Oral Adjuvant Curcumin Therapy for Attaining Clinical Remission in Ulcerative Colitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria and PICO
2.2. Search Strategy
2.3. Selection of Studies and Interventions of Interest
2.4. Data Extraction
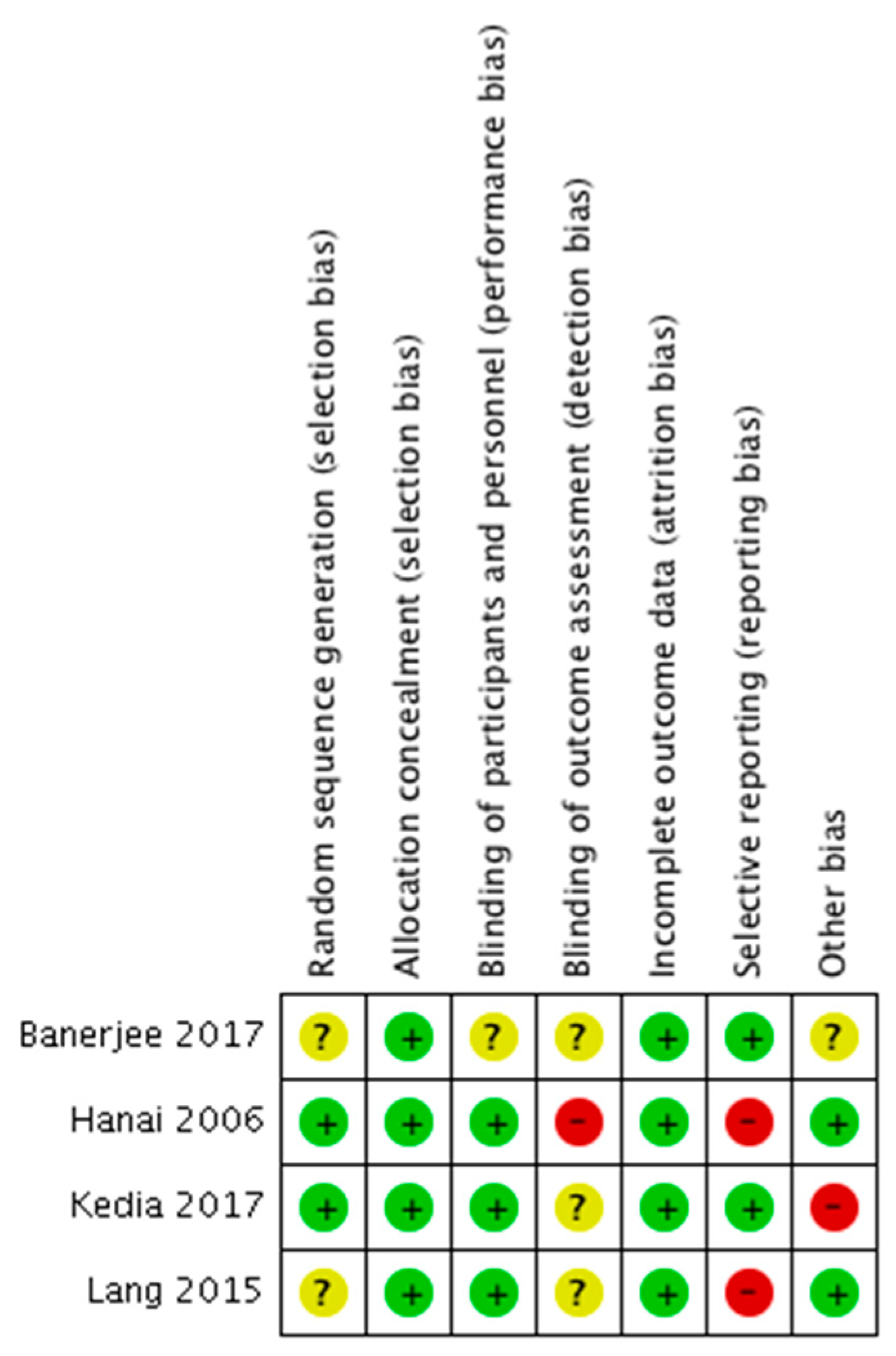
2.5. Risk of Bias and Quality Assessment
2.6. Statistical Analyses
3. Results
3.1. Study Characteristics and Risk of Bias
3.2. Exclusion of RCTs
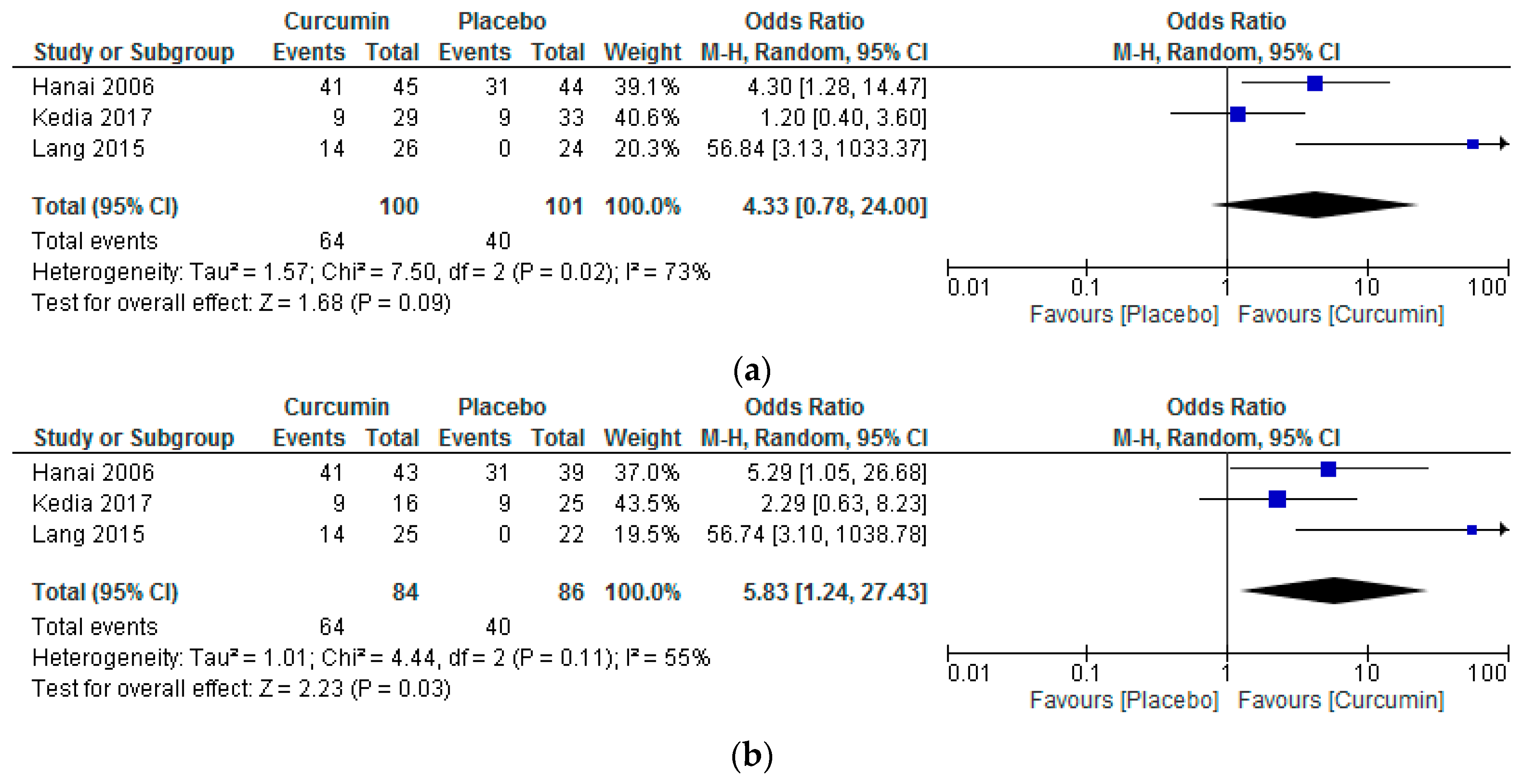
3.3. Effects of the Intervention on Remission Attainment
3.4. Effects of the Intervention on Other Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2018, 390, 2769–2778. [Google Scholar] [CrossRef]
- Weimers, P.; Munkholm, P. The Natural History of IBD: Lessons Learned. Curr. Treat. Opt. Gastroenterol. 2018, 16, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Durchschein, F.; Petritsch, W.; Hammer, H.F. Diet therapy for inflammatory bowel diseases: The established and the new. World J. Gastroenterol. 2016, 22, 2179–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN guideline: Clinical nutrition in inflammatory bowel disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limketkai, B.N.; Wolf, A.; Parian, A.M. Nutritional Interventions in the Patient with Inflammatory Bowel Disease. Gastroenterol. Clin. N. Am. 2018, 47, 155–177. [Google Scholar] [CrossRef] [PubMed]
- Eustace, G.J.; Melmed, G.Y. Therapy for Crohn’s Disease: A Review of Recent Developments. Curr. Gastroenterol. Rep. 2018, 20, 19. [Google Scholar] [CrossRef] [PubMed]
- Neurath, M. Current and emerging therapeutic targets for IBD. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Larussa, T.; Imeneo, M.; Luzza, F. Potential role of nutraceutical compounds in inflammatory bowel disease. World J. Gastroenterol. 2017, 23, 2483. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, F.; Javadi, M.; Karami, A.A.; Gholaminejad, F.; Kavianpour, M.; Haghighian, H.K. Curcumin nanomicelle improves semen parameters, oxidative stress, inflammatory biomarkers, and reproductive hormones in infertile men: A randomized clinical trial. Phytother. Res. 2018, 32, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Negi, P.S.; Jayaprakasha, G.K.; Jagan Mohan Rao, L.; Sakariah, K.K. Antibacterial Activity of Turmeric Oil: A Byproduct from Curcumin Manufacture. J. Agric. Food Chem. 1999, 47, 4297–4300. [Google Scholar] [CrossRef] [PubMed]
