Positive Association between Dietary Inflammatory Index and the Risk of Osteoporosis: Results from the KoGES_Health Examinee (HEXA) Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
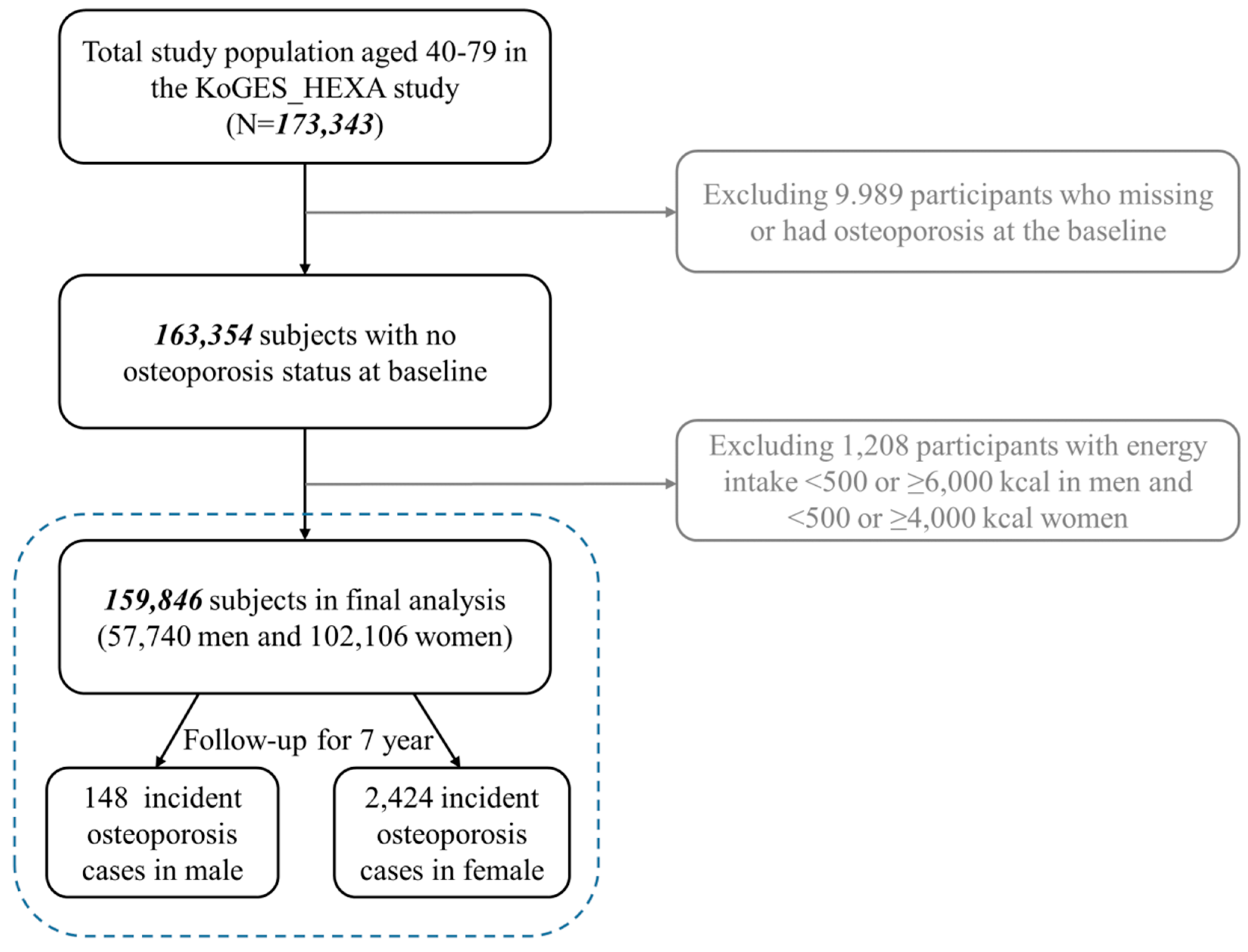
2.1. Study Population and Data Collection
2.2. Dietary Assessment Using SQ-FFQ and the Calculation of DII
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marini, F.; Cianferotti, L.; Brandi, M.L. Epigenetic mechanisms in bone biology and osteoporosis: Can they drive therapeutic choices? Int. J. Mol. Sci. 2016, 17, 1329. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.L.; Kaplan, F.S. Osteoporosis. Definition and clinical presentation. Spine 1997, 22, 12s–16s. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y. Epidemiology of osteoporosis in Korea. J. Korean Med. Assoc. 2016, 59, 836–841. [Google Scholar] [CrossRef]
- Martinez, B.K.; White, C.M. The emerging role of inflammation in cardiovascular disease. Ann. Pharmacother. 2018, 52, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Pannen, B.H.; Robotham, J.L. The acute-phase response. New Horiz. 1995, 3, 183–197. [Google Scholar] [PubMed]
- Page, R.C. The role of inflammatory mediators in the pathogenesis of periodontal disease. J. Periodontal. Res. 1991, 26, 230–242. [Google Scholar] [CrossRef]
- Lorenzo, J. Interactions between immune and bone cells: New insights with many remaining questions. J. Clin. Investig. 2000, 106, 749–752. [Google Scholar] [CrossRef]
- Schett, G. Effects of inflammatory and anti-inflammatory cytokines on the bone. Eur. J. Clin. Investig. 2011, 41, 1361–1366. [Google Scholar] [CrossRef]
- Phillips, C.M.; Shivappa, N.; Hebert, J.R.; Perry, I.J. Dietary inflammatory index and biomarkers of lipoprotein metabolism, inflammation and glucose homeostasis in adults. Nutrients 2018, 10, 33. [Google Scholar] [CrossRef]
- Oliveira, M.C.; Silveira, A.L.; Tavares, L.P.; Rodrigues, D.F.; van de Loo, F.A.; Sousa, L.P.; Teixeira, M.M.; Amaral, F.A.; Ferreira, A.V. Two opposite extremes of adiposity similarly reduce inflammatory response of antigen-induced acute joint inflammation. Nutrition 2017, 33, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.M.; Khang, Y.H.; Jung, C.H.; Bae, S.; Kim, D.J.; Chung, Y.E.; Kim, G.S. Higher circulating hsCRP levels are associated with lower bone mineral density in healthy pre- and postmenopausal women: Evidence for a link between systemic inflammation and osteoporosis. Osteoporos. Int. 2005, 16, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, K.; Teklehaimanot, S.; Tran, T.H.; Asuncion, M.; Norris, K. Relationship of C-reactive protein and bone mineral density in community-dwelling elderly females. J. Natl. Med. Assoc. 2005, 97, 329–333. [Google Scholar] [PubMed]
