The Use of Glycomacropeptide in Patients with Phenylketonuria: A Systematic Review and Meta-Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Question
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Appraisal
2.6. Assessment of Risk of Bias
2.7. Data Analysis
3. Results
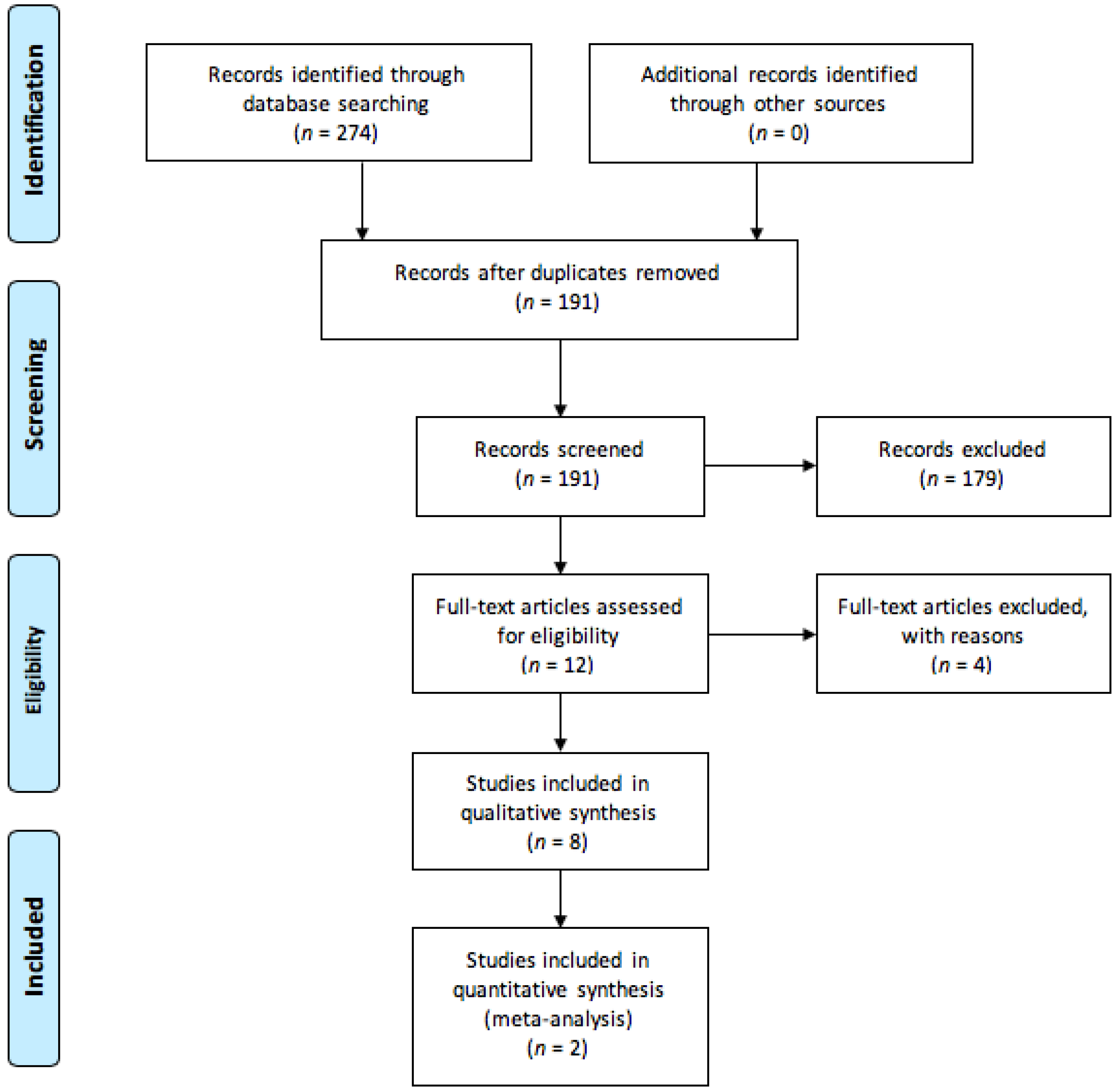
3.1. Study Selection
3.2. Study Characteristics
3.3. Treatment and Outcome Measures
3.4. Acceptability/Palatability of GMP Products
3.5. Quality Appraisal
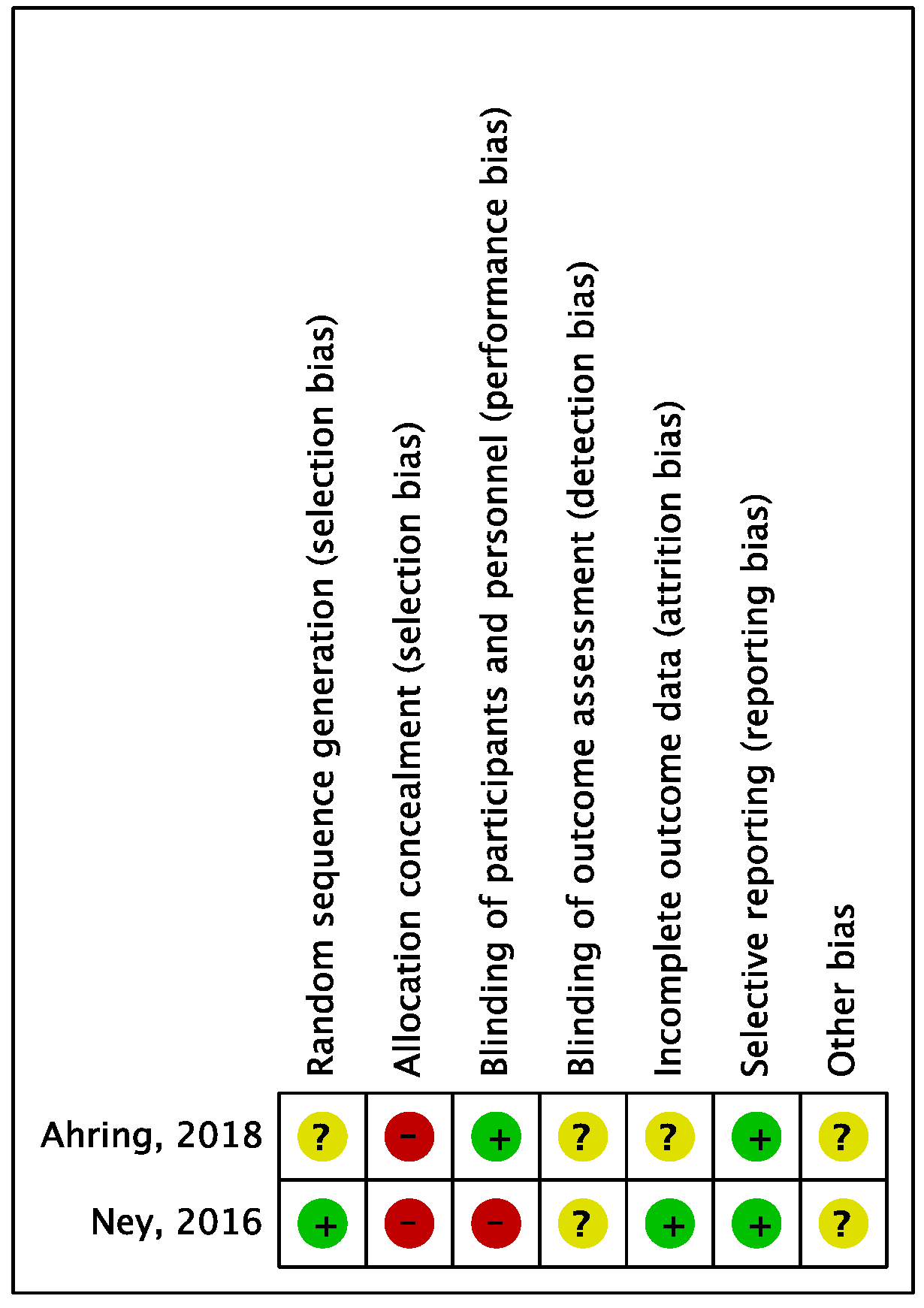
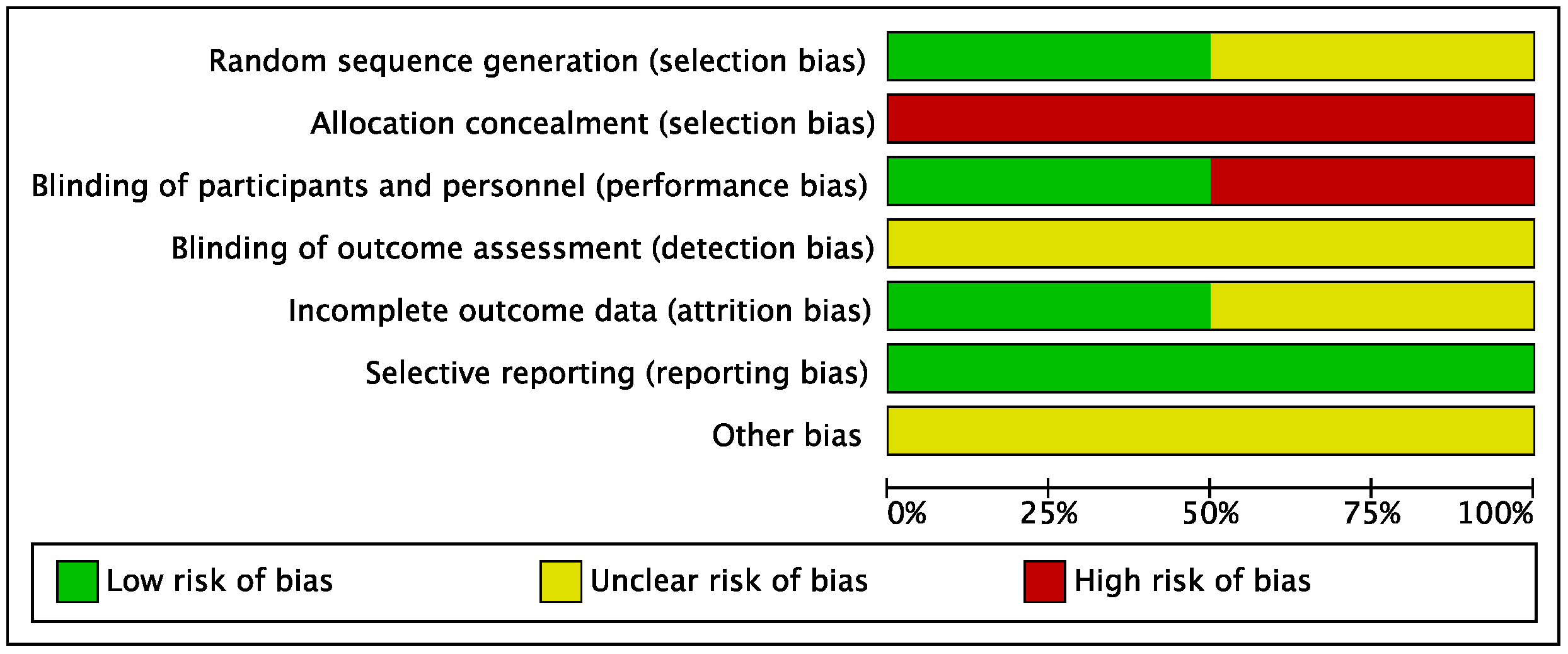
3.6. Assessment of Risk of Bias
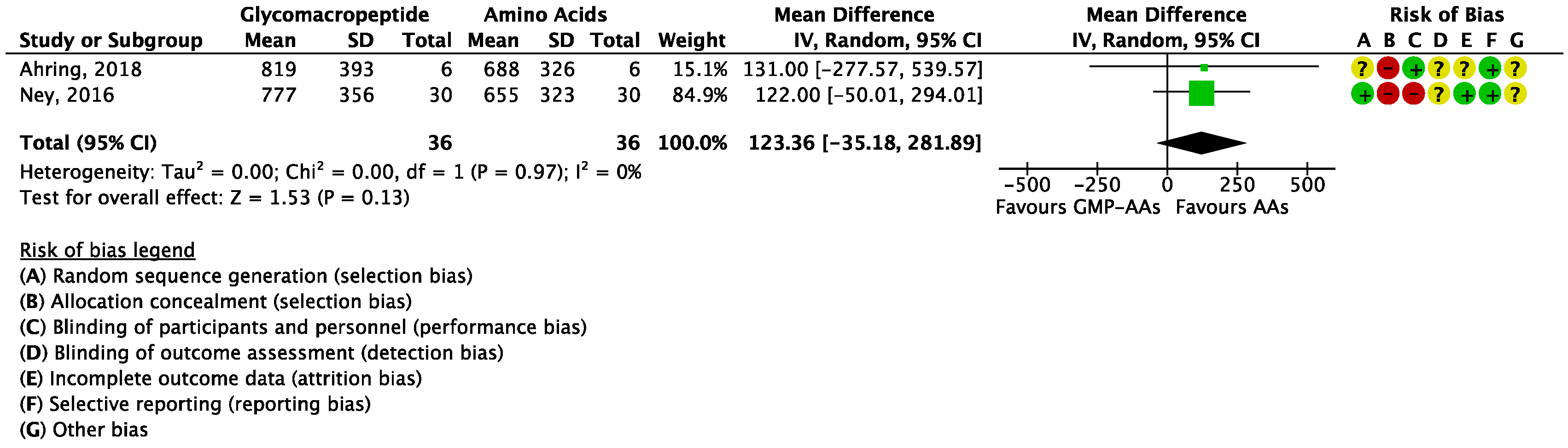
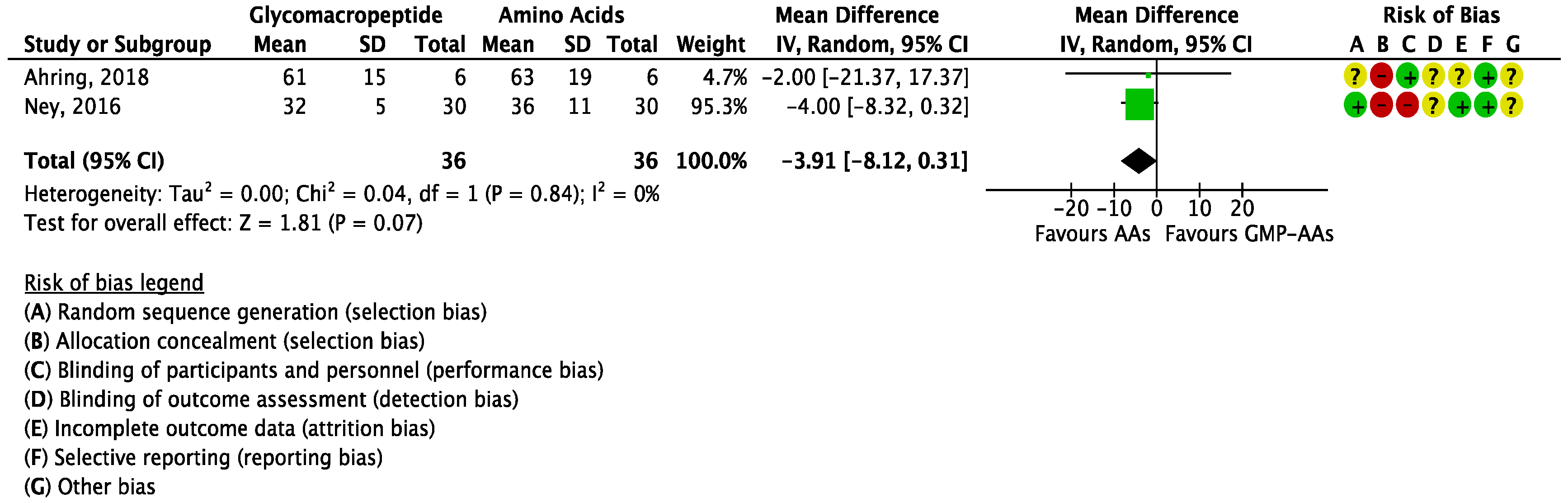
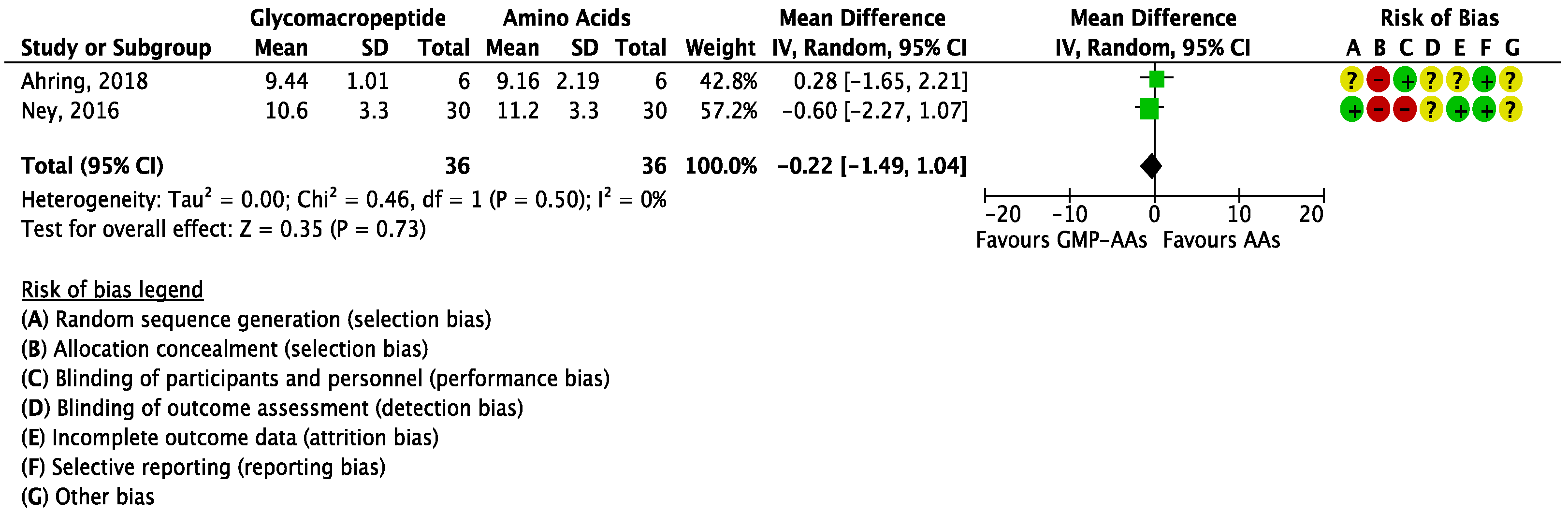
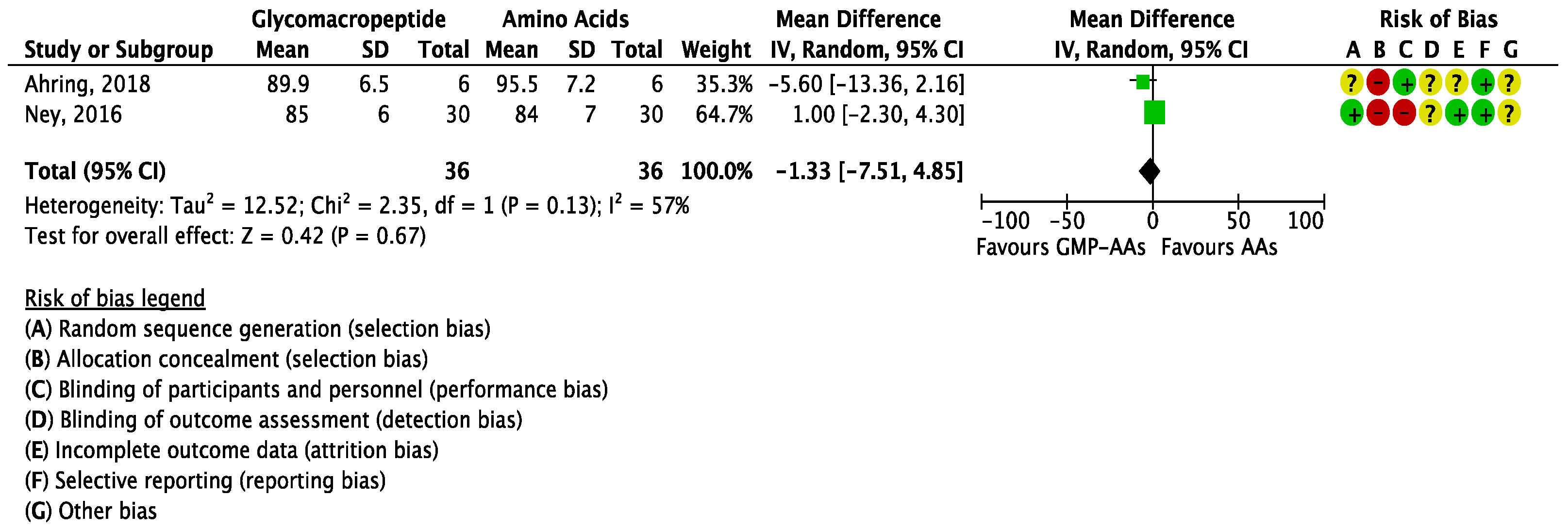
3.7. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blau, N.; Van Spronsen, F.J.; Levy, H.L. Phenylketonuria. Lancet 2010, 376, 1417–1427. [Google Scholar] [CrossRef]
- Bickel, H.; Gerrard, J.; Hickmans, E.M. Preliminary communication. Lancet 1953, 262, 812–813. [Google Scholar] [CrossRef]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 1–56. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Rocha, J.C.; van Rijn, M.; Feillet, F. Nutrition in phenylketonuria. Mol. Genet. MeTab. 2011, 104. [Google Scholar] [CrossRef] [PubMed]
- Pena, M.J.; De Almeida, M.F.; Van Dam, E.; Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Gokmen-Ozel, H.; Lammardo, A.M.; MacDonald, A.; Robert, M.; et al. Protein substitutes for phenylketonuria in Europe: Access and nutritional composition. Eur. J. Clin. Nutr. 2016, 70, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Kure, S.; Hou, D.; Ohura, T.; Iwamoto, H.; Suzuki, S.; Sugiyama, N.; Sakamoto, O.; Fujii, K.; Matsubara, Y.; Narisawa, K. Tetrahydrobiopterin-responsive phenylalanine hydroxylase deficiency. J. Pediatr. 1999, 135, 375–378. [Google Scholar] [CrossRef]
- MacDonald, A.; Van Rijn, M.; Gokmen-Ozel, H.; Burgard, P. The reality of dietary compliance in the management of phenylketonuria. J. Inherit. Metab. Dis. 2010, 33, 665–670. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, E.L.; Ney, D.M. Nutritional management of phenylketonuria. Ann. Nestle 2010, 68, 58–69. [Google Scholar] [CrossRef] [PubMed]
