Erythrocyte n-6 Fatty Acids and Risk for Cardiovascular Outcomes and Total Mortality in the Framingham Heart Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Covariates and Mortality Outcomes
2.3. RBC Fatty Acid Analysis
2.4. Statistical Analysis
3. Results
3.1. Cohort Description
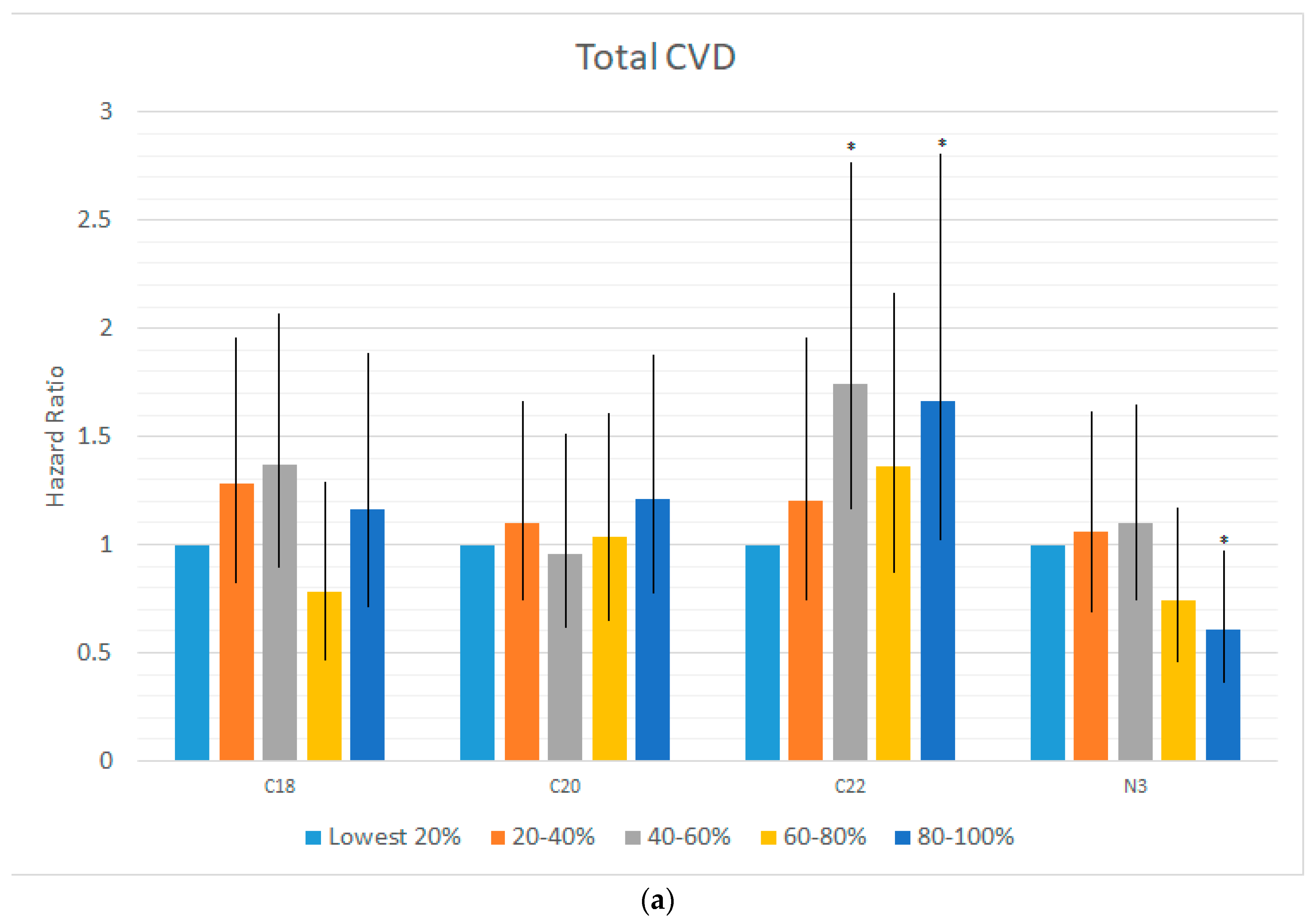
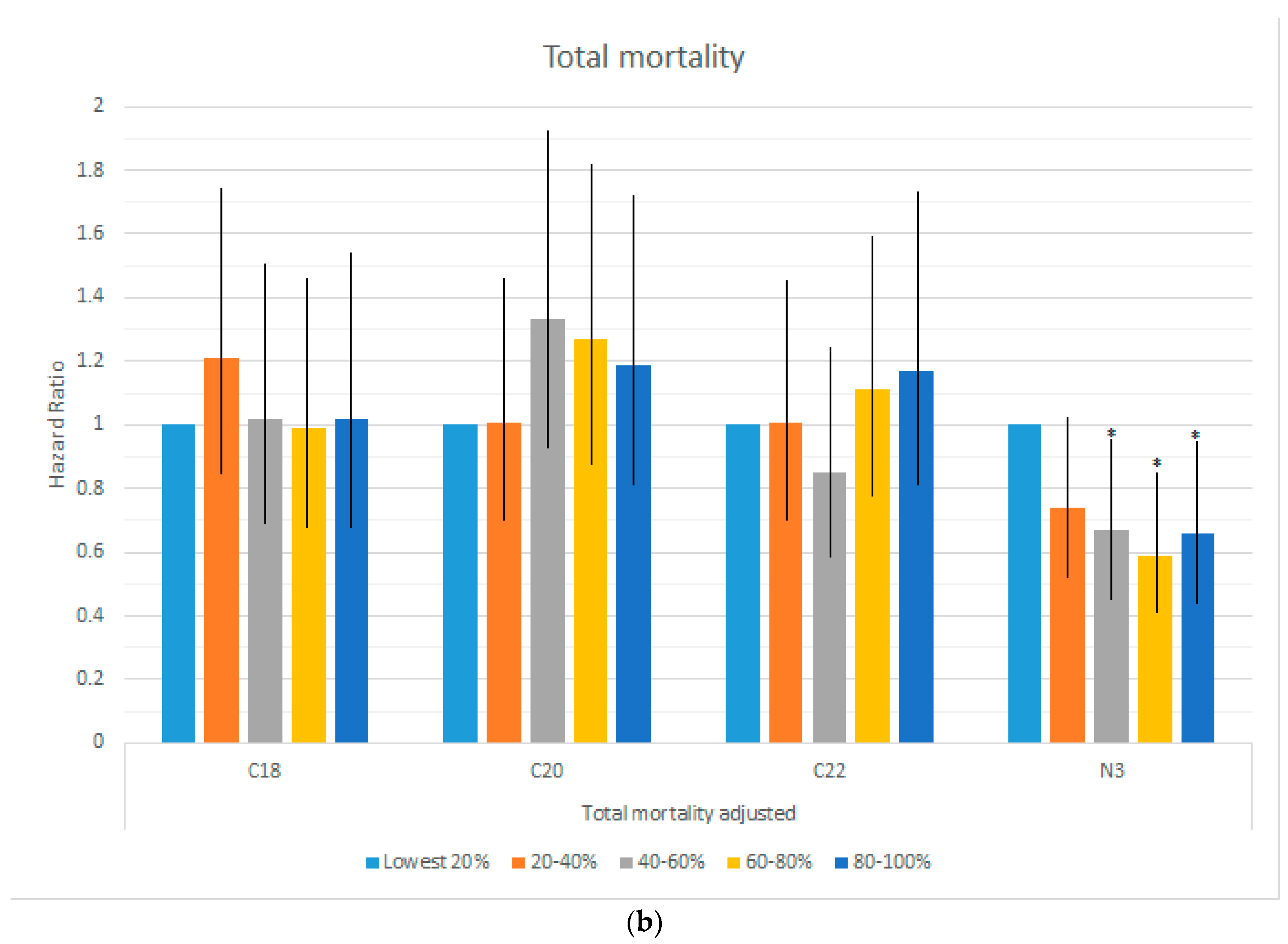
3.2. Omega-6 Fatty Acids and Mortality and Cardiovascular Disease Risk
3.3. Additional Fatty Acid Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADA | adrenic acid |
| AA | arachidonic acid |
| CVD | cardiovascular disease |
| DGLA | dihomo-gamma linolenic acid |
| DHA | docosahexaenoic acid |
| DPA n-6 | docosapentaenoic acid |
| EDA | eicosadienoic acid |
| EPA | eicosapentaenoic acid |
| FA | fatty acid |
| GLA | gamma-linolenic acid |
| HR | hazard ratio |
| LA | linoleic acid |
| MI | myocardial infarction |
| Omega-3 Index | erythrocyte EPA + DHA |
| PUFA | polyunsaturated FA |
| RBC | red blood cell |
| SD | standard deviation |
References
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann. Int. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef]
- Farvid, M.S.; Ding, M.; Pan, A.; Sun, Q.; Chiuve, S.E.; Steffen, L.M.; Willett, W.C.; Hu, F.B. Dietary linoleic acid and risk of coronary heart disease: A systematic review and meta-analysis of prospective cohort studies. Circulation 2014, 130, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.Y.; Marklund, M.; Imamura, F.; Tintle, N.; Korat, A.V.A.; De Goede, J.; Zhou, X.; Yang, W.S.; de Oliveira Otto, M.C.; Kröger, J.; et al. Omega-6 fatty acid biomarkers and incident type 2 diabetes: Pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies. Lancet Diabetes Endocrinol. 2017, 5, 965–974. [Google Scholar] [CrossRef]
- Ramsden, C.E.; Zamora, D.; Leelarthaepin, B.; Majchrzak-Hong, S.F.; Faurot, K.R.; Suchindran, C.M.; Ringel, A.; Davis, J.M.; Hibbein, J.R. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: Evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ 2013, 346, e8707. [Google Scholar] [CrossRef] [PubMed]
