Dietary Intakes and Dietary Quality during Pregnancy in Women with and without Gestational Diabetes Mellitus - A Norwegian Longitudinal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
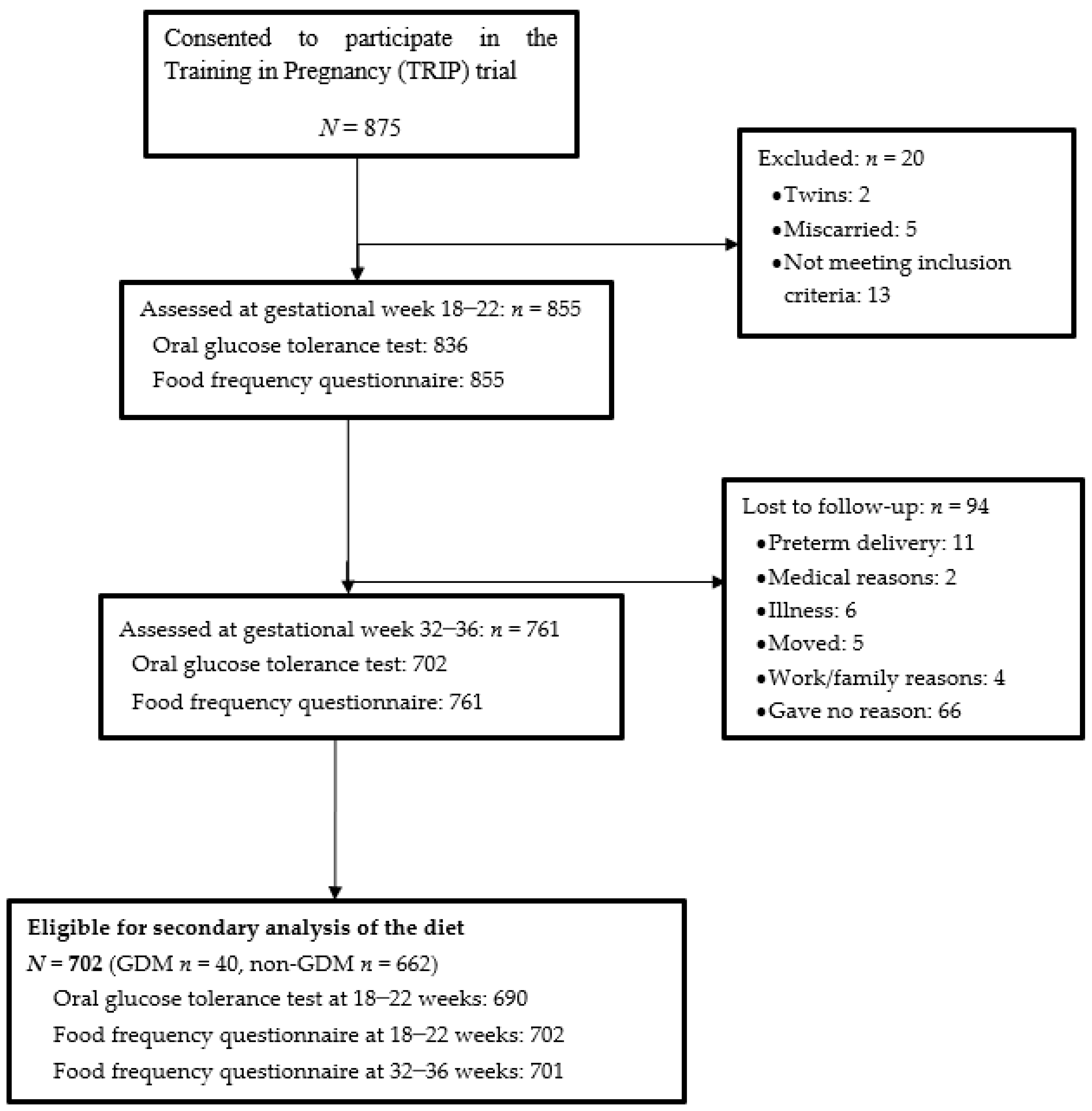
3.1. Study Population
3.2. Intakes of Foods and Beverages during Pregnancy
3.3. Intakes of Energy and Nutrients during Pregnancy
3.4. Dietary Intakes in Relation to Dietary Recommendations
3.5. Variability in Glucose Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997, 20, 1183–1197. [Google Scholar]
- Buchanan, T.A. Pancreatic B-cell defects in gestational diabetes: Implications for the pathogenesis and prevention of type 2 diabetes. J. Clin. Endocrinol. Metab. 2001, 86, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Nolan, C.J. Controversies in gestational diabetes. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M. Obesity, insulin resistance, and pregnancy outcome. Reproduction 2010, 140, 365–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCane, D.R.; Hod, M.; McIntyre, H.D. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Beharier, O.; Shoham-Vardi, I.; Pariente, G.; Sergienko, R.; Kessous, R.; Baumfeld, Y.; Szaingurten-Solodkin, I.; Sheiner, E. Gestational Diabetes Mellitus is a Significant Risk Factor for Long Term Maternal Renal Disease. J. Clin. Endocrinol. Metab. 2015, 100, 1412–1416. [Google Scholar] [CrossRef] [PubMed]
- Engeland, A.; Bjorge, T.; Daltveit, A.K.; Skurtveit, S.; Vangen, S.; Vollset, S.E.; Furu, K. Risk of diabetes after gestational diabetes and preeclampsia. A registry-based study of 230,000 women in Norway. Eur. J. Epidemiol. 2011, 26, 157–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coustan, R.D. Diabetes Mellitus in Pregnancy: Screening and Diagnosis. 2017. Available online: https://www.uptodate.com/contents/diabetes-mellitus-in-pregnancy-screening-and-diagnosis (accessed on 12 November 2017).
- Schoenaker, D.A.; Mishra, G.D. The Role of Energy, Nutrients, Foods, and Dietary Patterns in the Development of Gestational Diabetes Mellitus: A Systematic Review of Observational Studies. Diabetes Care 2016, 39, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C. Associations of Diet and Physical Activity with Risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Saldana, T.M.; Siega-Riz, A.M.; Adair, L.S. Effect of macronutrient intake on the development of glucose intolerance during pregnancy. Am. J. Clin. Nutr. 2004, 79, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, C.; Frederick, I.O.; Zhang, C.; Sorensen, T.K.; Enquobahrie, D.A.; Williams, M.A. Risk of gestational diabetes mellitus in relation to maternal egg and cholesterol intake. Am. J. Epidemiol. 