
Physical Exercise Improves Heart-Rate Variability in Obese Children and Adolescents: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Risk of Bias
2.3. Data Extraction
3. Results
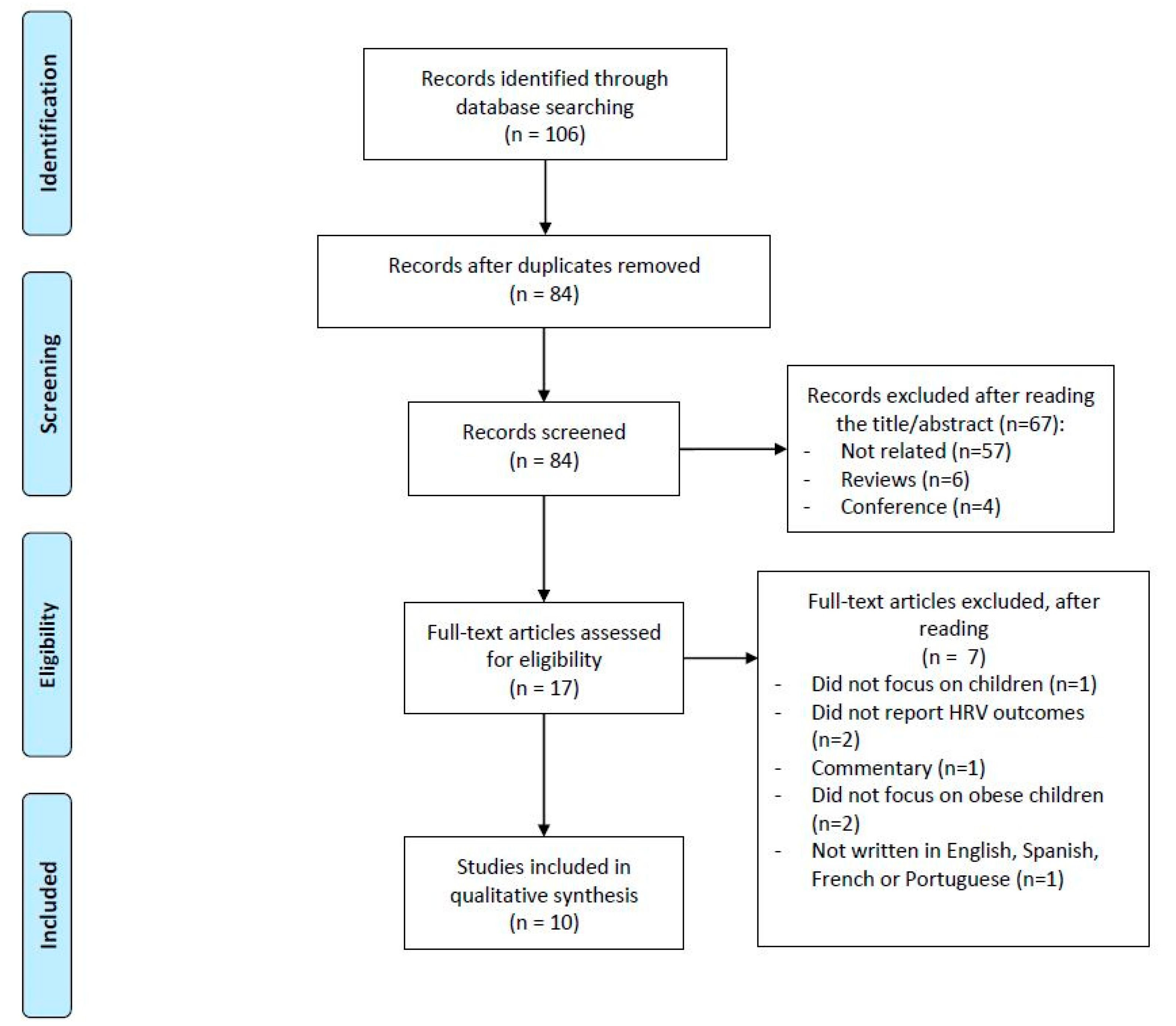
3.1. Article Selection
3.2. Risk of Bias
3.3. Participants
3.4. Study Design
3.5. Intervention
3.6. Comparison Groups
3.7. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NCD-Risk-Factor-Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Jastreboff, A.M.; Kotz, C.M.; Kahan, S.; Kelly, A.S.; Heymsfield, S.B. Obesity as a disease: The obesity society 2018 position statement. Obesity 2019, 27, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J.H. Health consequences of obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Pontifex, M.B.; O’Leary, K.C.; Scudder, M.R.; Wu, C.T.; Castelli, D.M.; Hillman, C.H. The effects of an afterschool physical activity program on working memory in preadolescent children. Dev. Sci. 2011, 14, 1046–1058. [Google Scholar] [CrossRef] [Green Version]
- Pelone, F.; Specchia, M.L.; Veneziano, M.A.; Capizzi, S.; Bucci, S.; Mancuso, A.; Ricciardi, W.; de Belvis, A.G. Economic impact of childhood obesity on health systems: A systematic review. Obes. Rev. 2012, 13, 431–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachs, J.D. From millennium development goals to sustainable development goals. Lancet 2012, 379, 2206–2211. [Google Scholar] [CrossRef]
- Wolters, E.A.; Steel, B.S. Sustainable futures: Healthy lifestyles, obesity, and access to food in US counties 2012. Agric. Agric. Sci. Procedia 2016, 8, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Skouteris, H.; Cox, R.; Huang, T.; Rutherford, L.; Edwards, S.; Cutter-Mackenzie, A. Promoting obesity prevention together with environmental sustainability. Health Promot. Int. 2014, 29, 454–462. [Google Scholar] [CrossRef] [Green Version]
- The Lancet Diabetes Endocrinology. Obesity and sustainability-in transition. Lancet Diabetes Endocrinol. 2019, 7, 161. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Prado, W.L.; Siegfried, A.; Dâmaso, A.R.; Carnier, J.; Piano, A.D.; Siegfried, W. Effects of long-term multidisciplinary inpatient therapy on body composition of severely obese adolescents. J. Pediatr. 2009, 85, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Tjønna, A.E.; Stølen, T.O.; Bye, A.; Volden, M.; Slørdahl, S.A.; Ødegård, R.; Skogvoll, E.; Wisløff, U. Aerobic interval training reduces cardiovascular risk factors more than a multitreatment approach in overweight adolescents. Clin. Sci. 2009, 116, 317–326. [Google Scholar] [CrossRef] [Green Version]
- Ingul, C.B.; Tjonna, A.E.; Stolen, T.O.; Stoylen, A.; Wisloff, U. Impaired cardiac function among obese adolescents: Effect of aerobic interval training. Arch. Pediatrics Adolesc. Med. 2010, 164, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Balagopal, P.; De Ferranti, S.D.; Cook, S.; Daniels, S.R.; Gidding, S.S.; Hayman, L.L.; McCrindle, B.W.; Mietus-Snyder, M.L.; Steinberger, J. Nontraditional risk factors and biomarkers for cardiovascular disease: Mechanistic, research, and clinical considerations for youth: A scientific statement from the American Heart Association. Circulation 2011, 123, 2749–2769. [Google Scholar] [CrossRef] [Green Version]