- Blasbalg, T.L.; Hibbeln, J.R.; Ramsden, C.E.; Majchrzak, S.F.; Rawlings, R.R. Changes in consumption of omega-3 and omega-6 fatty acids in the United States during the 20th century. Am. J. Clin. Nutr. 2011, 93, 950–962. [Google Scholar] [CrossRef] [Green Version]
- Lands, B. A critique of paradoxes in current advice on dietary lipids. Prog. Lipid. Res. 2008, 47, 77–106. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef]
- Yagi, S.; Aihara, K.I.; Fukuda, D.; Takashima, A.; Bando, M.; Hara, T.; Nishimoto, S.; Ise, T.; Kusunose, K.; Yamaguchi, K.; et al. Reduced ratio of eicosapentaenoic acid and docosahexaenoic acid to arachidonic acid is associated with early onset of acute coronary syndrome. Nutr. J. 2015, 14, 111. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S. The omega-6/omega-3 ratio and cardiovascular disease risk: Uses and abuses. Curr. Atheroscler. Rep. 2006, 8, 453–459. [Google Scholar] [CrossRef]
- Stanley, J.C.; Elsom, R.L.; Calder, P.C.; Griffin, B.A.; Harris, W.S.; Jebb, S.A.; Lovegrove, J.A.; Moore, C.S.; Riemersma, R.A.; Sanders, T.A.B. UK Food Standards Agency Workshop Report: The effects of the dietary n-6:n-3 fatty acid ratio on cardiovascular health. Br. J. Nutr. 2007, 98, 1305–1310. [Google Scholar] [CrossRef]
- Harris, W.S.; Shearer, G.C. Omega-6 fatty acids and cardiovascular disease: Friend, not foe? Circulation 2014, 130, 1562–1564. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S. The Omega-6:Omega-3 ratio: A critical appraisal and possible successor. Prostaglandins Leukot. Essent. Fat. Acids 2018, 132, 34–40. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Ascherio, A.; Hu, F.B.; Stampfer, M.J.; Willett, W.C.; Siscovick, D.S.; Rimm, E.B. Interplay Between Different Polyunsaturated Fatty Acids and Risk of Coronary Heart Disease in Men. Circulation 2005, 111, 157–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, G.H.; Fritsche, K. Effect of dietary linoleic acid on markers of inflammation in healthy persons: A systematic