Trajectories of Mediterranean Diet Adherence and Risk of Hypertension in China: Results from the CHNS Study, 1997–2011


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurements
2.2.1. Dietary Assessment
2.2.2. Blood Pressure and Hypertension
2.2.3. Other Variables
2.3. Statistical Analysis
3. Results
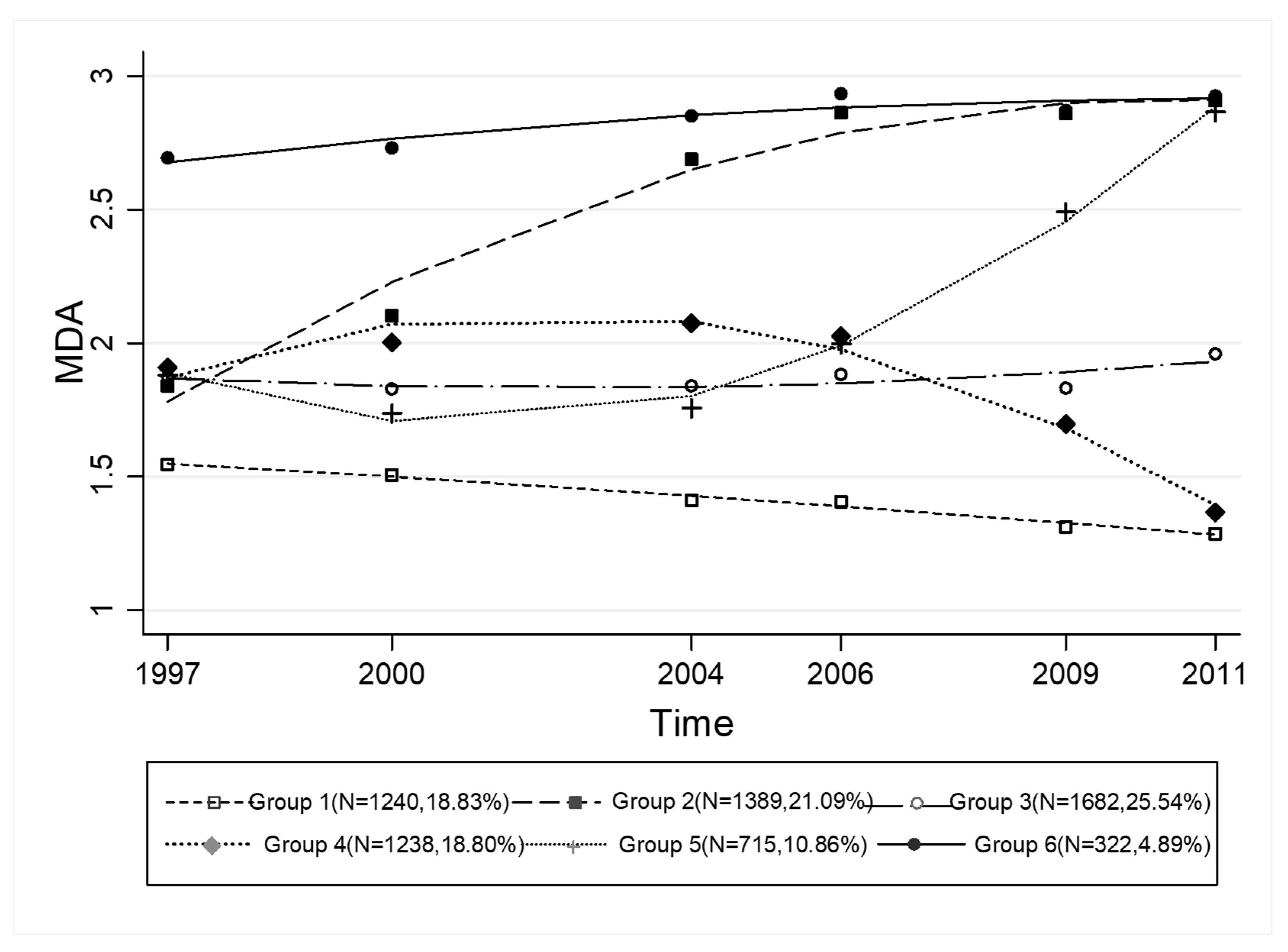
3.1. Trajectories of MDA
3.2. Participants’ Characteristics by Trajectory Groups
3.3. Trajectories of MDA and BP Change
3.4. MDA and the Risk of Hypertension
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferroluzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Paletas, K.; Athanasiadou, E.; Sarigianni, M.; Paschos, P.; Kalogirou, A.; Hassapidou, M.; Tsapas, A. The protective role of the Mediterranean diet on the prevalence of metabolic syndrome in a population of Greek obese subjects. J. Am. Coll. Nutr. 2010, 29, 41–45. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.H.; Chrysohoou, C.; Skoumas, J.; Papadimitriou, L.; Stefanadis, C.; Toutouzas, P.K. Status and management of hypertension in Greece: Role of the adoption of a Mediterranean diet the Attica study. J. Hypertens. 2003, 21, 1483–1489. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Naska, A.; Orfanos, P.; Trichopoulos, D.; Mountokalakis, T.; Trichopoulou, A. Olive oil, the Mediterranean diet, and arterial blood pressure: The Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2004, 80, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; Hu, F.B.; Estruch, R.; Buil-Cosiales, P.; Corella, D.; Salas-Salvadó, J.; Covas, M.I.; Arós, F.; Gómez-Gracia, E.; Fiol, M. Effect of the Mediterranean diet on blood pressure in the PREDIMED trial: Results from a randomized controlled trial. BMC Med. 2013, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Perona, J.S.; Cañizares, J.; Montero, E.; Sánchezdomínguez, J.M.; Catalá, A.; Ruizgutiérrez, V. Virgin olive oil reduces blood pressure in hypertensive elderly subjects. Clin. Nutr. 2004, 23, 1113–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Martinezgonzalez, M.A.; Corella, D.; Salassalvado, J.; Ruizgutierrez, V.; Covas, M.I.; Fiol, M.; Gomezgracia, E.; Lopezsabater, M.C.; Vinyoles, E. Effects of a Mediterranean-Style Diet on Cardiovascular Risk Factors: A. Randomized Trial. Ann. Int. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Suterzimmermann, K.; Bucher, H.C.; Shai, I.; Tuttle, K.R.; Estruch, R.; Briel, M. Meta-Analysis Comparing Mediterranean to Low-Fat Diets for Modification of Cardiovascular Risk Factors. Am. J. Med. 2011, 124, 841–851. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2571. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. New Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; Wang, H.; Du, S.; He, Y.; Wang, Z.; Ge, K.; Popkin, B.M. Prospective study on nutrition transition in China. Nutr. Rev. 2010, 67, S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Byles, J.E.; Shi, Z.; Hall, J.J. Evaluation of older Chinese people's macronutrient intake status: Results from the China Health and Nutrition Survey. Br. J. Nutr. 2015, 113, 1–13. [Google Scholar] [CrossRef]
- Ma, L.; Wu, Y.; Wang, W.; Chen, W. Interpretation of the report on cardiovascular diseases in China (2017). Chin. J. Cardiovasc. Med. 2018, 3–6. [Google Scholar]
- Appel, L.J.; Brands, M.W.; Daniels, S.R.; Karanja, N.; Elmer, P.J.; Sacks, F.M. Dietary approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension 2006, 47, 296–308. [Google Scholar] [CrossRef]
- Oh, J.; Hong, N.; Kang, S.M. Dietary therapy in hypertension. New Engl. J. Med. 2010, 362, 2102–2112. [Google Scholar]
- Appel, L.J.; Miller, E.R.; Seidler, A.J.; Whelton, P.K. Does Supplementation of Diet With 'Fish Oil' Reduce Blood Pressure? A Meta-analysis of Controlled Clinical Trials. JAMA Int. Med. 1993, 153, 1429–1438. [Google Scholar] [CrossRef]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS). Nutrients 2015, 7, 8170–8188. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Gordon-Larsen, P.; Siega-Riz, A.M.; Cai, J.; Wang, H.; Adair, L.S.; Popkin, B.M. Sociodemographic disparity in the diet quality transition among Chinese adults from 1991 to 2011. Eur. J. Clin. Nutr. 2016, 71, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Núñezcórdoba, J.M.; Valenciaserrano, F.; Toledo, E.; Alonso, A.; Martínezgonzález, M.A. The Mediterranean diet and incidence of hypertension: The Seguimiento Universidad de Navarra (SUN) Study. Am. J. Epidemiol. 2009, 169, 339. [Google Scholar] [CrossRef] [PubMed]
- Batis, C.; Sotres-Alvarez, D.; Gordon-Larsen, P.; Mendez, M.A.; Adair, L.; Popkin, B. Longitudinal analysis of dietary patterns in Chinese adults from 1991 to 2009. Br. J. Nutr. 2014, 111, 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- Melaku, Y.A.; Gill, T.K.; Appleton, S.L.; Taylor, A.W.; Adams, R.; Shi, Z. Prospective Associations of Dietary and Nutrient Patterns with Fracture Risk: A 20-Year Follow-Up Study. Nutrients 2017, 9, 1198. [Google Scholar] [CrossRef]