- Steinberger, J.; Kelly, A.S. Challenges of existing pediatric dyslipidemia guidelines: Call for reappraisal. Circulation 2008, 117, 9–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggio, A.B.R.; Aggoun, Y.; Martin, X.E.; Marchand, L.M.; Beghetti, M.; Farpour-Lambert, N.J. Long-term follow-up of cardiovascular risk factors after exercise training in obese children. Int. J. Pediatric Obes. 2011, 6, e603–e610. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1· 6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Freeman, J.V.; Dewey, F.E.; Hadley, D.M.; Myers, J.; Froelicher, V.F. Autonomic nervous system interaction with the cardiovascular system during exercise. Prog. Cardiovasc. Dis. 2006, 48, 342–362. [Google Scholar] [CrossRef]
- Dekker, J.M.; Crow, R.S.; Folsom, A.R.; Hannan, P.J.; Liao, D.; Swenne, C.A.; Schouten, E.G. Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes—The ARIC study. Circulation 2000, 102, 1239–1244. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Syme, C.; McCrindle, B.W.; Hamilton, J. Autonomic nervous system balance in children and adolescents with craniopharyngioma and hypothalamic obesity. Eur. J. Endocrinol. 2013, 168, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, C.L.; Kaiser, D.R.; Steinberger, J.; Kelly, A.S.; Dengel, D.R. Relationships of cardiac autonomic function with metabolic abnormalities in childhood obesity. Obesity 2007, 15, 1164–1171. [Google Scholar] [CrossRef] [Green Version]
- Rabbia, F.; Silke, B.; Conterno, A.; Grosso, T.; De Vito, B.; Rabbone, I.; Chiandussi, L.; Veglio, F. Assessment of cardiac autonomic modulation during adolescent obesity. Obesity Res. 2003, 11, 541–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva, D.F.; Bianchini, J.A.A.; Antonini, V.D.S.; Hermoso, D.A.M.; Lopera, C.A.; Pagan, B.G.M.; McNeil, J.; Junior, N.N. Parasympathetic cardiac activity is associated with cardiorespiratory fitness in overweight and obese adolescents. Pediatric Cardiol. 2014, 35, 684–690. [Google Scholar] [CrossRef]
- Amano, M.; Kanda, T.; Ue, H.; Moritani, T. Exercise training and autonomic nervous system activity in obese individuals. Med. Sci. Sports Exerc. 2001, 33, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, F.; Seabra, A.; Cunha, F.; Montenegro, R.; Penha, J.; Bouskela, E.; Nogueira Neto, J.F.; Collett-Solberg, P.; Farinatti, P. Health markers in obese adolescents improved by a 12-week recreational soccer program: A randomised controlled trial. J. Sports Sci. 2016, 34, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Farah, B.Q.; Ritti-Dias, R.M.; Balagopal, P.; Hill, J.O.; Prado, W.L. Does exercise intensity affect blood pressure and heart rate in obese adolescents? A 6-month multidisciplinary randomized intervention study. Pediatric Obes. 2014, 9, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Brasil, I.; Monteiro, W.; Lima, T.; Seabra, A.; Farinatti, P. Effects of judo training upon body composition, autonomic function, and cardiorespiratory fitness in overweight or obese children aged 8 to 13 years. J. Sports Sci. 2020, 38, 2508–2516. