The Effectiveness of Nutrition Education for Overweight/Obese Mother with Stunted Children (NEO-MOM) in Reducing the Double Burden of Malnutrition

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Theory
2.2. Sample Size and Allocation
2.3. Dietary Data
2.4. Behavioral Measures
2.5. Statistical Analysis
2.6. Ethical Clearance
3. Results
3.1. Characteristics of Participants and Groups
3.2. Intervention Effect on Outcomes and Mediators
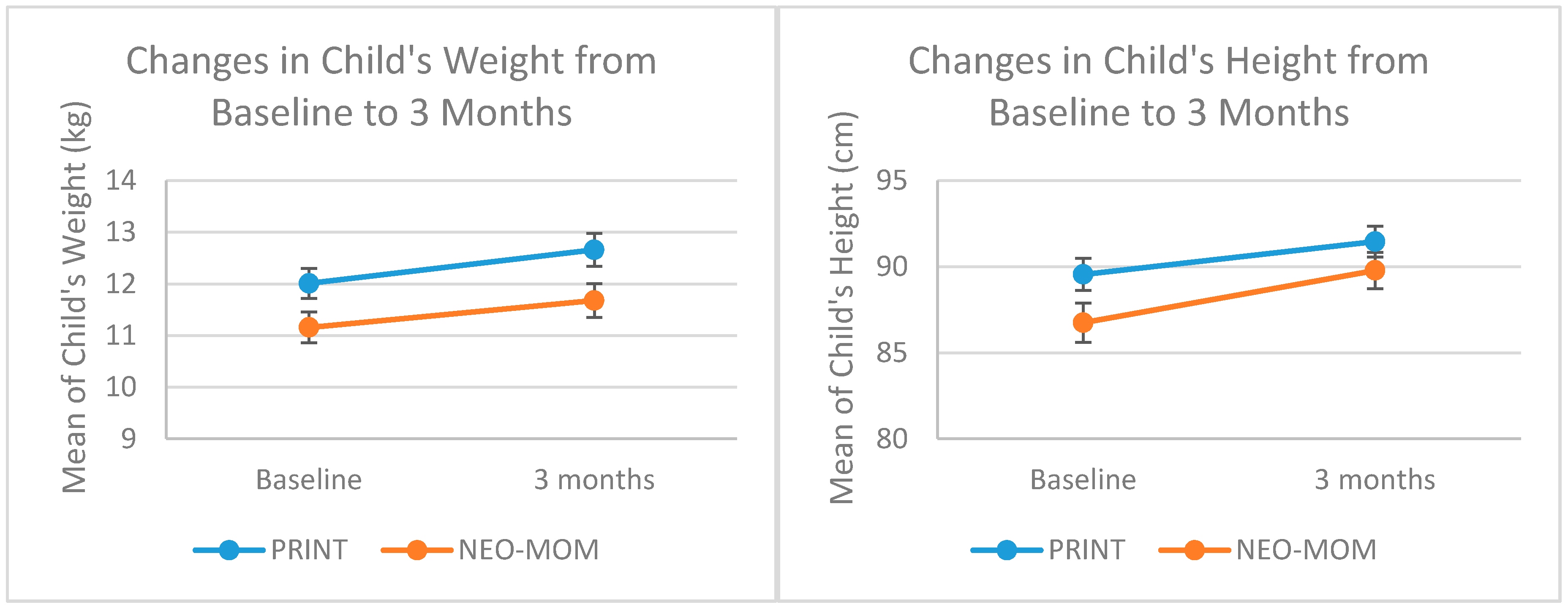
3.2.1. Child’s Outcomes
3.2.2. Maternal Outcomes
3.2.3. Household Dietary Diversity
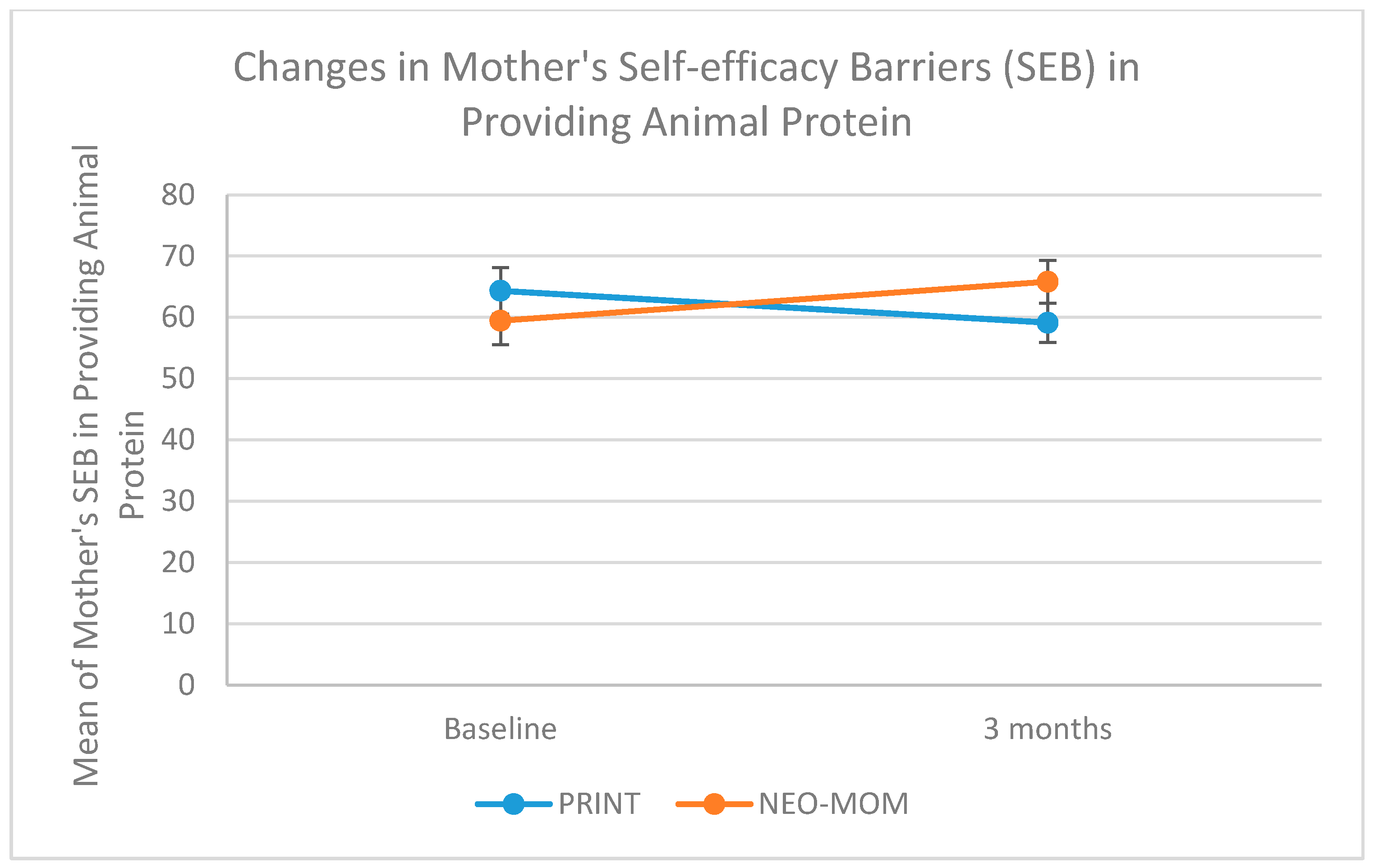
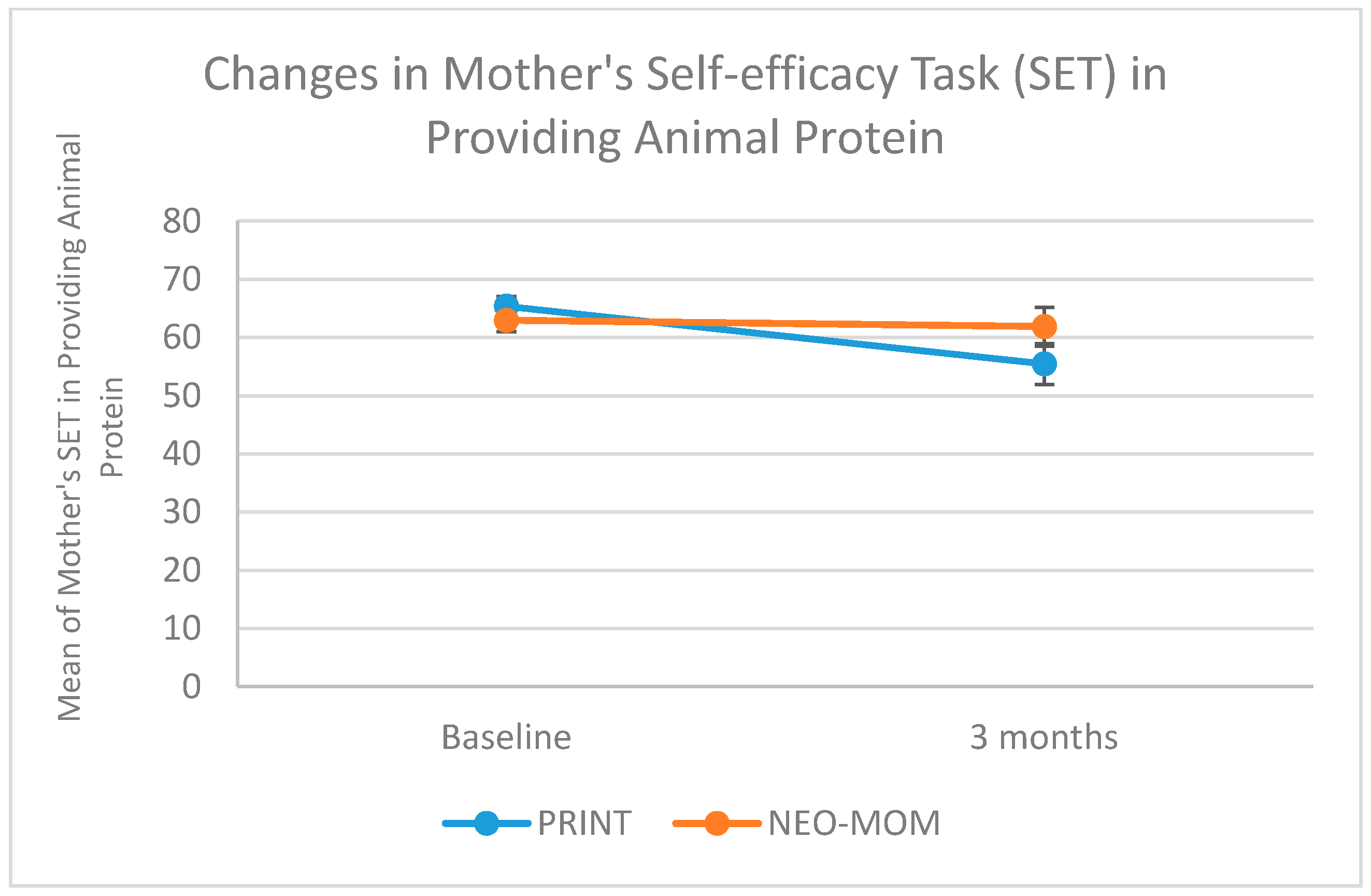
3.2.4. Maternal Self-Efficacy
3.2.5. Maternal Outcome Expectation
3.2.6. Maternal Nutrition Literacy
3.2.7. Maternal Dietary Intake
3.2.8. Moderation of Intervention Effects
4. Discussion
Strengths and Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Child Growth Standards: Methods and Development. WHO2014. Available online: http://www.who.int/childgrowth/standards/Technical_report.pdf (accessed on 23 March 2018).
