Donor Human Milk Protects against Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
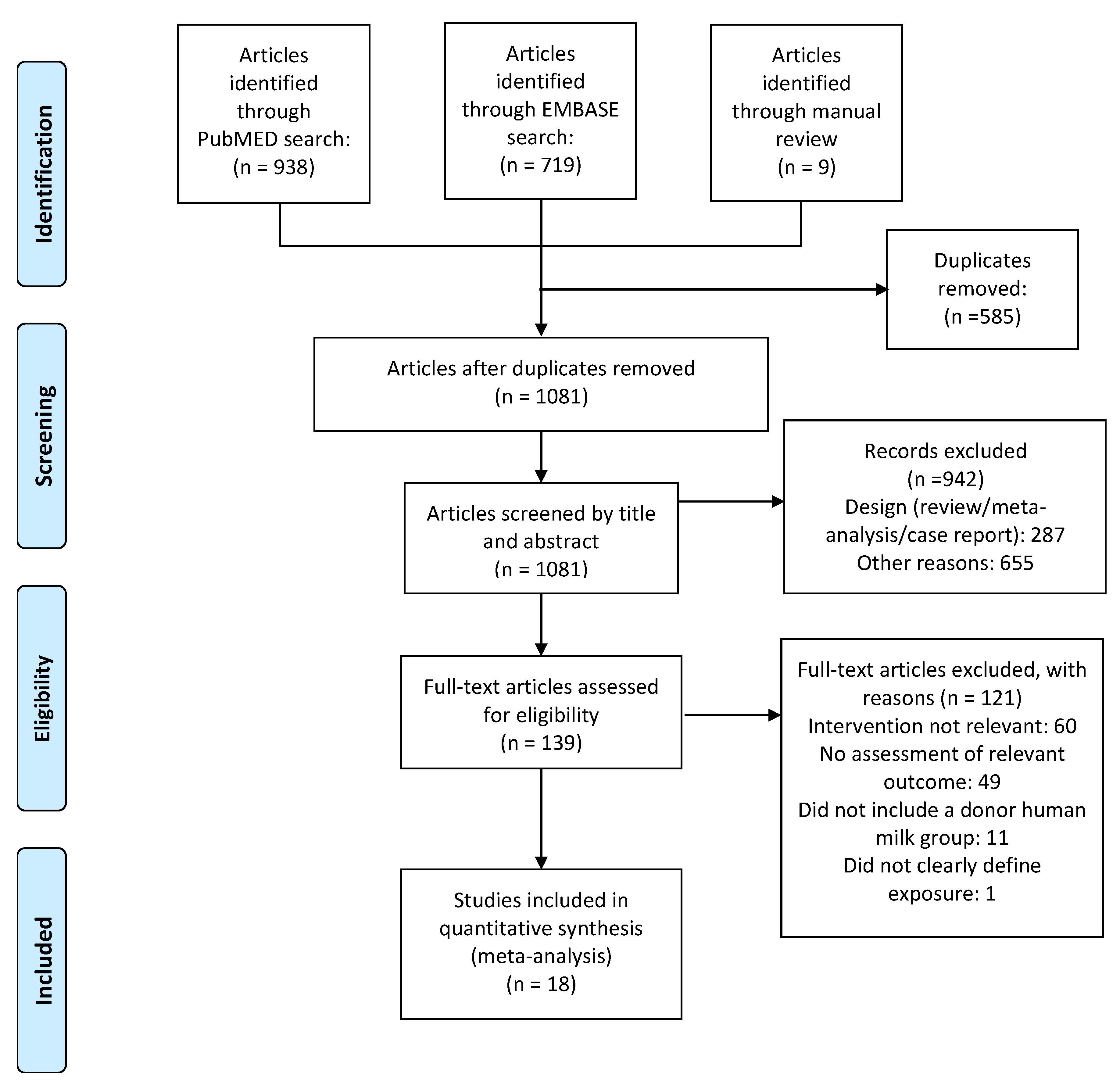
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction and Assessment of Risk of Bias
2.4. Statistical Analysis
3. Results
3.1. Quality Assessment and Publication Bias
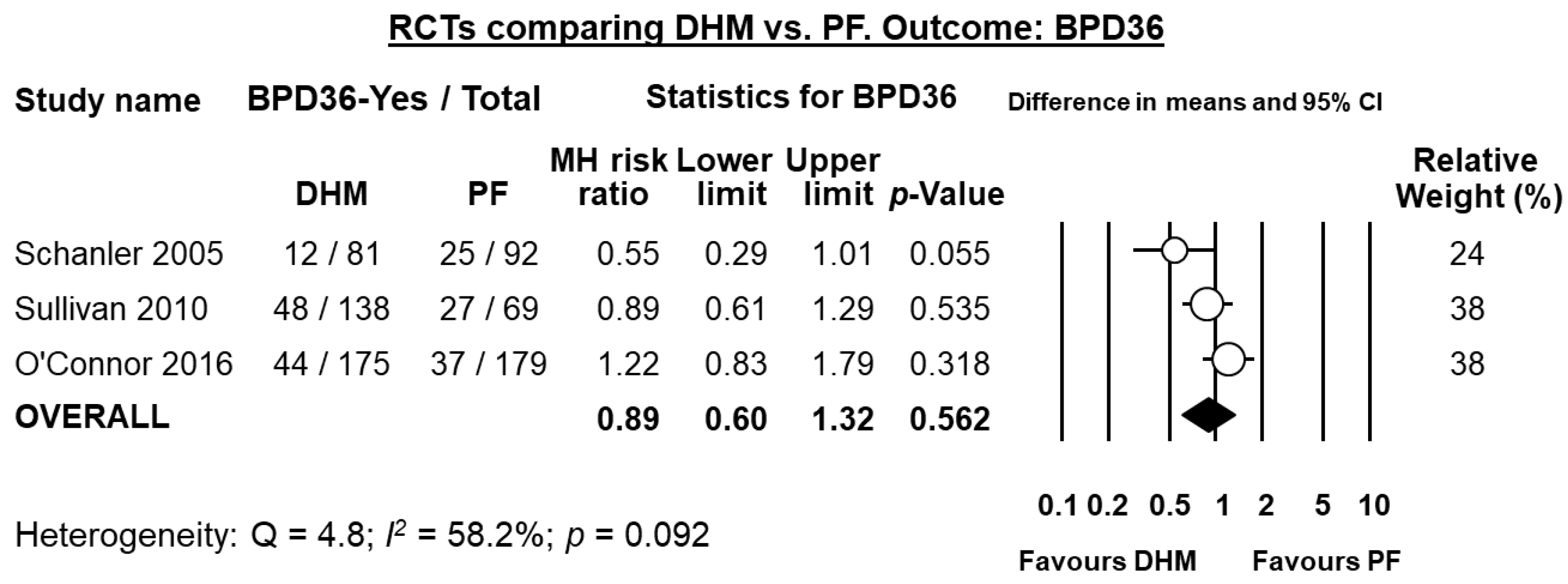
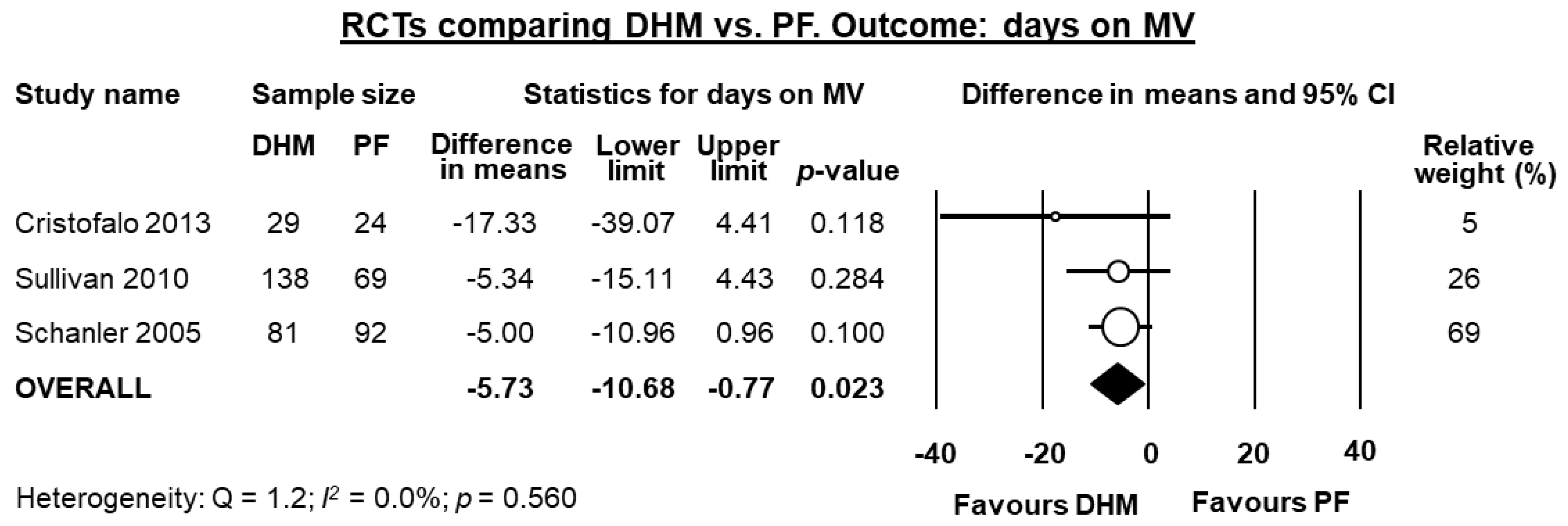
3.2. Randomized Controlled Trials: Donor Human Milk vs. Preterm Formula
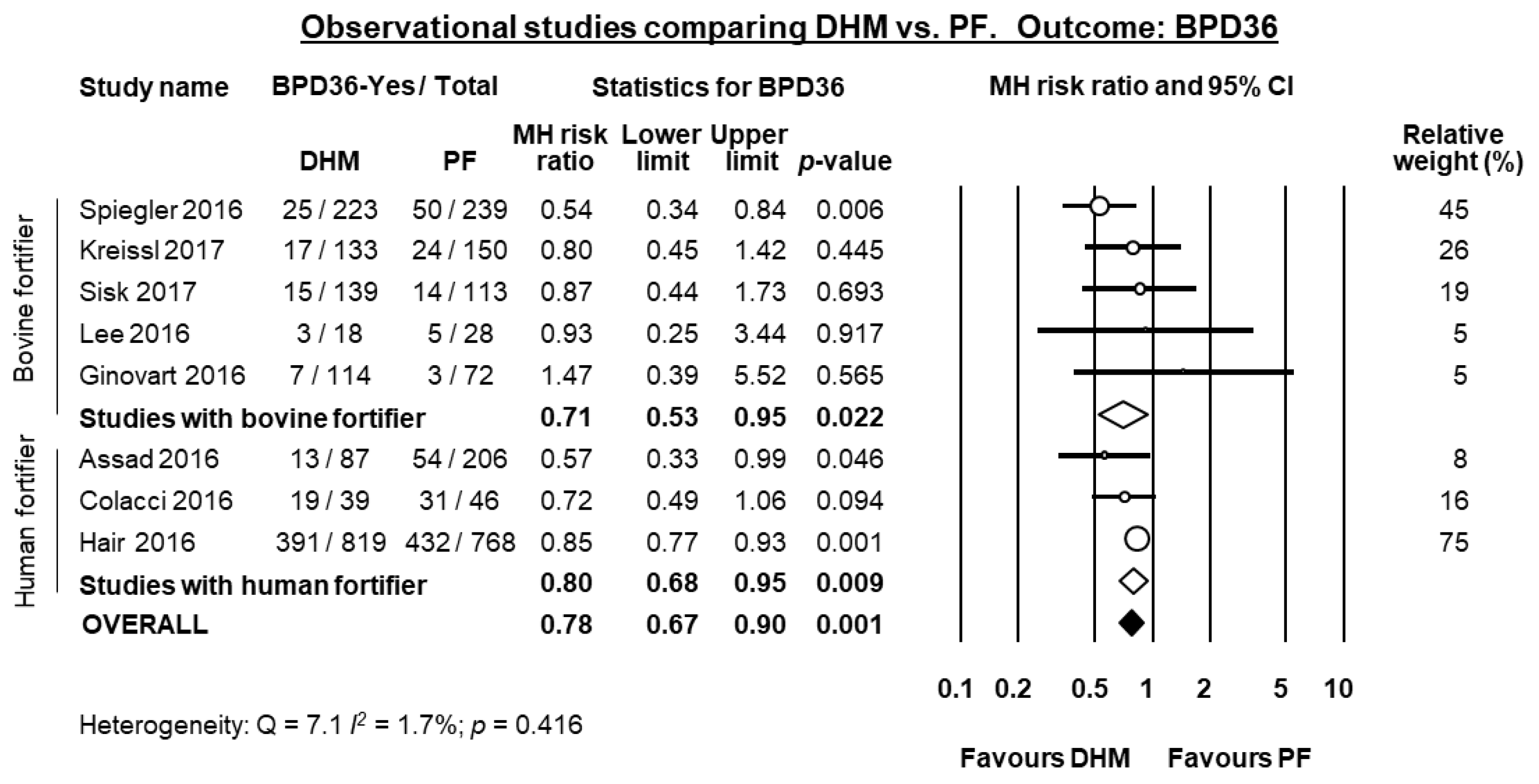
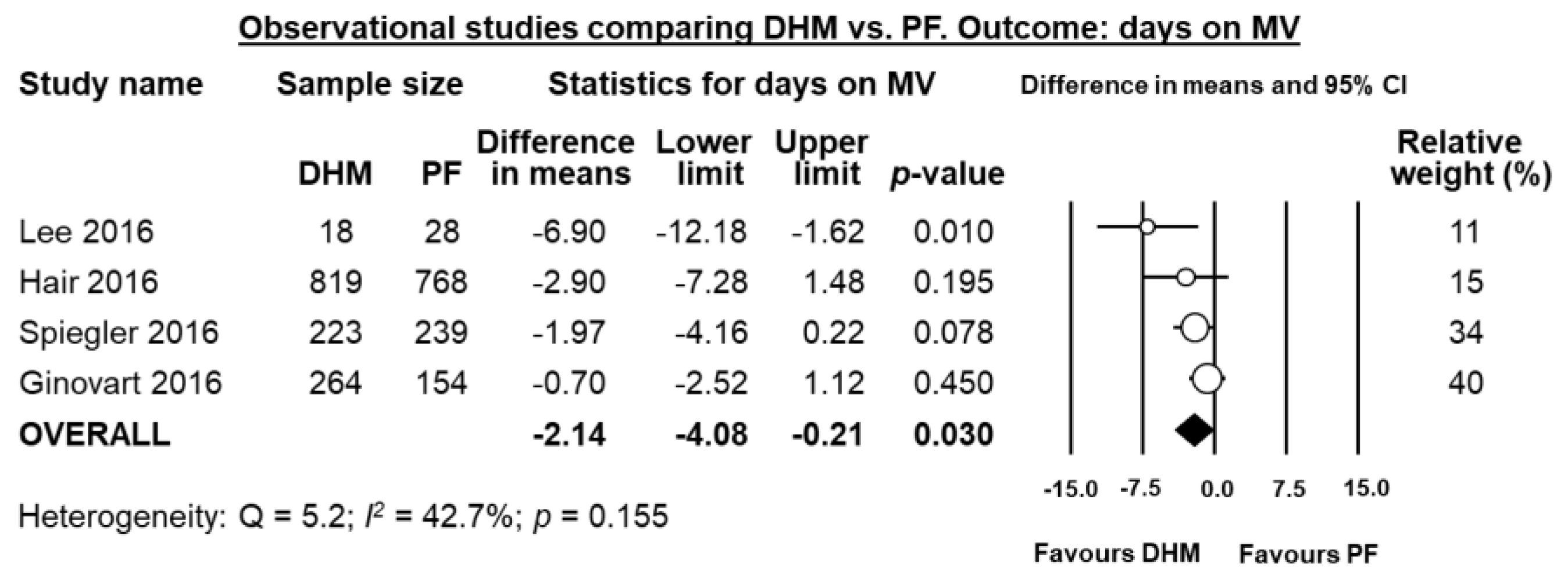
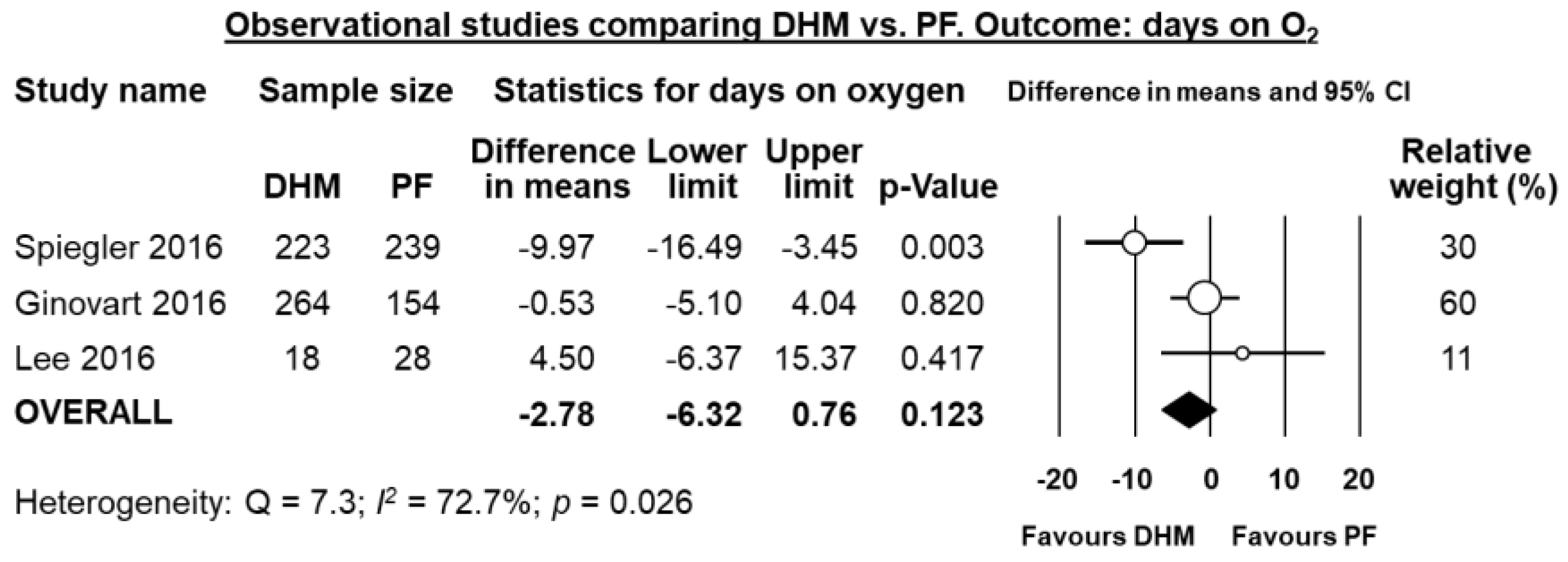
3.3. Observational Studies: Donor Human Milk vs. Preterm Formula
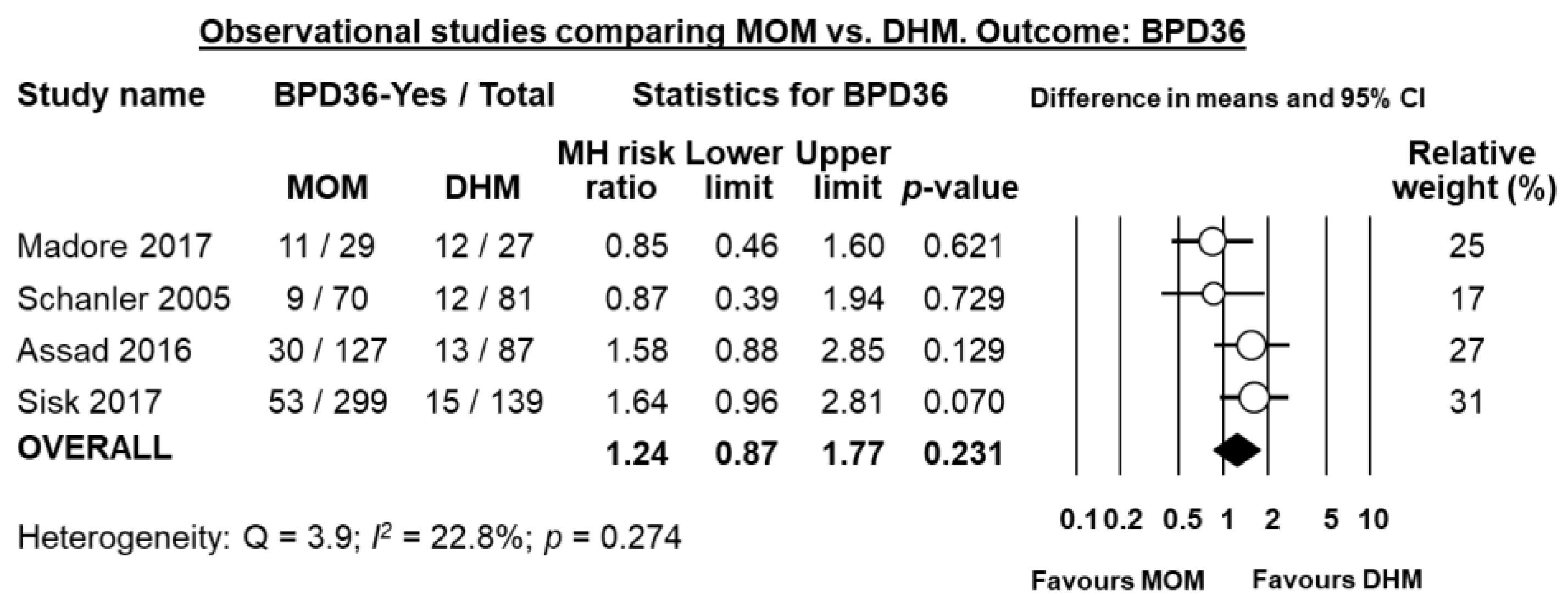
3.4. Mother’s Own Milk vs. Donor Human Milk
3.5. Raw Mother’s Own Milk vs. Pasteurized Mother’s Own Milk
3.6. Raw Mother’s Own Milk vs. Frozen Mother’s Own Milk
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Corpeleijn et al. 2016 [30] | LR | LR | LR | LR | LR | LR | LR |
| Cossey et al. 2013 [31] | LR | LR | HR | UR | LR | LR | LR |
| Cristofalo et al. 2013 [43] | LR | LR | LR | LR | LR | LR | LR |
| O’Connor et al. 2016 [41] | LR | LR | LR | LR | LR | LR | LR |
| Omarsdottir et al. 2015 [38] | UR | UR | HR | UR | LR | LR | LR |
| Schanler et al. 2005 [10] | LR | LR | HR | HR | LR | LR | LR |
| Sullivan et al. 2010 [40] | LR | LR | HR | LR | LR | LR | LR |
| Study Name | Study Design | Selection (0–4 Points) | Comparability (0–2) | Outcome (0–3) | Total (0–9) |
|---|---|---|---|---|---|
| Assad et al. 2015 [28] | Retrospective cohort | 4 | 0 | 3 | 7 |
| Colacci et al. 2017 [29] | Retrospective cohort | 4 | 0 | 3 | 7 |
| Dicky et al. 2017 [32] | Retrospective cohort | 4 | 2 | 3 | 9 |
| Ginovart et al. 2016 [33] | Retrospective cohort | 4 | 0 | 3 | 7 |
| Giuliani et al. 2012 [34] | Retrospective case-control | 4 | 0 | 3 | 7 |
| Hair et al. 2016 [35] | Retrospective cohort | 4 | 0 | 3 | 7 |
| Kreissl et al. 2017 [36] | Prospective cohort | 4 | 0 | 3 | 7 |
| Lee et al. 2016 [37] | Retrospective cohort | 4 | 0 | 2 | 6 |
| Madore et al. 2017 [42] | Retrospective case-control | 4 | 2 | 3 | 9 |
| Sisk et al. 2017 [39] | Retrospective cohort | 4 | 0 | 3 | 7 |
| Spiegler et al. 2016 [21] | Prospective cohort | 4 | 2 | 3 | 9 |
References
- Hylander, M.A.; Strobino, D.M.; Dhanireddy, R. Human milk feedings and infection among very low birth weight infants. Pediatrics 1998, 102, e38. [Google Scholar] [CrossRef] [PubMed]
- Morales, Y.; Schanler, R.J. Human milk and clinical outcomes in vlbw infants: How compelling is the evidence of benefit? Semin. Perinatol. 2007, 31, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Bertino, E.; Giuliani, F.; Occhi, L.; Coscia, A.; Tonetto, P.; Marchino, F.; Fabris, C. Benefits of donor human milk for preterm infants: Current evidence. Early Hum. Dev. 2009, 85, S9–S10. [Google Scholar] [CrossRef] [PubMed]
- Underwood, M.A. Human milk for the premature infant. Pediatr. Clin. N. Am. 2013, 60, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2014, CD002971. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Optimal Feeding of Low Birth-Weight Infants in Low-and Middle-Income Countries; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar]