- Asegaonkar, S.B.; Asegaonkar, B.N.; Takalkar, U.V.; Advani, S.; Thorat, A.P. C-reactive protein and breast cancer: New insights from old molecule. Int. J. Breast Cancer 2015, 2015, 145647. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Godos, J.; Hebert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary inflammatory index and colorectal cancer risk-a meta-analysis. Nutrients 2017, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; Gonzalez-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Na, W.; Kim, M.; Sohn, C. Dietary inflammatory index and its relationship with high-sensitivity C-reactive protein in Korean: Data from the health examinee cohort. J. Clin. Biochem. Nutr. 2018, 62, 83–88. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hebert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary inflammatory index and cardiovascular risk and mortality-a meta-analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Caan, B.; Hou, L.; Johnson, K.C.; Mossavar-Rahmani, Y.; Shivappa, N. The association between dietary inflammatory index and risk of colorectal cancer among postmenopausal women: Results from the Women’s Health Initiative. Cancer Causes Control 2015, 26, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Ramallal, R.; Toledo, E.; Martinez-Gonzalez, M.A.; Hernandez-Hernandez, A.; Garcia-Arellano, A.; Shivappa, N.; Hebert, J.R.; Ruiz-Canela, M. Dietary inflammatory index and incidence of cardiovascular disease in the sun cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Koyanagi, A.; Hebert, J.R.; Cooper, C.; Caruso, M.G.; Guglielmi, G.; Reginster, J.Y.; Rizzoli, R.; Maggi, S.; et al. Pro-inflammatory dietary pattern is associated with fractures in women: An eight-year longitudinal cohort study. Osteoporos. Int. 2018, 29, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Kim, Y.; Ahn, Y.O.; Paik, H.Y.; Ahn, Y.; Tokudome, Y.; Hamajima, N.; Inoue, M.; Tajima, K. Development of a food frequency questionnaire in Koreans. Asia Pac. J. Clin. Nutr. 2003, 12, 243–250. [Google Scholar]
- National Rural Resources Development Institute. Food Composition Table, 9th ed.; Rural Development Administration, National Rural Resources Development Institute: Suwon, Korea, 2016; Available online: http://koreanfood.rda.go.kr/eng/fctFoodSrchEng/engMain (accessed on 9 November 2018).