review of randomized controlled trials. J. Acad. Nutr. Diet. 2012, 112, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Kakutani, S.; Ishikura, Y.; Tateishi, N.; Horikawa, C.; Tokuda, H.; Kontani, M.; Kawashima, H.; Sakakibara, Y.; Kiso, Y.; Shibata, H.; et al. Supplementation of arachidonic acid-enriched oil increases arachidonic acid contents in plasma phospholipids, but does not increase their metabolites and clinical parameters in Japanese healthy elderly individuals: A randomized controlled study. Lipids Health Dis. 2011, 10, 241. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; von Schacky, C. The Omega-3 Index: A new risk factor for death from coronary heart disease? Prev. Med. 2004, 39, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Tintle, N.L.; Etherton, M.R.; Vasan, R.S. Erythrocyte long-chain omega-3 fatty acid levels are inversely associated with mortality and with incident cardiovascular disease: The Framingham Heart Study. J. Clin. Lipidol. 2018, 12, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Feinleib, M.; McNamara, P.M.; Garrison, R.J.; Castelli, W.P. An investigation of coronary heart disease in families. The Framingham offspring study. Am. J. Epidemiol. 1979, 110, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Splansky, G.L.; Corey, D.; Yang, Q.; Atwood, L.D.; Cupples, L.A.; Benjamin, E.J.; D'Agostino, R.B., Sr.; Fox, S.C.; Larson, M.G.; Murabito, J.M.; et al. The Third Generation Cohort of the National Heart, Lung, and Blood Institute′s Framingham Heart Study: Design, recruitment, and initial examination. Am. J. Epidemiol. 2007, 165, 1328–1335. [Google Scholar] [CrossRef]
- Harris, W.S.; Pottala, J.V.; Vasan, R.S.; Larson, M.G.; Robins, S.J. Changes in erythrocyte membrane trans and marine fatty acids between 1999 and 2006 in older Americans. J. Nutr. 2012, 142, 1297–1303. [Google Scholar] [CrossRef]
- R. Version 3; Software for Statistical Analysis; The R-Project for Statistical Computing. Available online: www.r-project.org (accessed on 19 December 2018).
