Vitamin D Status and Seasonal Variation among Danish Children and Adults: A Descriptive Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Description
2.2. Measurement of 25-hydroxyvitamin D (25(OH)D) in Serum Samples
2.3. Questionnaire Information on Supplement Use
2.4. Descriptive Statistics
3. Results
3.1. Overall Status Stratified by Sex and Age
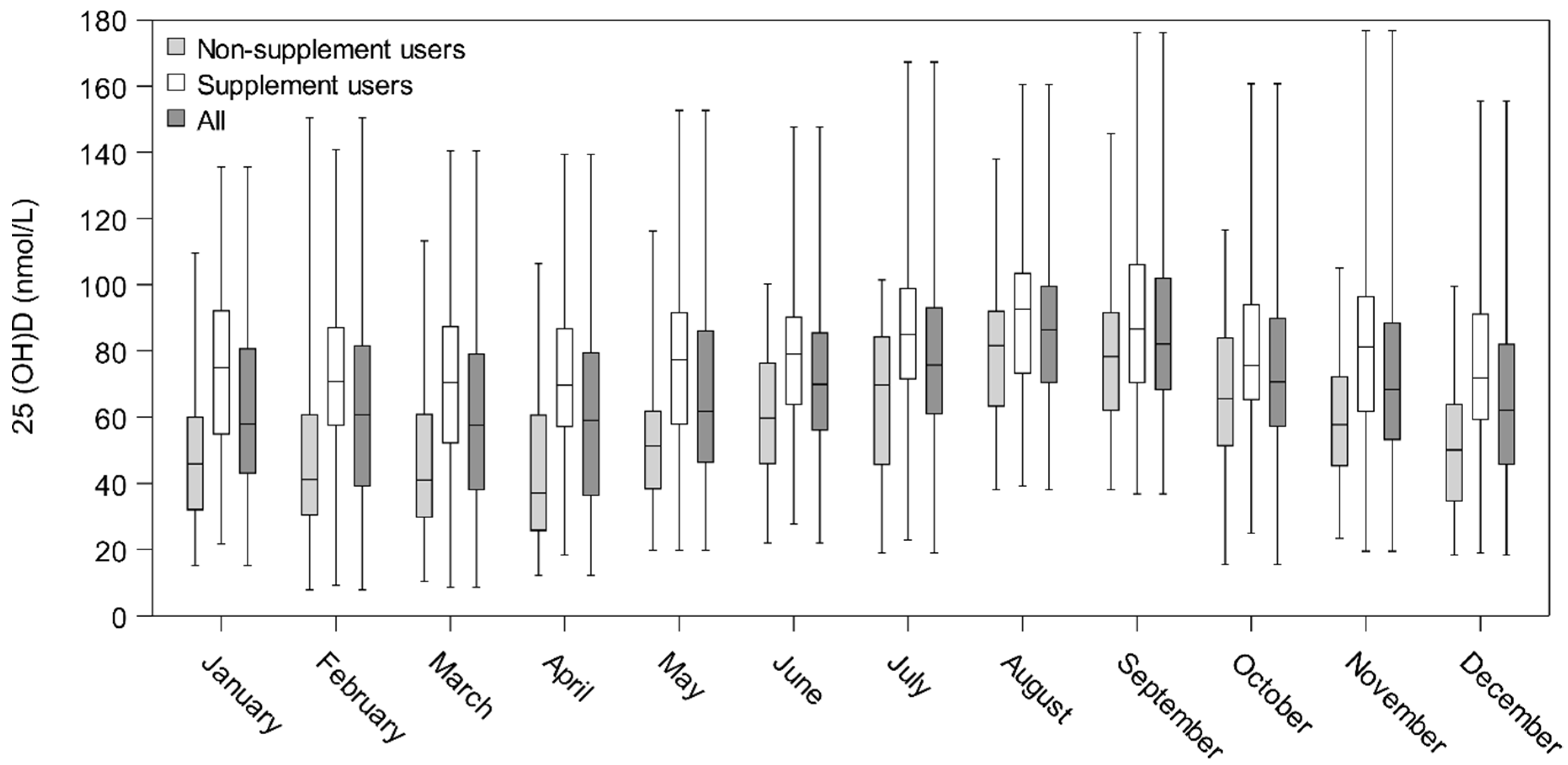
3.2. Seasonal Variation of 25(OH)D Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jacobs, E.T.; Kohler, L.N.; Kunihiro, A.G.; Jurutka, P.W. Vitamin D and colorectal, breast, and prostate cancers: A review of the epidemiological evidence. J. Cancer 2016, 7, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Mpandzou, G.; Ait Ben Haddou, E.; Regragui, W.; Benomar, A.; Yahyaoui, M. Vitamin D deficiency and its role in neurological conditions: A review. Rev. Neurol. 2016, 172, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Hamid, Z.T. The role of vitamin D in diabetes and cardiovascular disease: An updated review of the literature. Dis. Markers 2015, 580474. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Boniol, M.; Haukka, J.; Byrnes, G.; Cox, B.; Sneyd, M.J.; Mullie, P.; Autier, P. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int. J. Cancer 2011, 128, 1414–1424. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Shao, X.; Yao, Y.; Xu, L.; Chang, L.; Jiang, Z.; Lin, Z. Positive association between circulating 25-hydroxyvitamin D levels and prostate cancer risk: New findings from an updated meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Kimlin, M.G. Geographic location and vitamin D synthesis. Mol. Aspects Med. 2008, 29, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.J.; Curtis, E.M.; Davies, J.H.; Cooper, C.; Harvey, N.C. Seasonal variation in Internet searches for vitamin D. Arch. Osteoporos. 2017, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.; Gardner, K.; Taylor, W.; Marks, E.; Goodson, N. Vitamin D assessment in primary care: Changing patterns of testing. Lond. J. Prim. Care 2015, 7, 15–22. [Google Scholar] [CrossRef]
- Danish Health Authority. Recommendations for Vitamin D (in Danish). Available online: https://www.sst.dk/da/sundhed-og-livsstil/ernaering/d-vitamin (accessed on 23 October 2018).