- LaClair, C.E.; Ney, D.M.; MacLeod, E.L.; Etzel, M.R. Purification and use of glycomacropeptide for nutritional management of phenylketonuria. J. Food Sci. 2009, 74, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; van Calcar, S.C.; Nelson, K.L.; Gleason, S.T.; Ney, D.M. Acceptable low-phenylalanine foods and beverages can be made with glycomacropeptide from cheese whey for individuals with PKU. Mol. Genet. MeTab. 2007, 92, 176–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ney, D.M.; Etzel, M.R. Designing medical foods for inherited metabolic disorders: Why intact protein is superior to amino acids. Curr. Opin. Biotechnol. 2017, 44, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.M.; Hull, A.K.; van Calcar, S.C.; Liu, X.; Etzel, M.R. Dietary glycomacropeptide supports growth and reduces the concentrations of phenylalanine in plasma and brain in a murine model of phenylketonuria. J. Nutr. 2008, 138, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Solverson, P.; Murali, S.G.; Brinkman, A.S.; Nelson, D.W.; Clayton, M.K.; Yen, C.-L.E.; Ney, D.M. Glycomacropeptide, a low-phenylalanine protein isolated from cheese whey, supports growth and attenuates metabolic stress in the murine model of phenylketonuria. AJP Endocrinol. MeTab. 2012, 302, E885–E895. [Google Scholar] [CrossRef] [PubMed]
- Sawin, E.A.; Murali, S.G.; Ney, D.M. Differential effects of low-phenylalanine protein sources on brain neurotransmitters and behavior in C57Bl/6-Pah(enu2) mice. Mol. Genet. MeTab. 2014, 111, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Sawin, E.A.; De Wolfe, T.J.; Aktas, B.; Stroup, B.M.; Murali, S.G.; Steele, J.L.; Ney, D.M. Glycomacropeptide is a prebiotic that reduces Desulfovibrio bacteria, increases cecal short-chain fatty acids, and is anti-inflammatory in mice. Am. J. Physiol. Liver Physiol. 2015, 309, G590–G601. [Google Scholar] [CrossRef] [PubMed]
- Solverson, P.; Murali, S.G.; Litscher, S.J.; Blank, R.D.; Ney, D.M. Low bone strength is a manifestation of phenylketonuria in mice and is attenuated by a glycomacropeptide diet. PLoS ONE 2012, 7, e45165. [Google Scholar] [CrossRef] [PubMed]