- Delgado, G.E.; Marz, W.; Lorkowski, S.; von Schacky, C.; Kleber, M.E. Omega-6 fatty acids: Opposing associations with risk-The Ludwigshafen Risk and Cardiovascular Health Study. J. Clin. Lipidol. 2017, 11, 1082–1090. [Google Scholar] [CrossRef]
- Shearer, G.C.; Pottala, J.V.; Spertus, J.A.; Harris, W.S. Red blood cell fatty acid patterns and acute coronary syndrome. PLoS ONE 2009, 4, e5444. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Kennedy, K.F.; O′Keefe, J.H., Jr.; Spertus, J.A. Red blood cell fatty acid levels improve GRACE score prediction of 2-yr mortality in patients with myocardial infarction. Int. J. Cardiol. 2013, 168, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Sitkin, S.; Pokrotnieks, J. Alterations in Polyunsaturated Fatty Acid Metabolism and Reduced Serum Eicosadienoic Acid Level in Ulcerative Colitis: Is There a Place for Metabolomic Fatty Acid Biomarkers in IBD? Dig. Dis. Sci. 2018, 63, 2480–2481. [Google Scholar] [CrossRef] [PubMed]
- Forouhi, N.G.; Imamura, F.; Sharp, S.J.; Koulman, A.; Schulze, M.B.; Zheng, J.; Ye, Z.; Sluijs, I.; Guevara, M.; Huerta, J.M.; et al. Association of Plasma Phospholipid n-3 and n-6 Polyunsaturated Fatty Acids with Type 2 Diabetes: The EPIC-InterAct Case-Cohort Study. PLoS Med. 2016, 13, e1002094. [Google Scholar] [CrossRef] [PubMed]
- Shearer, G.C.; Walker, R.E. An overview of the biologic effects of omega-6 oxylipins in humans. Prostaglandins. Leukot. Essent. Fat. Acids 2018, 137, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Thomas, R.M. Biological variability of blood omega-3 biomarkers. Clin. Biochem. 2010, 43, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S.; Kennedy, K.F.; Maddox, T.M.; Kutty, S.; Spertus, J.A. Multiple differences between patients who initiate fish oil supplementation post-myocardial infarction and those who do not: The TRIUMPH Study. Nutr. Res. 2016, 36, 65–71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Died (n = 350) | Still Living (n = 2150) | Total | p-Value for Difference (Chi-Squared or t-Test) |
|---|---|---|---|---|
| % (n) or Mean (SD) | % (n) or Mean (SD) | % (n) or Mean (SD) | ||
| Sex | ||||
| Male | 52.9% (185) | 41.5% (893) | 43.1% (1078) | <0.001 |
| Female | 47.1% (165) | 58.5% (1257) | 56.9% (1422) | |
| Age | 72.9 (8.6) | 64.4 (8.2) | 65.56 (8.76) | <0.001 |
| Body Mass Index (BMI) | 27.9 (5.9) | 28.3 (5.4) | 28.2 (5.4) | <0.001 |
| Marital Status | ||||
| Single/Never Married | 4.3% (15) | 6.7% (144) | 6.4% (159) | <0.001 |
| Married | 63.7% (223) | 70.7% (1519) | 69.7% (1742) | |
| Separated/Divorced | 12.0% (42) | 12.7% (273) | 12.6% (315) | |
| Widowed | 18.3% (64) | 9.4% (203) | 10.7% (267) | |
| Education | ||||
| Some High School (HS) or less | 6.0% (21) | 2.4% (51) | 2.9% (72) | <0.001 |