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Kennedy, C.E.; Fonner, V.A.; Armstrong, K.A.; Denison, J.A.; Yeh, P.T.; O’Reilly, K.R.; Sweat, M.D. The evidence project risk of bias tool: Assessing study rigor for both randomized and non-randomized intervention studies. Syst. Rev. 2019, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Farinatti, P.; Neto, S.R.M.; Dias, I.; Cunha, F.A.; Bouskela, E.; Kraemer-Aguiar, L.G. Short-term resistance training attenuates cardiac autonomic dysfunction in obese adolescents. Pediatric Exerc. Sci. 2016, 28, 374–380. [Google Scholar] [CrossRef]
- Faulkner, M.S.; Michaliszyn, S.F.; Hepworth, J.T.; Wheeler, M.D. Personalized exercise for adolescents with diabetes or obesity. Biol. Res. Nurs. 2014, 16, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Lai, Q.; Wang, D.; Yin, H.; Liao, J.; Wang, S.; Xu, F.; Hou, X.; Hu, M. Effects Of Exercise Training With Dietary Restriction On Arterial Stiffness, Central Hemodynamic Parameters And Cardiac Autonomic Function In Obese Adolescents. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2157. [Google Scholar] [CrossRef] [Green Version]
- Gutin, B.; Barbeau, P.; Litaker, M.S.; Ferguson, M.; Owens, S. Heart rate variability in obese children: Relations to total body and visceral adiposity, and changes with physical training and detraining. Obes. Res. 2000, 8, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prado, D.M.; Silva, A.G.; Trombetta, I.C.; Ribeiro, M.M.; Guazzelli, I.C.; Matos, L.N.; Santos, M.S.; Nicolau, C.M.; Negrão, C.E.; Villares, S.M. Exercise training associated with diet improves heart rate recovery and cardiac autonomic nervous system activity in obese children. Int. J. Sports Med. 2010, 31, 860–865. [Google Scholar] [CrossRef]
- Chen, S.-R.; Tseng, C.-L.; Kuo, S.-Y.; Chang, Y.-K. Effects of a physical activity intervention on autonomic and executive functions in obese young adolescents: A randomized controlled trial. Health Psychol. 2016, 35, 1120. [Google Scholar] [CrossRef]
- Hamila, A.; Younes, M.; Cottin, F.; Amor, Y.B.; Shephard, R.; Tabka, Z.; Bouhlel, E. Effects of walking exercises on body composition, heart rate variability, and perceptual responses in overweight and obese adolescents. Sci. Sports 2018, 33, e191–e202. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Ayer, J.G.J. Childhood risk factors for adult cardiovascular disease and primary prevention in childhood. Heart 2006, 92, 1701–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, H.A.; Benton, D. Heart-rate variability: A biomarker to study the influence of nutrition on physiological and psychological health? Behav. Pharmacol. 2018, 29, 140–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsillio, L.E.; Manghi, T.; Carroll, M.S.; Balmert, L.C.; Wainwright, M.S. Heart rate variability as a marker of recovery from critical illness in children. PLoS ONE 2019, 14, e0215930. [Google Scholar] [CrossRef] [PubMed]