- Amalraj, A.; Varma, K.; Jacob, J.; Divya, C.; Kunnumakkara, A.B.; Stohs, S.J.; Gopi, S. A Novel Highly Bioavailable Curcumin Formulation Improves Symptoms and Diagnostic Indicators in Rheumatoid Arthritis Patients: A Randomized, Double-Blind, Placebo-Controlled, Two-Dose, Three-Arm, and Parallel-Group Study. J. Med. Food 2017, 20, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Asteriou, E.; Gkoutzourelas, A.; Mavropoulos, A.; Katsiari, C.; Sakkas, L.; Bogdanos, D. Curcumin for the Management of Periodontitis and Early ACPA-Positive Rheumatoid Arthritis: Killing Two Birds with One Stone. Nutrients 2018, 10, 908. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Khalili, N.; Sahebi, E.; Namazi, S.; Reiner, Ž.; Majeed, M.; Sahebkar, A. Curcuminoids modify lipid profile in type 2 diabetes mellitus: A randomized controlled trial. Complement. Ther. Med. 2017, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Santos-Parker, J.R.; Strahler, T.R.; Bassett, C.J.; Bispham, N.Z.; Chonchol, M.B.; Seals, D.R. Curcumin supplementation improves vascular endothelial function in healthy middle-aged and older adults by increasing nitric oxide bioavailability and reducing oxidative stress. Aging 2017, 9, 187–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, S.K.; Ahuja, V.; Sankar, M.J.; Kumar, A.; Moss, A.C. Curcumin for maintenance of remission in ulcerative colitis. Cochrane Database Syst. Rev. 2012, 10, CD008424. [Google Scholar] [CrossRef] [PubMed]
- Ali, T.; Shakir, F.; Morton, J. Curcumin and inflammatory bowel disease: Biological mechanisms and clinical implication. Digestion 2012, 85, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Iida, T.; Takeuchi, K.; Watanabe, F.; Maruyama, Y.; Andoh, A.; Tsujikawa, T.; Fujiyama, Y.; Mitsuyama, K.; Sata, M.; et al. Curcumin maintenance therapy for ulcerative colitis: Randomized, multicenter, double-blind, placebo-controlled trial. Clin. Gastroenterol. Hepatol. 2006, 4, 1502–1506. [Google Scholar] [CrossRef] [PubMed]
- Holt, P.R.; Katz, S.; Kirshoff, R. Curcumin Therapy in Inflammatory Bowel Disease: A Pilot Study. Dig. Dis. Sci. 2005, 50, 2191–2193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rachmilewitz, D. Coated mesalazine (5-aminosalicylic acid) versus sulphasalazine in the treatment of active ulcerative colitis: A randomised trial. BMJ 1989, 298, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, R.S.; Ayres, R.C.; Pounder, R.E.; Allan, R.N. A simple clinical colitis activity index. Gut 1998, 43, 29–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, L.R.; Martin, F.; Greer, S.; Robinson, M.; Greenberger, N.; Saibil, F.; Martin, T.; Sparr, J.; Prokipchuk, E.; Borgen, L. 5-Aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis. Gastroenterology 1987, 92, 1894–1898. [Google Scholar] [CrossRef]
