Gut Permeability Might be Improved by Dietary Fiber in Individuals with Nonalcoholic Fatty Liver Disease (NAFLD) Undergoing Weight Reduction

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. The Nutritional Intervention and Control
2.3. Laboratory Analyses
2.4. Statistics
3. Results
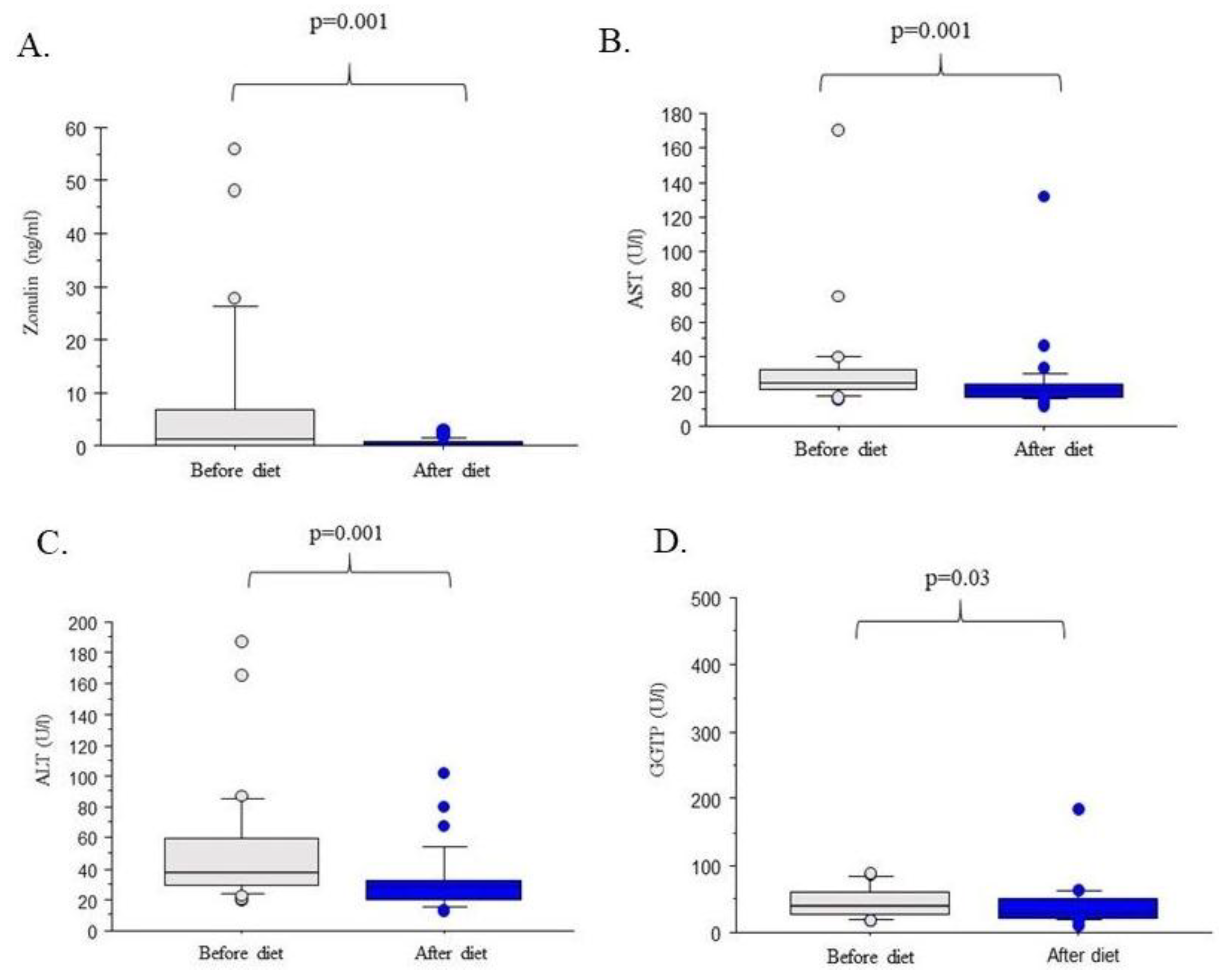
3.1. The Amount of Zonulin in Serum Decreases with the Improvement of Fatty Liver
3.2. The Content of Zonulin in the Serum May be Related to the Increase in Fiber Consumption
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lechuga, S.; Ivanov, A.I. Disruption of the epithelial barrier during intestinal inflammation: Quest for new molecules and mechanisms. Biochim. Biophys. Acta 2017, 7, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Yeruva, S.; Turner, J.R. Contributions of intestinal epithelial barriers to health and disease. Exp. Cell Res. 2017, 358, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M. Interaction between food substances and the intestinal epithelium. Biosci. Biotechnol. Biochem. 2010, 74, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Yan, H.; You, Z.; Wang, P.; Wang, S. Effects of enteral supplementation with glutamine granules on intestinal mucosal barrier function in severe burned patients. Burns 2004, 30, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.A.; Li, J.S. Effects of glutamine on intestinal permeability and bacterial translocation in TPN-rats with endotoxemia. World J. Gastroenterol. 2003, 9, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, J.; Fukumoto, K.; Fukushi, E.; Sonoyama, K.; Kawabata, J. Isolation of tryptophan as an inhibitor of ovalbumin permeation and analysis of its suppressive effect on oral sensitization. Biosci. Biotechnol. Biochem. 2004, 68, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Yasumatsu, H.; Tanabe, S. The casein peptide Asn-Pro-Trp-Asp-Gln enforces the intestinal tight junction partly by increasing occludin expression in Caco-2 cells. Br. J. Nutr. 2010, 104, 951–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, K.; Nakayama, T.; Shimizu, M. Effects of beta-lactoglobulin on the tight-junctional stability of Caco-2-SF monolayer. Biosci. Biotechnol. Biochem. 1998, 62, 1819–1821. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T. Regulation of intestinal epithelial permeability by tight junctions. Cell. Mol. Life Sci. 2013, 70, 631–659. [Google Scholar] [CrossRef] [PubMed]
- Hollon, J.; Puppa, E.L.; Greenwald, B.; Goldberg, E.; Guerrerio, A.; Fasano, A. Effect of gliadin on permeability of intestinal biopsy explants from celiac disease patients and patients with non-celiac gluten sensitivity. Nutrients 2015, 7, 1565–1576. [Google Scholar] [CrossRef] [PubMed]
- Usami, M.; Muraki, K.; Iwamoto, M.; Ohata, A.; Matsushita, E.; Miki, A. Effect of eicosapentaenoic acid (EPA) on tight junction permeability in intestinal monolayer cells. Clin. Nutr. 2001, 20, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Usami, M.L.; Komurasaki, T.; Hanada, A.; Ohata, A.; Matsushita, E.; Miki, A. Effect of gamma-linolenic acid or docosahexaenoic acid on tight junction permeability in intestinal monolayer cells and their mechanism by protein kinase C activation and/or eicosanoid formation. Nutrition 2003, 19, 150–166. [Google Scholar] [CrossRef]
