
A Study on the Motivation of Older Adults to Participate in Exercise or Physical Fitness Activities


1
Master of Science Degree Program in Innovation for Smart Medicine, Chang Gung University, Taoyuan 33302, Taiwan
2
Department of Industrial Design, Chang Gung University, Taoyuan 33302, Taiwan
3
Graduate Institute of Business and Management, Chang Gung University, Taoyuan 33302, Taiwan
4
Department of Physical Medicine and Rehabilitation, Chang Gung Memorial Hospital, Taoyuan 33305, Taiwan
5
Department of Visual Communication Design, Ming Chi University of Technology, New Taipei City 24301, Taiwan
6
Product Design and Development Laboratory, Taoyuan 33343, Taiwan
7
Department of Industrial Design, National Taipei University of Technology, Taipei 10608, Taiwan
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(10), 6355; https://0-doi-org.brum.beds.ac.uk/10.3390/su14106355
Submission received: 5 August 2021
/
Revised: 4 May 2022
/
Accepted: 19 May 2022
/
Published: 23 May 2022
(This article belongs to the Special Issue Physical Activity, Aging, and Lifestyle Sustainability)
Abstract
:Studies have found that older adults often experience severe problems due to a lack of exercise, including an increased risk of falls, increased psychological problems and reduced social participation. However, the practicality and sustainability of exercise or physical fitness activities among older adults are questionable because these adults may face physical and psychological obstacles. Hence, this study proposed a research model to explore the physical fitness behaviours of the elderly subjects and the specific factors for maintaining their motivation to participate in exercise or physical fitness activities. A survey for a total of 101 subjects of residents of Chang Gung Health and Culture Village (CGHCV) was conducted to investigate the effects of the elderly’s group identification and psychological proximity on their attitude and intention toward physical fitness. The results show that the group identification of the physical fitness activities, psychological proximity, intention toward physical fitness and subjective norms of the subjects did not affect their attitudes towards physical fitness or their intention to participate in exercise or physical fitness activities in the future. Therefore, the influence of group identification with other older adults of the same age on empathy allowed the subjects to understand the problematic aspects of physical fitness. Group identification among the subjects allowed them to adjust to their physical fitness problems through sympathy. It mediated the physical fitness problems of the subjects through the ageism effect.
1. Introduction
The rapid ageing of the population is a global phenomenon. Active preparation for ageing is one of the biggest concerns in the 21st century. It is essential for older adults to maintain independence and autonomy for as long as possible. Studies have found that older adults often experience severe problems due to a lack of exercise, including an increased risk of falls, increased psychological problems and reduced social participation. Muscle mass and strength gradually decrease as physical functions decline in older adults. The lack of muscle endurance for exercise and physical activity can easily lead to an increased risk of body function loss and noncommunicable diseases such as obesity, diabetes and stroke [1,2]. In addition, weak physical functioning and poor quality of life are easily caused among older adults with sarcopenia [3,4]. Exercise and nutrition are effective ways to prevent and treat sarcopenia [5,6]. However, the practicality and sustainability of exercise or physical fitness activities among older adults are questionable because these adults may face physical and psychological obstacles. Several studies have shown that cognitive stimuli [7], social life, and daily functions positively affect psychology and physiology. In a current study, ageing stereotypes were shown to contribute to the iatrogenic effect of social environments that increased the dependency of older adults [8]. Anti-age discriminatory behaviour affects the views of young people towards the elderly [9].
In contrast, exploring the effects of emotions or behaviours regarding age discrimination produces empathy [10]. From the perspective of an older adult, the reduction of self-stereotyping and in-group stereotyping allows elderly individuals to sympathise with and identify with people in the same age group, which promotes mutual respect among older adults [11]. A higher tendency towards empathy is correlated with a lower degree of age discrimination [12]. Group identification enables the elderly to apply self-compassion and empathy to motivate them to participate in exercise or physical fitness activities. However, more studies are required to understand how group identification affects the psychological proximity, attitudes towards and behavioural intentions to participate in physical fitness activities and enhance the elderly population’s motivation and attitudes toward physical fitness. In addition, studies also need to investigate how to alleviate age discrimination by improving physical fitness in older adults or how to use sympathy and empathy to increase the understanding of physical fitness in older adults and support the physical fitness activities in this population. Therefore, more exploration of factors that motivate older people to participate in exercise or physical fitness activities is needed.
Health-related physical fitness refers to the maintenance of health and the improvement of the cardiopulmonary, vascular and muscular functions that are closely related to the quality of life. Promoting health-related physical fitness protects the body from chronic diseases caused by a sedentary lifestyle [13]. Health-related physical fitness in older adults is also known as functional physical fitness. It is the basic physical ability that determines whether older adults can independently perform their daily life functions. The constituent elements of functional physical fitness include muscle strength, muscle endurance, cardiopulmonary endurance, flexibility, balance, coordination, response time and body composition [14]. In short, the three components of the theory of planned behaviour (TPB)—the attitudes towards a behaviour, subjective norms, and perceived behavioural control—all affect older adults’ intention to participate in exercise or physical fitness activities [15]. In this study, the TPB is used to explore the difficulties and obstacles that older adults face for performing physical fitness activities and anticipate this population’s maintenance of physical fitness. Ajzen proposed the TPB as a means to concisely explain how people perform various behaviours under the influence of intention [16]. This study assessed older adults’ motivation to participate in exercise or physical fitness activities by surveying variables. The purpose of this study was to construct a research model to investigate the motivation of the elderly to participate in exercise or physical fitness activities and explore the relationship of these variables among older adults with similar physical fitness levels and clarify the relationships among older adults’ cognition, attitudes and physical fitness behaviours.
The rest of this paper is organised as follows. Section 2 introduces a related literature review to explore the possible constructs of the motivation of the elderly to participate in exercise or physical fitness activities. Section 3 presents the proposed model and the measures. The hypothesis results are shown in Section 4. In Section 5, we discuss the factors that affect the physical fitness of older adults. Finally, the conclusions are drawn in Section 6.
2. Hypothesis Development
First, as the basis of the research model, we review the literature regarding physical fitness, group identification, empathy, sympathy, and ageism and study whether group identification in older adults can influence their attitude toward physical fitness. Furthermore, we also examine whether intention toward physical fitness has a mediating effect on subjective norms and perceived behavioural control (see Table 1).
2.1. Physical Fitness
Physical fitness aims to increase the amount of physical activity through a healthy lifestyle and regular moderate exercise. Physical fitness in the general public has received wide attention in medicine, education and other sectors of society. The purpose of physical training is to promote wellness. A report by the U.S. Department of Health and Human Services has indicated the significance of physical fitness [42]. Because physical fitness traits include those related to good health and those that promote physical training performance and skills, physical fitness can be divided into health-related fitness and performance-related fitness. According to the American Society of Sports Medicine and the American Heart Association guidelines on physical fitness for people over 65 years of age, older adults should engage in regular physical training (at least 3 to 5 times per week), and most of these activities should enhance the functional performance required for daily activities [43,44]. In terms of activities that promote physical health in elderly individuals, aerobic exercise and muscle-strengthening activities should be emphasised. These activities enable older adults to engage in or adapt to daily dynamic life and allow them to be active in old age. The goal of older adults in pursuing physical training is not sports performance or capacity but the happiness generated by physical fitness activities and the maintenance of physical functions. Studies also indicate that the modes of physical fitness activities must meet the particular health conditions and needs of elderly individuals. Persistent engagement in physical fitness activities is conducive to healthy physical function, keeping the body in a healthy state and improving physical fitness. In addition, scholars have pointed out that older adults engage in interpersonal interactions in the community through physical training; thus, exercise or physical fitness activities promote social participation and prevent the formation of psychological barriers and social loneliness as a result of the decline in physical functions. Physical training for older adults promotes physical fitness, improves the quality of life, and reduces the state’s social health care expenses. Such benefits will increase older adults’ motivation to participate in exercise or physical fitness activities and improve the effectiveness of physical training for older adults in the community.
