
REaCH-Resiliency Engagement and Care in Health; a Befriending Intervention to Address the Psycho-Social Challenges of Vulnerable Youth in the Context of COVID-19 Pandemic: An Exploratory Trial in India

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
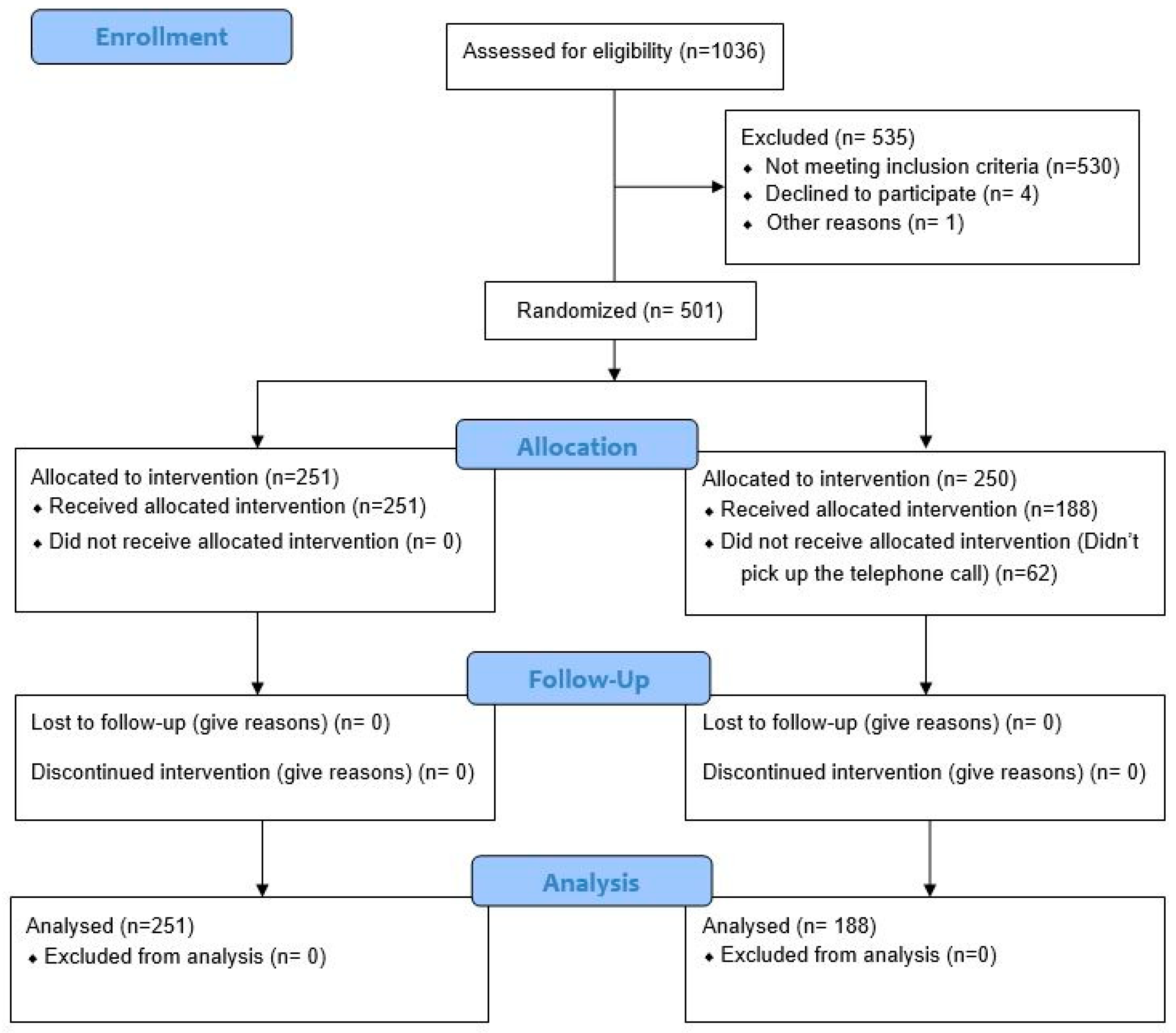
2.1. Study Design
2.2. Ethics
2.3. Study Participants
2.4. Randomisation
2.5. Intervention
- proactive engagement and crisis intervention,
- problem-solving oriented supportive therapy, and
- assertive linkage with community resources.