- Baron, J.H.; Connell, A.M.; Lennard-Jones, J.E. Variation between observers in describing mucosal appearances in proctocolitis. Br. Med. J. 1964, 1, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated Oral 5-Aminosalicylic Acid Therapy for Mildly to Moderately Active Ulcerative Colitis. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Sandborn, W.J.; Feagan, B.G.; Geboes, K.; Hanauer, S.B.; Irvine, E.J.; Lémann, M.; Marteau, P.; Rutgeerts, P.; Schölmerich, J.; et al. A Review of Activity Indices and Efficacy End Points for Clinical Trials of Medical Therapy in Adults with Ulcerative Colitis. Gastroenterology 2007, 132, 763–786. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 (updated March 2011); The Cochrane Collaboration: London, UK, 2011; ISBN 9780470057964. [Google Scholar]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [PubMed]
- The Nordic Cochrane Centre Review Manager; Cochrane Collaboration: London, UK, 2014.
- Sharma, T.; Gøtzsche, P.C.; Kuss, O. The Yusuf-Peto method was not a robust method for meta-analyses of rare events data from antidepressant trials. J. Clin. Epidemiol. 2017, 91, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.; Salomon, N.; Wu, J.C.Y.; Kopylov, U.; Lahat, A.; Har-Noy, O.; Ching, J.Y.L.; Cheong, P.K.; Avidan, B.; Gamus, D.; et al. Curcumin in Combination with Mesalamine Induces Remission in Patients with Mild-to-Moderate Ulcerative Colitis in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1444.e1–1449.e1. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Bhatia, V.; Thareja, S.; Garg, S.; Mouli, V.P.; Bopanna, S.; Tiwari, V.; Makharia, G.; Ahuja, V. Low dose oral curcumin is not effective in induction of remission in mild to moderate ulcerative colitis: Results from a randomized double blind placebo controlled trial. World J. Gastrointest. Pharmacol. Ther. 2017, 8, 147. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Medaboina, K.; Boramma, G.G.; Amsrala, S.; Reddy, D.N. Novel Bio-Enhanced Curcumin with Mesalamine for Induction of Remission in Mild to Moderate Ulcerative Colitis. Gastroenterology 2017, 152, S587. [Google Scholar] [CrossRef]
- Satsangi, J.; Silverberg, M.S.; Vermeire, S.; Colombel, J.-F. The Montreal classification of inflammatory bowel disease: Controversies, consensus, and implications. Gut 2006, 55, 749–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, S.P.L.; Schnell, D.; Krzeski, P.; Abreu, M.T.; Altman, D.G.; Colombel, J.