- Tarride, J.-E.; Lim, M.; DesMeules, M.; Luo, W.; Burke, N.; O’Reilly, D.; Bowen, J.; Goeree, R. A review of the cost of cardiovascular disease. Can. J. Cardiol. 2009, 25, e195–e202. [Google Scholar] [CrossRef] [Green Version]
- Movsisyan, N.K.; Vinciguerra, M.; Medina-Inojosa, J.R.; Lopez-Jimenez, F. Cardiovascular Diseases in Central and Eastern Europe: A Call for More Surveillance and Evidence-Based Health Promotion. Ann. Glob. Health 2020, 86, 21. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Freedman, N.D.; Albert, P.S.; Huxley, R.R.; Shiels, M.S.; Withrow, D.R.; Spillane, S.; Powell-Wiley, T.M.; de González, A.B. Association of cardiovascular disease with premature mortality in the United States. JAMA Cardiol. 2019, 4, 1230–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Blüher, S.; Petroff, D.; Keller, A.; Wagner, A.; Classen, J.; Baum, P. Effect of a 1-Year Obesity Intervention (KLAKS Program) on Preexisting Autonomic Nervous Dysfunction in Childhood Obesity. J. Child Neurol. 2015, 30, 1174–1181. [Google Scholar] [CrossRef]
- Eyre, E.L.; Duncan, M.J.; Birch, S.L.; Fisher, J.P. The influence of age and weight status on cardiac autonomic control in healthy children: A review. Auton. Neurosci. Basic Clin. 2014, 186, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Nagai, N.; Moritani, T. Effect of physical activity on autonomic nervous system function in lean and obese children. Int. J. Obes. 2004, 28, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, A.T.; Harris, K.C.; Panagiotopoulos, C.; Sandor, G.G.; Devlin, A.M. Childhood obesity and cardiovascular dysfunction. J. Am. Coll. Cardiol. 2013, 62, 1309–1319. [Google Scholar] [CrossRef] [Green Version]
- Krustrup, P.; Aagaard, P.; Nybo, L.; Petersen, J.; Mohr, M.; Bangsbo, J. Recreational football as a health promoting activity: A topical review. Scand. J. Med. Sci. Sports 2010, 20, 1–13. [Google Scholar] [CrossRef]


{kind=link}
| Study | Cohort | Control or Comparison Group | Pre-/Postintervention Data | Random Assignment of Participants to Intervention | Random Selection of Participants for Assessment | Follow-Up Rate of 80% or More | Comparison Groups Equivalent on Sociodemographics | Comparison Groups Equivalent at Baseline on Disclosure |
|---|---|---|---|---|---|---|---|---|
| Brasil (2020) |  | |  | | | | | |
| Chen (2016) | | | | | | | | |
| Farah (2012) | | | | | | | | |
| Farinatti (2016) | | | | | | | | |
| Faulkner (2013) | | | | | | | |  |
| Gutin (2000) | | | | | | | | |
| Hamila (2017) | | | | | | | | |
| Huang (2019) | | | | | | |  | |
| Prado (2010) | | | | | | | | |
| Vasconcellos (2015) | | | | | | | | |
| Study (Year) | Participants | Sample Size (N) | Age (SD) | Study Design | Control Group Protocol |
|---|---|---|---|---|---|
| Brasil (2020) | Obese children | 20 (10 g) | 11.1 (1.1) | Non-RCT | Usual life |
| Nonobese children | 15 (7 g) | 10.7 (1.6) | |||