2011, 173, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Zhang, C.; Gelaye, B.; Enquobahrie, D.A.; Frederick, I.O.; Williams, M.A. Gestational diabetes mellitus in relation to maternal dietary heme iron and nonheme iron intake. Diabetes Care 2011, 34, 1564–1569. [Google Scholar] [CrossRef] [PubMed]
- Stafne, S.N.; Salvesen, K.A.; Romundstad, P.R.; Eggebo, T.M.; Carlsen, S.M.; Morkved, S. Regular exercise during pregnancy to prevent gestational diabetes: A randomized controlled trial. Obstet. Gynecol. 2012, 119, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Elvebakken, K.T.; Thommessen, M. Nutrition in Pregnancy; Social- and Health Directorate: Oslo, Norway, 2005; pp. 1–11. [Google Scholar]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.D.; Hod, M.; Kitzmiler, J.L. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Solvoll, K.; Drevon, C.A. Very-long-chain n-3 fatty acids as biomarkers for intake of fish and n-3 fatty acid concentrates. Am. J. Clin. Nutr. 1996, 64, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Solvoll, K.; Johansson, L.R.; Salminen, I.; Aro, A.; Drevon, C.A. Evaluation of a food frequency questionnaire with weighed records, fatty acids, and alpha-tocopherol in adipose tissue and serum. Am. J. Epidemiol. 1999, 150, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Veierod, M.B.; Johansson, L.; Sakhi, A.; Solvoll, K.; Drevon, C.A. Evaluation of three dietary assessment methods and serum biomarkers as measures of fruit and vegetables intake, using the method of triads. Br. J. Nutr. 2005, 93, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Blomhoff, R.; Andersen, L.F.; Iversen, P.O.; Johansson, R.; Smeland, S. (Eds.) Kostråd for å fremme folkehelsen og forebygge kroniske sykdommer: Metodologi og vitenskapelig kunnskapsbidrag; Nasjonalt råd for ernæring. Norwegian Directorate of Health: Oslo, Norway, 2011; pp. 7–284, IS-1881. Available online: https://helsedirektoratet.no/Lists/Publikasjoner/Attachments/400/Kostrad-for-a-fremme-folkehelsen-og-forebygge-kroniske-sykdommer-metodologi-og-vitenskapelig-kunnskapsgrunnlag-IS-1881.pdf (accessed on 3 October 2018).