- Van Calcar, S.C.; MacLeod, E.L.; Gleason, S.T.; Etzel, M.R.; Clayton, M.K.; Wolff, J.A.; Ney, D.M. Improved nutritional management of phenylketonuria by using a diet ontaining glycomacropeptide compared with amino acids. Am. J. Clin. Nutr. 2009, 89, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Ahring, K.K.; Lund, A.M.; Jensen, E.; Jensen, T.G.; Brøndum-Nielsen, K.; Pedersen, M.; Bardow, A.; Holst, J.J.; Rehfeld, J.F.; Møller, L.B. Comparison of glycomacropeptide with phenylalanine free-synthetic amino acids in test meals to PKU patients: No significant differences in biomarkers, including plasma phe levels. J. Nutr. MeTab. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Stroup, B.M.; Nair, N.; Murali, S.G.; Broniowska, K.; Rohr, F.; Levy, H.L.; Ney, D.M. Metabolomic markers of essential fatty acids, carnitine, and cholesterol metabolism in adults and adolescents with phenylketonuria. J. Nutr. 2018, 148, 194–201. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, E.L.; Clayton, M.K.; van Calcar, S.C.; Ney, D.M. Breakfast with glycomacropeptide compared with amino acids suppresses plasma ghrelin levels in individuals with phenylketonuria. Mol. Genet. MeTable 2010, 100, 303–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaki, O.K.; El-Wakeel, L.; Ebeid, Y.; Ez Elarab, H.S.; Moustafa, A.; Abdulazim, N.; Karara, H.; Elghawaby, A. The use of glycomacropeptide in dietary management of phenylketonuria. J. Nutr. MeTab. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.M.; Stroup, B.M.; Clayton, M.K.; Murali, S.G.; Rice, G.M.; Rohr, F.; Levy, H.L. Glycomacropeptide for nutritional management of phenylketonuria: A randomized, controlled, crossover trial. Am. J. Clin. Nutr. 2016, 104, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.; Evans, S.; Chahal, S.; Santra, S.; MacDonald, A. Glycomacropeptide in children with phenylketonuria: Does its phenylalanine content affect blood phenylalanine control? J. Hum. Nutr. Diet. 2017, 30, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.; Almeida, M.F.; Ramos, P.C.; Rocha, S.; Guimas, A.; Ribeiro, R.; Martins, E.; Bandeira, A.; MacDonald, A.; Rocha, J.C. Nutritional status in patients with phenylketonuria using glycomacropeptide as their major protein source. Eur. J. Clin. Nutr. 2017, 71, 1230–1234. [Google Scholar] [CrossRef] [PubMed]