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Wirth, M.D.; Shivappa, N.; Davis, L.; Hurley, T.G.; Ortaglia, A.; Drayton, R.; Blair, S.N.; Hebert, J.R. Construct validation of the dietary inflammatory index among African Americans. J. Nutr. Health Aging 2017, 21, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.D.; Burch, J.; Shivappa, N.; Violanti, J.M.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Miller, D.B.; Mnatsakanova, A.; et al. Association of a dietary inflammatory index with inflammatory indices and metabolic syndrome among police officers. J. Occup. Environ. Med. 2014, 56, 986–989. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y. Multiple Imputation for Missing Data: Concepts and New Development, version 9.0; SAS Institute Inc.: Rockville, MD, USA, 2010; Volume 49. [Google Scholar]
- Orchard, T.; Yildiz, V.; Steck, S.E.; Hebert, J.R.; Ma, Y.; Cauley, J.A.; Li, W.; Mossavar-Rahmani, Y.; Johnson, K.C.; Sattari, M.; et al. Dietary inflammatory index, bone mineral density, and risk of fracture in postmenopausal women: Results from the women’s health initiative. J. Bone Miner. Res. 2017, 32, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Q.; Cao, W.T.; Shivappa, N.; Hebert, J.R.; Li, B.L.; He, J.; Tang, X.Y.; Liang, Y.Y.; Chen, Y.M. Association between diet inflammatory index and osteoporotic hip fracture in elderly Chinese population. J. Am. Med. Dir. Assoc. 2017, 18, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Casimir, G.J.; Duchateau, J. Gender differences in inflammatory processes could explain poorer prognosis for males. J. Clin. Microbiol. 2011, 49, 478–479. [Google Scholar] [CrossRef] [PubMed]
- Iseme, R.A.; McEvoy, M.; Kelly, B.; Agnew, L.; Walker, F.R.; Attia, J. Is osteoporosis an autoimmune mediated disorder? Bone Rep. 2017, 7, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Fairweather, D. Sex differences in inflammation during atherosclerosis. Clin. Med. Insights Cardiol. 2014, 8, 49–59. [Google Scholar] [CrossRef]
- Lerner, U.H. Inflammation-induced bone remodeling in periodontal disease and the influence of post-menopausal osteoporosis. J. Dent. Res. 2006, 85, 596–607. [Google Scholar] [CrossRef]
- Riggs, B.L.; Khosla, S.; Melton, L.J., 3rd. A unitary model for involutional osteoporosis: Estrogen deficiency causes both type I and type II osteoporosis in postmenopausal women and contributes to bone loss in aging men. J. Bone Miner. Res. 1998, 13, 763–773. [Google Scholar] [CrossRef]
- Tory, K.L.; Mancuso, M.E.; Butler, T.A.; Johnson, J.E. Exercise early and often: Effect of physical activity and exercise on women’s bone health. Int. J. Environ. Res. Public Health. 2018, 28, 15. [Google Scholar] [CrossRef]