- World Cancer Research Fund / American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. AICR: Washington, DC, USA, 2007. Available online: http://www.aicr.org/assets/docs/pdf/reports/Second_Expert_Report.pdf (accessed on 1 May 2018).
- Nordic Nutrition Recommendations 2012—Integrating Nutrition and Physical Activity. Nordic Counsil of Ministers: Copenhagen, Denmark, 2014, 5th ed. pp. 19–627. Available online: http://norden.diva-portal.org/smash/record.jsf?pid=diva2%3A704251&dswid=mainwindow (accessed on 4 April 2018).
- Norwegian Food Safety Authority. The Food Composition Table. 2011. Available online: http://www.matportalen.no/kontaktoss/about_us (accessed on 5 April 2018).
- von Ruesten, A.; Brantsaeter, A.L.; Haugen, M.; Meltzer, H.M.; Mehlig, K.; Winkvist, A.; Lissner, L. Adherence of pregnant women to Nordic dietary guidelines in relation to postpartum weight retention: Results from the Norwegian Mother and Child Cohort Study. BMC Public Health 2014, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, M.K.; Stafne, S.N.; Romundstad, P.R.; Mørkved, S.; Salvesen, K.; Helvik, A.S.; Syversen, U. Variation of 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels during pregnancy: A Norwegian longitudinal study. PLoS ONE 2018, 13, e0195041. [Google Scholar]
- Brembeck, P.; Winkvist, A.; Olausson, H. Determinants of vitamin D status in pregnant fair-skinned women in Sweden. Br. J. Nutr. 2013, 110, 856–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klovning, A.; Backe, B.; Eide, B.I.; Blix, E.; Aarseth, J.; Mathiesen, M.R.; Holan, S.; Roland, B. Guidelines for Antenatal Care; Social- and Health Directorate: Oslo, Norway, 2005. [Google Scholar]
- Norwegian Institute of Public Health. Medical Birth Registry of Norway. 2016. Available online: http://statistikkbank.fhi.no/mfr/ (accessed on 11 February 2018).
- Alvik, A.; Heyerdal, S.; Haldorsen, T.; Lindemann, R. Alcohol use before and during pregnancy: A population-based study. Acta. Obstet. Gynecol. Scand. 2006, 85, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Skretting, A.; Vedøy, T.F.; Lund, K.E.; Bye, E.K. Alkohol, tobakk, vanedannede legemidler, narkotika, sniffing, doping og tjenestetilbudet. In Rusmidler i Norge 2016; Norwegian Institute of Public Health: Oslo, Norway, 2016; pp. 14–115. [Google Scholar]
- Aberg, A.; Rydhstroem, H.; Frid, A. Impaired glucose tolerance associated with adverse pregnancy outcome: A population based-study in southern Sweden. AJOG 2001, 184, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Zhang, C.; Van Dam, R.M.; Bowers, K.; Hu, F.B. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: A meta-analysis. Diabetes Care 2011, 34, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radesky, J.S.; Oken, E.; Rifas-Shiman, S.L.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Diet during early pregnancy and development of gestational diabetes. Paediatr. Perinat. Epidemiol. 2008, 22, 47–59. [Google Scholar] [CrossRef]
- Zhang, C.; Tobias, D.K.; Chavarro, J.E.; Bao, W.; Wang, D.; Ley, S.H.; Hu, F.B. Adherence to healthy lifestyle and risk of gestational diabetes mellitus: Prospective cohort study. BMJ 2014, 349, g5450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health Development. The HUNT Study, Norway: HUNT 1 (1984-86)—HUNT 2 (1995-97)—HUNT 3 (2006-08). Krokstad, S., Knudtsen, M.S., Eds.; HUNT forskningssenter: Levanger, Norway, 2011. Available online: https://www.ntnu.no/documents/10304/1130562/folkehelse-i-endring-huntrapport-2011.pdf (accessed on 18 April 2018).
- Jenum, A.K.H.; Hanssen, K.F.; Thordarson, H.B.; Henriksen, T.; Bjerkan, K.; Holm, H.O.; Gudin, H.B. Gestational Diabetes. Norwegian Clinical Guideline for Gestational Diabetes. 2017. Available online: https://helsedirektoratet.no/retningslinjer/svangerskapsdiabetes (accessed on 4 April 2018).