- Fung, T.T.; Mccullough, M.L.; Newby, P.K.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Thomazella, M.C.D.; Góes, M.F.S.; Andrade, C.R.; Debbas, V.; Barbeiro, D.F.; Correia, R.L.; Marie, S.K.N.; Cardounel, A.J.; Daluz, P.L.; Laurindo, F.R.M. Effects of High Adherence to Mediterranean or Low-Fat Diets in Medicated Secondary Prevention Patients. Am. J. Cardiol. 2011, 108, 1523–1529. [Google Scholar] [CrossRef] [Green Version]
- Lau, K.K.; Wong, Y.K.; Chan, Y.H.; Li, O.Y.; Lee, P.Y.; Yuen, G.G.; Wong, Y.K.; Tong, S.; Wong, D.; Chan, K.H. Mediterranean-style diet is associated with reduced blood pressure variability and subsequent stroke risk in patients with coronary artery disease. Am. J. Hypertens. 2015, 28, 501–507. [Google Scholar] [CrossRef]
- Nissensohn, M.; Románviñas, B.; Sánchezvillegas, A.; Piscopo, S.; Serramajem, L. The Effect of the Mediterranean Diet on Hypertension: A Systematic Review and Meta-Analysis. J. Nutr. Educ. Behav. 2016, 48, 42–53. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J. Primary prevention of cardiovascular disease with a Mediterranean diet. New Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Doménech, M.; Roman, P.; Lapetra, J.; García de la Corte, F.J.; Sala-Vila, A.; De la Torre, R.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Lamuela-Raventós, R.-M. Mediterranean diet reduces 24-hour ambulatory blood pressure, blood glucose, and lipids: One-year randomized, clinical trial. Hypertension 2014, 64, 69–76. [Google Scholar] [CrossRef]
- Lelong, H.; Blacher, J.; Menai, M.; Galan, P.; Fezeu, L.; Hercberg, S.; Kesse-Guyot, E. Association between blood pressure and adherence to French dietary guidelines. Am. J. Hypertens. 2016, 29, 948–958. [Google Scholar] [CrossRef]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M. A clinical trial of the effects of dietary patterns on blood pressure. New Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.M.; Fitzgerald, A.P.; Kearney, P.M.; McCarthy, V.J.; Madden, J.; Browne, G.; Dolan, E.; Perry, I.J. DASH diet score and distribution of blood pressure in middle-aged men and women. Am. J. Hypertens. 2013, 26, 1311–1320. [Google Scholar] [PubMed]
- Martínez-González, M.Á.; De la Fuente-Arrillaga, C.; Nunez-Cordoba, J.; Basterra-Gortari, F.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef] [PubMed]
- León-Munoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to the Mediterranean Diet Pattern Has Declined in Spanish Adults–3. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef]


{kind=link}
| Group | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | chi2/F | p Value b |
|---|---|---|---|---|---|---|---|---|
| n | 1240 (18.83%) | 1389 (21.09%) | 1682 (25.54%) | 1238 (18.80%) | 715 (10.86%) | 322 (4.89%) | ||
| Gender (%) | 30.8 | <0.001 | ||||||