- Pacifico, L.; Bonci, E.; Marandola, L.; Romaggioli, S.; Bascetta, S.; Chiesa, C. Increased circulating zonulin in children with biopsy-proven nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 17107–17114. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A. Zonulin, regulation of tight junctions, and autoimmune diseases. Ann. N. Y. Acad. Sci. 2012, 1258, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hałasa, M.; Maciejewska, D.; Baśkiewicz-Hałasa, M.; Machaliński, B.; Safranow, K.; Stachowska, E. Oral Supplementation with Bovine Colostrum Decreases Intestinal Permeability and Stool Concentrations of Zonulin in Athletes. Nutrients 2017, 9, e370. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD Disease Burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Henao-Mejia, J.; Elinav, E.; Jin, C.; Hao, L.; Mehal, W.Z.; Strowig, T.; Thaiss, C.A.; Kau, A.L.; Eisenbarth, S.C.; Jurczak, M.J.; et al. Inflammasome-mediated dysbiosis regulates progression of NAFLD and obesity. Nature 2012, 482, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Zheng, R.D.; Sun, X.Q.; Ding, W.J.; Wang, X.Y.; Fan, J.G. Gut microbiota dysbiosis in patients with non-alcoholic fatty liver disease. Hepatobiliary Pancreat. Dis. Int. 2017, 16, 375–381. [Google Scholar] [CrossRef]
- Miele, L.; Marrone, G.; Lauritano, C.; Cefalo, C.; Gasbarrini, A.; Day, C.; Grieco, A. Gut-liver axis and microbiota in NAFLD: Insight pathophysiology for novel therapeutic target. Curr. Pharm. Des. 2013, 19, 5314–5324. [Google Scholar] [CrossRef] [PubMed]
- Hendy, O.M.; Elsabaawy, M.M.; Aref, M.M.; Khalaf, F.M.; Oda, A.M.A.; El Shazly, H.M. Evaluation of circulating zonulin as a potential marker in the pathogenesis of nonalcoholic fatty liver disease. Metabolism 2017, 69, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Wybranska, I.; Malczewska-Malec, M.; Partyka, L.; Kiec-Wilk, B.; Kosno, K.; Leszczynska-Golabek, I.; Zdzienicka, A.; Gruca, A.; Kwasniak, M.; Dembinska-Kiec, A. Evaluation of genetic predisposition to insulin resistance by nutrient-induced insulin output ratio (NIOR). Clin. Chem. Lab. Med. 2007, 45, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Poeta, M.; Pierri, L.; Vajro, P. Gut-Liver Axis Derangement in Non-Alcoholic Fatty Liver Disease. Children 2017, 4, 66. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Xu, W.; Zhang, X.; Wong, G.H.; Chan, A.H.; Chan, H.Y.; Tse, C.H.; Shu, S.T.; Choi, P.L.; Chan, H.Y.; et al. Significant positive association of endotoxemia with histological severity in 237 patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2017, 46, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Engstler, A.J.; Aumiller, T.; Degen, C.; Dürr, M.; Weiss, E.; Maier, I.B.; Schattenberg, J.M.; Jin, C.J.; Sellmann, C.; Bergheim, I. Insulin resistance alters hepatic ethanol metabolism: Studies in mice and children with non-alcoholic fatty liver disease. Gut 2016, 65, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- QuickCalcs. Available online: https://www.graphpad.com/quickcalcs/randomselect2 (accessed on 2 November 2016).