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I. Donor human milk for preterm infants: Current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Johnson, T.J.; Engstrom, J.L.; Fogg, L.F.; Jegier, B.J.; Bigger, H.R.; Meier, P.P. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J. Perinatol. 2013, 33, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J.; Lau, C.; Hurst, N.M.; Smith, E.O.B. Randomized trial of donor human milk versus preterm formula as substitutes for mothers’ own milk in the feeding of extremely premature infants. Pediatrics 2005, 116, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Hylander, M.A.; Strobino, D.M.; Pezzullo, J.C.; Dhanireddy, R. Association of human milk feedings with a reduction in retinopathy of prematurity among very low birthweight infants. J. Perinatol. 2001, 21, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.L.; Sorita, A.; Carey, W.A.; Colby, C.E.; Murad, M.H.; Alahdab, F. Interventions to prevent retinopathy of prematurity: A meta-analysis. Pediatrics 2016, 137. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Shukla, V.V.; John, D.; Chen, C. Human milk feeding as a protective factor for retinopathy of prematurity: A meta-analysis. Pediatrics 2015, 136, e1576–e1586. [Google Scholar] [CrossRef] [PubMed]
- Cacho, N.T.; Parker, L.A.; Neu, J. Necrotizing enterocolitis and human milk feeding: A systematic review. Clin. Perinatol. 2017, 44, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.; Patel, A.; Esquerra-Zwiers, A. Donor human milk update: Evidence, mechanisms, and priorities for research and practice. J. Pediatr. 2017, 180, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Moukarzel, S.; Soberanes, L.; Dyer, R.A.; Albersheim, S.; Elango, R.; Innis, S.M. Relationships among different water-soluble choline compounds differ between human preterm and donor milk. Nutrients 2017, 9, 369. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Lyden, E.; Furtado, J.; Van Ormer, M.; Anderson-Berry, A. A comparison of nutritional antioxidant content in breast milk, donor milk, and infant formulas. Nutrients 2016, 8, 681. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Jain, L.; Schmidt, B.; Abman, S.; Bancalari, E.; Aschner, J.L. Bronchopulmonary dysplasia: NHLBI workshop on the primary prevention of chronic lung diseases. Ann. Am. Thorac. Soc. 2014, 11, S146–S153. [Google Scholar] [CrossRef] [PubMed]
- Kramer, B.W.; Kallapur, S.; Newnham, J.; Jobe, A.H. Prenatal inflammation and lung development. Semin. Fetal Neonatal Med. 2009, 14, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Wemhöner, A.; Ortner, D.; Tschirch, E.; Strasak, A.; Rüdiger, M. Nutrition of preterm infants in relation to bronchopulmonary dysplasia. BMC Pulm. Med. 2011, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Spiegler, J.; Preuß, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Göpel, W.; Network, G.N. Does breastmilk influence the development of bronchopulmonary dysplasia? J. Pediatr. 