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation; WHO Production Services: Geneva, Switzerland, 2006; pp. 9–34. [Google Scholar]
- Byers, T. Food frequency dietary assessment: How bad is good enough? Am. J. Epidemiol. 2001, 154, 1087–1088. [Google Scholar] [CrossRef] [PubMed]
- Kristal, A.R.; Peters, U.; Potter, J.D. Is it time to abandon the food frequency questionnaire? Cancer Epidemiol. Biomarkers Prev. 2005, 14, 2826–2828. [Google Scholar] [CrossRef] [PubMed]
- Owe, K.M.; Nystad, W.; Bø, K. Correlates of regular exercise during pregnancy: The Norwegian Mother and Child Cohort Study. Scand. J. Med. Sci. Sports 2009, 19, 637–645. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| GDM Women n = 40 | Non-GDM Women n = 662 | ||||||
|---|---|---|---|---|---|---|---|
| 25th | Median | 75th | 25th | Median | 75th | p * | |
| Pre-pregnancy | |||||||
| Height (m) | 1.65 | 1.69 | 1.72 | 1.64 | 1.68 | 1.73 | 0.495 |
| Weight (kg) | 61 | 67 | 74 | 59 | 64 | 70 | 0.028 |
| BMI (kg/m2) | 21.6 | 24.2 | 27.0 | 21.0 | 22.5 | 24.3 | 0.009 |
| Exercised regularly † n (%) | 12 (30) | 220 (33) | 0.732 | ||||
| Gestational week 18–22 | |||||||
| Age (year) | 27 | 32 | 35 | 28 | 30 | 33 | 0.281 |
| Weight (kg) | 66.3 | 73.9 | 81.5 | 63.5 | 68.4 | 74.7 | 0.003 |
| Weight gained (kg) | 3.7 | 5.4 | 7.9 | 2.9 | 4.5 | 6.3 | 0.025 |
| OGTT glucose level ‡ (mmol/L) | |||||||
| Fasting | 4.4 | 4.7 | 5.0 | 4.1 | 4.3 | 4.5 | <0.001 |
| 2-h | 4.8 | 5.6 | 6.3 | 4.2 | 4.8 | 5.4 | <0.001 |
| Had one or more children before n (%) | 20 (50) | 276 (42) | 0.325 | ||||
| Smoking n (%) | 1 (3) | 5 (1) | 0.298 | ||||
| Diabetes in first degree-relatives n (%) | |||||||
| Yes | 3 (8) | 58 (9) | 0.024 | ||||
| No | 30 (84) | 570 (90) | |||||
| Do not know | 3 (8) | 6 (1) | |||||
| Allocated to intervention group n (%) | 17 (43) | 358 (54) | 0.191 | ||||
| Adhered to the exercise protocol n (%) | 9 (28) | 203 (40) | 0.197 | ||||
| Gestational week 32–36 | |||||||
| Weight (kg) | 73.2 | 81.8 | 89.4 | 70.0 | 75.9 | 82.3 | 0.001 |
| Weight gained (kg) | 10.8 | 14.3 | 17.6 | 9.0 | 11.8 | 13.9 | 0.012 |
| OGTT glucose level ‡ (mmol/L) | |||||||
| Fasting | 4.9 | 5.2 | 5.4 | 4.0 | 4.2 | 4.5 | <0.001 |
| 2-h | 6.0 | 7.2 | 9.0 | 4.8 | 5.5 | 6.3 | <0.001 |
| Smoking n (%) | 0 (0) | 4 (1) | 1.00 | ||||
| Gestational Week 18–22 | Gestational Week 32–36 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GDM Women n = 40 | Non-GDM Women n = 662 | GDM Women n = 40 | Non-GDM Women n = 661 | |||||||||||
| Edible Amounts, g/day | 25th | Median | 75th | 25th | Median | 75th | p * | 25th | Median | 75th | 25th | Median | 75th | p * |
| Bread | 146 | 189 | 242 | 133 | 174 | 217 | 0.198 | 124 | 175 | 218 | 134 | 168 | 207 | 0.762 |
| Cereals | 40 | 60 | 89 | 39 | 61 | 86 | 0.844 | 42 | 63 | 103 | 38 | 59 | 87 | 0.294 |