-F.; Feagan, B.G.; Hanauer, S.B.; Lémann, M.; Lichtenstein, G.R.; et al. Developing an instrument to assess the endoscopic severity of ulcerative colitis: The Ulcerative Colitis Endoscopic Index of Severity (UCEIS). Gut 2012, 61, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How Many Studies Do You Need? A Primer on Statistical Power for Meta-Analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Cumming, G. Understanding the New Statistics: Effect Sizes, Confidence Intervals, and Meta-Analysis; Routledge: Melbourne, Australia, 2011; ISBN 041587968X. [Google Scholar]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A Review of Its’ Effects on Human Health. Foods 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Holt, P.R. Curcumin for Inflammatory Bowel Disease: A Caution. Clin. Gastroenterol. Hepatol. 2016, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, Y.; Tsutsumi, Y.; Kataoka, Y.; Tsujimoto, H.; Yamamoto, Y.; Papola, D.; Guyatt, G.H.; Fukuhara, S.; Furukawa, T.A. Association between statistical significance and time to publication among systematic reviews: A study protocol for a meta-epidemiological investigation. BMJ Open 2017, 7, e018856. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Glaspole, I.; Glassberg, M.K.; Kardatzke, D.R.; Daigl, M.; Kirchgaessler, K.-U.; Lancaster, L.H.; et al. Effect of pirfenidone on mortality: Pooled analyses and meta-analyses of clinical trials in idiopathic pulmonary fibrosis. Lancet Respir. Med. 2017, 5, 33–41. [Google Scholar] [CrossRef]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for Medical Use. JAMA 2015, 313, 2456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschos, P.; Katsoula, A.; Salanti, G.; Giouleme, O.; Athanasiadou, E.; Tsapas, A. Systematic review with network meta-analysis: The impact of medical interventions for moderate-to-severe ulcerative colitis on health-related quality of life. Aliment. Pharmacol. Ther. 2018. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. The Mass Production of Redundant, Misleading, and Conflicted Systematic Reviews and Meta-analyses. Milbank Q. 2016, 94, 485–514. [Google Scholar] [CrossRef] [PubMed]
- Singla, V.; Pratap Mouli, V.; Garg, S.K.; Rai, T.; Choudhury, B.N.; Verma, P.; Deb, R.; Tiwari, V.; Rohatgi, S.; Dhingra, R.; et al. Induction with NCB-02 (curcumin) enema for mild-to-moderate distal ulcerative colitis—A randomized, placebo-controlled, pilot study. J. Crohns Colitis 2014, 8, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Efthimiou, O. Practical guide to the meta-analysis of rare events. Evid.-Based Ment. Health 2018, 21, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, U.; Anwar, H.; Quadri, A.A. Use of Curcumin in Achieving Clinical and Endoscopic Remission in Ulcerative Colitis: A Systematic Review and Meta-analysis. Am. J. Med. Sci. 2018, 356, 350–356. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author: | Hanai [17] | Lang [32] | Kedia [33] | Banerjee [34] |