- Stroup, B.M.; Sawin, E.A.; Murali, S.G.; Binkley, N.; Hansen, K.E.; Ney, D.M. Amino acid medical foods provide a high dietary acid load and increase urinary excretion of renal net acid, calcium, and magnesium compared with glycomacropeptide medical foods in phenylketonuria. J. Nutr. MeTab. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.M.; Murali, S.G.; Stroup, B.M.; Nair, N.; Sawin, E.A.; Rohr, F.; Levy, H.L. Metabolomic changes demonstrate reduced bioavailability of tyrosine and altered metabolism of tryptophan via the kynurenine pathway with ingestion of medical foods in phenylketonuria. Mol. Genet. MeTab. 2017, 121, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Stroup, B.M.; Ney, D.M.; Murali, S.G.; Rohr, F.; Gleason, S.T.; Van Calcar, S.C.; Levy, H.L. Metabolomic insights into the nutritional status of adults and adolescents with phenylketonuria consuming a low-phenylalanine diet in combination with amino acid and glycomacropeptide medical foods. J. Nutr. MeTab. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.; Green, S.; Higgins, J.P. Defining the review question and developing criteria for including studies. Cochrane Handb. Syst. Rev. Interv. Cochrane Book Ser. 2008, 81–94. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, M.; Trefz, F.; Muntau, A.C.; Feillet, F.; van Spronsen, F.J.; Burlina, A.; Bélanger-Quintana, A.; Gizewska, M.; Gasteyger, C.; Bettiol, E.; et al. Fluctuations in phenylalanine concentrations in phenylketonuria: A review of possible relationships with outcomes. Mol. Genet. MeTable 2013, 110, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.H.; Singh, R.H. Protein substitute for children and adults with phenylketonuria. Cochrane Database Syst. Rev. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.H.; Rohr, F.; Frazier, D.; Cunningham, A.; Mofidi, S.; Ogata, B.; Splett, P.L.; Moseley, K.; Huntington, K.; Acosta, P.B.; et al. Recommendations for the nutrition management of phenylalanine hydroxylase deficiency. Genet. Med. 2014, 16, 121–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arihan, O.; Wernly, B.; Lichtenauer, M.; Franz, M.; Kabisch, B.; Muessig, J.; Masyuk, M.; Lauten, A.; Schulze, P.C.; Hoppe, U.C.; et al. Blood Urea Nitrogen (BUN) is independently associated with mortality in critically ill patients admitted to ICU. PLoS ONE 2018, 13, e0191697. [Google Scholar] [CrossRef] [PubMed]