2.2. Group Identification
Older adults gain a sense of self-worth and social belonging from the group. Therefore, they have an incentive to make favourable comparisons between their own group and other groups [17]. Social identity depends on the sharing of common characteristics by members of an organisation (e.g., those living in the same community). The crucial influence of the group members on social behaviour creates group cohesion and social influence. Group identity also considers self-identity as a variable and a representative process within a major group [19]. Meaningful self-identity and the salience of social identity may increase people’s motivation to organise. There is a connection between the organisational status of a group and the personal self-esteem of its members. Individuals and their groups share the same significant social identity [21].
2.3. Empathy and Sympathy
Emotional reactions may produce psychological distancing or trigger altruistic behaviours (e.g., sympathy and empathy). Sympathy and empathy are the direct responses to other people’s emotions. Emotional contagion is the emotional experience in which an individual responds to other people’s sympathetic emotions. Emotional contagion is the basic manifestation of empathy [23] and can be interpreted as the frontier of empathy [24]. Emotional spreading generates empathy and sympathy [45]. When people sympathise with others, their empathy leads to altruism and appeals to the moral principle of upholding justice. Thus, people then tend to support altruistic goals related to relieving the pain or need of others [27]. Attention is a factor that generates sympathy. Sympathy for others is a key factor in deciding to help people in need. Sympathy relies on attention and other cognitive mechanisms. The interaction between attention and emotion drives the generation of guided feelings [31].
2.4. Ageism
Ageism (e.g., prejudiced attitudes towards the elderly) has a variety of manifestations, including a reduced willingness to communicate with the elderly [9]. Although the elderly are often stereotyped as incompetent but warm [32], such stereotypes raise concerns about the practical difficulties that accompany the ageing of society. However, studies have found that some of the important psychological and social needs of the elderly are met through self-expression of their values. Providing meaningful participation during retirement and promoting interaction in the community and society are vital to the well-being of elderly individuals [33]. Ageism is often unconscious. We often seek to solve problems associated with ageing through technology, an endeavour that forms the framework of research. For example, older adults will protest on the street and go out to vote. Compared with young people, the elderly present different generational patterns [34]. People’s concerns about socialisation with age and the decline in ability and performance in relation to technology use typically define ageing. Such narratives, which reflect elderly adults’ passiveness and disinterest in technology [46], eventually perpetuate age stereotypes and reveal the problem of ageism towards older adults.
2.5. Hypothetical Inference of the Effect of Group Identification on Physical Fitness in Older Adults
Erikson’s model of adult personality development suggests that the task of older adults is to accept and resolve their own lives [47,48,49]. The old-age stage is the last stage of life, and elderly individuals must show wisdom to deal with the tasks of psychosocial development. Older adults are constrained by physiological decline and differences in values and norms, and they gradually disengage from their previous social activities. They maintain group identification through their own strength and the strength of peer groups during retired life. Older adults classify themselves as a part of a specific group in a way that leads to a stronger emotional connection with that group [50]. Group identification allows an elderly individual to extend his/her self-compassion to other older adults. This transferred sympathy may reduce negative perceptions of the elderly and ageism. Sympathy is defined as the ability to experience compassion when one is negatively affected by another person’s emotions. Sympathy is the ability to apprehend another person’s emotions [45,51]. When people feel sympathy, it is easier for them to support others or help others to achieve their goals. In view of the role of sympathy and empathy in social behaviour, research has discovered the factors that drive the generation of emotion-oriented feelings [31].
We predicted that older subjects’ attitudes and motivation would translate into exercise or physical fitness activities according to their degree of group identification/social identification, their emotional feelings of sympathy and empathy and the actual impact of age discrimination. Therefore, this study hypothesised that older adults’ emotional connection and group identification are strengthened through participation in the same activities. The direct effects of group identification on factors related to empathy, sympathy and ageism were hypothesised as follows:
Hypothesis H1.
Increased group identification with other older adults of the same age occurs through participation in exercise or physical fitness activities.
Hypothesis H2a.
The group identification with older adults of the same age has an impact on empathy.
Hypothesis H2b.
The empathy effect allows elderly individuals to understand the difficult aspects of their physical fitness.
Hypothesis H3a.
Group identification allows older adults to adjust to their physical fitness problems through the sympathy effect.
Hypothesis H3b.
The sympathy effect enables older adults to actively mediate their physical fitness problems.
Hypothesis H4a.
The group identification of older adults has an impact on ageism.
Hypothesis H4b.
The effect of ageism causes elderly individuals to negatively mediate their physical fitness problems.
2.6. Theory of Planned Behavior and Physical Fitness in Older Adults
The self-connectivity and concreteness of older adults increase when their psychological distance decreases due to group identification, which further affects their sympathy, empathy and ageism. We sought to determine whether psychological proximity triggers a positive attitude towards physical fitness and an intention to support physical fitness in older adults. Age-related changes lead to changes in self-image, which lead to psychological changes in mentality [52]. Changes in the mentality of elderly adults lead to a reduced distance from self-image, which may cause them to feel an urgent need for physical fitness [53,54]. When elderly individuals form psychological proximity to physical fitness, it may serve as a powerful indicator for the elderly’s attitudes towards physical fitness and their behavioural intentions to support participation in physical training. Therefore, the hypothesised relationships were as follows.
Hypothesis H5.
There would be a positive correlation between the psychological proximity of the elderly and the elderly’s attitude towards physical fitness.
Hypothesis H6.
There would be a positive correlation between the psychological proximity towards old age and the elderly’s intention to actively participate in physical training.
Studies related to TPB suggest that there is a close relationship between the elderly’s attitudes towards physical fitness and their behavioural intentions [15,55]. A positive attitude, such as altruism, is a powerful predictor of the willingness to participate [56,57]. The preferences of the elderly for physical fitness may prompt them to participate in exercise or physical fitness activities. The hypotheses were proposed as follows.
Hypothesis H7.
The elderly’s intentions towards physical fitness was negatively correlated with the behaviour of the elderly towards participation in physical training.
The intention of humans to participate in social activities is the precursor to behaviour. According to the TPB proposed by Ajzen [16], intentions are governed by three concepts: attitude, subjective norms, and perceived behavioural control. The more favourable the attitudes and subjective norms, the stronger the behaviour control, and the stronger the individual’s intention to perform specific behaviours. The attitude towards physical fitness is defined as the overall evaluation of the physical fitness behaviours. The subjective norm is a person’s own assessment of the social pressure to perform or not to perform a targeted behaviour. The behavioural stress faced during performing physical fitness activities is measured. Perceived behavioural control is a person’s perception of his/her ability to perform a given behaviour. This aspect will measure the degree to which physical fitness is implemented by the elderly. According to physical fitness activity, every constructive part of the TPB is transformed into a variable that can be analysed and measured. Therefore, the hypothetical relationships were as follows.
Hypothesis H8.
The elderly’s attitude towards physical fitness was positively correlated with their intention to participate in exercise or physical fitness activities.
Hypothesis H9a.
Subjective norm was positively correlated with the elderly’s intention to participate in exercise or physical fitness activities.
Hypothesis H9b.
Subjective norm was positively correlated with the elderly’s attitude towards participation in exercise or physical fitness activities.
Hypothesis H10.
Perceived behavioural control was positively correlated with the elderly’s willingness to participate in exercise or physical fitness activities.
Hypothesis H11.
Perceived behavioural control was positively correlated with the elderly’s behaviour of participating in exercise or physical fitness activities.
Regarding the relationship and differences between physical activity and health status, the health status of individuals who exercise regularly is better than that of those who are unhealthy [58]. Information on physical activity patterns shows that the level of physical activity declines sharply as age increases. Therefore, the following relationships were hypothesised.
Hypothesis H12.