| Cakes | 9 | 17 | 31 | 10 | 19 | 31 | 0.496 | 13 | 21 | 37 | 12 | 21 | 33 | 0.641 |
| Potatoes | 20 | 37 | 61 | 24 | 41 | 61 | 0.791 | 22 | 48 | 61 | 21 | 34 | 58 | 0.652 |
| French fries | 0 | 3 | 10 | 1 | 3 | 10 | 0.965 | 1 | 7 | 11 | 1 | 3 | 7 | 0.042 |
| Vegetables | 150 | 233 | 284 | 127 | 200 | 296 | 0.303 | 105 | 177 | 271 | 117 | 177 | 256 | 0.898 |
| Fruit and berries | 191 | 296 | 382 | 229 | 322 | 448 | 0.343 | 211 | 275 | 397 | 222 | 329 | 479 | 0.729 |
| Fruit juices | 34 | 62 | 140 | 54 | 108 | 157 | 0.027 | 23 | 54 | 108 | 47 | 107 | 161 | 0.010 |
| Meat | 64 | 96 | 139 | 77 | 104 | 137 | 0.610 | 65 | 93 | 127 | 71 | 98 | 126 | 0.611 |
| Fish and shellfish | 28 | 41 | 61 | 29 | 48 | 71 | 0.479 | 25 | 38 | 58 | 27 | 43 | 67 | 0.266 |
| Eggs | 9 | 18 | 28 | 9 | 17 | 22 | 0.378 | 10 | 17 | 22 | 8 | 14 | 20 | 0.190 |
| Dairy products † | 210 | 367 | 502 | 176 | 341 | 514 | 0.484 | 319 | 405 | 515 | 202 | 363 | 554 | 0.287 |
| Cheese | 10 | 23 | 52 | 15 | 32 | 51 | 0.252 | 13 | 32 | 52 | 14 | 29 | 45 | 0.627 |
| Whey cheese | 0 | 0 | 5 | 4 | 10 | 24 | 0.009 | 0 | 2 | 10 | 0 | 5 | 10 | 0.140 |
| Butter, margarine, oil | 19 | 34 | 47 | 15 | 29 | 45 | 0.135 | 19 | 33 | 51 | 15 | 28 | 42 | 0.089 |
| Sugar and sweets | 11 | 21 | 37 | 10 | 17 | 28 | 0.152 | 13 | 19 | 31 | 11 | 19 | 30 | 0.681 |
| Beverages ‡ | 773 | 915 | 1531 | 728 | 1028 | 1510 | 0.925 | 779 | 1080 | 1551 | 658 | 957 | 1341 | 0.055 |
| Various intake § | 82 | 122 | 187 | 77 | 114 | 164 | 0.332 | 73 | 107 | 161 | 74 | 106 | 150 | 0.728 |
| Gestational Week 18–22 | Gestational Week 32–36 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Recommendations | GDM Women n = 40 | Non-GDM Women n = 662 | GDM Women n = 40 | Non-GDM Women n = 661 | |||||||||||
| 25th | Median | 75th | 25th | Median | 75th | p * | 25th | Median | 75th | 25th | Median | 75th | p * | ||
| Food groups, per day or week | |||||||||||||||
| Fruit and vegetables g/day | ≥500 † g/day | 391 | 542 | 652 | 404 | 531 | 710 | 0.430 | 363 | 494 | 670 | 376 | 521 | 712 | 0.604 |
| Vegetables g/day | ≥250 † g/day | 150 | 233 | 284 | 127 | 200 | 296 | 0.303 | 105 | 177 | 271 | 117 | 177 | 256 | 0.898 |
| Red and processed meat g/week | ≤500 † g/week | 423 | 588 | 964 | 462 | 646 | 864 | 0.771 | 383 | 590 | 842 | 438 | 613 | 808 | 0.721 |
| Fish and shellfish g/week | 300–450 † g/week | 198 | 288 | 427 | 204 | 337 | 498 | 0.479 | 174 | 263 | 403 | 189 | 298 | 468 | 0.266 |
| Fatty fish g/week | 200 † g/week | 8 | 49 | 116 | 25 | 64 | 123 | 0.157 | 0 | 28 | 83 | 17 | 57 | 116 | 0.014 |
| Energy and macronutrients per day | |||||||||||||||
| Total energy intake kcal | 1963 | 2164 | 2561 | 1755 | 2086 | 2451 | 0.238 | 1826 | 2213 | 2605 | 1741 | 2060 | 2421 | 0.208 | |
| Total fat E% | 25–40 E% ‡ | 29 | 34 | 37 | 29 | 33 | 36 | 0.690 | 29 | 33 | 37 | 29 | 33 | 36 | 0.587 |