- Pena, M.J.; Rocha, J.C.; Borges, N. Amino acids, glucose metabolism and clinical relevance for phenylketonuria management. Ann. Nutr. Disord. Ther. 2015, 2, 1026. [Google Scholar]
- Proserpio, C.; Pagliarini, E.; Zuvadelli, J.; Paci, S.; Re Dionigi, A.; Banderali, G.; Cattaneo, C.; Verduci, E. Exploring drivers of liking of low-phenylalanine products in subjects with phenyilketonuria using check-all-that-apply method. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Barton, S. Which clinical studies provide the best evidence? The best RCT still trumps the best observational study. BMJ 2000, 321, 255–256. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year (Ref.) | Country | Study Design | Sample Size (N) | Age (Range)—Years | Gender | PKU Phenotype |
|---|---|---|---|---|---|---|
| Lim et al. 2007 [10] | United States | Cross-sectional study | 49 | 12–42 | N/A | N/A |
| van Calcar et al. 2009 [17] | United States | Crossover clinical study | 11 | 23 ± 7 (11–31) | 4 F; 7 M | 10 classical; 1 variant form |
| MacLeod et al. 2010 [20] | United States | Crossover clinical study | 11 | 23 ± 7 (11–31) | 4 F; 7 M | 11 classical |
| Zaki et al. 2016 [21] | Egypt | Clinical study | 10 | 6.73 [5.02; 11.79] | 4 F; 6 M | 10 classical |
| Ney et al. 2016 [22] | United States | Randomised crossover clinical trial | 30 | 15–49 | 18 F; 12 M | 20 classical; 10 variant form |
| Daly et al. 2017 [23] | United Kingdom | Clinical study | 22 | 11 (6–16) | 9 F; 13 M | N/A |
| Pinto et al. 2017 [24] | Portugal | Retrospective, longitudinal study | 11 | 27 ± 10 (13–42) | 8 F; 3 M | 6 classical; 4 mild; 1 HPA |
| Ahring et al. 2018 [18] | Denmark | Randomised crossover clinical trial | 8 1 | 33.25 ± 11.21 (15–48) | 7 F; 1 M | 8 classical |
| Author, Year (Ref.) | Length of Intervention | Intervention | Comparator | Primary Outcome | Secondary Outcomes |
|---|---|---|---|---|---|
| Lim et al. 2007 [10] | N/A | GMP-AAs | AAs | N/A | Acceptability * |
| van Calcar et al. 2009 [17] | Two treatments for four days each: AAs (days 1–4) and GMP-AAs (days 5–8) | Period I—0% GMP-AAs; Period II—100% GMP-AAs; 11 patients | Period I—100% AAs; Period II—0% AAs; 11 patients | Blood Phe | Blood Tyr BUN Glucose Acceptability * |