2016, 169, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://s3.amazonaws.com/academia.edu.documents/37210401/0470699515.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1518487789&Signature=K9uRr67lWsWC8w5ktrWqgY652HU%3D&response-content-disposition=inline%3B%20filename%3D20_Qualitative_research_and_Cochrane_rev.pdf (accessed on 10 December 2017).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies. Available online: https://scholar.google.com.hk/scholar?hl=zh-CN&as_sdt=0%2C5&as_vis=1&q=Newcastle-ottawa+quality+assessment+scale+cohort+studies&btnG= (accessed on 10 December 2017).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Subgroup analyses. In Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 149–186. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Chapter 16: Identifying and quantifying heterogeneity. In Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2009; Volume 123, pp. 2009–2124. [Google Scholar]
- Assad, M.; Elliott, M.; Abraham, J. Decreased cost and improved feeding tolerance in vlbw infants fed an exclusive human milk diet. J. Perinatol. 2016, 36, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Colacci, M.; Murthy, K.; DeRegnier, R.-A.O.; Khan, J.Y.; Robinson, D.T. Growth and development in extremely low birth weight infants after the introduction of exclusive human milk feedings. Am. J. Perinatol. 2017, 34, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, W.E.; de Waard, M.; Christmann, V.; van Goudoever, J.B.; Jansen-van der Weide, M.C.; Kooi, E.M.; Koper, J.F.; Kouwenhoven, S.M.; Lafeber, H.N.; Mank, E. Effect of donor milk on severe infections and mortality in very low-birth-weight infants: The early nutrition study randomized clinical trial. JAMA Pediatr. 2016, 170, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Cossey, V.; Vanhole, C.; Eerdekens, A.; Rayyan, M.; Fieuws, S.; Schuermans, A. Pasteurization of mother’s own milk for preterm infants does not reduce the incidence of late-onset sepsis. Neonatology 2013, 103, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Dicky, O.; Ehlinger, V.; Montjaux, N.; Gremmo-Féger, G.; Sizun, J.; Rozé, J.C.; Arnaud, C.; Casper, C. Policy of feeding very preterm infants with their mother’s own fresh expressed milk was associated with a reduced risk of bronchopulmonary dysplasia. Acta Paediatr. 2017, 106, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Ginovart, G.; Gich, I.; Verd, S. Human milk feeding protects very low-birth-weight infants from retinopathy of prematurity: A pre–post cohort analysis. J. Matern. Fetal Neonatal Med. 2016, 29, 3790–3795. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, F.; Prandi, G.; Coscia, A.; Cresi, F.; Di Nicola, P.; Raia, M.; Sabatino, G.; Occhi, L.; Bertino, E. Donor human milk versus mother’s own milk in preterm vlbwis: A case control study. J. Biol. Regul. Homeost. Agents 2012, 26, 19–24. [Google Scholar] [PubMed]