| Protein E% | 10–20 E% ‡ | 15 | 16 | 17 | 15 | 16 | 17 | 0.962 | 14 | 15 | 17 | 14 | 16 | 20 | 0.456 |
| Carbohydrates E% | 45–60 E% ‡ | 45 | 49 | 52 | 45 | 48 | 51 | 0.796 | 45 | 50 | 53 | 46 | 49 | 52 | 0.880 |
| Added sugar E% | <10 E% ‡ | 4 | 7 | 9 | 5 | 6 | 9 | 0.548 | 6 | 6 | 9 | 5 | 7 | 9 | 0.962 |
| Alcohol E% | Abstinence § | 0 | 0 | 0.1 | 0 | 0 | 0.1 | 0.930 | 0 | 0 | 0.1 | 0 | 0 | 0.1 | 0.612 |
| Fiber g | 25–35 g ‡ | 25 | 28 | 33 | 23 | 28 | 33 | 0.453 | 23 | 27 | 36 | 22 | 27 | 33 | 0.600 |
| Micronutrients per day | |||||||||||||||
| Cholesterol (mg/mL) | 193 | 274 | 331 | 205 | 266 | 325 | 0.937 | 205 | 255 | 288 | 197 | 252 | 312 | 0.867 | |
| Vitamin A RAE ‖ | 800 µg ¶ | 839 | 1386 | 1686 | 879 | 1195 | 1617 | 0.640 | 744 | 1162 | 1258 | 838 | 1142 | 1542 | 0.925 |
| Vitamin D (µg) | 10 µg ¶ | 6.0 | 9.2 | 13.7 | 5.5 | 8.6 | 14.1 | 0.712 | 7.0 | 10.2 | 14.0 | 5.2 | 8.3 | 13.9 | 0.166 |
| Tocopherol (mg) | 10 µg ¶ | 10.4 | 17.5 | 22.2 | 11.7 | 16.7 | 22.6 | 0.955 | 11.8 | 17.8 | 25.4 | 10.8 | 16.4 | 22.0 | 0.220 |
| Thiamin (mg) | 1.5 mg ¶ | 1.4 | 1.6 | 2.3 | 1.3 | 1.6 | 2.0 | 0.204 | 1.4 | 1.7 | 2.4 | 1.2 | 1.5 | 2.0 | 0.008 |
| Riboflavin (mg) | 1.6 mg ¶ | 1.6 | 1.9 | 2.6 | 1.4 | 1.9 | 2.4 | 0.329 | 1.6 | 2.0 | 2.9 | 1.4 | 1.8 | 2.4 | 0.028 |
| Folate (µg) | 400 µg # | 244 | 314 | 581 | 232 | 313 | 453 | 0.515 | 223 | 299 | 443 | 209 | 270 | 362 | 0.062 |
| Vitamin C (mg) | 85 mg ¶ | 111 | 164 | 220 | 110 | 153 | 217 | 0.548 | 106 | 158 | 252 | 99 | 145 | 202 | 0.241 |
| Calcium (mg) | 900 mg ¶ | 758 | 930 | 1260 | 718 | 919 | 1154 | 0.481 | 853 | 1003 | 1239 | 711 | 932 | 1155 | 0.068 |
| Fe (mg) | 15 mg ** | 9.0 | 11.0 | 13.1 | 8.9 | 10.9 | 14.0 | 0.932 | 8.5 | 11.0 | 18.6 | 8.6 | 10.7 | 14.2 | 0.236 |
| Magnesium (mg) | 280 mg ¶ | 301 | 354 | 403 | 288 | 341 | 410 | 0.542 | 308 | 359 | 431 | 285 | 342 | 408 | 0.867 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elvebakk, T.; Mostad, I.L.; Mørkved, S.; Salvesen, K.Å.; Stafne, S.N. Dietary Intakes and Dietary Quality during Pregnancy in Women with and without Gestational Diabetes Mellitus - A Norwegian Longitudinal Study. Nutrients 2018, 10, 1811. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111811
Elvebakk T, Mostad IL, Mørkved S, Salvesen KÅ, Stafne SN. Dietary Intakes and Dietary Quality during Pregnancy in Women with and without Gestational Diabetes Mellitus - A Norwegian Longitudinal Study. Nutrients. 2018; 10(11):1811. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111811
Chicago/Turabian StyleElvebakk, Trude, Ingrid L. Mostad, Siv Mørkved, Kjell Å. Salvesen, and Signe N. Stafne. 2018. "Dietary Intakes and Dietary Quality during Pregnancy in Women with and without Gestational Diabetes Mellitus - A Norwegian Longitudinal Study" Nutrients 10, no. 11: 1811. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10111811