- Hamaguchi, K.; Kurihara, T.; Fujimoto, M.; Iemitsu, M.; Sato, K.; Hamaoka, T.; Sanada, K. The effects of low-repetition and light-load powewr training on bone mineral density in postmenopausal women with sarcopenia: A pilot study. BMC Geriatr. 2017, 17, 102. [Google Scholar] [CrossRef] [PubMed]
- Stilles, V.H.; Metcalf, B.S.; Knapp, K.M.; Rowlands, A.V. A small amount of precisely measured high-intensity habitual physcial activity predicts bone health in pre- and post-menopausal women in UK Bioban. Int. J. Epidemiol. 2017, 46, 1847–1856. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.; Millett, P.J.; Mist, B.; Laskey, M.A.; Rushton, N. Effect of exercise training programme on bone mineral density in novice college rowers. Br. J. Sports Med. 1995, 29, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, B.L. Exercise in the prevention of osteoporosis. Osteoporos. Int. 1993, 3 (Suppl. 1), 169–171. [Google Scholar] [CrossRef]
- Kitchin, B.; Morgan, S. Nutritional considerations in osteoporosis. Curr. Opin. Rheumatol. 2003, 15, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.M.; Horcajada, M.N.; Offord, E. Phytonutrients for bone health during ageing. Br. J. Clin. Pharmacol. 2013, 75, 697–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Feskanich, D. Dietary patterns and risk of hip fractures in postmenopausal women and men over 50 years. Osteoporos. Int. 2015, 26, 1825–1830. [Google Scholar] [CrossRef] [Green Version]
- Haring, B.; Crandall, C.J.; Wu, C.; LeBlanc, E.S.; Shikany, J.M.; Carbone, L.; Orchard, T.; Thomas, F.; Wactawaski-Wende, J.; Li, W.; et al. Dietary patterns and fractures in postmenopausal women: Results from the Women’s Health Initiative. JAMA Intern. Med. 2016, 176, 645–652. [Google Scholar] [CrossRef]
- Feart, C.; Lorrain, S.; Coupez, V.G.; Samieri, C.; Letenneur, L.; Paineau, D.; Barberger-Gateau, P. Adherence to a Mediterranean diet and risk of fractures in French older persons. Osteoporos. Int. 2013, 24, 3031–3041. [Google Scholar] [CrossRef]
- Pérez, A.R.; Velasco, A.R. Adhence to mediterranean diet and bone health. Nutr. Hosp. 2014, 29, 989–996. [Google Scholar]
- Pandey, M.K.; Gupta, S.C.; Karelia, D.; Gihooley, P.J.; Shakibaei, M.; Aggarwal, B.B. Dietary nutraceuticals as backbone for bone health. Biotechnol. Adv. 2018, 36, 1633–1648. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Quintiles of Dietary Inflammatory Index (DII) | p Value d | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ||
| N | n = 31,894 | n = 31,937 | n = 31,971 | n = 32,034 | n = 32,000 | |