2.6. Training of the Staff
2.7. Intervention Arm: Resiliency Engagement and Care in Health (REaCH)
2.8. Control Arm: General Enquiry Phone Calls (GETC)
2.9. Study Tools
2.9.1. Assessments and Procedures
2.9.2. Outcome Measures
2.10. Data Analysis
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zandifar, A.; Badrfam, R. Iranian mental health during the COVID-19 epidemic. Asian J. Psychiatry 2020, 51, 101990. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Social Determinants of Mental Health. Available online: https://apps.who.int/iris/bitstream/handle/10665/112828/9789241506809_eng.pdf (accessed on 5 August 2021).
- Campion, J.; Bhugra, D.; Bailey, S.; Marmot, M. Inequality and mental disorders: Opportunities for action. Lancet 2013, 382, 183–184. [Google Scholar] [CrossRef]
- Patel, V.; Kleinman, A. Poverty and common mental disorders in developing countries. Bull. World Health Organ. 2003, 81, 609–615. [Google Scholar] [PubMed]
- McManus, S.; Meltzer, H.; Brugha, T.; Bebbington, P.E.; Jenkins, R. Adult Psychiatric Morbidity in England—2007, Results of a Household Survey; Health and Social Care Information Centre: Leeds, UK, 2009.
- Lehtinen, V.; Sohlman, B.; Kovess-Masfety, V. Level of positive mental health in the European Union: Results from the Eurobarometer 2002 survey. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebarik, D.; Ethorat, A. Issues of Unequal Access to Public Health in India. Front. Public Health 2015, 3, 245. [Google Scholar] [CrossRef] [Green Version]
- Harandi, T.F.; Taghinasab, M.M.; Nayeri, T.D. The correlation of social support with mental health: A meta-analysis. Electron. Physician 2017, 9, 5212–5222. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.; Pistrang, N. Befriending for mental health problems: Processes of helping. Psychol. Psychother. Theory Res. Pract. 2011, 84, 151–169. [Google Scholar] [CrossRef] [PubMed]
- Peardon, L.; Yellowlees, D.; Pratt, R.; Reid, J.; O’Donnell, M.; Ness, A.; Chalmers, C.; Leslie, S.J.; Denvir, M.A. The Use of Innovative Methods Designed to Relieve Social Isolation in Patients with Chronic Heart Failure; Volunteer Befriending, Forums and a Newsletter. Eur. J. Cardiovasc. Nurs. 2010, 9, 181–187. [Google Scholar] [CrossRef]
- Bradshaw, T.; Haddock, G. Is befriending by trained volunteers of value to people suffering from long-term mental illness? J. Adv. Nurs. 1998, 27, 713–720. [Google Scholar] [CrossRef]
- Hoeft, T.J.; Fortney, J.C.; Patel, V.; Unützer, J. Task-Sharing Approaches to Improve Mental Health Care in Rural and Other Low-Resource Settings: A Systematic Review. J. Rural. Health 2018, 34, 48–62. [Google Scholar] [CrossRef]
- Deen Dayal Upadhyaya Grameen Kaushalya Yojana. Available online: http://ddugky.gov.in/ (accessed on 5 August 2021).
- Census of India Website: Office of the Registrar General & Census Commissioner, India. Available online: https://censusindia.gov.in/2011-common/censusdata2011.html (accessed on 6 August 2021).
- FICCI. FICCI Survey on Labour/Skill Shortage for Industry. Available online: https://ficci.in/sedocument/20165/ficci_labour_survey.pdf (accessed on 4 August 2021).