| MacLeod et al. 2010 [20] | Two treatments for four days each: AAs (days 1–4) and GMP-AAs (days 5–8) | Period I—0% GMP-AAs; Period II—100% GMP-AAs; 11 patients | Period I—100% AAs; Period II—0% AAs; 11 patients | Blood Phe | Blood Tyr Acceptability * |
| Zaki et al. 2016 [21] | Eighteen weeks | Period I—50% GMP; Period II—0% GMP; 10 patients | Period I—50% AAs; Period II—100% AAs; 10 patients | Blood Phe | Urea/BUN Acceptability * |
| Ney et al. 2016 [22] | Eleven weeks | Three weeks each of GMP-AAs or AAs; 15 patients in each arm | Three weeks each of GMP-AAs or AAs; 15 patients in each arm | Blood Phe | Blood Tyr BUN Glucose Acceptability * |
| Daly et al. 2017 [23] | Twenty-six weeks | 12 patients—GMP-AAs | 9 patients—AAs | Blood Phe | Blood Tyr Acceptability * |
| Pinto et al. 2017 [24] | Twenty months | 11 patients—GMP-AAs | 11 patients—AAs | Blood Phe | Blood Tyr Urea/BUN Glucose |
| Ahring et al. 2018 [18] | Four visits, analysis at five timepoints (0, 15, 30, 60, 120 and 240 min) | 6 patients tested the four DMs (DM1 = GMP; DM3 = GMP + AAs) | 6 patients tested the four DMs [DM2 = AAs (equivalent amino acid profile to DM1); DM4 = AAs (equivalent amino acid profile to DM3 but without Phe)] | Blood Phe | Blood Tyr BUN Glucose Acceptability * |
| Author, Year (Ref.) | Method | Number of Items Evaluated | Type of Items Evaluated | Main Findings |
|---|---|---|---|---|
| Lim et al. 2007 [10] | Five-point hedonic scale 1 | Seven products (five GMP-AAs and two AAs) | GMP-AAs (strawberry pudding, strawberry fruit leather, chocolate beverage, snack crackers, orange sports beverage) and AAs (crackers, chocolate beverage) | Decreasing order of overall acceptability—strawberry pudding (4.2 ± 0.9), snack cracker (3.6 ± 1.4), strawberry fruit leather (3.4 ± 1.0), chocolate beverage (3.3 ± 1.0), orange sports beverage (3.3 ± 1.1), AAs in crackers (2.9 ± 1.3), AAs in a chocolate beverage (2.5 ± 1.4) |
| van Calcar et al. 2009 [17] | No methodology described | Six GMP-AAs and subject’s usual AAs | GMP-AAs (orange-flavoured sports beverage, chocolate-flavoured or caramel-flavoured beverage, chocolate or strawberry pudding, cinnamon crunch bar) and subject’s usual AAs | After consuming the GMP-AAs diet for four days, 10 of 11 subjects claimed that the GMP-AAs products were superior in sensory qualities to their usual AAs. Moreover, at the end of the study, 6 of 7 adults expressed a strong preference to consume GMP-AAs products rather than their usual AAs |