- Hair, A.B.; Peluso, A.M.; Hawthorne, K.M.; Perez, J.; Smith, D.P.; Khan, J.Y.; O’Donnell, A.; Powers, R.J.; Lee, M.L.; Abrams, S.A. Beyond necrotizing enterocolitis prevention: Improving outcomes with an exclusive human milk–based diet. Breastfeed. Med. 2016, 11, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Kreissl, A.; Sauerzapf, E.; Repa, A.; Binder, C.; Thanhaeuser, M.; Jilma, B.; Ristl, R.; Berger, A.; Haiden, N. Starting enteral nutrition with preterm single donor milk instead of formula affects time to full enteral feeding in very low birth weight infants. Acta Paediatr. 2017, 106, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, J.H.; Kim, C.S.; Lee, S.L. Clinical findings according to feeding diets in very low birth weight infants: Human breast milk versus bovine milk-based formula. Neonat. Med. 2016, 23, 23–28. [Google Scholar] [CrossRef]
- Omarsdottir, S.; Casper, C.; Naver, L.; Legnevall, L.; Gustafsson, F.; Grillner, L.; Zweygberg-Wirgart, B.; Soderberg-Naucler, C.; Vanpee, M. Cytomegalovirus infection and neonatal outcome in extremely preterm infants after freezing of maternal milk. Pediatr. Infect. Dis. J. 2015, 34, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Sisk, P.M.; Lambeth, T.M.; Rojas, M.A.; Lightbourne, T.; Barahona, M.; Anthony, E.; Auringer, S.T. Necrotizing enterocolitis and growth in preterm infants fed predominantly maternal milk, pasteurized donor milk, or preterm formula: A retrospective study. Am. J. Perinatol. 2017, 34, 676–683. [Google Scholar] [PubMed]
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotten, C.M.; et al. An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products. J. Pediatr. 2010, 156, 562–567.e561. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.L.; Gibbins, S.; Kiss, A.; Bando, N.; Brennan-Donnan, J.; Ng, E.; Campbell, D.M.; Vaz, S.; Fusch, C.; Asztalos, E. Effect of supplemental donor human milk compared with preterm formula on neurodevelopment of very low-birth-weight infants at 18 months: A randomized clinical trial. JAMA 2016, 316, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Madore, L.S.; Bora, S.; Erdei, C.; Jumani, T.; Dengos, A.R.; Sen, S. Effects of donor breastmilk feeding on growth and early neurodevelopmental outcomes in preterm infants: An observational study. Clin. Ther. 2017, 39, 1210–1220. [Google Scholar] [CrossRef] [PubMed]
- Cristofalo, E.A.; Schanler, R.J.; Blanco, C.L.; Sullivan, S.; Trawoeger, R.; Kiechl-Kohlendorfer, U.; Dudell, G.; Rechtman, D.J.; Lee, M.L.; Lucas, A. Randomized trial of exclusive human milk versus preterm formula diets in extremely premature infants. J. Pediatr. 2013, 163, 1592–1595.e1591. [Google Scholar] [CrossRef] [PubMed]
- Ginovart, G.; Gich, I.; Gutiérrez, A.; Verd, S. A fortified donor milk policy is associated with improved in-hospital head growth and weight gain in very low-birth-weight infants. Adv. Neonatal Care 2017, 17, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Binns, C.; Lee, M.K.; Kagawa, M. Ethical challenges in infant feeding research. Nutrients 2017, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Bancalari, E.H. Controversies about the definition of bronchopulmonary dysplasia at 50 years. Acta Paediatr. 2017, 106, 692–693. [Google Scholar] [CrossRef] [PubMed]