- Durup, D.; Jorgensen, H.L.; Christensen, J.; Schwarz, P.; Heegaard, A.M.; Lind, B. A reverse J-shaped association of all-cause mortality with serum 25-hydroxyvitamin D in general practice: The CopD study. J. Clin. Endocrinol. Metab. 2012, 97, 2644–2652. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.; Brot, C.; Jakobsen, J.; Mejborn, H.; Molgaard, C.; Skovgaard, L.T.; Trolle, E.; Tetens, I.; Ovesen, L. Seasonal changes in vitamin D status among Danish adolescent girls and elderly women: The influence of sun exposure and vitamin D intake. Eur. J. Clin. Nutr. 2013, 67, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.; Molgaard, C.; Skovgaard, L.T.; Brot, C.; Cashman, K.D.; Jakobsen, J.; Lamberg-Allardt, C.; Ovesen, L. Pakistani immigrant children and adults in Denmark have severely low vitamin D status. Eur. J. Clin. Nutr. 2008, 62, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Brot, C.; Vestergaard, P.; Kolthoff, N.; Gram, J.; Hermann, A.P.; Sorensen, O.H. Vitamin D status and its adequacy in healthy Danish perimenopausal women: relationships to dietary intake, sun exposure and serum parathyroid hormone. Br. J. Nutr. 2001, 86 (Suppl. 1), S97–S103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molgaard, C.; Larnkjaer, A.; Cashman, K.D.; Lamberg-Allardt, C.; Jakobsen, J.; Michaelsen, K.F. Does vitamin D supplementation of healthy Danish Caucasian girls affect bone turnover and bone mineralization? Bone 2010, 46, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.A.; Damsgaard, C.T.; Dalskov, S.M.; Sorensen, L.B.; Hjorth, M.F.; Ritz, C.; Kjolbaek, L.; Andersen, R.; Tetens, I.; Krarup, H.; et al. Vitamin D status and its determinants during autumn in children at northern latitudes: A cross-sectional analysis from the optimal well-being, development and health for Danish children through a healthy New Nordic Diet (OPUS) School Meal Study. Br. J. Nutr. 2016, 115, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Tonnesen, R.; Hovind, P.H.; Jensen, L.T.; Schwarz, P. Determinants of vitamin D status in young adults: Influence of lifestyle, sociodemographic and anthropometric factors. BMC Public Health 2016, 16, 385. [Google Scholar] [CrossRef] [PubMed]
- Madsen, K.H.; Rasmussen, L.B.; Mejborn, H.; Andersen, E.W.; Molgaard, C.; Nissen, J.; Tetens, I.; Andersen, R. Vitamin D status and its determinants in children and adults among families in late summer in Denmark. Br. J. Nutr. 2014, 112, 776–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thuesen, B.; Husemoen, L.; Fenger, M.; Jakobsen, J.; Schwarz, P.; Toft, U.; Ovesen, L.; Jorgensen, T.; Linneberg, A. Determinants of vitamin D status in a general population of Danish adults. Bone 2012, 50, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Tjonneland, A.; Koster, B.; Brot, C.; Andersen, R.; Lundqvist, M.; Christensen, J.; Olsen, A. Sun exposure guidelines and serum vitamin D status