- Martins, P.A.; Hoffman, D.J.; Fernandes, M.T.B.; Nascimento, C.R.; Roberts, S.B.; Sesso, R.; Sawaya, A.L. Stunted children gain less lean body mass and more fat mass than their non-stunted counterparts: A prospective study. Br. J. Nutr. 2004, 92, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Cameron, N.; Wright, M.M.; Griffiths, P.L.; Norris, S.A.; Petiffor, J.M. Stunting at 2 years in relation to body composition at 9 years in African urban children. Obesity 2005, 13, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Improving Child Nutrition. The Achievable Imperative for Global Progress. Available online: https://www.unicef.org/gambia/Improving_Child_Nutrition_-_the_achievable_imperative_for_global_progress.pdf (accessed on 23 March 2018).
- Lassi, Z.S.; Das, J.K.; Zahid, G.; Imdad, A.; Bhutta, Z.A. Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: A systematic review. BMC Public Health 2013, 13, S13. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Yakoob, M.Y.; Bhutta, Z.A. Impact of maternal education about complementary feeding and provision of complementary foods on child growth in developing countries. BMC Public Health 2011, 11, S4. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.K.; Fuchs, G.J.; Mahmud, Z.; Ara, G.; Islam, S.; Shafique, S.; Akter, S.S.; Chakraborty, B. Intensive nutrition education with or without supplementary feeding improves the nutritional status of moderately-malnourished children in Bangladesh. J. Health. Popul. Nutr. 2005, 23, 320–330. [Google Scholar] [PubMed]
- Majamanda, J.; Maureen, D.; Munkhondia, T.M.; Carrier, J. The Effectiveness of Community-Based Nutrition Education on the Nutrition Status of Under-five Children in Developing Countries. A Systematic Review. Malawi Med. J. 2014, 26, 115–118. [Google Scholar] [PubMed]
- Lee, J.; Houser, R.F.; Must, A.; de Fulladolsa, P.P.; Bermudez, O.I. Socioeconomic disparities and the familial coexistence of child stunting and maternal overweight in Guatemala. Econ. Hum. Biol. 2012, 10, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Human agency in social cognitive theory. Am. Psycho. 1989, 44, 1175–1184. [Google Scholar] [CrossRef]
- Bandura, A. Guide for constructing self-efficacy scales. In Self-Efficacy Beliefs of Adolescents; Urdan, T., Pajares, F., Eds.; Information Age Publishing Inc.: Charlotte, CA, USA, 2006; pp. 307–337. ISBN 978-1593113667. [Google Scholar]
- Mahmudiono, T.; Nindya, T.S.; Andrias, D.R.; Megatsari, H.; Rosenkranz, R.R. The effectiveness of nutrition education for overweight/obese mothers with stunted children (NEO-MOM) in reducing the double burden of malnutrition in Indonesia: Study protocol for a randomized controlled trial. BMC Public Health 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, E.; Francis, D.K.; Liberato, S.; Benkhalti Jandu, M.; Welch, V.; Batal, M.; Greenhalgh, T.; Rader, T.; Noonan, E.; Shea, B.; et al. Food supplementation for improving the physical and psychosocial health of socio-economically disadvantaged children aged three months to five years. Cochrane Dat. Sys. Rev. 2015, 3, CD009924. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.J.; Lacy, K.E.; Campbell, K.J.; McNaughton, S.A. The Predictors of Diet Quality among Australian Children Aged 3.5 Years. J. Ac. Nutr. Diet. 2016, 116, 1114–1126.e2. [Google Scholar] [CrossRef] [PubMed]