- Poindexter, B.B.; Feng, R.; Schmidt, B.; Aschner, J.L.; Ballard, R.A.; Hamvas, A.; Reynolds, A.M.; Shaw, P.A.; Jobe, A.H. Comparisons and limitations of current definitions of bronchopulmonary dysplasia for the prematurity and respiratory outcomes program. Ann. Am. Thorac. Soc. 2015, 12, 1822–1830. [Google Scholar] [CrossRef] [PubMed]
- Beam, K.S.; Aliaga, S.; Ahlfeld, S.K.; Cohen-Wolkowiez, M.; Smith, P.B.; Laughon, M.M. A systematic review of randomized controlled trials for the prevention of bronchopulmonary dysplasia in infants. J. Perinatol. 2014, 34, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Villamor-Martínez, E.; Pierro, M.; Cavallaro, G.; Mosca, F.; Kramer, B.; Villamor, E. Probiotic supplementation in preterm infants does not affect the risk of bronchopulmonary dysplasia: A meta-analysis of randomized controlled trials. Nutrients 2017, 9, 1197. [Google Scholar] [CrossRef] [PubMed]
- Peila, C.; Moro, G.E.; Bertino, E.; Cavallarin, L.; Giribaldi, M.; Giuliani, F.; Cresi, F.; Coscia, A. The effect of holder pasteurization on nutrients and biologically-active components in donor human milk: A review. Nutrients 2016, 8, 477. [Google Scholar] [CrossRef] [PubMed]
- Daniels, B.; Schmidt, S.; King, T.; Israel-Ballard, K.; Amundson Mansen, K.; Coutsoudis, A. The effect of simulated flash-heat pasteurization on immune components of human milk. Nutrients 2017, 9, 178. [Google Scholar] [CrossRef] [PubMed]
- Gormaz, M.; Torres-Cuevas, I.; Cernada, M.; Kuligowski, J.; Cubells, E.; Escobar, J.; Vento, M. Role of human milk in oxidative stress associated with prematurity. J. Pediatr. Biochem. 2013, 3, 169–177. [Google Scholar] [CrossRef]
- Hamprecht, K.; Goelz, R. Postnatal cytomegalovirus infection through human milk in preterm infants: Transmission, clinical presentation, and prevention. Clin. Perinatol. 2017, 44, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, W.E.; Kouwenhoven, S.M.P.; Paap, M.C.; van Vliet, I.; Scheerder, I.; Muizer, Y.; Helder, O.K.; van Goudoever, J.B.; Vermeulen, M.J. Intake of own mother’s milk during the first days of life is associated with decreased morbidity and mortality in very low birth weight infants during the first 60 days of life. Neonatology 2012, 102, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Niño, D.F.; Sodhi, C.P.; Hackam, D.J. Necrotizing enterocolitis: New insights into pathogenesis and mechanisms. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Vongbhavit, K.; Underwood, M.A. Prevention of necrotizing enterocolitis through manipulation of the intestinal microbiota of the premature infant. Clin. Ther. 2016, 38, 716–732. [Google Scholar] [CrossRef] [PubMed]
- Neu, J. Preterm infant nutrition, gut bacteria, and necrotizing enterocolitis. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Cacho, N.T.; Harrison, N.A.; Parker, L.A.; Padgett, K.A.; Lemas, D.J.; Marcial, G.E.; Li, N.; Carr, L.E.; Neu, J.; Lorca, G.L. Personalization of the microbiota of donor human milk with mother’s own milk. Front. Microbiol. 2017, 8, 1470. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Sato, M.; Go, H.; Ogasawara, K.; Kanai, Y.; Maeda, H.; Chishiki, M.; Shimizu, H.; Mashiyama, F.; Goto, A.; et al. The microbiome of the lower respiratory tract in premature infants with and without severe bronchopulmonary dysplasia. Am. J. Perinatol. 2017, 34, 80–87. [Google Scholar] [PubMed]