| Chen (2016) | Obese adolescents | 25 (13 g) | EG: 12.64 (0.70) | RCT | Usual life |
| 25 (9 g) | CG: 12.84 (0.75) | ||||
| Farah (2012) | Obese adolescents | 9 (5 g) | HIT: 15.4 (0.4) | RCT | Light-intensity training |
| 10 (5 g) | LIT: 14.8 (0.4) | ||||
| Farinatti (2016) | Obese adolescents | 24 (17 g) | 13–17 | Non-RCT | Usual life |
| Nonobese adolescents | 20 (7 g) | ||||
| Faulkner (2013) | Obese adolescents | 10 (6 g) | 14.6 (1.6) | Non-RCT | Personalized aerobic training |
| Type II DM adolescents | 9 (8 g) | 14.7 (1.8) | |||
| Gutin (2000) | Obese children | 79 (53 g) | 9.5 (1) | Crossover | Usual life |
| Hamila (2017) | Obese adolescents | 7 (4 g) | EG: 14.5 (1) | RCT | Usual life |
| 8 (5 g) | CG: 14.5 (0.9) | ||||
| Huang (2019) | Obese adolescents | 21 (10 g) | 10–16 | Observational | - |
| Prado (2010) | Obese children | 18 | EG: 10.3 (0.2) | RCT | Diet |
| 15 | CG: 10.2 (0.3) | ||||
| Vasconcellos (2015) | Obese adolescents | 10 (4 g) | EG: 14.3 (1.3) | RCT | Usual life |
| 10 (2 g) | CG: 14.8 (1.4) |
| Study (Year) | Intervention Duration (Weeks) | Session Duration (Minute) | Weekly Frequency (Days) | Intensity | Activities Included in Session |
|---|---|---|---|---|---|
| Brasil (2020) | 12 | 60 | 2 | 65–75% maximal heart rate | Sessions consisted of 60 min of judo training for beginners (including 10 min warmup and 10 min cooldown). |
| Chen (2016) | 12 | 40 | 4 | 60–70% maximal heart rate | Participants were free to choose one of the provided exercise types (e.g., fast walking, stair climbing, jumping rope, or aerobic dancing). |
| Farah (2012) | 24 | Not fixed | 31 | HIT: at ventilatory threshold I. LIT: 20% below ventilatory threshold I. | Treadmill. |
| Farinatti (2016) | 12 | 30–40 | 3 | 50–85% 10 RM, progressively | One set of 10–15 repetitions (reps) with 50–70% of load corresponding to 10 RM for first 2 weeks; two sets of 8–12 reps with 60–80% 10 RM in weeks 3–6, and three sets of 6–10 reps with 70–85% 10 RM in weeks 7–12. |
| Faulkner (2013) | 16 | 60 | 7 | 65–75% maximal heart rate | Personalized training (based on participant interest) where participants performed activities such as calisthenics, kickboxing, dancing, cycling, walking, and Dance Dance Revolution (Konami, Japan). Activities could be conducted at gym facilities, parks, schools, participants’ homes, or all of the above. |
| Gutin (2000) | 16 | 40 | 5 | - | First 20 min were spent on machines (e.g., treadmill, cycle, Nordic ski machine), and next 20 min were devoted to games modified to maintain a high rate of energy expenditure. |
| Hamila (2017) | 8 | 50 | 3 | 70% maximal aerobic speed | Each session included a 10 min collective warmup based on ball games followed by 2 × 20 min periods of walking, interspersed by 10 maximal sprints on a cycle ergometer against a braking force equal to 0.75 g/kg body mass. |