Gender has an interfering effect on elderly individuals’ participation in physical training and on their physical training behaviour.
3. Research Methods
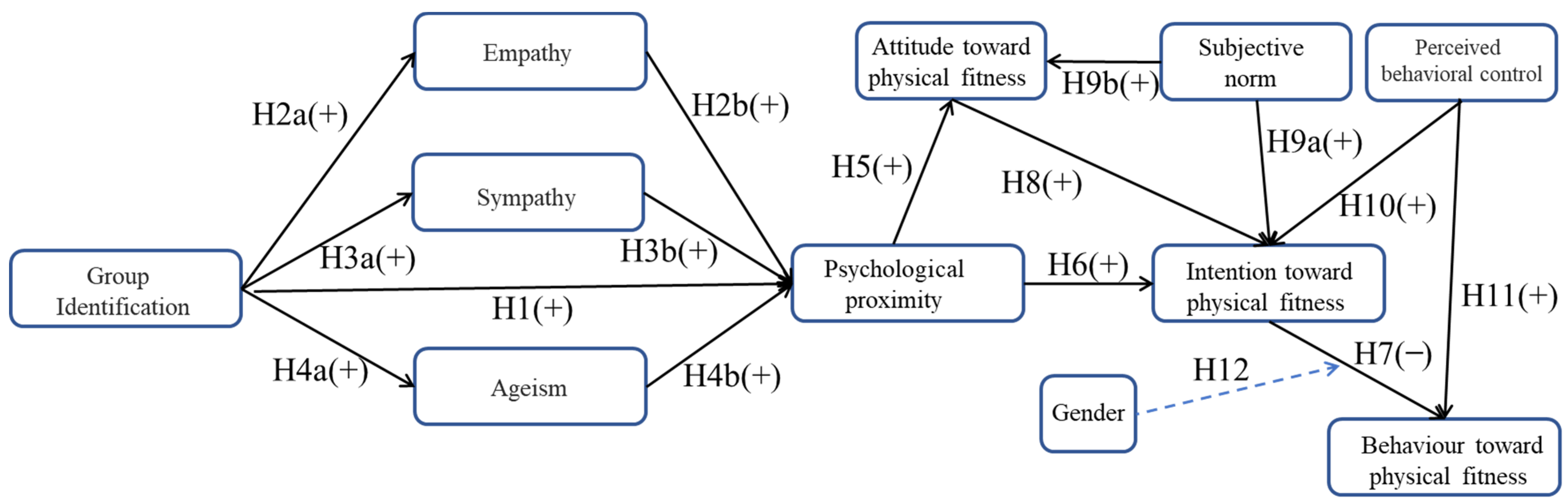
The research method employed in this study involved the construction of a structural equation model that allowed the understanding of the relationships of behavioural intentions to participate in physical training with psychological continuity, group identification, empathy, sympathy, ageism, psychological proximity, and physical fitness attitudes in older adults (see Figure 1). The proposed model is based on the TPB and was further used to explore the physical fitness behaviours of the elderly participants and the specific factors for maintaining their motivation to participate in physical fitness activities. In this study, a semi-structured questionnaire was designed to collect data (see Appendix A). The questionnaire used a Likert 5-point scale for responses. A total of 101 subjects aged 50 years and older residing at Chang Gung Health and Culture Village (CGHCV) were randomly recruited (see Figure 2). Table 2 shows the descriptive statistics of the sample. The study protocol was approved by the Institutional Review Board of Chang Gung Hospital, Taoyuan, Taiwan (approval number: 201700360B0C502). The subjects participated voluntarily and written informed consents were obtained from all subjects.
Measurement Model
In partial least squares structural equation modeling (PLS-SEM), the reflective measurement model was assessed in terms of internal consistency (i.e., reliability), convergent validity and discriminative validity. In terms of internal consistency, the Smart PLS software provided composite reliability metrics. Research literature shows that Cronbach’s alpha can be used as a complementary indicator. Convergent validity was established through average variance extracted (AVE) values (AVE > 0.5) and outer loading (see Table 3). All facets had AVE values greater than 0.5, which confirmed the convergent validity. The validity was confirmed by verifying the AVE and cross loading [59,60]. In terms of internal consistency, all facet measures were very reliable according to Cronbach’s alpha for ageism (5 terms; α = 0.788). Internal consistency measurements are provided in Table 4, as suggested by Chin [61].
4. Results
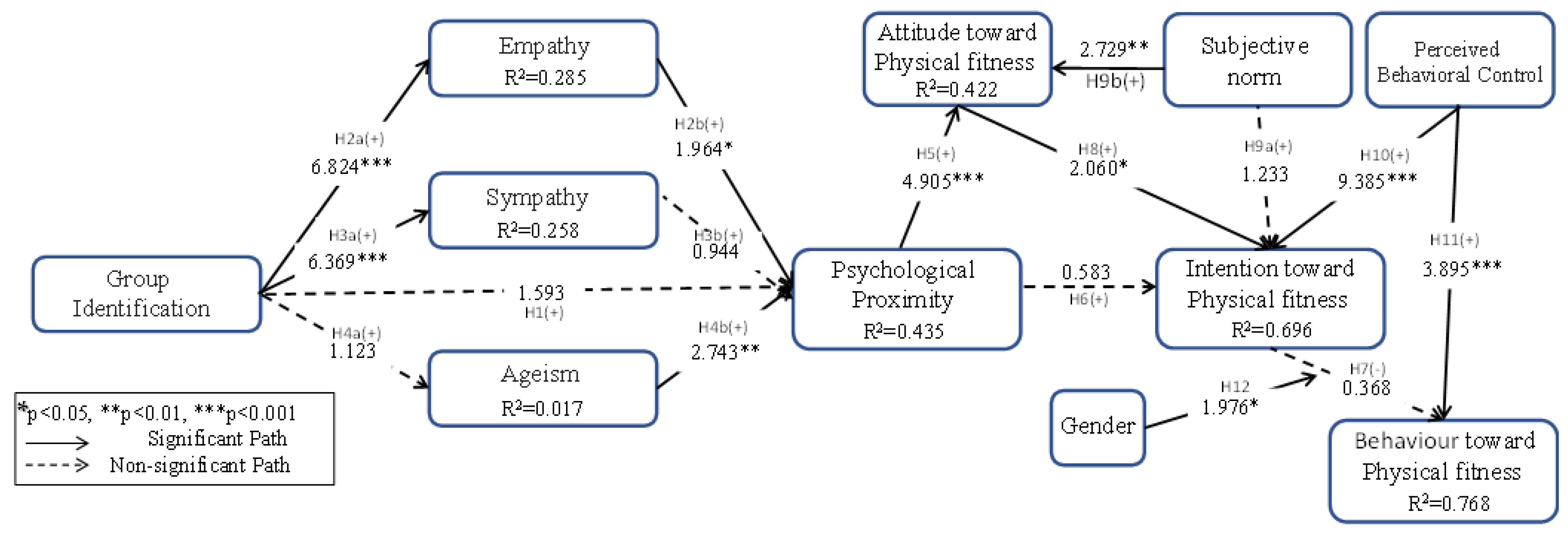
In the PLS-SEM path analysis, bootstrapping was performed with 5000 resamples to automatically compute t statistics (|O/STERR|), standard deviation and standard error, thereby estimating the significance of the hypothetical relationships among facets [61,65]. The statistical measure R2 refers to the proportion of variation explained by related latent variables. Figure 3 used R2 to intuitively summarise the conceptual model, path coefficient and significance level. The results of the structural model analysis are shown in Table 5. There were significant relationships between group identity (GI) and empathy (EM), between EM and psychological proximity (HA), between GI and sympathy (SY), and between ageism (AD) and HA (H4b β = 0.266, p < 0.01). Significant relationships also existed between HA and attitude towards physical fitness (EA), between EA and physical fitness intentions (EI), between subjective norms (SJ) and EA, between perceived behaviour control (PA) and EI, and between PA and physical fitness behaviours (EH). Gender had mediating effects on EI and EH.