- Mead, N.; Lester, H.; Chew-Graham, C.; Gask, L.; Bower, P. Effects of befriending on depressive symptoms and distress: Systematic review and meta-analysis. Br. J. Psychiatry 2010, 196, 96–101. [Google Scholar] [CrossRef] [PubMed]
- McGowan, B.; Jowett, M.C. Promoting Positive Mental Health through Befriending. Int. J. Ment. Health Promot. 2003, 5, 12–24. [Google Scholar] [CrossRef]
- Balaam, M.-C. A concept analysis of befriending. J. Adv. Nurs. 2015, 71, 24–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devassy, S.M.; Allagh, K.P.; Benny, A.M.; Scaria, L.; Cheguvera, N.; Sunirose, I.P. Resiliency Engagement and Care in Health (REaCH): A telephone befriending intervention for upskilled rural youth in the context of COVID-19 pandemic—study protocol for a multi-centre cluster randomised controlled trial. Trials 2021, 22, 500. [Google Scholar] [CrossRef] [PubMed]
- Saju, M.D.; Scaria, L.; Cheguvera, N.; Benny, A.M.; Lizy, P.J.; Joseph, B. Evidencing the need for psycho-socio-economic action to support the rural upskilled youth to cope with the COVID-19 health crisis: A state-wide audit. F1000Research 2020, 9, 1375. [Google Scholar] [CrossRef]
- O’Neill, A. Youth Unemployment Rate in India in 2019. 2021. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/812106/youth-unemployment-rate-in-india/ (accessed on 17 September 2021).
- Mehrotra, S. India Has an Unemployment Crisis. And It Predates COVID-19. 2021. Available online: https://www.hindustantimes.com/opinion/india-has-an-unemployment-crisis-and-it-predates-covid19-101629287437935.html (accessed on 17 September 2021).
- UNESCO. India’s Youth: Hit Hard by the Pandemic. Available online: https://en.unesco.org/courier/2021-2/indias-youth-hit-hard-pandemic (accessed on 17 September 2021).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- WHO. Well-Being Measures in Primary Health Care/The Depcare Project. 1998. Available online: https://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf (accessed on 4 July 2020).
- Dambi, J.M.; Corten, L.; Chiwaridzo, M.; Jack, H.; Mlambo, T.; Jelsma, J. A systematic review of the psychometric properties of the cross-cultural translations and adaptations of the Multidimensional Perceived Social Support Scale (MSPSS). Health Qual. Life Outcomes 2018, 16, 80. [Google Scholar] [CrossRef] [Green Version]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Indu, P.S.; Anilkumar, T.V.; Vijayakumar, K.; Kumar, K.; Sarma, P.S.; Remadevi, S.; Andrade, C. Reliability and validity of PHQ-9 when administered by health workers for depression screening among women in primary care. Asian J. Psychiatry 2018, 37, 10–14. [Google Scholar] [CrossRef]
- Zimet, G.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric Characteristics of the Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1990, 55, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Laksmita, O.D.; Chung, M.-H.; Liao, Y.-M.; Chang, P.-C. Multidimensional Scale of Perceived Social Support in Indonesian adolescent disaster survivors: A psychometric evaluation. PLoS ONE 2020, 15, e0229958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortazavi, F.; Mousavi, S.A.; Chaman, R.; Khosravi, A. Dünya Sağlık Örgütü-5 İyilik Hali Endeksi Geçerliği:Annenin İyilik Hali ve Bununla İlişkili Faktörlerin Değerlendirilmesi [Validation of the World Health Organization-5 Well-Being Index; Assessment of Maternal Well-Being and Its Associated Factors]. Turk. J. Psychiatry 2015, 26, 48–55. [Google Scholar]
- Siette, J.; Cassidy, M.; Priebe, S. Effectiveness of befriending interventions: A systematic review and meta-analysis. BMJ Open 2017, 7, e014304. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, N.; Myers, B.J. Cultural influences on perceptions of health, illness, and disability: A review and focus on autism. J. Child Fam. Stud. 2012, 21, 311–319. [Google Scholar] [CrossRef]
- Taub, A. A New COVID-19 Crisis: Domestic Abuse Rises Worldwide. The New York Times. Available online: https://www.nytimes.com/2020/04/06/world/coronavirus-domestic-violence.html (accessed on 19 April 2021).