- Stachowska, E.; Ryterska, K.; Maciejewska, D.; Banaszczak, M.; Milkiewicz, P.; Milkiewicz, M.; Gutowska, I.; Ossowski, P.; Kaczorowska, M.; Jamioł-Milc, D.; et al. Nutritional Strategies for the Individualized Treatment of Non-Alcoholic Fatty Liver Disease (NAFLD) Based on the Nutrient-Induced Insulin Output Ratio (NIOR). Int. J. Mol. Sci. 2016, 17, 1172. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Itoh, Y.; Harano, Y.; Fujii, K.; Nakajima, T.; Kato, T.; Takeda, N.; Okuda, J.; Ida, K.; et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am. J. Gastroenterol. 2007, 102, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- Laskowski, W. Wartość Odżywcza Diety Polaków Oraz jej Zmiany; Współczesne Kierunki Działań Prozdrowotnych, red. A.; Wolska-Adamczyk, WSIiZ: Warszawa, Poland, 2015. [Google Scholar]
- Damms-Machado, A.; Louis, S.; Schnitzerm, A.; Volynets, V.; Rings, A.; Basrai, M. Gut permeability is related to body weight, fatty liver disease, and insulin resistance in obese individuals undergoing weight reduction. Am. J. Clin. Nutr. 2017, 105, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Cantero, I.; Abete, I.; Monreal, J.I.; Martinez, J.A.; Zulet, M.A. Fruit Fiber Consumption Specifically Improves Liver Health Status in Obese Subjects under Energy Restriction. Nutrients 2017, 9, e667. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Sanyal, A.J. Management of NAFLD: A stage-based approach. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 196–205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Recommendation | Recommended Sources |
|---|---|---|
| Energy | Calculated Individually | |
| Fiber (g/day) | 30–35 | 3 portions of vegetables a day; 2 portions of fruit as: fresh, fermented or boiled, wheat bread, whole-wheat pasta, cereal and brown rice |
| Fat as percentage of total calories (%) | 20–30 | Vegetable fats with a predominance of rapeseed oil and olive oil. |
| Carbohydrates (low and medium IG), percentage of total calories (%) | 55–65 | Low and medium glycemic index as: wheat and mix rye/wheat bread, whole-pasta, cereal and brown rice, fruit and vegetables. |
| Simple carbohydrate, percentage of total calories (%) | 5–10 | Dry fruits |
| Protein (%) | 15 | Poultry (chicken and turkey), fish (oily fish 3 times a week), fermented dairy products (2 times a day), eggs (4–5 a week), lean cottage cheese, cheese with reduced fat content. |
| Fluid (mL/kg) | 35 | Water, coffee (1–2 cup a day) tea (black, green). |
| Vitamins and minerals | Consistent with recommended daily allowance | Natural sources from vegetables and fruit |
| Parameters | Before Diet | After Diet | p Value |
|---|---|---|---|
| Age (year) | 48.03 ±13.13 | - | - |
| Body Mass (kg) | 98.76 ± 19.80 | 91.64 ± 16.60 | NS |
| BMI (kg/m2) | 33.19 ±5.71 | 30.91 ± 5.45 | NS |
| Fat mass (kg) | 38.08 ± 6.06 | 32.84 ± 9.41 | NS |
| Lean body mass (kg) | 60.93 ± 12.90 | 58.48 ± 12.04 | NS |
| Water content (kg) | 45.25 ± 9.16 | 43.81 ± 8.07 | NS |
| Fatty liver (Hamaguchi score) | 2.87 ± 0.60 | 1.40 ± 0.93 | 0.009 |
| Triacylglycerols (mg/dL) | 219.09 ± 326.01 | 166.31 ± 219.71 | 0.036 |
| Total cholesterol (mg/dL) | 206.06 ± 52.54 | 200.56 ± 45.44 | NS |
| High density lipoprotein (mg/dL) | 44.84 ± 10.09 | 49.47 ± 14.47 | NS |