| Huang (2019) | 6 | 5 h/day | 6 | - | Program primarily comprised various types of aerobic exercise such as bicycling, walking, running, dancing, and ball games for 5 h/day. It was supplemented by strength training. Endurance exercises involved moderate- (70–85% of maximal heart rate) and high-intensity (~90% of maximal heart rate) training. Strength training was conducted 2–3 times per week at 40–50% maximal strength for 2–3 sets of 12–15 repetitions maximum, with 2–3 min of rest between sets. Furthermore, participants were provided with calorie-restricted but nutritionally complete diet based on their age. |
| Prado (2010) | 16 | 60 | 3 | Ventilatory anaerobic threshold | Each exercise session consisted of 30 min of walking and/or jogging (aerobic exercise) on a jogging track, and 30 min of recreational exercise. |
| Vasconcellos (2015) | 12 | 60 | 3 | - | Each session consisted of a 10 min warmup followed by 40 min of games performed in small pitch areas (such as 2 vs. 2, 3 vs. 3, and 4 vs. 4), and a 10 min cooldown. |
| Authors | Recording Protocol and Instrument | Outcome Measure | EG Baseline | EG after Treatment | CG Baseline | CG after Treatment | Reported Effect |
|---|---|---|---|---|---|---|---|
| Brasil (2020) | 5 min (Polar RS800cx, PolarTM, Kempele, Finland) | RR (ln ms) | 2.85 (0.02) | 2.88 (0.02) | 2.88 (0.02) | - | WG |
| SDNN (ln ms) | 1.66 (0.06) | 1.64 (0.07) | 1.66 (0.05) | - | - | ||
| Rmssd (ln ms) | 1.64 (0.07) | 1.63 (0.07) | 1.67 (0.07) | - | - | ||
| Pnn50 (ln %) | 1.16 (0.12) | 1.19 (0.11) | 1.24 (0.12) | - | - | ||
| LF (ln ms2) | 1.75 (0.03) | 1.72 (0.02) | 1.71 (0.02) | - | - | ||
| HF (ln ms2) | 1.63 (0.02) | 1.70 (0.03) | 1.66 (0.03) | - | WG | ||
| LF/HF (ln ms2) | 0.13 (0.05) | 0.02 (0.03) | 0.06 (0.04) | - | BG (pre)/WG | ||
| Chen (2016) | 5 min Handheld device (CheckMyHeart 3.0, DailyCare BioMedical, Inc., Taoyuan, Taiwan) | Lf (nu) | 57.82 (15.64) | 62.85 (18.27) | 52.09 (16.3) | 48.56 (15.46) | BG |
| Hf (nu) | 42.27 (13.38) | 42.37 (13.38) | 42.27 (13.38) | 42.37 (13.38) | EG (WG)/BG | ||
| Farah (2012) | 7 min (Polar RS800cx, PolarTM, Kempele, Finland) | Mean RR (ms) | 757 (55) | - | 810 (31) | - | EG (WG)/BG |
| SDNN (ms) | 75 (16) | - | 88 (9) | - | |||
| rMSSD (ms) | 57 (18) | - | 66 (9) | - | |||
| Pnn50 (%) | 26 (10) | - | 33 (5) | - | EG (WG)/BG | ||
| LF (ms2) | 3941 (1320) | - | 5090 (1000) | - | |||
| HF (ms2) | 1602 (1014) | - | 1842 (392) | - | EG (WG) | ||
| Farinatti (2016) | 15 min Noninvasive device (Finometer, Finapres Medical Systems, Amsterdam, The Netherlands) | Mean RR (ms) | 746.2 (71.4) | - | 862.4 (126) | - | WG |
| SDNN (ms) | 58.3 (25.5) | - | 79.8 (35.9) | - | WG | ||
| rMSSD (ms) | 46 (18.4) | - | 74.3 (21.5) | - | BG (pre)/WG | ||
| Pnn50 (%) | 24.8 (16) | - | 44.6 (13.6) | - | BG (pre)/WG | ||
| LF (nu) | 50.4 (16.3) | - | 31.4 (17.2) | - | |||
| Total power | - | - | - | - | WG | ||
| HF (nu) | 49.6 (16.3) | - | 68.6 (17.2) | - | BG (pre)/WG | ||
| LH/HF ratio | 1.3 (0.9) | - | 0.59 (0.6) | - | BG (pre) | ||
| Faulkner (2013) | 24 h Vision Premier Holter Analysis System Software, (Cardiac Science, Bothell, WA). | Total Power (ln ms2) | 8.3 (0.9) | 8.0 (1) | 7.6 (0.6) | 7.6 (0.8) | - |
| HF (ln ms2) | 6.8 (1) | 6.5 (1.1) | 6 (0.8) | 6.1 (0.8) | - | ||