|---|---|---|---|---|
| Duration: | 2004–2005 | 2011–2014 | 2003–2005 | 2016–2017 |
| Countries: | Japan | Israel, Cyprus, Hong Kong | India | India |
| Registry: | - | NCT01320436 | - | NCT02683733 |
| Ethical Approval: | √ | √ | √ | NR |
| Multicentre: | √ | √ | - | - |
| Masking: | Double-blind | Double-blind | Double-blind | Triple-blind |
| Results publication: | Clin. Gastroenterol. Hepatol. (Journal) | Clin. Gastroenterol. Hepatol. (Journal) | World J. Gastrointest. Pharmacol. Ther. (Journal) | AGA 2017 DDW (abstract published in Gastroenterol. Journal) |
| Timing of publication: | 2006 | 2015 | 2017 | 2017 |
| Publication form: | Full-text | Full-text | Full-text | Abstract only |
| Patients: | CAI ≤ 4 (stable previous 4 weeks) * | Mild–moderate UC (5 ≤ SCCAI < 12) | Mild–moderate UC (3 ≤ UCDAI < 9) | Mild–moderate UC (2 ≤ MES < 6) |
| Age (years): | 13–65 as inclusion, 18–75 as PP | 18–70 | ≥18 | 18–70 |
| Disease extent (Montreal Classification) [35]: | NR | NR | NR | NR |
| Treatment: | SZ (1–3 g/day) or Mesalamine (1.5–3 g/day) | Mesalamine oral 4 g/day + topical enema | Mesalamine 2.4 g/day | Mesalamine (oral + enema) with physician defined dose |
| Inclusion criteria: | √ | √ | √ | √ |
| Exclusion criteria: | √ | √ | √ | √ |
| Treatment arm: | n = 43 on curcumin | n = 26 on curcumin | n = 29 on curcumin | n = 22 on curcumin |
| Control arm: | n = 39 on placebo | n = 24 on placebo | n = 33 on placebo | n = 25 on placebo |
| Intervention: | 2 g curcumin/day | 3 g curcumin/day | 150 mg purified curcumin × 3/day | Registry: 50 mg SMEDDS caps increased to 100 mg after 2 weeks, if no response was noted Results: 50 mg SMEDDS caps |
| Comparator: | Placebo | Placebo | Placebo | Placebo |
| Duration: | 6 months | 1 month | 8 weeks | Registry: 1 year Results: 3 months |
| Measures: | CAI, EI | SCCAI, MES, Hb, CRP, | UCDAI, BES | MES, UCEIS |
| Timing of clinical remission evaluation: | At month 0, 2, 4, 6, 12 | At week 0 and 4 | At week 0, 4, and 8, or as required | At week 0 and 6, and 3 months |
| Timing of relapse evaluation: | At month 2, 4, 6, 12 | At week 4 | At week 4 and 8, or as required | At week 6, and 3 months |
| Timing of endoscopic remission: | At month 0 and 6 | At week 0 and 4 | At week 0, 4, and 8, or as required | At week 6, and 3 months |