5. Discussion
The current study investigated the factors that affect the physical fitness of older adults. In this study, PLS-SEM analysis of the samples showed that group identification affected the sympathy, empathy and ageism towards physical fitness in older adults’ attitudes and intentions. The novelty of this study performed, for the first time, an empirical test of the effects of the general social perspective of ageism on older adults’ attitudes and intentions towards physical fitness, thereby elucidating the impact of physical fitness on the daily lives of the elderly. This study has several theoretical and practical implications. First, it showed the value of prompting older adults to acknowledge the difficulties and emotions they might encounter through the influence of psychological mechanisms (sympathy and empathy) and ageism. Psychological connection and proximity trigger strong emotions about the future in the subjects, which then affected their perception and group identification. In this study, the average age of the subjects was 78.81 years. The subjects’ passiveness and disinterest in technology and the effects of physiological ageing demonstrated the ageism issues. The study showed that subjects would not form a group identity with their peers when participating in physical fitness activities. In addition, the subjects were unable to mitigate their physical fitness problems. The group identification of the subjects did not affect ageism. Attitudes, subjective norms and perceived behavioural control, which affect the physical fitness behaviour of the subjects, also affected their intention to participate in physical fitness activities. The psychological proximity of the subjects was not correlated with their intention to actively participate in physical fitness activities, and their intentions regarding physical fitness were also not correlated with their behaviour of participating in physical fitness activities. Subjective norms were not correlated with the subjects’ attitudes towards participation in physical fitness activities. The group identification of the physical fitness activities, psychological proximity, intention toward physical fitness and subjective norms of the subjects did not affect their attitudes towards physical fitness or their intention to participate in physical fitness activities in the future. Therefore, the influence of group identification with other older adults of the same age on empathy allowed the subjects to understand the problematic aspects of physical fitness. Group identification among the subjects allowed them to adjust to their physical fitness problems through sympathy. It mediated the physical fitness problems of the subjects through the ageism effect. In addition, this study attempted to extend the model to show that there were significant correlations between the psychological proximity of the subjects and their attitudes and intentions towards physical fitness, between the subjective norms and the subjects’ attitudes towards participation in physical fitness activities, and between perceived behavioural control and the subjects’ intentions and behaviour toward physical fitness. Such correlations affected the relationship between the subjects’ group identification to perform physical fitness activities either directly or through attitude.
5.1. Theoretical Contribution
In this study, three broad perspectives were adopted: (1) physical fitness is an essential factor in the daily life of older adults; (2) older adults’ intentions to engage in physical fitness and their physical fitness activities had a significant effect on their psychological functions (sympathy and empathy) and ageism; and (3) physical fitness intentions and behaviours were planned behaviours. In terms of the first point of view, people use various social and gaming application programs to encourage themselves and others to maintain exercise habits. Studies have questioned how social influence predicts attitudes towards exercise, behaviours and future exercise [66]. The results of this study showed that older adults had positive recognition and reciprocity of exercise or physical fitness intentions and attitudes due to the impact of group identification. Older adults believe that physical fitness should be a daily requirement rather than a factor required for training or short-term exercise. In addition, this study found that older adults’ desire for physical fitness tended to focus on factors necessary for life rather than on the short-term results of short training.
Second, group identification forms the relationships between psychological proximity, attitudes and behavioural intentions through the positive mediation of sympathy, empathy and ageism. The psychological continuity formed through vivid images of a person’s future self may lead to group identification among older adults and affect their psychological proximity [22]. This study found that group identification had a significant effect on empathy. However, empathy failed to affect the psychological proximity of the elderly, which was different from previous studies. Ageism is another factor of variation. Group identification did not cause age discrimination, whereas ageism affected the psychological proximity of physical fitness. The results show that older adults aim to pursue a pleasant and healthy life, and their levels of vanity and the intention to compete were relatively weak. Older adults believe they can make the final life journey more enjoyable through physical fitness. In addition, older adults’ unique needs for life, rendered through physical fitness, are a key predictive factor for sympathy, empathy, and ageism.
Third, physical fitness activity in older adults is the result of planned behaviour. The TPB model has been used to determine the specific factors that are most conducive to and predictive of actual exercise behaviour and the main predictive index of exercise intention. The TPB model determines and predicts exercise maintenance in sarcopenic elderly patients [37]. This study found that because the age of the subjects was mainly between 70 and 89 years (approximately 80.2%), age had no significant effect on subjective norms for physical fitness. In addition, the subjects’ personal behaviour was mainly predicted by behavioural intentions. The intentions to engage in physical fitness had no significant effect on increasing social identification or gaining health. Therefore, for the subjects, physical fitness activity was a planned, rational behaviour. It was not affected by subjective norms or the will of others. In addition, the interference effect of gender on the relationship between physical fitness intention and behaviour was significant.
The older adults’ intentions and behaviour regarding physical fitness were not precisely the same as their general attitude towards sports. The physical fitness behaviour of older adults is a social process involving interactions between psychological functions (sympathy and empathy) and ageism. The subjects were influenced by subjective norms and intentions to participate in physical fitness activities; they did not care about increasing their social recognition or gaining health.
5.2. Limitations and Future Studies
This was essentially an exploratory study. The study attempted to examine the effects of physical fitness intentions and behaviours among older adults for use as an aid to encourage older adults to participate in physical fitness activities or to make adjustments to their fitness activities. In addition, the study attempted to examine the potential mechanisms underlying these effects. The results of the path analysis supported the proposed relationships. However, this study was limited in terms of examining the elderly subjects’ attitudes towards physical fitness, given that the fundamental purpose of the study was to examine their attitudes and behavioural intention. Future studies may investigate the factors underlying the long-term effects on the subjects’ use of future-related technologies and determine ways to experience the plight of the elderly through real experience.
Future studies may focus on the specific factors, such as socioeconomic factors (age, gender or having a partner), involved in the effect of ageism on group identification among older adults. Age and gender differences may produce different results regarding empathy and sympathy. Ageism manifests as different emotional responses or intensities of response towards age-related changes. Different degrees of emotional sensitivity and empathy lead to changes in people’s views, attitudes and behaviours regarding the elderly. Gender may also be an influencing factor. The testing of such factors will expand the scope of research.
Another limitation of this study was the age of the subjects [37,67]. The majority of older adults have specific misunderstandings about physical fitness activities and exercise, which renders them physically inactive. In this study, the attitude was a key factor affecting exercise behaviour. However, the specific factors that affect exercise vary among populations and regions. Attitudes, subjective norms and perceived behavioural control are all conducive to exercise. Because most of the subjects could no longer perform strenuous exercise due to various restrictions, the effects of old age on actual exercise behavioural intention and perceived behavioural control showed an increasing trend. The effect of subjective norms on intention was significantly enhanced. Family support, the main factor affecting the subjects’ intention to exercise was somewhat decreased. In community-based interventions, the support of family members and important people (such as best friends) is an important factor in ensuring that older adults exercise regularly. Furthermore, the lack of randomisation in subject selection might be a limitation.
Additionally, the sample size of this study was relatively small, and there was also a difference in the number of males and females. Finally, the respondents were mainly older adults living in the elderly residential area of CGHCV in Taiwan. Future studies should consider randomisation and should include other ethnic groups, cultures and geographical locations.
6. Conclusions
When older adults experience vivid self-images as they age, exercise or physical fitness activities can be an individual or group activity. Physical fitness activity allows a person to identify with people his/her own age and choose activities that suit him/herself. Group identification allows elderly individuals to convey their self-compassion to other elderly adults, enhancing motivation to participate in physical fitness activities. Group identification has a significant impact on sympathy and empathy. However, in terms of ageism in relation to the general conception, it is found that modern older adults have a healthier concept of physical fitness. This concept was not affected by external discrimination. In addition, this research found that intentions to exercise affected the attitude towards physical fitness and significantly affected perceived behavioural control and subjective norms. However, exercise behaviour was not affected. We hope that the findings of this study can help researchers better understand how to motivate the older adults’ attitude toward physical fitness to increase their intention towards physical fitness further or participate in exercise or physical fitness.