- Lohmann, P.; Luna, R.A.; Hollister, E.B.; Devaraj, S.; Mistretta, T.-A.; Welty, S.E.; Versalovic, J. The airway microbiome of intubated premature infants: Characteristics and changes that predict the development of bronchopulmonary dysplasia. Pediatr. Res. 2014, 76, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Berkhout, D.J.; Niemarkt, H.J.; Benninga, M.A.; Budding, A.E.; van Kaam, A.H.; Kramer, B.W.; Pantophlet, C.M.; van Weissenbruch, M.M.; de Boer, N.K.; de Meij, T.G. Development of severe bronchopulmonary dysplasia is associated with alterations in fecal volatile organic compounds. Pediatr. Res. 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Wagner, B.D.; Sontag, M.K.; Harris, J.K.; Miller, J.I.; Morrow, L.; Robertson, C.E.; Stephens, M.; Poindexter, B.B.; Abman, S.H.; Mourani, P.M. Airway microbial community turnover differs by bpd severity in ventilated preterm infants. PLoS ONE 2017, 12, e0170120. [Google Scholar] [CrossRef] [PubMed]
- Thoene, M.; Hanson, C.; Lyden, E.; Dugick, L.; Ruybal, L.; Anderson-Berry, A. Comparison of the effect of two human milk fortifiers on clinical outcomes in premature infants. Nutrients 2014, 6, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Thoene, M.; Lyden, E.; Weishaar, K.; Elliott, E.; Wu, R.; White, K.; Timm, H.; Anderson-Berry, A. Comparison of a powdered, acidified liquid, and non-acidified liquid human milk fortifier on clinical outcomes in premature infants. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Adamkin, D.H.; Radmacher, P.G. Fortification of human milk in very low birth weight infants (VLBW <1500 g birth weight). Clin. Perinatol. 2014, 41, 405–421. [Google Scholar] [PubMed]
- Radmacher, P.G.; Adamkin, D.H. Fortification of human milk for preterm infants. Semin. Fetal Neonatal Med. 2017, 22, 30–35. [Google Scholar] [CrossRef] [PubMed]








| Authors | n of Infants (Centers) | Inclusion Criteria | Primary Outcome(s) | Respiratory Outcome(s) | Studied Intervention | Duration of Intervention | Fortification | Comments |
|---|---|---|---|---|---|---|---|---|
| Corpeleijn et al. 2016 [30] | 373 (6) | BW <1500 g, MOM insufficiently available. | Composite incidence of NEC, serious infection (sepsis or meningitis), or all-cause mortality between 72 h and 60 days of life. | BPD28 | - MOM + DHM - MOM + PF | 10 days or hospital transfer or death. | Bovine fortifier added to MOM and DHM. | Median MOM intakes were higher in the DHM group, 89.1% in the DHM group vs. 84.5% in the PF group. |
| Cossey et al. 2013 [31] | 303 (1) | GA <32 weeks, BW <1500 g. | Incidence of proven late-onset sepsis. | BPD36, days on MV | - Raw MOM + PF - Pasteurized MOM + PF | Eight weeks or discharge. | Not specified. | MV defined as respiratory support. |