| Primary outcome: | Clinical remission (CAI ≤ 4) at 6 months | Clinical remission (SCCAI ≤ 2) at 4 weeks | Clinical remission (UCDAI ≤ 2) at 8 weeks | Clinical remission (MES ≤ 1) |
| Secondary outcomes: | CAI reduction EI reduction | Clinical response (SCCAI ↓ ≥ 3) Endoscopic remission (MES ≤ 1) Hb < 12 g/dL at 4 weeks) elevated CRP (4 weeks) | Clinical response (UCDAI ↓ ≥ 3) Sigmoidoscopic remission (BES = 0/1) Treatment failure (UCDAI ↑ ≥ +3 points, or treatment intolerance) | Clinical response (MES ↓ ≥ 3) Endoscopic remission (MES ≤ 1 per Results, UCEIS < 3 per Registry) |
| Relapse definition: | CAI ≥ 5 | SCCAI ≥ 5 | UCDAI ≥ +3 points from baseline | NR |
| Mucosal Healing ‡ definition: | NR | any drop of ≥ 1 in MES | BES of 0/1 | any drop of ≥ 1 in MES |
| Non-compliance definition: | - | - | failure to take ≥ 80% of medication | - |
| Adverse effects (severe) (n): | - | n = 3, indifferent between arms (On 1 patient with peptic ulcer before initiation and 2 with worsening UC symptoms) | - | NR |
| Adverse effects (mild) (n): | n = 7 Abdominal bulging, (transient hypertension, transient increase in the number of stools, nausea, and elevated γ–guanosine triphosphate levels in a regular alcohol drinker) | n = 4, indifferent between arms (mild nausea, transient increase in stool frequency, and abdominal bloating) | - | NR |
| Discontinuation (n): | Treatment arm: 2/45 (1 with hypertension withdrew and 1 received prednisone) Control arm: 5/44 (2 withdrew and 3 received either prednisone, or immunosuppressants) | Treatment arm: 1/26 (with pre-existing peptic ulcer) Control arm: 2/24 (1 lost to follow-up, 1 withdrew consent) | Treatment arm: 13/29 (8 with worsening UC symptoms) Control arm: 8/33 (2 with worsening UC symptoms) | Treatment arm: 3/22 Control arm: 2/25 (No further data were reported) |
| Clinical remission PP (n): | Treatment arm: 41/43 (6 months), 33/43 (12 months) Control arm: 31/39 (6 months), 25/39 (12 months) | Treatment arm: 14/25 Control arm: 0/22 | Treatment arm: 9/16 Control arm: 9/25 | † |
| Clinical remission ITT (n): | Treatment arm: 41/45 (6 months), 33/45 (12 months) Control arm: 31/44 (6 months), 25/44 (12 months) | Treatment arm: 14/26 Control arm: 0/24 | Treatment arm: 9/29 Control arm: 9/33 | † |
| Improved DAI # PP (n): | NR | Treatment arm: 16/25 Control arm: 3/22 | Treatment arm: 6/16 Control arm: 12/25 | Treatment arm: 12/19 Control arm: 5/23 |
| Improved DAI # ITT (n): | NR | Treatment arm: 16/26 Control arm: 3/24 | Treatment arm: 6/29 Control arm: 12/33 | Treatment arm: 12/22 Control arm: 5/25 |