| HS graduate | 33.7% (118) | 24.8% (533) | 26.0% (651) | |
| Some college or vocational | 22.9% (78) | 21.9% (471) | 22.0% (549) | |
| College graduate | 36.6% (128) | 50.5% (1086) | 48.6% (1214) | |
| Employment | ||||
| Employed | 31.1% (109) | 56.3% (1210) | 52.8% (1319) | <0.001 |
| Disabled/unemployed | 3.1% (11) | 2.5% 53) | 2.6% (64) | |
| Retired | 64.3% (225) | 40.8% (877) | 44.1% (1102) | |
| Health insurance status | ||||
| No insurance | 2.3% (8) | 1.9% (40) | 1.9% (48) | 0.053 |
| Insurance, but no prescription | 11.4% (40) | 8.4% (181) | 8.8% (221) | |
| Full insurance | 84.0% (294) | 88.7% (1906) | 88.0% (2200) | |
| Regular aspirin use | 49.7% (174) | 38.6% (830) | 40.2% (1004) | <0.001 |
| Prevalent hypertension | 57.1% (200) | 42.2% (908) | 44.3% (1108) | <0.001 |
| Cholesterol medication | 41.4% (145) | 36.9% (794) | 37.6% (939) | 0.06 |
| Prevalent diabetes | 22.3% (78) | 11.6% (249) | 13.1% (327) | <0.001 |
| Alcohol consumption | ||||
| None | 34.0% (119) | 23.2% (499) | 24.7% (618) | <0.001 |
| <1 drink/day | 36.0% (126) | 50.7% (1089) | 48.6% (1215) | |
| 1–2 drinks/day | 22.6% (79) | 20.2% (434) | 20.5% (513) | |
| >2 drinks/day | 6.9% (24) | 5.7% (123) | 5.9% (147) | |
| Smoking | ||||
| Not current smoker | 89.1% (312) | 90.5% (1946) | 90.3% (2258) | 0.70 |
| Current | 10.6% (37) | 9.3% (200) | 9.5% (237) | |
| METS | 4.7 (15.4) | 3.3 (8.6) | 3.5 (9.9) | <0.001 |
| Total to High-Density Lipoprotein (HDL) cholesterol ratio | 3.5 (1.1) | 3.5 (1.0) | 3.5 (1.1) | <0.001 |
| Systolic Blood Pressure | 133.6 (19.8) | 128.2 (16.9) | 129.0 (17.4) | <0.001 |
| C-reactive protein | 4.9 (12.7) | 3.0 (6.1) | 3.3 (7.4) | <0.001 |
| Omega-3 index | 0.054 (0.017) | 0.056 (0.017) | 0.0554 (0.0168) | <0.001 |
| (a) | |||||||
| Total Events | Mortality | ||||||
| CVD | CHD | Stroke | CVD | Cancer | Other | Total | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| A. Unadjusted | |||||||
| <9.8% 18-carbon (n = 433) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 9.8%–10.7% (n = 488) | 1.07 (0.71, 1.61) | 1.30 (0.72, 2.35) | 1.28 (0.67, 2.43) | 1.14 (0.45, 2.89) | 0.96 (0.58, 1.58) | 0.56 (0.31, 1.02) | 0.92 (0.64, 1.31) |
| 10.7%–11.5% (n = 522) | 1.05 (0.71, 1.57) | 1.08 (0.59, 1.98) | 1.33 (0.72, 2.43) | 0.86 (0.33, 2.19) | 0.81 (0.48, 1.36) | 0.51 (0.29, 0.92) * | 0.77 (0.54, 1.11) |
| 11.5%–12.5% (n = 522) | 0.74 (0.48, 1.13) | 0.80 (0.42, 1.52) | 0.70 (0.35, 1.38) | 1.74 (0.71, 4.25) | 0.56 (0.32, 1.00) | 0.86 (0.53, 1.39) | 0.94 (0.67, 1.31) |
| >12.5% (n = 535) | 0.73 (0.48, 1.13) | 1.01 (0.56, 1.81) | 0.80 (0.39, 1.63) | 0.57 (0.22, 1.53) | 0.74 (0.43, 1.25) | 0.52 (0.29, 0.93) * | 0.74 (0.52, 1.06) |