Author Contributions
Conceptualization, T.-H.T. and K.C.T.; Data curation, H.-F.L. and T.-H.T.; Formal analysis, T.-H.T.; Funding acquisition, A.M.W. and K.C.T.; Investigation, T.-H.T. and K.C.T.; Methodology, T.-H.T. and K.C.T.; Project administration, T.-H.T.; Resources, A.M.W. and K.C.T.; Software, H.-F.L. and T.-H.T.; Supervision, T.-H.T., A.M.W. and K.C.T.; Writing—original draft, T.-H.T., H.-F.L. and K.C.T.; Writing—review & editing, T.-H.T. and K.C.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministry of Science and Technology, Taiwan (MOST 109-2410-H-027-003-MY2), Ministry of Science and Technology, Taiwan (MOST 108-2410-H-027-024-MY3), Chang Gung Medical Foundation (CMRPD2F0213), Chang Gung Medical Foundation (CMRPG5J0043), Chang Gung University (EMRPD1K0391), Chang Gung University (EMRPD1K0481). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
The study protocol was approved by the Institutional Review Board of Chang Gung Hospital, Taoyuan, Taiwan (approval number: 201700360B0C502).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Questionnaire
| Construct | Question |
|---|---|
| Group identification |
|
| Empathy |
|
| Sympathy |
|
| Ageism |
|
| Attitude toward physical fitness |
|
| Subjective norms |
|
| Perceived behavioural control |
|
| Intention toward physical fitness |
|
References
- Garland, T., Jr.; Schutz, H.; Chappell, M.A.; Keeney, B.K.; Meek, T.H.; Copes, L.E.; Acosta, W.; Drenowatz, C.; Maciel, R.C.; van Dijk, G.; et al. The biological control of voluntary exercise, spontaneous physical activity and daily energy expenditure in relation to obesity: Human and rodent perspectives. J. Exp. Biol. 2011, 214, 206–229. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [Green Version]
- Lima, R.M.; Bezerra, L.M.A.; Rabelo, H.T.; Silva, M.A.F.; Silva, A.J.R.; Bottaro, M.; de Oliveira, R.J. Fat-free mass, strength, and sarcopenia are related to bone mineral density in older women. J. Clin. Densitom. 2009, 12, 35–41. [Google Scholar] [CrossRef]
- Bunce, S.; Schroeder, K. Interventions for sarcopenia and muscle weakness in older people. Age Ageing 2005, 34, 414–415. [Google Scholar] [CrossRef] [Green Version]
- Lang, T.; Streeper, T.; Cawthon, P.; Baldwin, K.; Taaffe, D.R.; Harris, T.B. Sarcopenia: Etiology, clinical consequences, intervention, and assessment. Osteoporos Int. 2010, 21, 543–559. [Google Scholar] [CrossRef] [Green Version]
- Vernooij-Dassen, M.; Vasse, E.; Zuidema, S.; Cohen-Mansfield, J.; Moyle, W. Psychosocial interventions for dementia patients in long-term care. Int. Psychogeriatr. 2010, 22, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Coudin, G.; Alexopoulos, T. ‘Help me! I’m old!’ How negative aging stereotypes create dependency among older adults. Aging Ment. Health 2010, 14, 516–523. [Google Scholar] [CrossRef]
- Harwood, J.; Joyce, N.; Chen, C.-Y.; Paolini, S.; Xiang, J.; Rubin, M. Effects of past and present intergroup communication on perceived fit of an outgroup member and desire for future intergroup contact. Commun. Res. 2017, 44, 530–555. [Google Scholar] [CrossRef]
- Allan, L.J.; Johnson, J.A.; Emerson, S.D. The role of individual difference variables in ageism. Personal. Individ. Differ. 2014, 59, 32–37. [Google Scholar] [CrossRef]
- Galinsky, A.D.; Moskowitz, G.B. Perspective-taking: Decreasing stereotype expression, stereotype accessibility, and in-group favoritism. J. Personal. Soc. Psychol. 2000, 78, 708–724. [Google Scholar] [CrossRef]
- Boudjemad, V.; Gana, K. Ageism: Adaptation of the Fraboni of Ageism Scale-Revised to the French language and testing the effects of empathy, social dominance orientation and dogmatism on ageism. Can. J. Aging 2009, 28, 371–389. [Google Scholar] [CrossRef]
- U.S. Department of Education. Research Digest Toward a Uniform Definition of Wellness: A Commentary. Pres. Counc. Phys. Fit. Sports Res. Dig. 2001, 3, 213. [Google Scholar]
- Brill, P.A.; Brill, P. Functional Fitness for Older Adults, 1st ed.; Human Kinetics, Inc.: Champaign, IL, USA, 2004; p. 144. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action Control: From Cognition to Behavior; Kuhl, J., Beckmann, J., Eds.; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Tajfel, H.; Turner, J.C. The Social Identity Theory of Intergroup Behavior; Psychology Press: New York, NY, USA, 2004; pp. 276–293. [Google Scholar]
- Hornsey, M.J. Social identity theory and self-categorization theory: A historical review. Soc. Personal. Psychol. Compass 2008, 2, 204–222. [Google Scholar] [CrossRef]
- Turner, J.C.; Hogg, M.A.; Oakes, P.J.; Reicher, S.D.; Wetherell, M.S. Rediscovering the Social Group: A Self-Categorization Theory, 1st ed.; Basil Blackwell: Cambridge, MA, USA, 1987; p. 239. [Google Scholar]
- Derks, B.; van Laar, C.; Ellemers, N. Working for the self or working for the group: How self- versus group affirmation affects collective behavior in low-status groups. J. Personal. Soc. Psychol. 2009, 96, 183–202. [Google Scholar] [CrossRef] [Green Version]
- James, K.; Greenberg, J. In-group salience, intergroup comparison, and individual performance and self-esteem. Personal. Soc. Psychol. Bull. 1989, 15, 604–616. [Google Scholar] [CrossRef]
- Lee, A.R. Psychological proximity to issues of the elderly: The role of age-morphing technology in campaigns for the elderly. Comput. Hum. Behav. 2017, 69, 311–323. [Google Scholar] [CrossRef]
- Darwall, S. Empathy, sympathy, care. Philos. Stud. Int. J. Philos. Anal. Tradit. 1998, 89, 261–282. [Google Scholar]
- Harman, G. The nonexistence of character traits. Proc. Aristot. Soc. 2000, 100, 223–226. [Google Scholar] [CrossRef]
- Hogan, R. Development of an empathy scale. J. Consult. Clin. Psychol. 1969, 33, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Strayer, J. Empathy in conduct-disordered and comparison youth. Dev. Psychol. 1996, 32, 988–998. [Google Scholar] [CrossRef]
- Batson, C.D.; Klein, T.R.; Highberger, L.; Shaw, L.L. Immorality from empathy-induced altruism: When compassion and justice conflict. J. Personal. Soc. Psychol. 1995, 68, 1042–1054. [Google Scholar] [CrossRef]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Personal. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Escalas, J.E.; Stern, B.B. Sympathy and empathy: Emotional responses to advertising dramas. J. Consum. Res. 2003, 29, 566–578. [Google Scholar] [CrossRef]
- Eisenberg, N.; Strayer, J. Critical issues in the study of empathy. In Empathy and Its Development; Cambridge Studies in Social and Emotional Development; Cambridge University Press: New York, NY, USA, 1987; pp. 3–13. [Google Scholar]
- Dickert, S.; Slovic, P. Attentional mechanisms in the generation of sympathy. Judgm. Decis. Mak. 2009, 4, 297–306. [Google Scholar]
