 2.2 | 21.0 ± 2.1 | 21.3 ± 2.3 |
| Sex, n (%) | |||
| Male | 57 (45.6) | 30 (50.0) | 27 (41.5) |
| Female | 68 (54.4) | 30 (50.0) | 38 (58.5) |
| Belong to an active community, n (%) | |||
| Yes | 52 (41.6) | 23 (38.3) | 29 (44.6) |
| No | 73 (58.4) | 37 (61.7) | 36 (55.4) |
| Experience watching exercise videos, n (%) | |||
| Yes | 87 (69.6) | 38 (63.3) | 49 (75.4) |
| No | 38 (30.4) | 22 (33.7) | 16 (24.6) |
| Expected effects of video streaming, n (%) | |||
| Health promotion | 52 (41.6) | 25 (41.7) | 27 (41.5) |
| Muscle strength | 36 (28.8) | 14 (23.3) | 22 (33.9) |
| Change of mood | 25 (20.0) | 12 (20.0) | 13 (20.0) |
| Diet | 6 (4.8) | 4 (6.7) | 2 (3.1) |
| Other | 6 (4.8) | 5 (6.3) | 1 (1.5) |
| Sedentary time (hour), mean ± SD | 9.7 ± 2.8 | 9.4 ± 2.6 | 9.9 ± 2.7 |
| Intervention | Control | |||
|---|---|---|---|---|
| Baseline (n = 60) | Follow-Up (n = 39) | Baseline (n = 65) | Follow-Up (n = 49) | |
| IPAQ, mean ± SEM | ||||
| Total physical activity (MET-min/week) | 1304.4 ± 128.9 | 1851 ± 162.1 | 1485.1 ± 173.0 | 1670.9 ± 163.3 |
| Sedentary time (hour/day) | 9.66 ± 0.22 | 8.82 ± 0.27 | 8.99 ± 0.29 | 9.48 ± 0.28 |
| SF-8 (score), mean ± SEM | ||||
| PCS | 51.9 ± 0.4 | 53.1 ± 0.5 | 52.6 ± 0.5 | 52.4 ± 0.5 |
| MCS | 48.6 ± 0.4 | 49.6 ± 0.6 | 49.2 ± 0.6 | 49.0 ± 0.6 |
| General health | 53.1 ± 0.4 | 54.6 ± 0.6 | 53.8 ± 0.6 | 53.9 ± 0.6 |
| Physical function | 51.9 ± 0.3 | 52.6 ± 0.4 | 52.0 ± 0.4 | 52.5 ± 0.5 |
| Role physical | 51.6 ± 0.4 | 53.1 ± 0.5 | 52.6 ± 0.5 | 52.5 ± 0.4 |
| Bodily pain | 51.6 ± 0.5 | 53.2 ± 0.7 | 53.5 ± 0.7 | 51.3 ± 0.7 |
| Vitality | 54.1 ± 0.3 | 54.1 ± 0.4 | 52.9 ± 0.4 | 53.9 ± 0.4 |
| Social functioning | 50.4 ± 0.5 | 51.8 ± 0.6 | 51.3 ± 0.6 | 50.9 ± 0.6 |
| Mental health | 49.6 ± 0.4 | 50.8 ± 0.5 | 50.5 ± 0.6 | 49.8 ± 0.5 |
| Role emotional | 49.9 ± 0.4 | 50.7 ± 0.5 | 50.4 ± 0.5 | 50.2 ± 0.5 |
| WHO-5 (score), mean ± SEM | 15.9 ± 0.4 | 17.0 ± 0.43 | 16.4 ± 16.6 | 16.6 ± 0.4 |
| K6 (score), mean ± SEM | 4.7 ± 0.3 | 3.8 ± 0.3 | 4.0 ± 0.3 | 4.5 ± 0.4 |
| Outcome and Source | Intercept | Time | Group | Interactive Effect (Time × Group) | ||||
|---|---|---|---|---|---|---|---|---|
| F test | p Value | F test | p Value | F test | p Value | F test | p Value * | |
| IPAQ | ||||||||
| Total physical activity | 1932.53 | <0.001 | 10.23 | 0.002 | 0.61 | 0.432 | 0.02 | 0.891 |
| Sedentary time | 2059.69 | <0.001 | 8.68 | 0.004 | 1.42 | 0.235 | 0.29 | 0.586 |
| SF-8 | ||||||||
| PCS | 18,834.15 | <0.001 | 4.15 | 0.043 | 0.07 | 0.782 | 0.28 | 0.596 |
| MCS | 12,228.78 | <0.001 | 2.38 | 0.125 | 0.03 | 0.855 | 2.02 | 0.157 |
| General health | 13,517.86 | <0.001 | 5.33 | 0.023 | <0.001 | 0.988 | 9.52 | 0.003 |
| Physical function | 29,077.31 | <0.001 | 1.83 | 0.179 | 0.86 | 0.353 | 0.71 | 0.403 |
| Role physical | 21,454.89 | <0.001 | 3.48 | 0.064 | 3.48 | 0.064 | 0.22 | 0.638 |
| Bodily pain | 9370.03 | <0.001 | 4.61 | 0.034 | 4.35 | 0.038 | 0.23 | 0.626 |
| Vitality | 24,718.25 | <0.001 | 8.18 | 0.005 | 2.13 | 0.146 | 2.97 | 0.087 |
| Social functioning | 12,454.57 | <0.001 | 3.87 | 0.051 | 0.17 | 0.679 | 0.92 | 0.337 |
| Mental health | 13,645.09 | <0.001 | 3.88 | 0.051 | 0.71 | 0.398 | 0.90 | 0.342 |
| Role emotional | 15,365.89 | <0.001 | 1.56 | 0.212 | 0.04 | 0.829 | 2.06 | 0.153 |
| WHO-5 | 24,497.38 | <0.001 | 6.18 | 0.010 | 0.11 | 0.730 | 6.70 | 0.010 |
| K6 | 24,902.61 | <0.001 | 7.21 | 0.008 | 0.84 | 0.360 | 7.83 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukui, K.; Suzuki, Y.; Kaneda, K.; Kuroda, S.; Komiya, M.; Maeda, N.; Urabe, Y. Do “Stay-at-Home Exercise” Videos Induce Behavioral Changes in College Students? A Randomized Controlled Trial. Sustainability 2021, 13, 11600. https://0-doi-org.brum.beds.ac.uk/10.3390/su132111600
Fukui K, Suzuki Y, Kaneda K, Kuroda S, Komiya M, Maeda N, Urabe Y. Do “Stay-at-Home Exercise” Videos Induce Behavioral Changes in College Students? A Randomized Controlled Trial. Sustainability. 2021; 13(21):11600. https://0-doi-org.brum.beds.ac.uk/10.3390/su132111600
Chicago/Turabian StyleFukui, Kazuki, Yuta Suzuki, Kazuki Kaneda, Sayo Kuroda, Makoto Komiya, Noriaki Maeda, and Yukio Urabe. 2021. "Do “Stay-at-Home Exercise” Videos Induce Behavioral Changes in College Students? A Randomized Controlled Trial" Sustainability 13, no. 21: 11600. https://0-doi-org.brum.beds.ac.uk/10.3390/su132111600