| p-value for linear trend | 0.032 * | 0.45 | 0.15 | 0.26 | 0.08 | 0.17 | 0.14 |
| B. Adjusted for demos | |||||||
| <9.8% 18-carbon (n = 433) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 9.8%–10.7% (n = 488) | 1.28 (0.83, 1.95) | 1.42 (0.76, 2.67) | 1.46 (0.71, 3.00) | 1.19 (0.48, 2.96) | 1.09 (0.63, 1.88) | 0.87 (0.47, 1.60) | 1.21 (0.84, 1.73) |
| 10.7%–11.5% (n = 522) | 1.37 (0.90, 2.08) | 1.38 (0.74, 2.56) | 1.51 (0.77, 2.96) | 1.12 (0.42, 2.97) | 0.89 (0.49, 1.61) | 0.83 (0.45, 1.56) | 1.02 (0.69, 1.50) |
| 11.5%–12.5% (n = 522) | 0.78 (0.48, 1.27) | 0.96 (0.46, 2.02) | 0.72 (0.33, 1.61) | 1.59 (0.67, 3.75) | 0.65 (0.35, 1.20) | 1.02 (0.58, 1.80) | 0.99 (0.68, 1.44) |
| >12.5% (n = 535) | 1.16 (0.72, 1.89) | 1.53 (0.75, 3.13) | 1.12 (0.52, 2.40) | 0.96 (0.33, 2.80) | 0.88 (0.47, 1.65) | 0.62 (0.29, 1.33) | 1.02 (0.68, 1.53) |
| p-value for linear trend | 0.68 | 0.59 | 0.49 | 0.68 | 0.30 | 0.42 | 0.69 |
| C. Adjusted for demos and O3I | |||||||
| <9.8% 18-carbon (n = 433) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 9.8%–10.7% (n = 488) | 1.19 (0.78, 1.82) | 1.32 (0.70, 2.49) | 1.29 (0.62, 2.66) | 1.08 (0.43, 2.73) | 1.07 (0.62, 1.87) | 0.74 (0.39, 1.41) | 1.14 (0.79, 1.64) |
| 10.7%–11.5% (n = 522) | 1.28 (0.84, 1.95) | 1.28 (0.69, 2.38) | 1.34 (0.67, 2.65) | 1.04 (0.38, 2.78) | 0.87 (0.47, 1.61) | 0.71 (0.38, 1.34) | 0.95 (0.64, 1.41) |
| 11.5%–12.5% (n = 522) | 0.71 (0.44, 1.16) | 0.86 (0.41, 1.79) | 0.62 (0.28, 1.39) | 1.49 (0.65, 3.44) | 0.64 (0.34, 1.19) | 0.83 (0.46, 1.50) | 0.92 (0.63, 1.34) |
| >12.5% (n = 535) | 1.03 (0.63, 1.67) | 1.32 (0.64, 2.73) | 0.93 (0.43, 2.03) | 0.78 (0.26, 2.34) | 0.86 (0.45, 1.63) | 0.52 (0.24, 1.11) | 0.92 (0.61, 1.40) |
| p-value for linear trend | 0.34 | 0.92 | 0.23 | 0.87 | 0.28 | 0.18 | 0.38 |
| p-value for omega-3 | 0.005 ** | 0.034 * | 0.004 ** | 0.10 | 0.70 | 0.004 ** | 0.011 |
| (b) | |||||||
| Total Events | Mortality | ||||||
| CVD | CHD | Stroke | CVD | Cancer | Other | Total | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| A. Unadjusted | |||||||
| <17.5% 20-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 17.5%–18.4% (n = 509) | 1.03 (0.71, 1.50) | 0.95 (0.53, 1.70) | 0.96 (0.54, 1.70) | 1.19 (0.54, 2.62) | 0.80 (0.48, 1.32) | 0.84 (0.49, 1.46) | 0.89 (0.65, 1.22) |
| 18.4%–19.1% (n = 502) | 0.92 (0.61, 1.39) | 0.95 (0.52, 1.71) | 0.78 (0.41, 1.49) | 0.83 (0.31, 2.20) | 0.90 (0.53, 1.53) | 1.59 (0.94, 2.67) | 1.16 (0.83, 1.63) |
| 19.1%–19.9% (n = 502) | 0.88 (0.58, 1.33) | 1.22 (0.71, 2.09) | 0.63 (0.32, 1.24) | 1.24 (0.55, 2.80) | 0.87 (0.52, 1.46) | 1.19 (0.67, 2.09) | 1.02 (0.73, 1.42) |
| >19.9% (n = 479) | 1.03 (0.70, 1.52) | 0.99)0.55, 1.77) | 1.04 (0.59, 1.82) | 0.77 (0.37, 1.60) | 0.92 (0.55, 1.53) | 1.14 (0.65, 2.01) | 0.95 (0.69, 1.33) |