| MacLeod et al. 2010 [20] | Four questions, motivation-to-eat VAS questionnaires | Six GMP-AAs and subject’s usual AAs | GMP-AAs (orange-flavoured sports beverage, chocolate-flavoured or caramel-flavoured beverage, chocolate or strawberry pudding, cinnamon crunch bar) and subject’s usual AAs | The motivation-to-eat VAS profiles were not significantly different at any timepoint between the AAs (day 4) and GMP-AAs (day 8) |
| Zaki et al. 2016 [21] | Questionnaire | N/A | N/A | Throughout the study, all patients preferred the diet supplemented with GMP over the classical AAs due to better taste and satiety |
| Ney et al., 2016 [22] | Six-question survey and six-point scale 2 | Fifteen AAs and N/A the exact number of GMP-AAs | N/A | AAs vs GMP-AAs (1) 3.97 ± 0.24 vs 4.90 ± 0.18, P = 0.001 (2) 4.79 ± 0.22 vs 5.07 ± 0.16, P = 0.366 (3) 4.50 ± 0.25 vs 4.86 ± 0.19, P = 0.172 (4) 4.19 ± 0.18 vs 4.69 ± 0.16, P = 0.019 (5) 3.83 ± 0.26 vs 4.72 ± 0.27, P = 0.003 (6) 3.34 ± 0.31 vs 4.47 ± 0.23, P = 0.001 |
| Daly et al., 2017 [23] | Acceptability questionnaires (taste, smell, texture, mouthfeel and overall acceptability) | N/A | In the GMP-AAs group, subjects took a berry flavoured GMP-AAs powder (35 g sachet = 20 g protein equivalent) which subjects prepared with water or low-protein milk | All of the subjects in the GMP-AAs group described the protein substitute as acceptable, with improved taste, mouth feel, texture, and smell compared to their conventional AAs |
| Pinto et al., 2017 [24] | N/A | N/A | N/A | N/A |
| Ahring et al., 2018 [18] | Two questions—VAS 3 | Four DMs | DM1 = GMP; DM2 = AAs (equivalent amino acid profile as DM1); DM3 = GMP + AAs (0.16 g Phe/100 g amino acids present in GMP); DM4 = AAs (equivalent amino acid profile as DM3 but without Phe) | 1) DM1: 36 ± 18, DM2: 41 ± 16, DM3: 28 ± 27, DM4: 35 ± 30); 2) DM1: 34 ± 31, DM2: 44 ± 22, DM3: 36 ± 28, DM4: 26 ± 22); all comparisons (DM1 and DM2, DM3 and DM4, DM3 to DM1 and DM2, respectively) were statistically insignificant |
| Outcomes | Number of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision |
|---|---|---|---|---|---|---|
| Blood Phe | 2 | Randomised trials | Not serious | Serious | Not serious | Very serious |