- Bettinger-Lopez, C.; Bro, A. A Double Pandemic: Domestic Violence in the Age of COVID-19. Available online: https://www.cfr.org/in-brief/double-pandemic-domestic-violence-age-covid-19 (accessed on 15 April 2021).
- Zhang, H. The Influence of the Ongoing COVID-19 Pandemic on Family Violence in China. J. Fam. Violence 2020, 1–11. [Google Scholar] [CrossRef]
- Gjesfjeld, C.D.; Greeno, C.G.; Kim, K.H.; Anderson, C.M. Economic Stress, Social Support, and Maternal Depression: Is Social Support Deterioration Occurring? Soc. Work. Res. 2010, 34, 135–143. [Google Scholar] [CrossRef]
- Divan, G.; Vajaratkar, V.; Desai, M.U.; Strik-Lievers, L.; Patel, V. Challenges, coping strategies, and unmet needs of families with a child with autism spectrum disorder in Goa, India. Autism Res. 2012, 5, 190–200. [Google Scholar] [CrossRef]
- Nelson, R. Combating Global Health Worker Shortages. AJN Am. J. Nurs. 2012, 112, 17–18. [Google Scholar] [CrossRef]
- Buttorff, C.; Hock, R.S.; Weiss, H.A.; Naik, S.; Araya, R.; Kirkwood, B.R.; Chisholm, D.; Patel, V. Economic evaluation of a task-shifting intervention for common mental disorders in India. Bull. World Health Organ. 2012, 90, 813–821. [Google Scholar] [CrossRef]
- Niti Ayog. Planning and Implementation Issues. Available online: https://niti.gov.in/planningcommission.gov.in/docs/plans/planrel/fiveyr/10th/volume3/v3_ch5.pdf (accessed on 17 September 2021).


{kind=link}
| Variables | Total | General enquiry Telephonic Calls Group (n = 188) | REaCH Befriending Intervention Group (n = 251) |
|---|---|---|---|
| Age, in years | 25.1 (5.7) | 25.5 (6.2) | 24.8 (5.2) |
| Gender | |||
| Female | 282 (64.24%) | 122 (64.89%) | 160 (63.75%) |
| Male | 157 (35.76%) | 66 (35.11%) | 91 (36.25%) |
| Education | |||
| Completed 10th | 38 (8.66%) | 19 (10.11%) | 19 (7.57%) |
| Completed 12th | 174 (39.64%) | 77 (40.96%) | 97 (38.65%) |
| Completed graduation | 206 (46.92%) | 81 (43.09%) | 125 (49.80%) |
| Completed post-graduation | 21 (4.78%) | 11 (5.85%) | 10 (3.98%) |
| Occupation | |||
| Paid job | 147 (33.49%) | 63 (33.51%) | 84 (33.47%) |
| Self employed | 5 (1.14%) | 4 (2.13%) | 1 (0.40%) |
| Housewife | 54 (12.30%) | 26 (13.83%) | 28 (11.16%) |
| Unemployed | 134 (30.52%) | 48 (25.53%) | 86 (34.26%) |
| Daily wage | 99 (22.55%) | 47 (25.00%) | 52 (20.72%) |
| Marital status | |||
| Unmarried | 279 (63.55%) | 120 (63.83%) | 159 (63.35%) |
| Married | 153 (34.85%) | 67 (35.64%) | 86 (34.26%) |
| Divorced/widowed/separated | 7 (1.59%) | 1 (0.53%) | 6 (2.39%) |
| Colour of ration card a | |||
| Yellow | 35 (7.97%) | 15 (7.98%) | 20 (7.97%) |
| Pink | 218 (49.66%) | 95 (50.53%) | 123 (49.00%) |
| Blue | 147 (33.49%) | 61 (32.45%) | 86 (34.26%) |
| White | 39 (8.88%) | 17 (9.04%) | 22 (8.76%) |