| DII (Range) | −9.1296–−0.9826 | −0.9824–0.3988 | 0.3989–1.2867 | 1.2868–2.1761 | 2.1762–7.1055 | |
| Energy intake (Kcal/day) | 2270.4(581.4) a | 1908.2(426.8) | 1675.8(372.9) | 1501.2(388.6) | 1414.0(365.4) | <0.0001 |
| Age at enrollment (year) | 52.0(7.9) | 52.1(8.1) | 52.4(8.2) | 53.0(8.4) | 54.2(8.6) | <0.0001 |
| Calcium intake (mg/day) | 759.6(304.1) | 506.4(170.4) | 394.6(142.7) | 311.7(144.8) | 266.91(129.4) | <0.0001 |
| Sex | ||||||
| Men | 11,070(34.7) b | 11,566(36.2) | 11,636(36.4) | 11,470(35.8) | 11,998(37.5) | |
| Women | 20,824(65.3) | 20,381(63.8) | 20,335(63.6) | 20,564(64.2) | 20,002(62.5) | <0.0001 |
| BMI, kg/m2 c | ||||||
| <18.5 | 559(1.8) | 571(1.8) | 600(1.9) | 702(2.2) | 901(2.8) | <0.0001 |
| 18.5–25 | 20,234(63.4) | 20,641(64.6) | 20,878(65.2) | 20,989(65.6) | 21,012(65.7) | |
| >25 | 11,104(34.8) | 10,725(33.6) | 10,530(32.9) | 10,319(32.2) | 10,081(31.5) | |
| Marriage | ||||||
| Married | 31,090(98.0) | 31,114(97.9) | 31,113(97.8) | 31,109(97.6) | 30,971(97.2) | <0.0001 |
| Single/divorced | 625(2.0) | 674(2.1) | 717(2.2) | 782(2.4) | 882(2.8) | |
| Education level | ||||||
| ~Elementary school | 3588(11.4) | 3988(12.7) | 4838(15.3) | 5831(18.5) | 7912(25.1) | <0.0001 |
| Middle~High school | 18,633(59.2) | 18,520(58.8) | 18,341(58.1) | 18,298(57.9) | 17,694(56.1) | |
| College~ | 9247(29.4) | 9003(28.5) | 8397(26.6) | 7477(23.6) | 5925(18.8) | |
| Income (10,000 won) | ||||||
| Less than 100 | 2031(7.8) | 2169(8.0) | 2660(9.9) | 3406(12.6) | 4615(16.8) | <0.0001 |
| 100~less than 200 | 4697(17.9) | 4975(18.5) | 5307(19.7) | 5791(21.4) | 6637(24.1) | |
| 200~less than 300 | 6014(22.9) | 6487(24.0) | 6218(23.0) | 6049(22.4) | 5904(21.4) | |
| More than 300 | 13,478(51.4) | 13,353(49.5) | 12,790(47.4) | 11,806(43.6) | 10,380(37.7) | |
| Smoking status | ||||||
| Never | 23,198(73.1) | 22,852(71.8) | 22,902(71.9) | 23,061(72.2) | 22,005(69.0) | <0.0001 |
| Past | 4638(14.6) | 5040(16.8) | 5035(15.8) | 4874(15.3) | 4929(15.5) | |
| Current | 3908(12.3) | 3934(12.4) | 3933(12.3) | 3997(12.5) | 4972(15.5) | |
| Alcohol consumption | ||||||
| Never | 15,406(48.5) | 15,299(48.0) | 15,578(48.9) | 15,997(50.1) | 16,405(51.4) | <0.0001 |
| Past | 1320(4.2) | 1200(3.8) | 1177(3.7) | 1330(4.2) | 1365(4.3) | |
| Current | 15,042(47.3) | 15,042(48.2) | 15,135(47.4) | 14,616(45.7) | 14,141(44.3) | |
| Physical activity | ||||||
| Irregular | 12,476(39.2) | 14,038(44.1) | 14,881(46.7) | 16,019(50.2) | 18,249(57.2) | <0.0001 |
| Regular e | 19,345(60.8) | 17,828(55.9) | 17,021(53.3) | 15,910(49.8) | 13,663(42.8) | |
| Menopausal status | ||||||