- Cuddy, A.J.C.; Fiske, S.T. Doddering but dear: Process, content, and function in stereotyping of older persons. In Ageism: Stereotyping and Prejudice Against Older Persons; The MIT Press: Cambridge, MA, USA, 2002; pp. 3–26. [Google Scholar]
- Brewer, R.; Piper, A.M. “Tell It like It really is”: A case of online content creation and sharing among older adult bloggers. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 5529–5542. [Google Scholar]
- Zukin, C.; Keeter, S.; Andolina, M.; Jenkins, K.; Carpini, M.X.D. A New Engagement?: Political Participation, Civic Life, and the Changing American Citizen; Oxford University Press: New York, NY, USA, 2006; p. 253. [Google Scholar]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Rise, J.; Thompson, M.; Verplanken, B. Measuring implementation intentions in the context of the theory of planned behavior. Scand. J. Psychol. 2003, 44, 87–95. [Google Scholar] [CrossRef]
- Ahmad, M.H.; Shahar, S.; Teng, N.I.; Manaf, Z.A.; Sakian, N.I.; Omar, B. Applying theory of planned behavior to predict exercise maintenance in sarcopenic elderly. Clin. Interv. Aging 2014, 9, 1551–1561. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.; Choi, S.; Kim, S.; Yeh, Y.-H. Factors affecting advertising avoidance on online video sites. Korean J. Advert. 2013, 2, 87–121. [Google Scholar] [CrossRef]
- Hartmann, C.; Dohle, S.; Siegrist, M. A self-determination theory approach to adults’ healthy body weight motivation: A longitudinal study focussing on food choices and recreational physical activity. Psychol. Health 2015, 30, 924–948. [Google Scholar] [CrossRef] [PubMed]
- Schüler, J.; Wegner, M.; Knechtle, B. Implicit motives and basic need satisfaction in extreme endurance sports. J. Sport Exerc. Psychol. 2014, 36, 293–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, C.J.; Norman, P.; Conner, M. Can the Theory of Planned Behaviour mediate the effects of age, gender and multidimensional health locus of control? Br. J. Health Psychol. 2002, 7, 299–316. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Physical Activity and Health: A Report of the Surgeon General; DIANE Publishing: Darby, PA, USA, 1996; p. 278.
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Maibom, H.L. Feeling for others: Empathy, sympathy, and morality. Inquiry 2009, 52, 483–499. [Google Scholar] [CrossRef]
- Vines, J.; Pritchard, G.; Wright, P.; Olivier, P.; Brittain, K. An age-old problem: Examining the discourses of ageing in HCI and strategies for future research. ACM Trans. Comput.-Hum. Interact. 2015, 22, 2. [Google Scholar] [CrossRef]
- Erikson, E.H. Identity and the life cycle: Selected papers. Psychol. Issues 1959, 1, 1–171. [Google Scholar]
- Erikson, E.H.; Erikson, J.M. The Life Cycle Completed (Extended Version); W. W. Norton & Company: New York, NY, USA, 1998; p. 144. [Google Scholar]
- Erikson, E.H.; Erikson, J.M.; Kivnick, H.Q. Vital Involvement in Old Age; W W Norton & Co: New York, NY, USA, 1989; p. 352. [Google Scholar]
- Haslam, S.A.; Oakes, P.J.; Reynolds, K.J.; Turner, J.C. Social identity salience and the emergence of stereotype consensus. Personal. Soc. Psychol. Bull. 1999, 25, 809–818. [Google Scholar] [CrossRef]
- Gruen, R.J.; Mendelsohn, G. Emotional responses to affective displays in others: The distinction between empathy and sympathy. J. Personal. Soc. Psychol. 1986, 51, 609–614. [Google Scholar] [CrossRef]
- Fujita, K.; Trope, Y.; Liberman, N.; Levin-Sagi, M. Construal levels and self-control. J. Personal. Soc. Psychol. 2006, 90, 351–367. [Google Scholar] [CrossRef] [PubMed]
- Liberman, N.; Trope, Y. The psychology of transcending the here and now. Science 2008, 322, 1201–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trope, Y.; Liberman, N. Construal-level theory of psychological distance. Psychol. Rev. 2010, 117, 440–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajzen, I.; Fishbein, M. Attitude-behavior relations: A theoretical analysis and review of empirical research. Psychol. Bull. 1977, 84, 888–918. [Google Scholar] [CrossRef]
- Greenslade, J.H.; White, K.M. The prediction of above-average participation in volunteerism: A test of the theory of planned behavior and the volunteers functions inventory in older Australian adults. J. Soc. Psychol. 2005, 145, 155–172. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.R.; McSweeney, A. Charitable giving: The effectiveness of a revised theory of planned behaviour model in predicting donating intentions and behaviour. J. Community Appl. Soc. Psychol. 2007, 17, 363–386. [Google Scholar] [CrossRef]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical Activity and Public Health: A Recommendation From the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Ringle, C.M.; Mena, J.A. An assessment of the use of partial least squares structural equation modeling in marketing research. J. Acad. Mark. Sci. 2012, 40, 414–433. [Google Scholar] [CrossRef]
- Lowry, P.B.; Gaskin, J. Partial least squares (PLS) structural equation modeling (SEM) for building and testing behavioral causal theory: When to choose it and how to use it. IEEE Trans. Prof. Commun. 2014, 57, 123–146. [Google Scholar] [CrossRef]
- Chin, W.W. How to write up and report PLS analyses. In Handbook of Partial Least Squares: Concepts, Methods and Applications; Esposito Vinzi, V., Chin, W.W., Henseler, J., Wang, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 655–690. [Google Scholar]
- Venkatesh, V.; Bala, H. Technology Acceptance Model 3 and a research agenda on interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Yi, M.Y.; Hwang, Y. Predicting the use of web-based information systems: Self-efficacy, enjoyment, learning goal orientation, and the technology acceptance model. Int. J. Hum.-Comput. Stud. 2003, 59, 431–449. [Google Scholar] [CrossRef]
- Roca, J.C.; García, J.J.; Vega, J.J.d.l. The importance of perceived trust, security and privacy in online trading systems. Inf. Manag. Comput. Secur. 2009, 17, 96–113. [Google Scholar] [CrossRef]
- Wong, K. Partial least square structural equation modeling (PLS-SEM) techniques using SmartPLS. Mark. Bull. 2013, 24, 1–32. [Google Scholar]
- Hamari, J.; Koivisto, J. “Working out for likes”: An empirical study on social influence in exercise gamification. Comput. Hum. Behav. 2015, 50, 333–347. [Google Scholar] [CrossRef]
- Foley, A.; Hillier, S.; Barnard, R. Effectiveness of once-weekly gym-based exercise programmes for older adults post discharge from day rehabilitation: A randomised controlled trial. Br. J. Sports Med. 2011, 45, 978–986. [Google Scholar] [CrossRef]
Figure 1.
Model framework.

Figure 2.
Subject selection process.

Figure 3.