| p-value for linear trend | 0.82 | 0.71 | 0.68 | 0.54 | 0.83 | 0.32 | 0.90 |
| B. Adjusted for demos | |||||||
| <17.5% 20-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 17.5%–18.4% (n = 509) | 1.10 (0.74, 1.65) | 0.96 (0.52, 1.75) | 1.19 (0.62, 2.30) | 1.58 (0.61, 4.11) | 0.84 (0.49, 1.42) | 0.86 (0.45, 1.67) | 1.01 (0.71, 1.44) |
| 18.4%–19.1% (n = 502) | 0.96 (0.61, 1.51) | 0.93 (0.49, 1.79) | 1.09 (0.54, 2.21) | 1.23 (0.38, 4.02) | 0.98 (0.53, 1.81) | 1.91 (1.08, 3.36) * | 1.33 (0.92, 1.92) |
| 19.1%–19.9% (n = 502) | 1.04 (0.67, 1.61) | 1.29 (0.71, 2.36) | 0.88 (0.43, 1.80) | 1.98 (0.75, 5.19) | 1.02 (0.58 1.78) | 1.45 (0.77, 2.70) | 1.27 (0.88, 1.81) |
| >19.9% (n = 479) | 1.21 (0.78, 1.88) | 1.06 (0.56, 2.02) | 1.48 (0.75, 2.92) | 1.19 (0.44, 3.21) | 1.21 (0.69, 2.13) | 1.40 (0.75, 2.61) | 1.19 (0.82, 1.73) |
| p-value for linear trend | 0.52 | 0.52 | 0.53 | 0.55 | 0.42 | 0.11 | 0.16 |
| C. Adjusted for demos and O3I | |||||||
| <17.5% 20-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 17.5%–18.4% (n = 509) | 0.97 (0.65, 1.46) | 0.84 (0.46, 1.51) | 0.96 (0.50, 1.86) | 1.30 (0.47, 3.61) | 0.84 (0.49, 1.44) | 0.77 (0.40, 1.51) | 0.94 (0.65, 1.36) |
| 18.4%–19.1% (n = 502) | 0.81 (0.51, 1.30) | 0.77 (0.39, 1.51) | 0.82 (0.39, 1.72) | 0.99 (0.28, 3.55) | 0.99 (0.52, 1.88) | 1.62 (0.92, 2.86) | 1.19 (0.81, 1.75) |
| 19.1%–19.9% (n = 502) | 0.85 (0.53, 1.34) | 1.03 (0.55, 1.91) | 0.61 (0.28, 1.33) | 1.55 (0.56, 4.30) | 1.03 (0.57, 1.86) | 1.17 (0.60, 2.27) | 1.12 (0.76, 1.65) |
| >19.9% (n = 479) | 0.97 (0.60, 1.56) | 0.82 (0.41, 1.65) | 1.03 (0.49, 2.15) | 0.85 (0.27, 2.72) | 1.23 (0.67, 2.26) | 1.12 (0.58, 2.16) | 1.04 (0.70, 1.56) |
| p-value for linear trend | 0.72 | 0.87 | 0.91 | 0.89 | 0.42 | 0.44 | 0.58 |
| p-value for omega-3 | 0.011 * | 0.039 * | 0.009 ** | 0.13 | 0.87 | 0.03 * | 0.04 * |
| (c) | |||||||
| Total Events | Mortality | ||||||
| CVD | CHD | Stroke | CVD | Cancer | Other | Total | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| A. Unadjusted | |||||||
| <3.6% 22-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 3.6%–4.3% (n = 508) | 1.37 (0.88, 2.12) | 1.24 (0.63, 2.43) | 1.25 (0.62, 2.53) | 0.93 (0.42, 2.03) | 0.86 (0.52, 1.42) | 1.11 (0.64, 1.93) | 0.96 (0.69, 1.31) |
| 4.3%–4.7% (n = 500) | 1.73 (1.14, 2.62) ** | 2.43 (1.34, 4.42) ** | 1.36 (0.71, 2.61) | 0.81 (0.35, 1.83) | 0.65 (0.38, 1.13) | 0.96 (0.53, 1.73) | 0.80 (0.57, 1.13) |
| 4.7%–5.3% (n = 509) | 1.46 (0.96, 2.22) | 1.61 (0.86, 3.03) | 1.58 (0.83, 2.98) | 1.16 (0.54, 2.49) | 0.78 (0.46, 1.31) | 1.27 (0.72, 2.26) | 1.04 (0.75, 1.45) |
| >5.3% (n = 469) | 1.73 (1.12, 2.68) * | 2.25 (1.22, 4.16) ** | 1.48 (0.74, 2.98) | 0.63 (0.24, 1.67) | 1.18 (0.71, 1.95) | 1.43 (0.82, 2.50) | 1.10 (0.77, 1.56) |