| Female | 48.79% | 43.52% | 52.51% | 45.67% | 48.55% | 41.25% | ||
| Male | 51.21% | 56.48% | 47.49% | 54.33% | 51.45% | 58.75% | ||
| Age a | 38.13 ± 13.92 | 25.00 ± 20.86 | 38.42 ± 17.27 | 34.54 ± 15.82 | 26.21 ± 10.20 | 20.50 ± 8.45 | 460.97 | <0.001 |
| Smoking status (%) | 227.14 | <0.001 | ||||||
| Noncurrent smokers | 71.31% | 81.97% | 73.40% | 71.82% | 90.77% | 84.69% | ||
| Current smokers | 28.69% | 18.03% | 26.60% | 28.18% | 9.23% | 15.31% | ||
| Exercise | 665.33 | <0.001 | ||||||
| Had not achieved 10 MET/h per person per week | 51.22% | 68.03% | 40.07% | 46.52% | 80.38% | 74.37% | ||
| Had achieved 10 MET/h per person per week | 48.78% | 31.97% | 59.93% | 53.48% | 19.62% | 25.63% |
| SBP | DBP | |||||||
|---|---|---|---|---|---|---|---|---|
| Coef. | p Value | 95% CI | Coef. | p Value | 95% CI | |||
| Low Adherence (reference group) | 0.00 | 0.00 | ||||||
| Group 2 | −13.40 | <0.001 | −14.51 | −12.29 | −7.57 | <0.001 | −8.26 | −6.89 |
| Group 3 | −0.12 | 0.803 | −1.04 | 0.80 | −0.03 | 0.908 | −0.59 | 0.53 |
| Group 4 | −0.65 | 0.328 | −1.97 | 0.66 | 0.11 | 0.782 | −0.68 | 0.91 |
| Group 5 | −7.75 | <0.001 | −8.90 | −6.59 | −4.50 | <0.001 | −5.20 | −3.79 |
| Group 6 | −8.44 | <0.001 | −11.15 | −5.72 | −3.64 | <0.001 | −5.33 | −1.95 |
| Age- and Gender-Adjusted a | Multivariate-Adjusted b | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | |||
| Group 1 (reference group) | 1.00 | 1.00 | ||||
| Group 2 | 0.29 | 0.22 | 0.39 | 0.32 | 0.23 | 0.42 |
| Group 3 | 0.96 | 0.85 | 1.09 | 0.96 | 0.84 | 1.08 |
| Group 4 | 0.92 | 0.77 | 1.10 | 0.92 | 0.77 | 1.10 |
| Group 5 | 0.73 | 0.61 | 0.88 | 0.75 | 0.63 | 0.91 |
| Group 6 | 0.15 | 0.08 | 0.29 | 0.17 | 0.09 | 0.32 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, M.; Wang, F.; Shen, Y.; Zhu, X.; Zhang, X.; Sun, X. Trajectories of Mediterranean Diet Adherence and Risk of Hypertension in China: Results from the CHNS Study, 1997–2011. Nutrients 2018, 10, 2014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122014
Gao M, Wang F, Shen Y, Zhu X, Zhang X, Sun X. Trajectories of Mediterranean Diet Adherence and Risk of Hypertension in China: Results from the CHNS Study, 1997–2011. Nutrients. 2018; 10(12):2014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122014
Chicago/Turabian StyleGao, Min, Fengbin Wang, Ying Shen, Xiaorou Zhu, Xing Zhang, and Xinying Sun. 2018. "Trajectories of Mediterranean Diet Adherence and Risk of Hypertension in China: Results from the CHNS Study, 1997–2011" Nutrients 10, no. 12: 2014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10122014