- Koh, G.A.; Scott, J.A.; Woodman, R.J.; Kim, S.W.; Daniels, L.A.; Magarey, A.M. Maternal feeding self-efficacy and fruit and vegetable intakes in infants. Results from the SAIDI study. Appetite 2014, 81, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Kilanowski, J.F. Influences on Healthy-Eating Decision Making in Latino Adolescent Children of Migrant and Seasonal Agricultural Workers. J. Ped. Health Care 2015, 30, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.M.; Dunton, G.F.; Pinard, C.A.; Yaroch, A.L. Factors influencing food preparation behaviors: Findings from focus groups with Mexican-American mothers in southern California. Public Health Nutr. 2016, 19, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, W.S.; Frongillo, E.A.; Valois, P. Understanding the experience of food insecurity by elders suggests ways to improve its measurement. J. Nutr. 2003, 133, 2762–2769. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R. Principles of Nutritional Assessment, 2nd ed.; Oxford University Press: New York, NY, USA, 2005; pp. 123–125. ISBN 978-0195171693. [Google Scholar]
- Gibbs, H.; Chapman-Novakofski, K. Establishing content validity for the nutrition literacy assessment instrument. Prev. Chronic Dis. 2013, 10, E109. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | NEO-MOM (n = 35) | PRINT (n = 36) | p-Value | ||
|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | ||
| Child characteristics | |||||
| Age (months) | 39.57 | 7.82 | 40.24 | 8.11 | 0.679 |
| Weight (kg) | 11.32 | 1.92 | 12.25 | 2.44 | 0.045 * |
| Height (cm) | 86.84 | 6.34 | 89.43 | 5.34 | 0.060 |
| Height-for-age Z-score | −2.998 | 0.85 | −2.674 | 0.57 | 0.071 |
| Maternal characteristics | |||||
| Age (years) | 34.09 | 6.86 | 31.47 | 6.76 | 0.123 |
| Education (years) | 7.29 | 7.75 | 7.89 | 3.62 | 0.417 |
| Weight (kg) | 64.59 | 8.83 | 67.99 | 10.15 | 0.233 |
| Height (cm) | 147.43 | 5.11 | 148.23 | 4.67 | 0.441 |
| Waist circumference (cm) | 92.61 | 8.30 | 93.91 | 9.72 | 0.364 |
| Household characteristics | |||||
| Dietary diversity score | 7.29 | 1.86 | 7.22 | 1.80 | 0.737 |
| HFIAS score | 8.94 | 5.75 | 5.92 | 5.49 | 0.061 |
| Monthly Income (IDR) | 1,532,857 | 512,769 | 2,116,666 | 1,448,562 | 0.054 |
| Monthly Food expenditure (IDR) | 974,074 | 343,726 | 1,217,307 | 316,418 | 0.010 * |
| Maternal physical activity | |||||
| Average daily step | 3156 | 2134 | 2899 | 2356 | 0.196 |
| Variable | F | p-Value | Partial Eta Squared | Adjusted R Squared |
|---|---|---|---|---|
| Child’s outcomes | ||||
| Weight (kg) | 0.629 | 0.431 | 0.010 | 0.151 |
| Height (cm) | 0.407 | 0.526 | 0.007 | −0.022 |
| Maternal outcomes | ||||
| Weight (kg) | 0.027 | 0.871 | 0.000 | −0.028 |
| Waist circumference (mm) | 0.726 | 0.397 | 0.012 | −0.025 |
| BMI # | 0.115 | 0.736 | 0.002 | −0.023 |