| p-value for linear trend | 0.02 * | 0.006 ** | 0.18 | 0.57 | 0.74 | 0.17 | 0.48 |
| B. Adjusted for demos | |||||||
| <3.6% 22-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 3.6%–4.3% (n = 508) | 1.20 (0.75, 1.93) | 1.05 (0.50, 2.20) | 1.39 (0.62, 3.13) | 0.83 (0.28, 2.41) | 0.94 (0.56, 1.60) | 1.06 (0.60, 1.88) | 1.01 (0.71, 1.44) |
| 4.3%–4.7% (n = 500) | 1.74 (1.13, 2.67) * | 2.38 (1.26,4.48) ** | 1.73 (0.85, 3.55) | 0.65 (0.26, 1.62) | 0.74 (0.41, 1.32) | 0.85 (0.41, 1.76) | 0.85 (0.58, 1.25) |
| 4.7%–5.3% (n = 509) | 1.36 (0.87, 2.13) | 1.51 (0.76, 2.99) | 1.89 (0.92, 3.87) | 1.28 (0.62, 2.62) | 0.74 (0.41, 1.31) | 1.31 (0.68, 2.51) | 1.11 (0.78, 1.59) |
| >5.3% (n = 469) | 1.66 (1.02, 2.69) * | 1.91 (0.95, 3.83) | 2.01 (0.92, 4.42) | 0.60 (0.18, 2.01) | 1.21 (0.71, 2.07) | 1.53 (0.85, 2.74) | 1.17 (0.81, 1.71) |
| p-value for linear trend | 0.031 * | 0.04 * | 0.04 * | 0.80 | 0.91 | 0.10 | 0.32 |
| C. Adjusted for demos and O3I | |||||||
| <3.6% 22-carbon (n = 508) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 3.6%–4.3% (n = 508) | 1.11 (0.69, 1.79) | 0.99 (0.48, 2.05) | 1.20 (0.53, 2.69) | 0.62 (0.20, 1.95) | 0.93 (0.54, 1.60) | 0.89 (0.48, 1.63) | 0.89 (0.62, 1.29) |
| 4.3%–4.7% (n = 500) | 1.52 (0.96, 2.39) | 2.09 (1.07, 4.06) * | 1.35 (0.65, 2.80) | 0.42 (0.17, 1.06) | 0.72 (0.38, 1.36) | 0.67 (0.32, 1.42) | 0.69 (0.45, 1.05) |
| 4.7%–5.3% (n = 509) | 1.14 (0.70, 1.86) | 1.25 (0.60, 2.62) | 1.37 (0.64, 2.97) | 0.69 (0.27, 1.76) | 0.71 (0.38, 1.34) | 0.97 (0.48, 1.94) | 0.87 (0.58, 1.30) |
| >5.3% (n = 469) | 1.33 (0.77, 2.28) | 1.51 (0.69, 3.30) | 1.38 (0.60, 3.18) | 0.30 (0.07, 1.26) | 1.15 (0.57, 2.33) | 0.98 (0.48, 1.98) | 0.85 (0.54, 1.34) |
| p-value for linear trend | 0.42 | 0.34 | 0.44 | 0.14 | 0.97 | 0.88 | 0.57 |
| p-value for omega-3 | 0.09 | 0.22 | 0.049 * | 0.034 * | 0.92 | 0.03 * | 0.021 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harris, W.S.; Tintle, N.L.; Ramachandran, V.S. Erythrocyte n-6 Fatty Acids and Risk for Cardiovascular Outcomes and Total Mortality in the Framingham Heart Study. Nutrients 2018, 10, 2012. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122012
Harris WS, Tintle NL, Ramachandran VS. Erythrocyte n-6 Fatty Acids and Risk for Cardiovascular Outcomes and Total Mortality in the Framingham Heart Study. Nutrients. 2018; 10(12):2012. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122012
Chicago/Turabian StyleHarris, William S., Nathan L. Tintle, and Vasan S. Ramachandran. 2018. "Erythrocyte n-6 Fatty Acids and Risk for Cardiovascular Outcomes and Total Mortality in the Framingham Heart Study" Nutrients 10, no. 12: 2012. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122012