| REaCH—Befriending Intervention | GETC | REaCH Model v/s GETC | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean (S.D) | T(df) | p | Mean (S.D) | T(df) | p | OR (95% CI) | p | |
| Wellbeing | ||||||||
| Baseline | 15.82 (5.7) | −3.99 (250) | 0.000 | 15.26 (5.2) | −3.12 (187) | 0.010 | ||
| Post-assessment | 17.42 (4.9) | 16.87(5.5) | 1.02 (0.98, 1.05) | 0.274 | ||||
| Depressive symptoms | ||||||||
| Baseline | 4.80 (3.5) | 0.88 (250) | 0.812 | 4.93 (3.5) | −1.06 (187) | 0.143 | ||
| Post-assessment | 4.53 (3.6) | 5.26 (4.1) | 0.95 (0.90, 1.00) | 0.055 | ||||
| Social Support | ||||||||
| Baseline | 65.37 (13.8) | −2.55 (250) | 0.005 | 64.5 (12.8) | 1.96 (187) | 0.97 | ||
| Post-assessment | 67.89 (13.4) | 62.84 (14.0) | 1.03 (1.01, 1.04) | 0.000 | ||||
| Suicidality | ||||||||
| Baseline | 0.25 (0.6) | 0.14 (250) | 0.55 | 0.24 (0.6) | −1.23 (187) | 0.10 | ||
| Post Assessment | 0.24 (0.6) | 0.32 (0.6) | 0.80 (0.59, 1.08) | 0.156 | ||||
| REaCH—Befriending Intervention | GETC | REaCH Model v/s GETC | ||
|---|---|---|---|---|
| Mean (S.D) | Mean (S.D) | Odds Ratio (95% CI) | p | |
| Social support-Family | ||||
| Baseline | 22.26 (5.1) | 22.11 (4.4) | ||
| Post-assessment | 21.71 (5.6) | 20.20 (6.7) | 1.04 (1.00, 1.07) | 0.012 |
| Social Support-friends | ||||
| Baseline | 21.24 (4.9) | 20.66 (5) | ||
| Post-assessment | 20.84 (5.4) | 19.14 (6.8) | 1.04 (1.01, 1.08) | 0.004 |
| Social support-Significant others | ||||
| Baseline | 21.85 (5.1) | 21.76 (4.6) | ||
| Post-assessment | 20.52 (5.3) | 20.06 (6.9) | 1.04 (1.00, 1.07) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devassy, S.M.; Scaria, L.; Shaju, K.K.; Cheguvera, N.; Joseph, M.K.; Benny, A.M.; Joseph, B. REaCH-Resiliency Engagement and Care in Health; a Befriending Intervention to Address the Psycho-Social Challenges of Vulnerable Youth in the Context of COVID-19 Pandemic: An Exploratory Trial in India. Sustainability 2021, 13, 12920. https://0-doi-org.brum.beds.ac.uk/10.3390/su132212920
Devassy SM, Scaria L, Shaju KK, Cheguvera N, Joseph MK, Benny AM, Joseph B. REaCH-Resiliency Engagement and Care in Health; a Befriending Intervention to Address the Psycho-Social Challenges of Vulnerable Youth in the Context of COVID-19 Pandemic: An Exploratory Trial in India. Sustainability. 2021; 13(22):12920. https://0-doi-org.brum.beds.ac.uk/10.3390/su132212920
Chicago/Turabian StyleDevassy, Saju Madavanakadu, Lorane Scaria, Kalluparambil Kesavan Shaju, Natania Cheguvera, Mannooparambil K. Joseph, Anuja Maria Benny, and Binoy Joseph. 2021. "REaCH-Resiliency Engagement and Care in Health; a Befriending Intervention to Address the Psycho-Social Challenges of Vulnerable Youth in the Context of COVID-19 Pandemic: An Exploratory Trial in India" Sustainability 13, no. 22: 12920. https://0-doi-org.brum.beds.ac.uk/10.3390/su132212920