| Post- | 10,519(54.7) | 10,558(54.6) | 10,867(56.2) | 11,535(58.9) | 12,404(63.7) | <0.0001 |
| Pre/peri- | 8711(45.3) | 8766(45.4) | 8474(43.8) | 8046(41.1) | 7064(36.3) | |
| Quintiles of Dietary Inflammatory Index (DII) a | P Trend b | P Int c | |||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | |||
| All subjects | |||||||
| Person-years | 247,723 | 238,409 | 236,933 | 234,420 | 223,910 | ||
| Cases | 440 | 491 | 517 | 578 | 546 | ||
| Crude HR (95% CI) | 1.0 | 1.18 (1.03–1.34) | 1.25 (1.10–1.42) | 1.43 (1.26–1.61) | 1.45 (1.28–1.64) | <0.0001 | |
| Multivariate HR (95% CI) d | 1.0 | 1.21 (1.05–1.39) | 1.25 (1.08–1.46) | 1.38 (1.17–1.62) | 1.33 (1.12–1.58) | 0.0168 | 0.9136 |
| All subjects with imputation | |||||||
| Multivariate HR (95% CI) d | 1.0 | 1.19 (1.04–1.37) | 1.25 (1.07–1.45) | 1.37 (1.17–1.61) | 1.32 (1.12–1.57) | 0.0163 | 0.9955 |
| Men | |||||||
| Person-years | 84,194 | 85,223 | 85,971 | 84,029 | 85,292 | ||
| Cases | 22 | 30 | 25 | 37 | 34 | ||
| Crude HR (95% CI) | 1.0 | 1.37 (0.79–2.37) | 1.13 (0.64–2.00) | 1.72 (1.02–2.92) | 1.59 (0.93–2.72) | 0.1237 | |
| Multivariate HR (95% CI) d | 1.0 | 1.39 (0.76–2.54) | 1.10 (0.56–2.15) | 1.53 (0.77–3.04) | 1.32 (0.64–2.71) | 0.9183 | |
| Men with imputation | |||||||
| Multivariate HR (95% CI) d | 1.0 | 1.35 (0.74–2.44) | 1.07 (0.55–2.07) | 1.52 (0.78–2.99) | 1.27 (0.63–2.60) | 0.9795 | |
| Women | |||||||
| Person-years | 163,529 | 153,186 | 150,962 | 150,391 | 138,618 | ||
| Cases | 418 | 461 | 492 | 541 | 512 | ||
| Crude HR (95% CI) | 1.0 | 1.20 (1.05–1.36) | 1.30 (1.15–1.49) | 1.45 (1.28–1.65) | 1.53 (1.35–1.72) | <0.0001 | |
| Multivariate HR (95% CI) d | 1.0 | 1.20 (1.04–1.39) | 1.26 (1.08–1.48) | 1.37 (1.16–1.62) | 1.33 (1.11–1.59) | 0.0147 | |
| Women with imputation | |||||||
| Multivariate HR (95% CI) d | 1.0 | 1.18 (1.03–1.37) | 1.26 (1.08–1.47) | 1.37 (1.16–1.61) | 1.33 (1.11–1.58) | 0.0136 | |
| Menopausal Status | Quintiles of Dietary Inflammatory Index (DII) a | P Trend b | P Int c | ||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | |||
| Pre/peri-menopause | 1.0 d | 0.98 (0.67–1.43) | 1.13 (0.73–1.77) | 1.13 (0.73 -1.77) | 1.39 (0.87–2.21) | 0.1655 | 0.4033 |
| Postmenopause | 1.0 d | 1.24 (1.05–1.46) | 1.36 (1.14–1.62) | 1.41 (1.17–1.70) | 1.33 (1.09–1.63) | 0.0723 | |
| Menopausal status with imputation | |||||||
| Pre/peri-menopause | 1.0 d | 0.97 (0.67–1.42) | 0.98 (0.65–1.47) | 1.14 (0.74–1.77) | 1.37 (0.87–2.18) | 0.1421 | 0.3522 |
| Post-menopause | 1.0 d | 1.23 (1.04–1.44) | 1.35 (1.13–1.60) | 1.40 (1.16–1.68) | 1.33 (1.09–1.61) | 0.0820 | |