| Mucosal Healing ‡ PP (n): | NR | Treatment arm: 8/22 Control arm: 0/16 | Treatment arm: 10/16 Control arm: 10/25 | Treatment arm: 5/19 † Control arm: 0/23 † |
| Mucosal Healing ‡ ITT (n): | NR | 4 patients in the intervention and 8 controls did not provide permission for endoscopy | Treatment arm: 10/29 Control arm: 10/33 | Treatment arm: 5/22 † Control arm: 0/25† |
| Baseline DAI (mean ± SD): | Treatment arm: CAI = 1.3 ± 1.1 Control arm: CAI = 1.0 ± 1.1 | Treatment arm: SCCAI = 6.5 ± 1.5 Control arm: SCCAI = 7.0 ± 1.8 | Treatment arm: UCDAI = 5.2 ± 2.0 Control arm: UCDAI = 5.5 ± 1.9 | NR |
| Post-treatment DAI (mean ± SD): | Treatment arm: CAI = 1.0 ± 2.0 (6 months) Control arm: CAI = 2.2 ± 2.3 (6 months) | NR | Treatment arm: UCDAI = 3.4 ± 3.1 Control arm: UCDAI = 3.8 ± 2.8 | NR |
| Baseline EI (mean ± SD): | Treatment arm: EI = 1.3 ± 0.8 Control arm: EI = 1.3 ± 1.0 | Treatment arm: EI = 1.9 ± 0.4 Control arm: EI = 2.1 ± 0.39 | NR | NR |
| Post-treatment EI (mean ± SD): | Treatment arm: EI = 0.8 ± 0.6 (6 months) Control arm: EI = 1.6 ± 1.6 (6 months) | Treatment arm: EI = 1.35 ± 1.19 Control arm: EI = 2.25 ± 0.88 | NR | NR |
| Jadad [28] score | 4 | 4 | 5 | 2 |
| Funding: | Eli and Edythe L. Broad Foundation, but placebo and curcumin tabs supplied by API Co, Ltd. (Japan) | Partly by the Talpiot Medical Leadership grant (Sheba Medical Center, Leona M. and Harry B. Helmsley Charitable Trust) | NR, but curcumin and placebo were supplied by Himalaya Drug Company (India) | Asian Institute of Gastroenterology |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grammatikopoulou, M.G.; Gkiouras, K.; Theodoridis, X.; Asteriou, E.; Forbes, A.; Bogdanos, D.P. Oral Adjuvant Curcumin Therapy for Attaining Clinical Remission in Ulcerative Colitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 1737. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111737
Grammatikopoulou MG, Gkiouras K, Theodoridis X, Asteriou E, Forbes A, Bogdanos DP. Oral Adjuvant Curcumin Therapy for Attaining Clinical Remission in Ulcerative Colitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2018; 10(11):1737. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111737
Chicago/Turabian StyleGrammatikopoulou, Maria G., Konstantinos Gkiouras, Xenophon Theodoridis, Eleni Asteriou, Alastair Forbes, and Dimitrios P. Bogdanos. 2018. "Oral Adjuvant Curcumin Therapy for Attaining Clinical Remission in Ulcerative Colitis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 10, no. 11: 1737. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111737