| Maternal self-efficacy (Barrier) | ||||
| Being physically active | 2.035 | 0.159 | 0.032 | 0.323 |
| Eating fruit | 10.011 | 0.002 * | 0.139 | 0.404 |
| Eating vegetables | 10.238 | 0.002 * | 0.142 | 0.236 |
| Providing animal protein for kids | 5.224 | 0.026 * | 0.078 | 0.474 |
| Maternal self-efficacy (Task) | ||||
| Being physically active | 3.922 | 0.052 | 0.059 | 0.276 |
| Eating fruit | 4.624 | 0.036 * | 0.070 | 0.096 |
| Eating vegetables | 3.137 | 0.081 | 0.048 | 0.179 |
| Providing animal protein for kids | 4.468 | 0.039 * | 0.067 | 0.081 |
| Outcome/Mediator | Mean (SE) | Test of Within-Subject Effect | Test of Between-Subject Effect | ||||
|---|---|---|---|---|---|---|---|
| Intervention (n = 32) | Comparison (n = 34) | Partial Eta Square (p) | |||||
| Baseline | 3 Month | Baseline | 3 Month | Time | Time by Group Interaction | Group Difference | |
| Child’s outcomes | |||||||
| Weight (kg) | 11.19 (0.31) | 11.69 (0.34) | 11.98 (0.29) | 12.64 (0.33) | 0.080 (0.023) * | 0.005 (0.578) | 0.059 (0.050) * |
| Height (cm) | 86.80 (1.07) | 89.90 (1.01) | 89.49 (1.04) | 91.34 (0.98) | 0.173 (0.001) ** | 0.027 (0.189) | 0.034 (0.143) |
| Maternal outcomes | |||||||
| Weight (kg) | 65.17 (1.49) | 64.87 (1.54) | 68.35 (1.44) | 67.91 (1.49) | 0.034 (0.139) | 0.001 (0.819) | 0.033 (0.146) |
| Waist circumference (mm) | 92.18 (1.60) | 91.73 (1.80) | 95.08 (1.56) | 95.67 (1.74) | 0.000 (0.992) | 0.008 (0.505) | 0.034 (0.141) |
| BMI a | 30.13 (0.62) | 29.95 (0.59) | 31.01 (0.66) | 30.63 (0.75) | 0.054 (0.062) | 0.006 (0.543) | 0.022 (0.235) |
| Maternal self-efficacy (Barrier) | |||||||
| Being physically active | 50.55 (2.53) | ||||||
| Eating fruit | 43.95 (2.61) | 49.11 (2.88) | 55.66 (3.69) | 45.34 (2.79) | 0.008 (0.472) | 0.072 (0.030) * | 0.003 (0.650) |
| Eating vegetables | 53.04 (3.80) | 62.49 (3.41) | 38.03 (2.54) | 49.82 (3.30) | 0.025 (0.207) | 0.115 (0.006) * | 0.021 (0.251) |
| Providing animal | 35.29 (2.62) | 61.13 (3.39) | 63.47 (3.83) | 48.54 (3.28) | 0.376 (<0.001) *** | 0.146 (0.002) ** | 0.029 (0.174) |
| protein for kids | 60.36 (3.95) | 67.24 (3.31) | 57.78 (3.21) | 0.008 (0.491) | 0.064 (0.042) * | 0.009 (0.448) | |
| Maternal self-efficacy (Task) | |||||||
| Being physically active | 34.71 (3.99) | 56.19 (4.17) | 30.53 (3.86) | 43.62 (4.04) | |||
| Eating fruit | 49.16 (2.12) | 58.19 (3.73) | 50.08 (2.09) | 47.66 (3.67) | 0.203 (<0.001) *** | 0.026 (0.199) | 0.047 (0.083) |
| Eating vegetables | 55.17 (2.19) | 58.57 (3.48) | 55.30 (2.12) | 49.98 (3.38) | 0.028 (0.185) | 0.071 (0.034) * | 0.031 (0.167) |
| Providing animal | 63.51 (1.83) | 63.18 (3.42) | 64.78 (1.78) | 54.20 (3.32) | 0.014 (0.355) | 0.041 (0.105) | 0.028 (0.182) |
| protein for kids | 0.002 (0.717) | 0.071 (0.032) * | 0.024 (0.217) | ||||
| Outcome/Mediator | Intervention | Comparison | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Z | p-Value | Mean (SD) | Z | p-Value | |||
| Baseline (n = 32) | 3 Month (n = 32) | Baseline (n = 34) | 3 Month (n = 34) | |||||
| Child’s HAZ | −2.99 (0.85) | −2.85 (0.79) | −1.333 | 0.183 | −2.67 (0.57) | −2.55 (0.61) | −1.951 | 0.051 |