| Cristofalo et al. 2013 [43] | 53 (7) | BW 500–1250 g, no intention to provide MOM, parenteral nutrition within 48 h, enteral feeding within 21 days. | Duration of parenteral nutrition. | Days on MV, days on O2 | - Exclusive DHM - Exclusive PF | 91 days of age or discharge, or attainment of 50% oral feedings. | DHM fortifier added to DHM. | |
| O’Connor et al. 2016 [41] | 363 (4) | BW < 1500 g, enteral feeding within 7 days. | Bayley-III score at 18 months. | BPD36 | - MOM + DHM - MOM + PF | 90 days or discharge. | Bovine fortifier added to MOM and DHM. | MOM + DHM group: MOM = 58% of intake. MOM + PF group: MOM = 63% of intake. |
| Omarsdottir et al. 2015 [38] | 140 (2) | GA < 28 weeks, intention to provide MOM, intention to breastfeed. | CMV transmission to infants from breast milk, rate of symptomatic CMV infection. | BPD36 | - Frozen MOM + DHM - Fresh MOM + frozen MOM + DHM | Until 32 weeks PMA. | Not specified. | Frozen MOM: stored for ≥3 days at −20 °C. Fresh MOM: fed immediately or after refrigeration at +4 °C. |
| Schanler et al. 2005 [10] | 243 (1) | GA ≤ 29 weeks. | Incidence of late-onset sepsis and/or NEC. | BPD36, days on MV | - MOM + DHM - MOM + PF | 90 days or discharge. | Bovine fortifier added to MOM and DHM. | |
| Sullivan et al. 2010 [40] | 207 (12) | BW 500–1250 g, intention to provide MOM. | NEC. | BPD36, days on MV, days on O2 | - MOM + DHM + DHM fortifier - MOM + PF + bovine fortifier | 91 days or ≥50% oral feedings or discharge. | Donor DHM-based fortifier in DHM group, bovine fortifier in PF group. |
| Authors | Study Design | n of Infants (Centers) | Inclusion Criteria | Primary Outcome(s) | Respiratory Outcome(s) | Groups | Duration of Intervention | Fortification | Comments |
|---|---|---|---|---|---|---|---|---|---|
| Assad et al. 2015 [28] | Retrospective cohort | 293 (1) | GA < 29 and/or BW ≤ 1500 g. | Feeding intolerance, time to full feeds, length of stay. | BPD36 | - MOM + DHM + DHM-based fortifier; - MOM + bovine fortifier; - MOM + PF + bovine fortifier; - Exclusive PF | Until discharge. | DHM fortifier in exclusive human diet, bovine fortifier in bovine groups. | |
| Colacci et al. 2017 [29] | Retrospective cohort | 85 (1) | BW < 1000 g, GA < 37 weeks. | Neurodevelopmental impairment (Bayley-III score). | BPD36 | - MOM + DHM + DHM-based fortifier; - MOM + PF + bovine fortifier | At least four weeks, until weight ≥ 1500 g, or 34 weeks PMA. | DHM-based fortifier in exclusive human milk group, bovine fortifier in other group. | |
| Dicky et al. 2017 [32] | Retrospective cohort | 926 (63) | GA < 32 weeks, alive at 7 days of life. | In-hospital mortality, short-term morbidity, weight gain. | BPD36, Days on MV, Days on oxygen | - Raw MOM + PF/DHM; - Pasteurized MOM + PF/DHM | Until 33 weeks corrected age or until discharge. | Bovine fortifier added to both groups. | The supplement (PF, DHM, infant formula) to raw or pasteurized MOM varied per center. |