Structural model adoption with path coefficients.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Construct definition.
| Construct | Definition and Operations | Source of Inquiry |
|---|---|---|
| Group identification | Self-categorisation and social recognition theories propose that people have different selves and display different identities based on circumstances and representation [17]. When people focus on social identity, they consider themselves to be members of certain groups and tend to view their group more favourably than they view other groups [18,19]. When an older adult experiences a vivid self-image during ageing, this image of him/herself as elderly may increase the emotional attachment to other older adults who are the same age and have similar physical functions [20,21]. At CGHCV, physical fitness activities can be either individual or group activities. Physical fitness activities allow individuals to identify with people their own age. As a result, individuals can choose the activities that suit them best and enjoy exercising. Moreover, individuals may enjoy having companions of the same age during these activities. Group identification allows the older adult to convey compassion towards other older adults and enhances their motivation to participate in physical fitness activities. | [22] |
| Empathy | Emotional contagion is the essential manifestation of empathy [23] and can be interpreted as the frontier of empathy [24]. Empathy has both cognitive and emotional components. It is the ability to apprehend the emotions of others [25] and to acknowledge and experience the feelings of others [26,27]. At CGHCV, empathy is the perception of the cognitive and emotional dimensions of other people that elderly participants experience when they engage in exercise or physical fitness activities [28]. The identity of older adults as members of a robust social community may prompt others to understand and share the physical and functional challenges of the elderly, thus inducing altruistic behaviour. | [29] |
| Sympathy | Sympathy emphasises the consistency between the emotional state of a person and the emotional state of the target. Sympathy does not require the emotional response to be the same. On the contrary, sympathy includes evaluating one’s feelings about the emotional state of another person (as in [30]). Sympathy relies on attention and other cognitive mechanisms. The interaction between attention and emotion drives the generation of guided feelings [31]. We intended to explore the effect of the emotional proximity of older adults’ empathy on cognition and problem solving during the fitness activities and to approach behaviour-intention issues with a sympathetic attitude. | [29] |
| Ageism | Discrimination is the result of stereotyping. It describes any basic attitudes and structural bias that acts against the members of a specific group [9]. This bias leads to various positive and negative evaluations. Stereotypes have produced conflicting results [32]. Studies have found that some of the important psychological and social needs of the elderly are met through self-expression of their values. Providing meaningful participation during retirement and promoting interaction in the community and society are vital to the well-being of elderly individuals [33,34]. This study aimed to explore misunderstandings about older adults caused by stereotyping and correct impressions regarding the physical fitness of the elderly. Such misunderstandings include the following: older adults cannot participate in physical training; older adults are rather stingy with money; older adults are unwilling to pay for physical training. | [22] |
| Attitude toward physical fitness | Cognitive behavioural control is the only component directly interacting with intentions and actual behaviours [35,36]. Older adults may face physical, psychological, and demographic barriers to participation in exercise or physical fitness activities. Cognitive behavioural control is widely used to promote the understanding of certain health behaviours. This study explored the physical and psychological barriers that older adults face when performing physical fitness activities with the aim of encouraging them to maintain physical fitness activities. | [37] |
| Subjective norms | Subjective norms are factors that influence an individual’s behaviour, such as the effect of the behaviours of relatives and friends on the behaviours of an individual and the tendency to copy the behaviours of relatives and friends [38]. Regular physical fitness habits or the involvement of family members will affect the sustainability of physical fitness. This study explores the impact of such factors on the physical fitness of older adults. | [37] |
| Perceived behavioural control | Perceived behavioural control is the extent to which an individual perceives him/herself to be able to perform a particular behaviour. It can be divided into the following aspects: the degree of control an individual has over behaviour and whether or not an individual can perform the behaviour. Older adults are concerned about whether they can access the necessary resources and opportunities when participating in physical fitness activities. Such access will better able older adults to engage in physical fitness activities. | [37] |
| Intention toward physical fitness | Studies have found that intention predicts motivational behaviour regarding physical training [39,40]. Behavioural intention is considered a key variable in behaviour that affects the likelihood of a person engaging in behaviour being able to complete the behaviour [41]. When older adults believe they are able to obtain opportunities to participate in physical fitness activities, their personal behaviour is mainly predicted by behavioural intention. This study examines whether the intention to participate in physical fitness activities can increase social identification or achieve health goals. | [37] |
Table 2.
Descriptive statistics of respondents.
| Variables | Subgroup | N (%) |
|---|---|---|
| Total | - | 101 (100.0) |
| Gender | Male | 25 (24.8) |
| Female | 76 (75.2) | |
| 50–59 | 2 (2.0) | |
| Age | 60–69 | 8 (7.9) |
| 70–79 | 43 (42.6) | |
| (Mean = 78.81 years) | 80–89 | 38 (37.6) |
| 90–99 | 8 (7.9) | |
| ≥100 | 2 (2.0) | |
| Graduate level | 10 (9.9) | |
| Education | University (4 years) | 44 (43.6) |
| High school | 30 (29.7) | |
| Junior high school | 10 (9.9) | |
| <Junior high school | 7 (6.9) |
Table 3.
Outer loadings and cross-loadings.
| Construct | AD | EA | EH | EI | EM | GI | HA | PA | SJ | SY |
|---|---|---|---|---|---|---|---|---|---|---|
| AD1 | 0.735 | 0.451 | 0.067 | 0.217 | 0.182 | 0.012 | 0.349 | 0.098 | 0.192 | 0.291 |
| AD2 | 0.818 | 0.510 | 0.102 | 0.234 | 0.273 | 0.207 | 0.390 | 0.149 | 0.283 | 0.431 |