| Low density lipoprotein (mg/dL) | 121.15 ± 33.43 | 122. ± 60.32 | NS |
| Total lipids (mg/dL) | 731.06 ± 414.63 | 706.44 ± 300.43 | NS |
| Glucose (mg/mL) | 104.50 ± 20.01 | 100.78 ± 10.72 | NS |
| Insulin (U/mL) | 17.90 ± 11.44 | 7.47 ± 5.34 | 0.034 |
| HOMA-IR | 4.85 ± 3.14 | 1.89 ± 1.36 | 0.041 |
| Parameters | RHO | p Value |
|---|---|---|
| Age (years) | 0.05 | NS |
| Body Mass (kg) | <0.01 | NS |
| BMI (kg/m²) | (−) 0.18 | NS |
| Fat mass (kg) | (−) 0.13 | NS |
| Fat content (%) | (−) 0.17 | NS |
| Lean body mass (kg) | 0.09 | NS |
| Water content (kg) | 0.13 | NS |
| Aspartate transaminase (U/L) | 0.35 | 0.041 |
| Alanine transaminase (U/L) | 0.36 | 0.043 |
| Gamma-glutamyltransferase (U/L) | 0.19 | NS |
| Triacylglycerols (mg/dL) | 0.17 | NS |
| Total cholesterol (mg/dL) | 0.22 | NS |
| High density lipoprotein (mg/dL) | (−) 0.30 | 0.029 |
| Low density lipoprotein (mg/dL) | 0.37 | 0.032 |
| Total Lipids (mg/dL) | 0.31 | 0.041 |
| Glucose (mg/mL) | (−) 0.07 | NS |
| Insulin (U/mL) | (−) 0.10 | NS |
| Fatty liver (Hamaguchi score) | 0.33 | 0.037 |
| Frequency of Consumption According FFQ | Before Intervention | During the Diet | Change in Frequency |
|---|---|---|---|
| Dairy products | Every day | Every day | No change |
| Cereal products | A few times a day | A few times a day | No change |
| Fats | Every day | Every day | No change |
| Fruits | A few times a week | A few times a day | Increased |
| Vegetables and grains | A few times a week | A few times a day | Increased |
| Poultry, meet and fish | Every day | Every day | No change |
| Parameters | RHO | p Value |
|---|---|---|
| Energy of diet (kcal) | 0.01 | NS |
| Protein (%) | (−) 0.01 | NS |
| Fat (%) | (−) 0.07 | NS |
| Saturated fatty acids (%) | (−) 0.02 | NS |
| Monounsaturated fatty acids (%) | (−) 0.03 | NS |
| Polyunsaturated fatty acids (%) | (−) 0.20 | NS |
| Carbohydrates (%) | 0.07 | NS |
| Fiber (%) | (−) 0.30 | 0.043 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krawczyk, M.; Maciejewska, D.; Ryterska, K.; Czerwińka-Rogowska, M.; Jamioł-Milc, D.; Skonieczna-Żydecka, K.; Milkiewicz, P.; Raszeja-Wyszomirska, J.; Stachowska, E. Gut Permeability Might be Improved by Dietary Fiber in Individuals with Nonalcoholic Fatty Liver Disease (NAFLD) Undergoing Weight Reduction. Nutrients 2018, 10, 1793. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111793
Krawczyk M, Maciejewska D, Ryterska K, Czerwińka-Rogowska M, Jamioł-Milc D, Skonieczna-Żydecka K, Milkiewicz P, Raszeja-Wyszomirska J, Stachowska E. Gut Permeability Might be Improved by Dietary Fiber in Individuals with Nonalcoholic Fatty Liver Disease (NAFLD) Undergoing Weight Reduction. Nutrients. 2018; 10(11):1793. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111793
Chicago/Turabian StyleKrawczyk, Marcin, Dominika Maciejewska, Karina Ryterska, Maja Czerwińka-Rogowska, Dominika Jamioł-Milc, Karolina Skonieczna-Żydecka, Piotr Milkiewicz, Joanna Raszeja-Wyszomirska, and Ewa Stachowska. 2018. "Gut Permeability Might be Improved by Dietary Fiber in Individuals with Nonalcoholic Fatty Liver Disease (NAFLD) Undergoing Weight Reduction" Nutrients 10, no. 11: 1793. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111793