| LF (ln ms2) | 7 (1) | 6.7 (1.1) | 6.4 (0.5) | 6.3 (0.6) | - | ||
| SDNN (ms) | 150 (46) | 148 (57) | 108 (22) | 110 (35) | - | ||
| SDANN (ms) | 127 (37) | 127 (52) | 94 (22) | 95 (32) | - | ||
| Pnn50 (%) | 23 (15) | 19 (12) | 11 (6) | 12 (9) | - | ||
| rMSSD (ms) | 72 (37) | 62 (36) | 41 (15) | 46 (25) | - | ||
| Gutin (2000) | 10 min Schiller ECG system(Baar, Switzerland) | rMSSD (ms) | 54.3 (26.3) | Change = 6.1 (27.8) | - | - | BG |
| Hamila (2017) | 5 min (Polar S-810, PolarTM, Kempele, Finland) | Mean RR (ms) | 644 (40.6) | 670.4 (64.1) | 611 (30.5) | 621.7 (30.5) | - |
| ln rMSSD | 1.58 (0.2) | 1.78 (0.2) | 1.53 (0.19) | 1.62 (0.33) | - | ||
| HF (nu) | 24.6 (14.4) | 34.5 (15.1) | 27.02 (8.98) | 28.1 (6.46) | EG (WG) | ||
| HF (ln ms2) | 2.5 (0.5) | 2.6 (0.5) | 2.3 (0.51) | 2.37 (0.81) | - | ||
| LF (nu) | 72.2 (12.8) | 48.1 (23.9) | 71.8 (22.34) | 71.17 (19.56) | EG (WG)/BG | ||
| LF (ln ms2) | 2.9 (0.5) | 2.5 (1.3) | 2.59 (0.35) | 2.83 (0.55) | - | ||
| LF/HF | 4 (2.3) | 2.6 (1.6) | 2.81 (0.9) | 2.91 (1.28) | - | ||
| SD1 (ms) | 34.8 (10.5) | 45.7 (15.6) | 34.5 (8.16) | 35.29 (17.5) | EG (WG) | ||
| SD2 (ms) | 75.5 (32.1) | 98.21 (23.59) | 69.3 (10.5) | 77.57 (12.8) | - | ||
| Huang (2019) | 10 min SphygmoCor system (AtCor Medical, Sydney, Australia) | SDNN (ms) | 65.2 (18.98) | 88.3 (28.36) | - | - | WG |
| rMSSD (ms) | 65.8 (27.49) | 100.5 (37.68) | - | - | WG | ||
| Pnn50 (%) | 37.8 (17.05) | 57.8 (12.31) | - | - | WG | ||
| Total Power (ms2) | 4012.8 (2272.3) | 4633.7 (1978.1) | - | - | - | ||
| LF (ms2) | 1172.8 (1189.5) | 1882.8 (2465.1) | - | - | - | ||
| HF (ms2) | 1372.5 (908.8) | 1988 (983.3) | - | - | - | ||
| LF/HF | 1 (0.55) | 0.7 (0.43) | - | - | WG | ||
| Prado (2010) | 3 min 12-lead ECG (Marquette Medical Systems, CardioSoft, Wisconsin, USA) | LF (ms2) | - | - | - | - | BG/EG (WG) |
| HF (ms2) | - | - | - | - | BG/EG (WG) | ||
| LF (nu) | - | - | - | - | BG/EG (WG) | ||
| HF (nu) | - | - | - | - | BG/EG (WG) | ||
| LF/HF | - | - | - | - | BG/EG (WG) | ||
| Vasconcellos (2015) | 5 min (Polar RS800cx, PolarTM, Kempele, Finland) | LF (nu) | - | - | - | - | WG |
| HF (nu) | - | - | - | - | WG | ||
| LF/HF | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villafaina, S.; Fuentes-García, J.P.; Leon-Llamas, J.L.; Collado-Mateo, D. Physical Exercise Improves Heart-Rate Variability in Obese Children and Adolescents: A Systematic Review. Sustainability 2021, 13, 2946. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052946
Villafaina S, Fuentes-García JP, Leon-Llamas JL, Collado-Mateo D. Physical Exercise Improves Heart-Rate Variability in Obese Children and Adolescents: A Systematic Review. Sustainability. 2021; 13(5):2946. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052946
Chicago/Turabian StyleVillafaina, Santos, Juan Pedro Fuentes-García, Juan Luis Leon-Llamas, and Daniel Collado-Mateo. 2021. "Physical Exercise Improves Heart-Rate Variability in Obese Children and Adolescents: A Systematic Review" Sustainability 13, no. 5: 2946. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052946