| AD3 | 0.685 | 0.373 | 0.040 | 0.181 | 0.198 | 0.020 | 0.243 | −0.034 | 0.139 | 0.310 |
| AD4 | 0.716 | 0.172 | 0.063 | 0.187 | 0.310 | 0.118 | 0.326 | 0.083 | 0.312 | 0.337 |
| AD5 | 0.710 | 0.164 | 0.022 | 0.189 | 0.211 | 0.062 | 0.284 | 0.070 | 0.165 | 0.312 |
| EA1 | 0.535 | 0.847 | 0.129 | 0.332 | 0.473 | 0.272 | 0.492 | 0.165 | 0.522 | 0.476 |
| EA2 | 0.162 | 0.708 | 0.523 | 0.595 | 0.220 | 0.521 | 0.497 | 0.595 | 0.136 | 0.345 |
| EA3 | 0.454 | 0.874 | 0.145 | 0.321 | 0.408 | 0.235 | 0.478 | 0.190 | 0.437 | 0.442 |
| EH1 | 0.147 | 0.213 | 0.844 | 0.694 | 0.298 | 0.386 | 0.167 | 0.593 | 0.236 | 0.335 |
| EH2 | 0.034 | 0.385 | 0.900 | 0.798 | 0.245 | 0.405 | 0.301 | 0.782 | 0.134 | 0.239 |
| EH3 | 0.061 | 0.311 | 0.950 | 0.765 | 0.282 | 0.395 | 0.245 | 0.792 | 0.126 | 0.338 |
| EI1 | 0.267 | 0.584 | 0.744 | 0.931 | 0.447 | 0.520 | 0.468 | 0.794 | 0.273 | 0.560 |
| EI2 | 0.338 | 0.319 | 0.648 | 0.812 | 0.329 | 0.327 | 0.289 | 0.498 | 0.299 | 0.436 |
| EI3 | 0.171 | 0.476 | 0.846 | 0.937 | 0.381 | 0.497 | 0.382 | 0.811 | 0.235 | 0.436 |
| EM1 | 0.278 | 0.479 | 0.353 | 0.488 | 0.765 | 0.446 | 0.450 | 0.363 | 0.483 | 0.594 |
| EM2 | 0.308 | 0.384 | 0.122 | 0.265 | 0.876 | 0.502 | 0.436 | 0.134 | 0.648 | 0.597 |
| EM3 | 0.299 | 0.302 | 0.241 | 0.324 | 0.896 | 0.406 | 0.549 | 0.276 | 0.496 | 0.651 |
| EM4 | 0.233 | 0.379 | 0.299 | 0.392 | 0.916 | 0.519 | 0.462 | 0.316 | 0.569 | 0.699 |
| EM5 | 0.300 | 0.423 | 0.315 | 0.427 | 0.908 | 0.459 | 0.563 | 0.310 | 0.575 | 0.714 |
| GI1 | 0.139 | 0.357 | 0.365 | 0.441 | 0.524 | 0.853 | 0.418 | 0.410 | 0.310 | 0.433 |
| GI2 | 0.077 | 0.357 | 0.287 | 0.366 | 0.345 | 0.742 | 0.218 | 0.262 | 0.296 | 0.349 |
| GI3 | 0.098 | 0.379 | 0.430 | 0.461 | 0.443 | 0.898 | 0.433 | 0.383 | 0.233 | 0.475 |
| HA1 | 0.326 | 0.543 | 0.388 | 0.517 | 0.405 | 0.384 | 0.864 | 0.500 | 0.088 | 0.511 |
| HA2 | 0.382 | 0.384 | −0.048 | 0.079 | 0.504 | 0.299 | 0.677 | −0.045 | 0.606 | 0.345 |
| PA1 | 0.109 | 0.341 | 0.668 | 0.679 | 0.276 | 0.433 | 0.316 | 0.857 | 0.104 | 0.342 |
| PA2 | 0.059 | 0.342 | 0.796 | 0.700 | 0.231 | 0.384 | 0.249 | 0.914 | 0.142 | 0.268 |
| PA3 | 0.075 | 0.309 | 0.683 | 0.653 | 0.284 | 0.354 | 0.354 | 0.914 | 0.127 | 0.276 |
| PA4 | 0.104 | 0.359 | 0.699 | 0.720 | 0.301 | 0.354 | 0.282 | 0.936 | 0.154 | 0.276 |
| PA5 | 0.158 | 0.466 | 0.802 | 0.851 | 0.352 | 0.424 | 0.395 | 0.909 | 0.219 | 0.421 |
| SJ1 | 0.258 | 0.367 | 0.149 | 0.191 | 0.517 | 0.277 | 0.303 | 0.067 | 0.872 | 0.280 |
| SJ2 | 0.277 | 0.455 | 0.270 | 0.372 | 0.597 | 0.331 | 0.360 | 0.275 | 0.920 | 0.390 |
| SJ3 | 0.280 | 0.309 | −0.024 | 0.149 | 0.547 | 0.241 | 0.325 | 0.027 | 0.828 | 0.385 |
| SY1 | 0.357 | 0.431 | 0.322 | 0.487 | 0.649 | 0.518 | 0.473 | 0.362 | 0.385 | 0.881 |
| SY2 | 0.522 | 0.392 | 0.083 | 0.267 | 0.644 | 0.298 | 0.568 | 0.071 | 0.416 | 0.775 |
| SY3 | 0.314 | 0.459 | 0.415 | 0.526 | 0.605 | 0.472 | 0.463 | 0.403 | 0.247 | 0.859 |
| SY4 | 0.387 | 0.479 | 0.308 | 0.522 | 0.632 | 0.417 | 0.399 | 0.348 | 0.315 | 0.871 |
Note: AD = Agesim; EA = Attitude toward physical fitness; EH = Behaviour toward physical fitness; EI = Intention toward physical fitness; EM = Empathy; GI = Group identification; HA = Psychological proximity; PA = Perceived behavioural control; SJ = Subjective norm; SY = Sympathy.
Table 4.
Internal consistency and correlation across constructs.
| AVE | Composite Reliability | Construct | AD | EA | EH | EI | EM | GI | HA | PA | SJ | SY |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.539 | 0.854 | AD | 0.788 | |||||||||
| 0.661 | 0.853 | EA | 0.467 | 0.738 | ||||||||
| 0.808 | 0.926 | EH | 0.086 | 0.342 | 0.880 | |||||||
| 0.801 | 0.923 | EI | 0.277 | 0.525 | 0.839 | 0.876 | ||||||
| 0.764 | 0.942 | EM | 0.324 | 0.449 | 0.305 | 0.433 | 0.921 | |||||
| 0.694 | 0.871 | GI | 0.129 | 0.434 | 0.439 | 0.510 | 0.534 | 0.781 | ||||
| 0.602 | 0.749 | HA | 0.443 | 0.608 | 0.268 | 0.430 | 0.565 | 0.443 | 0.352 | |||
| 0.822 | 0.958 | PA | 0.113 | 0.405 | 0.809 | 0.801 | 0.320 | 0.431 | 0.354 | 0.946 | ||
| 0.764 | 0.906 | SJ | 0.308 | 0.443 | 0.179 | 0.294 | 0.635 | 0.331 | 0.378 | 0.168 | 0.849 | |
| 0.718 | 0.910 | SY | 0.464 | 0.519 | 0.336 | 0.533 | 0.747 | 0.508 | 0.563 | 0.353 | 0.403 | 0.868 |
Note: AVE = Average variance extracted; AD = Agesim; EA = Attitude toward physical fitness; EH = Behaviour toward physical fitness; EI = Intention toward physical fitness; EM = Empathy; GI = Group identification; HA = Psychological proximity; PA = Perceived behavioural control; SJ = Subjective norm; SY = Sympathy.
Table 5.
Summary of the hypothesis result.
| Hypothesis | Path | Original Sample (O) | Sample Mean (M) | Standard Error (STERR) | T Statistics (|O/STERR|) | p Value |
|---|---|---|---|---|---|---|
| H1 | GI -> HA | 0.194 | 0.190 | 0.122 | 1.593 | |
| H2a | GI -> EM | 0.534 | 0.541 | 0.078 | 6.824 | *** |
| H2b | EM -> HA | 0.272 | 0.259 | 0.138 | 1.964 | * |
| H3a | GI -> SY | 0.508 | 0.521 | 0.080 | 6.369 | *** |
| H3b | SY -> HA | 0.138 | 0.142 | 0.147 | 0.944 | |
| H4a | GI -> AD | 0.129 | 0.154 | 0.115 | 1.123 | |
| H4b | AD -> HA | 0.266 | 0.287 | 0.097 | 2.743 | ** |
| H5 | HA -> EA | 0.513 | 0.520 | 0.105 | 4.905 | *** |
| H6 | HA -> EI | 0.044 | 0.054 | 0.075 | 0.583 | |
| H7 | EI -> EH | 0.093 | 0.088 | 0.254 | 0.368 | |
| H8 | EA -> EI | 0.179 | 0.176 | 0.087 | 2.060 | * |
| H9a | SJ -> EI | 0.081 | 0.084 | 0.066 | 1.233 | |
| H9b | SJ -> EA | 0.249 | 0.254 | 0.091 | 2.729 | ** |
| H10 | PA -> EI | 0.699 | 0.691 | 0.075 | 9.385 | *** |
| H11 | PA -> EH | 0.380 | 0.379 | 0.098 | 3.895 | *** |
| H12 | EI Gender -> EH | 0.566 | 0.575 | 0.286 | 1.976 | * |
Note: * p < 0.05, ** p < 0.01, *** p < 0.00.1; AD = Agesim; EA = Attitude toward physical fitness; EH = Behaviour toward physical fitness; EI = Intention toward physical fitness; EM = Empathy; GI = Group identification; HA = Psychological proximity; PA = Perceived behavioural control; SJ = Subjective norm; SY = Sympathy.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tsai, T.-H.; Wong, A.M.; Lee, H.-F.; Tseng, K.C. A Study on the Motivation of Older Adults to Participate in Exercise or Physical Fitness Activities. Sustainability 2022, 14, 6355. https://0-doi-org.brum.beds.ac.uk/10.3390/su14106355
AMA Style
Tsai T-H, Wong AM, Lee H-F, Tseng KC. A Study on the Motivation of Older Adults to Participate in Exercise or Physical Fitness Activities. Sustainability. 2022; 14(10):6355. https://0-doi-org.brum.beds.ac.uk/10.3390/su14106355
Chicago/Turabian StyleTsai, Tsai-Hsuan, Alice M. Wong, Hsiu-Feng Lee, and Kevin C. Tseng. 2022. "A Study on the Motivation of Older Adults to Participate in Exercise or Physical Fitness Activities" Sustainability 14, no. 10: 6355. https://0-doi-org.brum.beds.ac.uk/10.3390/su14106355
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.