in Denmark: The statusD study. Nutrients 2016, 8, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, W.D.; Milan, A.M. Vitamin D assays: Past and present debates, difficulties, and developments. Calcif. Tissue Int. 2013, 92, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Roth, H.J.; Schmidt-Gayk, H.; Weber, H.; Niederau, C. Accuracy and clinical implications of seven 25-hydroxyvitamin D methods compared with liquid chromatography-tandem mass spectrometry as a reference. Ann. Clin. Biochem. 2008, 45, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Skrabakova, Z.; Kiely, M.; Lamberg-Allardt, C.; Durazo-Arvizu, R.A.; Sempos, C.T.; Koskinen, S.; Lundqvist, A.; Sundvall, J.; et al. Standardizing serum 25-hydroxyvitamin D data from four Nordic population samples using the Vitamin D Standardization Program protocols: Shedding new light on vitamin D status in Nordic individuals. Scand. J. Clin. Lab. Investig. 2015, 75, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Schottker, B.; Jansen, E.H.; Haug, U.; Schomburg, L.; Kohrle, J.; Brenner, H. Standardization of misleading immunoassay based 25-hydroxyvitamin D levels with liquid chromatography tandem-mass spectrometry in a large cohort study. PLoS ONE 2012, 7, e48774. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.J.; Saha, S.; Burne, T.H.; Eyles, D.W. A systematic review of the association between common single nucleotide polymorphisms and 25-hydroxyvitamin D concentrations. J. Steroid Biochem. Mol. Biol. 2010, 121, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Nissen, J.; Rasmussen, L.B.; Ravn-Haren, G.; Andersen, E.W.; Hansen, B.; Andersen, R.; Mejborn, H.; Madsen, K.H.; Vogel, U. Common variants in CYP2R1 and GC genes predict vitamin D concentrations in healthy Danish children and adults. PLoS ONE 2014, 9, e89907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissen, J.; Vogel, U.; Ravn-Haren, G.; Andersen, E.W.; Madsen, K.H.; Nexo, B.A.; Andersen, R.; Mejborn, H.; Bjerrum, P.J.; Rasmussen, L.B.; et al. Common variants in CYP2R1 and GC genes are both determinants of serum 25-hydroxyvitamin D concentrations after UVB irradiation and after consumption of vitamin D(3)-fortified bread and milk during winter in Denmark. Am. J. Clin. Nutr. 2015, 101, 218–227. [Google Scholar] [CrossRef] [PubMed]
- DTU-Fødevareinstituttet. D-vitamin. Opdatering af Videnskabelig Evidens for Sygdomsforebyggelse og Anbefalinger. 2010. Available online: http://www.food.dtu.dk/Publikationer/Ernaering-og-kostvaner/Kostraad_og_naeringsstofanbefalinger (accessed on 28 October 2018). (In Danish).