| Physical Activity | Quintiles of Dietary Inflammatory Index (DII) a | P Trend b | P Int c | ||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | |||
| All subject | |||||||
| Irregular | 1.0 d | 1.26 (1.01–1.58) | 1.39 (1.10–1.77) | 1.47 (1.14–1.90) | 1.49 (1.14–1.93) | 0.0521 | 0.6866 |
| Regular | 1.0 d | 1.17 (0.98–1.41) | 1.15 (0.94–1.41) | 1.31 (1.05–1.63) | 1.21 (0.96–1.53) | 0.1408 | |
| All subject with imputation | |||||||
| Irregular | 1.0 d | 1.27(1.02–1.59) | 1.41 (1.12–1.79) | 1.50 (1.17–1.93) | 1.51 (1.16–1.95) | 0.0345 | 0.5304 |
| Regular | 1.0 d | 1.16(0.97–1.39) | 1.15 (0.94–1.41) | 1.29 (1.04–1.60) | 1.21 (0.96–1.52) | 0.1749 | |
| Men | |||||||
| Irregular | 1.0 d | 0.76(0.28–2.03) | 0.83 (0.30–2.26) | 0.75 (0.26–2.17) | 0.86 (0.30–2.53) | 0.6626 | 0.7958 |
| Regular | 1.0 d | 2.03(0.93–4.40) | 1.33 (0.54–3.29) | 2.53 (1.03–6.20) | 1.67 (0.63–4.46) | 0.5958 | |
| Men with imputation | |||||||
| Irregular | 1.0 d | 0.72 (0.27–1.87) | 0.80 (0.30–2.13) | 0.73 (0.26–2.05) | 0.84 (0.30–2.38) | 0.5999 | |
| Regular | 1.0 d | 2.01 (0.93–4.37) | 1.32 (0.54–3.27) | 2.50 (1.02–6.13) | 1.65 (0.62–4.40) | 0.6155 | 0.6514 |
| Women | |||||||
| Irregular | 1.0 d | 1.30 (1.03–1.64) | 1.44 (1.12–1.84) | 1.53 (1.18–1.99) | 1.53 (1.17–2.01) | 0.0340 | |
| Regular | 1.0 d | 1.13 (0.94–1.37) | 1.15 (0.93–1.41) | 1.26 (1.00–1.57) | 1.19 (0.93–1.52) | 0.1720 | 0.6398 |
| Women with imputation | |||||||
| Irregular | 1.0 d | 1.32 (1.05–1.66) | 1.47 (1.15–1.87) | 1.57 (1.22–2.03) | 1.56 (1.20–2.04) | 0.0202 | 0.4769 |
| Regular | 1.0 d | 1.12 (0.93–1.34) | 1.14 (0.93–1.40) | 1.24 (0.99–1.55) | 1.19 (0.93–1.51) | 0.2093 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Sohn, C.; Kwon, M.; Na, W.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive Association between Dietary Inflammatory Index and the Risk of Osteoporosis: Results from the KoGES_Health Examinee (HEXA) Cohort Study. Nutrients 2018, 10, 1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121999
Kim HS, Sohn C, Kwon M, Na W, Shivappa N, Hébert JR, Kim MK. Positive Association between Dietary Inflammatory Index and the Risk of Osteoporosis: Results from the KoGES_Health Examinee (HEXA) Cohort Study. Nutrients. 2018; 10(12):1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121999
Chicago/Turabian StyleKim, Hye Sun, Cheongmin Sohn, Minji Kwon, Woori Na, Nitin Shivappa, James R. Hébert, and Mi Kyung Kim. 2018. "Positive Association between Dietary Inflammatory Index and the Risk of Osteoporosis: Results from the KoGES_Health Examinee (HEXA) Cohort Study" Nutrients 10, no. 12: 1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10121999