| 5 | Observational studies | Not serious | Serious | Not serious | Very serious | |
| Blood Tyr | 2 | Randomised trials | Not serious | Serious | Not serious | Very serious |
| 4 | Observational studies | Not serious | Serious | Not serious | Very serious | |
| BUN | 2 | Randomised trials | Not serious | Serious | Not serious | Very serious |
| 3 | Observational studies | Not serious | Serious | Not serious | Very serious | |
| Glucose | 2 | Randomised trials | Not serious | Serious | Not serious | Very serious |
| 4 | Observational studies | Not serious | Serious | Not serious | Very serious | |
| Acceptability | 2 | Randomised trials | Not serious | Serious | Not serious | Very serious |
| 5 | Observational studies | Not serious | Serious | Not serious | Very serious |
| Author, year (Ref.) | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Domain 6 | Domain 7 | Overall |
|---|---|---|---|---|---|---|---|---|
| Lim et al. 2007 * [10] | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| van Calcar et al. 2009 [17] | 3 | 3 | 1 | 1 | 1 | 1 | 1 | 2—Moderate |
| MacLeod et al. 2010 [20] | 3 | 3 | 1 | 1 | 1 | 1 | 1 | 2—Moderate |
| Zaki et al. 2016 [21] | 3 | 3 | 1 | 1 | 1 | 3 | 3 | 2—Moderate |
| Daly et al. 2017 [23] | 3 | 3 | 1 | 1 | 1 | 1 | 1 | 2—Moderate |
| Pinto et al. 2017 [24] | 3 | 3 | 1 | 1 | 1 | 1 | 1 | 2—Moderate |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pena, M.J.; Pinto, A.; Daly, A.; MacDonald, A.; Azevedo, L.; Rocha, J.C.; Borges, N. The Use of Glycomacropeptide in Patients with Phenylketonuria: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1794. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111794
Pena MJ, Pinto A, Daly A, MacDonald A, Azevedo L, Rocha JC, Borges N. The Use of Glycomacropeptide in Patients with Phenylketonuria: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(11):1794. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111794
Chicago/Turabian StylePena, Maria João, Alex Pinto, Anne Daly, Anita MacDonald, Luís Azevedo, Júlio César Rocha, and Nuno Borges. 2018. "The Use of Glycomacropeptide in Patients with Phenylketonuria: A Systematic Review and Meta-Analysis" Nutrients 10, no. 11: 1794. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111794