- Lucas, R.; Neale, R. What is the optimal level of vitamin D?—Separating the evidence from the rhetoric. Aust. Fam. Physician 2014, 43, 119–122. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Age in Years by Sex (n) | Spring | Autumn | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | SU a | NSU b | All | SU a | NSU b | |||||
| Median (5–95%) | n | Median (5–95%) | n | Median (5–95%) | Median (5–95%) | n | Median (5–95%) | n | Median (5–95%) | |
| Boys | ||||||||||
| 2–5 (n = 36) | 56 (24–98) | 18 | 63 (25–107) | 18 | 37 (24–94) | 75 (48–108) | 14 | 82 (60–122) | 22 | 73 (48–95) |
| 6–14 (n = 175) | 44 (20–82) | 63 | 54 (34–89) | 112 | 38 (19–72) | 67 (41–97) | 44 | 70 (50–98) | 131 | 65 (40–95) |
| 15–17 (n = 53) | 29 (10–82) | 11 | 55 (27–89) | 42 | 24 (10–61) | 61 (39–99) | 7 | 74 (44–102) | 46 | 58 (39–92) |
| Total boys (n = 264) | 43 (19–82) | 92 | 56 (33–92) | 172 | 35 (16–74) | 67 (40–98) | 65 | 73 (50–101) | 199 | 65 (39–95) |
| Men | ||||||||||
| 18–29 (n = 118) | 38 (17–73) | 24 | 46 (32–77) | 94 | 35 (16–70) | 68 (31–105) | 21 | 77 (49–102) | 97 | 66 (30–109) |
| 30–39 (n = 209) | 37 (15–84) | 51 | 53 (26–95) | 158 | 33 (14–75) | 66 (38–106) | 44 | 75 (42–103) | 165 | 64 (36–98) |
| 40–49 (n = 271) | 40 (18–83) | 82 | 63 (32–91) | 189 | 33 (17–66) | 67 (38–106) | 62 | 74 (41–121) | 209 | 66 (36–101) |
| 50–59 (n = 225) | 47 (19–88) | 71 | 65 (36–102) | 154 | 40 (19–84) | 70 (36–108) | 65 | 72 (42–108) | 160 | 69 (34–107) |
| 60+ (n = 225) | 56 (22–96) | 94 | 67 (37–99) | 131 | 41 (18–94) | 73 (41–111) | 87 | 79 (45–108) | 138 | 69 (36–116) |
| Total men (n = 1048) | 43 (18–87) | 322 | 63 (32–97) | 726 | 36 (16–80) | 69 (37–105) | 279 | 74 (41–109) | 769 | 66 (36–102) |
| Girls | ||||||||||
| 2–5 (n = 39) | 59 (20–101) | 24 | 67 (41–101) | 15 | 30 (18–83) | 72 (50–106) | 17 | 78 (58–106) | 22 | 66 (49–94) |
| 6–14 (n = 164) | 43 (17–74) | 52 | 52 (29–84) | 112 | 39 (16–67) | 67 (39–96) | 55 | 68 (44–96) | 109 | 65 (33–87) |
| 15–17 (n = 60) | 47 (19–84) | 11 | 63 (48–112) | 49 | 38 (18–84) | 67 (39–117) | 13 | 78 (33–121) | 47 | 65 (40–108) |
| Total girls (n = 263) | 45 (18–84) | 87 | 57 (33–101) | 176 | 38 (17–71) | 68 (40–102) | 85 | 72 (49–103) | 178 | 65 (38–102) |
| Women | ||||||||||
| 18–29 (n = 233) | 49 (20–102) | 66 | 67 (38–121) | 167 | 43 (17–88) | 76 (43–122) | 50 | 78 (43–122) | 183 | 75 (44–122) |
| 30–39 (n = 280) | 46 (20–99) | 118 | 66 (29–107) | 162 | 35 (17–85) | 69 (41–117) | 99 | 76 (47–118) | 181 | 65 (38–114) |
| 40–49 (n = 384) | 49 (19–94) | 170 | 64 (33–103) | 214 | 40 (16–82) | 71 (37–109) | 147 | 75 (42–109) | 237 | 67 (35–110) |
| 50–59 (n = 335) | 63 (23–111) | 159 | 73 (42–115) | 176 | 50 (19–90) | 77 (40–117) | 139 | 82 (47–127) | 196 | 74 (34–116) |
| 60+ (n = 285) | 71 (24–109) | 165 | 81 (47–117) | 120 | 51 (21–98) | 81 (45–125) | 146 | 86 (58–129) | 139 | 73 (37–118) |
| Total women (n = 1517) | 57 (21–103) | 678 | 72 (34–114) | 839 | 43 (18–88) | 74 (40–118) | 581 | 81 (47–123) | 936 | 70 (37–116) |
| 25(OH)D (nmol/L) Range in Spring Percentage Distribution within Each Age Group | 25(OH)D (nmol/L) Range in Autumn Percentage Distribution within Each Age Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age in Years by Sex (n) | ||||||||||