| Ginovart et al. 2016 [33] | Retrospective cohort | 186 (1) | BW < 1500 g. | Retinopathy of prematurity. | BPD28, BPD36, days on MV, days on O2 | - MOM + DHM; - MOM + PF | Four weeks. | Bovine fortifier added to MOM and to DHM. | Additional data provided by authors, and from later (2017) report of Ginovart et al. [ 44]. |
| Giuliani et al. 2012 [34] | Retrospective cohort | 92 (1) | GA > 23 weeks, BW < 1500 g. | Growth, and short-term clinical outcomes. | BPD28 | - Mainly MOM (>80%); - Mainly DHM (>80%) | 32 weeks corrected GA. | Bovine fortifier added to MOM. | |
| Hair et al. 2016 [35] | Retrospective cohort | 1587 (4) | BW < 1250 g. | NEC, mortality. | BPD36, days on MV | - MOM + DHM + DHM-based fortifier; - MOM + PF + bovine fortifier | 32–34 corrected GA, or 60 days of life. depending on the centre. | DHM-based fortifier in DHM group. Bovine fortifier in bovine group. | |
| Kreissl et al. 2017 [36] | Prospective cohort | 283 (1) | GA < 32 weeks, BW < 1500 g. | Time to full enteral feeding. | BPD36 | - MOM + DHM; - MOM + PF | Until term or discharge. DHM group received DHM until MOM was available or until reaching 140 mL/kg/day, then switched to term formula. | Bovine fortifier added to MOM and DHM when infant reached intake of 100 mL/kg/day. | DHM provided by other preterm mothers. |
| Lee et al. 2016 [37] | Retrospective cohort | 46 (1) | BW < 1500 g. | Morbidity, duration parenteral nutrition, length of hospital stay. | BPD36, days on MV, days on O2 | - MOM + DHM; - MOM + PF | Not specified. | Not specified. | Days on MV: defined as invasive ventilation. Days on O2 defined as non-invasive ventilation. |
| Madore et al. 2017 [42] | Retrospective case-control | 81 (1) | BW < 1000 g. | Growth, neurodevelopment. | BPD36 | - Exclusive MOM; - DHM > 50%; - PF > 50% | First month of life. | Bovine fortifier added to MOM and to DHM. | |
| Sisk et al. 2017 [39] | Retrospective cohort | 563 (1) | GA ≤ 32 weeks and BW ≤ 1500 g. | NEC stage ≥ 2. | BPD36 | - MOM ≥ 50%; - DHM ≥ 50%; - PF ≥ 50% | Within 2 h of birth until 34 weeks PMA. | Bovine fortifier added to MOM and to DHM. | |
| Spiegler et al. 2016 [21] | Prospective cohort | 1433 (48) | GA 22–31 6/7, BW < 1500 g. | BPD. | BPD36, days on MV, days on O2 | - MOM + DHM; - MOM + DHM + PF; - Exclusive PF | Until discharge. | Bovine fortifier added to MOM and to DHM. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villamor-Martínez, E.; Pierro, M.; Cavallaro, G.; Mosca, F.; Kramer, B.W.; Villamor, E. Donor Human Milk Protects against Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 238. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020238
Villamor-Martínez E, Pierro M, Cavallaro G, Mosca F, Kramer BW, Villamor E. Donor Human Milk Protects against Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(2):238. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020238
Chicago/Turabian StyleVillamor-Martínez, Eduardo, Maria Pierro, Giacomo Cavallaro, Fabio Mosca, Boris W. Kramer, and Eduardo Villamor. 2018. "Donor Human Milk Protects against Bronchopulmonary Dysplasia: A Systematic Review and Meta-Analysis" Nutrients 10, no. 2: 238. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10020238