| Mother’s BMI | 30.13 (3.52) | 29.95 (3.34) | −0.895 | 0.371 | 31.01 (3.84) | 30.63 (4.36) | −1.646 | 0.100 |
| Household dietary diversity | 7.44 (1.70) | 6.50 (2.11) | −2.847 | 0.004 * | 7.29 (1.75) | 5.68 (1.61) | −3.380 | <0.001 ** |
| Maternal outcome expectation | ||||||||
| Being physically active | 5.04 (0.65) | 5.21 (0.48) | −1.381 | 0.167 | 5.01 (0.72) | 4.86 (0.72) | −1.082 | 0.279 |
| Eating fruit & vegetables | 5.06 (0.56) | 5.18 (0.49) | −1.312 | 0.190 | 4.98 (0.54) | 4.97 (0.57) | −0.152 | 0.879 |
| Providing animal protein for kids | 5.12 (0.54) | 5.33 (0.48) | −2.242 | 0.025 * | 5.13 (0.59) | 5.17 (0.56) | −0.320 | 0.749 |
| Maternal nutrition literacy | ||||||||
| Macronutrient | 2.63 (1.62) | 2.47 (1.48) | -0.630 | 0.529 | 3.15 (1.50) | 3.03 (1.62) | −0.367 | 0.714 |
| Household food measures | 1.78 (1.01) | 1.75 (0.76) | −0.339 | 0.735 | 1.53 (1.11) | 1.32 (0.98) | −0.920 | 0.358 |
| MyPlate categorization | 12.72 (1.78) | 13.19 (2.39) | −1.442 | 0.149 | 12.79 (1.90) | 12.82 (1.96) | −0.039 | 0.969 |
| Maternal dietary intake | ||||||||
| Energy | 1075 (538) | 845 (559) | −2.393 | 0.017 * | 1029 (774) | 840 (502) | −1.135 | 0.257 |
| Protein | 57.29 (42.11) | 44.69 (39.59) | −1.627 | 0.104 | 46.50 (38.99) | 39.28 (32.47) | −1.027 | 0.304 |
| Fat | 49.95 (51.99) | 37.82 (48.80) | −1.646 | 0.100 | 56.21 (62.00) | 43.29 (48.23) | −0.652 | 0.514 |
| Carbohydrate | 103.18 (74.50) | 90.75 (69.79) | −0.926 | 0.355 | 91.71 (59.06) | 77.71 (39.49) | −1.349 | 0.177 |
| Iron | 6.62 (8.04) | 6.58 (11.54) | −1.197 | 0.231 | 6.32 (7.69) | 5.22 (3.40) | −0.527 | 0.598 |
| Zinc | 3.93 (2.13) | 3.18 (2.27) | −1.833 | 0.067 | 3.62 (2.51) | 3.35 (1.89) | −0.225 | 0.822 |
| Calcium | 140.17 (96.21) | 144.31 (200.88) | −1.141 | 0.254 | 157.05 (190.80) | 159.81 (186.58) | −0.527 | 0.698 |
| Vitamin A | 842 (559) | 680 (1466) | −1.496 | 0.135 | 982 (2441) | 503 (738) | −1.930 | 0.054 |
| Fiber | 6.77 (7.29) | 6.75 (10.60) | −1.029 | 0.303 | 8.47 (14.88) | 5.45 (5.22) | −1.524 | 0.127 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmudiono, T.; Mamun, A.A.; Nindya, T.S.; Andrias, D.R.; Megatsari, H.; Rosenkranz, R.R. The Effectiveness of Nutrition Education for Overweight/Obese Mother with Stunted Children (NEO-MOM) in Reducing the Double Burden of Malnutrition. Nutrients 2018, 10, 1910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121910
Mahmudiono T, Mamun AA, Nindya TS, Andrias DR, Megatsari H, Rosenkranz RR. The Effectiveness of Nutrition Education for Overweight/Obese Mother with Stunted Children (NEO-MOM) in Reducing the Double Burden of Malnutrition. Nutrients. 2018; 10(12):1910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121910
Chicago/Turabian StyleMahmudiono, Trias, Abdullah Al Mamun, Triska Susila Nindya, Dini Ririn Andrias, Hario Megatsari, and Richard R. Rosenkranz. 2018. "The Effectiveness of Nutrition Education for Overweight/Obese Mother with Stunted Children (NEO-MOM) in Reducing the Double Burden of Malnutrition" Nutrients 10, no. 12: 1910. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121910