| <12.5 | 12.5–<25 | 25–<50 | 50–<75 | >75 | <12.5 | 12.5–<25 | 25–<50 | 50–<75 | >75 | |
| Boys | ||||||||||
| 2–5 (n = 36) | 0 | 11 | 33 | 36 | 20 | 0 | 0 | 6 | 44 | 50 |
| 6–14 (n = 175) | 0 | 14 | 46 | 34 | 6 | 0 | 1 | 14 | 57 | 28 |
| 15–17 (n = 53) | 7 | 36 | 38 | 11 | 8 | 0 | 0 | 26 | 53 | 21 |
| Total boys (n =264) | 2 | 18 | 42 | 30 | 8 | 0 | 0 | 16 | 54 | 30 |
| Men | ||||||||||
| 18–29 (n = 118) | 0 | 22 | 46 | 28 | 4 | 0 | 1 | 23 | 37 | 39 |
| 30–39 (n = 209) | 2 | 20 | 50 | 18 | 10 | 0 | 1 | 20 | 47 | 32 |
| 40–49 (n = 271) | 1 | 16 | 51 | 24 | 8 | 0 | 1 | 19 | 46 | 34 |
| 50–59 (n = 225) | 2 | 8 | 45 | 32 | 13 | 0 | 2 | 14 | 48 | 36 |
| 60+ (n = 225) | 1 | 7 | 35 | 37 | 20 | 0 | 0 | 12 | 45 | 43 |
| Total men (n = 1048) | 1 | 14 | 45 | 28 | 12 | 0 | 1 | 17 | 45 | 37 |
| Girls | ||||||||||
| 2–5 (n = 39) | 0 | 5 | 36 | 33 | 26 | 0 | 0 | 5 | 54 | 41 |
| 6–14 (n = 164) | 1 | 9 | 56 | 29 | 5 | 0 | 1 | 13 | 58 | 28 |
| 15–17 (n = 60) | 2 | 10 | 43 | 35 | 10 | 0 | 0 | 17 | 51 | 32 |
| Total girls (n = 263) | 1 | 9 | 50 | 31 | 9 | 0 | 1 | 12 | 56 | 31 |
| Women | ||||||||||
| 18–29 (n = 233) | 1 | 11 | 40 | 30 | 18 | 0 | 1 | 11 | 37 | 51 |
| 30–39 (n = 280) | 1 | 12 | 42 | 25 | 20 | 0 | 1 | 14 | 49 | 36 |
| 40–49 (n = 384) | 1 | 10 | 40 | 31 | 18 | 0 | 0 | 15 | 45 | 40 |
| 50–59 (n = 335) | 0 | 5 | 27 | 37 | 31 | 0 | 1 | 11 | 34 | 54 |
| 60+ (n = 285) | 0 | 6 | 18 | 31 | 45 | 0 | 0 | 8 | 33 | 59 |
| Total women (n = 1517) | 1 | 9 | 33 | 31 | 26 | 0 | 1 | 12 | 39 | 48 |
| All | Non-Supplement Users a | |||||
|---|---|---|---|---|---|---|
| Spring | Spring | |||||
| <25 nmol/L | 25–50 nmol/L | >50 nmol/L | <25 nmol/L | 25–50 nmol/L | >50 nmol/L | |
| Autumn | Adults (n = 2565; 18–69 years) | Adults (n = 1390) | ||||
| <25 nmol/L | 1% | 0% | 0% | 1% | 0% | 0% |
| 25–50 nmol/L | 6% | 7% | 1% | 10% | 8% | 1% |
| >50 nmol/L | 5% | 31% | 49% | 8% | 43% | 29% |
| Autumn | Children (n = 527; 2–17 years) | Children (n = 308) | ||||
| <25 nmol/L | 0% | 0% | 0% | 1% | 0% | 0% |
| 25–50 nmol/L | 8% | 6% | 1% | 12% | 6% | 0% |
| >50 nmol/L | 7% | 40% | 38% | 10% | 49% | 22% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, L.; Tjønneland, A.; Køster, B.; Brot, C.; Andersen, R.; Cohen, A.S.; Frederiksen, K.; Olsen, A. Vitamin D Status and Seasonal Variation among Danish Children and Adults: A Descriptive Study. Nutrients 2018, 10, 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111801
Hansen L, Tjønneland A, Køster B, Brot C, Andersen R, Cohen AS, Frederiksen K, Olsen A. Vitamin D Status and Seasonal Variation among Danish Children and Adults: A Descriptive Study. Nutrients. 2018; 10(11):1801. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111801
Chicago/Turabian StyleHansen, Louise, Anne Tjønneland, Brian Køster, Christine Brot, Rikke Andersen, Arieh S. Cohen, Kirsten Frederiksen, and Anja Olsen. 2018. "Vitamin D Status and Seasonal Variation among Danish Children and Adults: A Descriptive Study" Nutrients 10, no. 11: 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111801