Disparate Habitual Physical Activity and Dietary Intake Profiles of Elderly Men with Low and Elevated Systemic Inflammation

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design and Participants
2.2. Body Composition
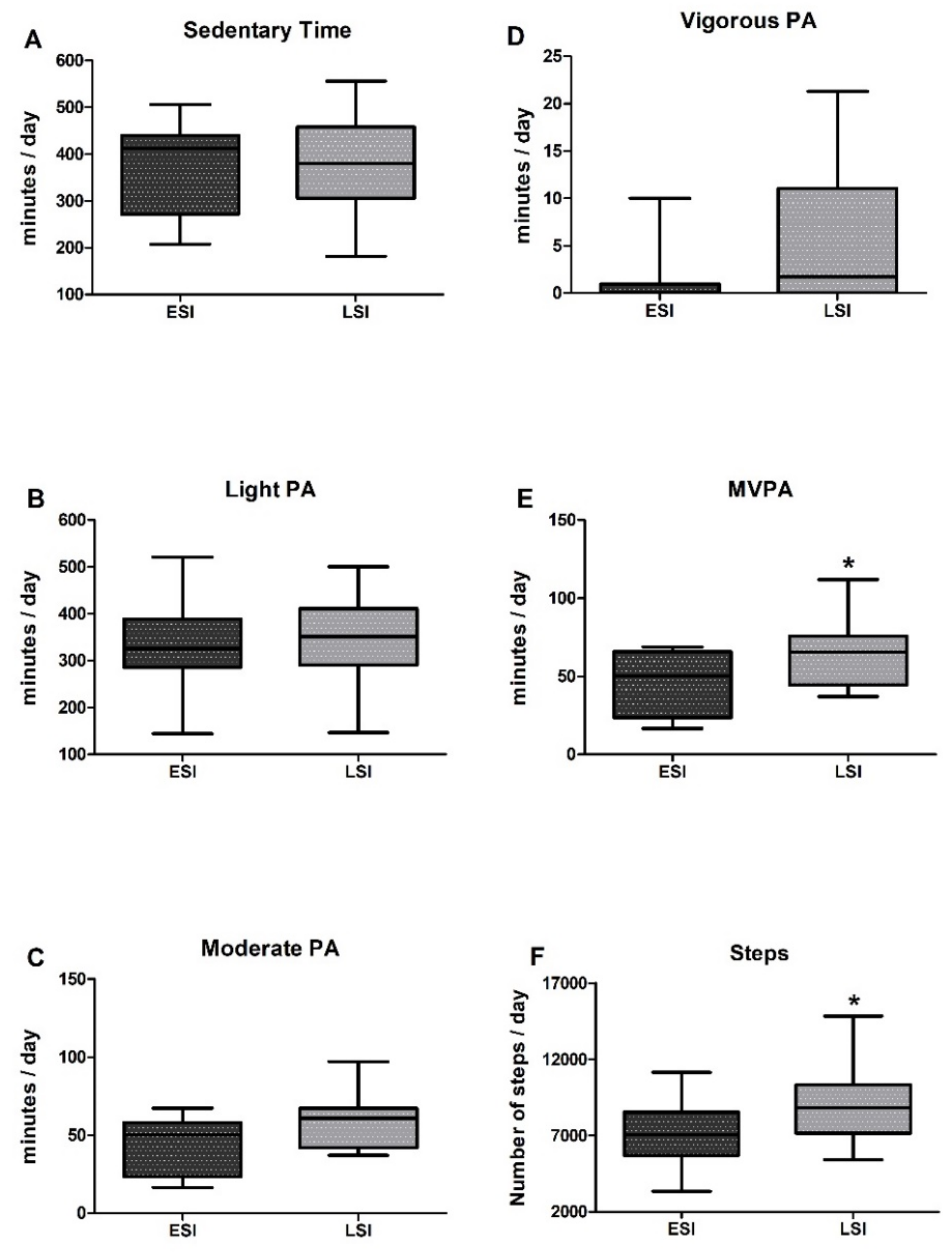
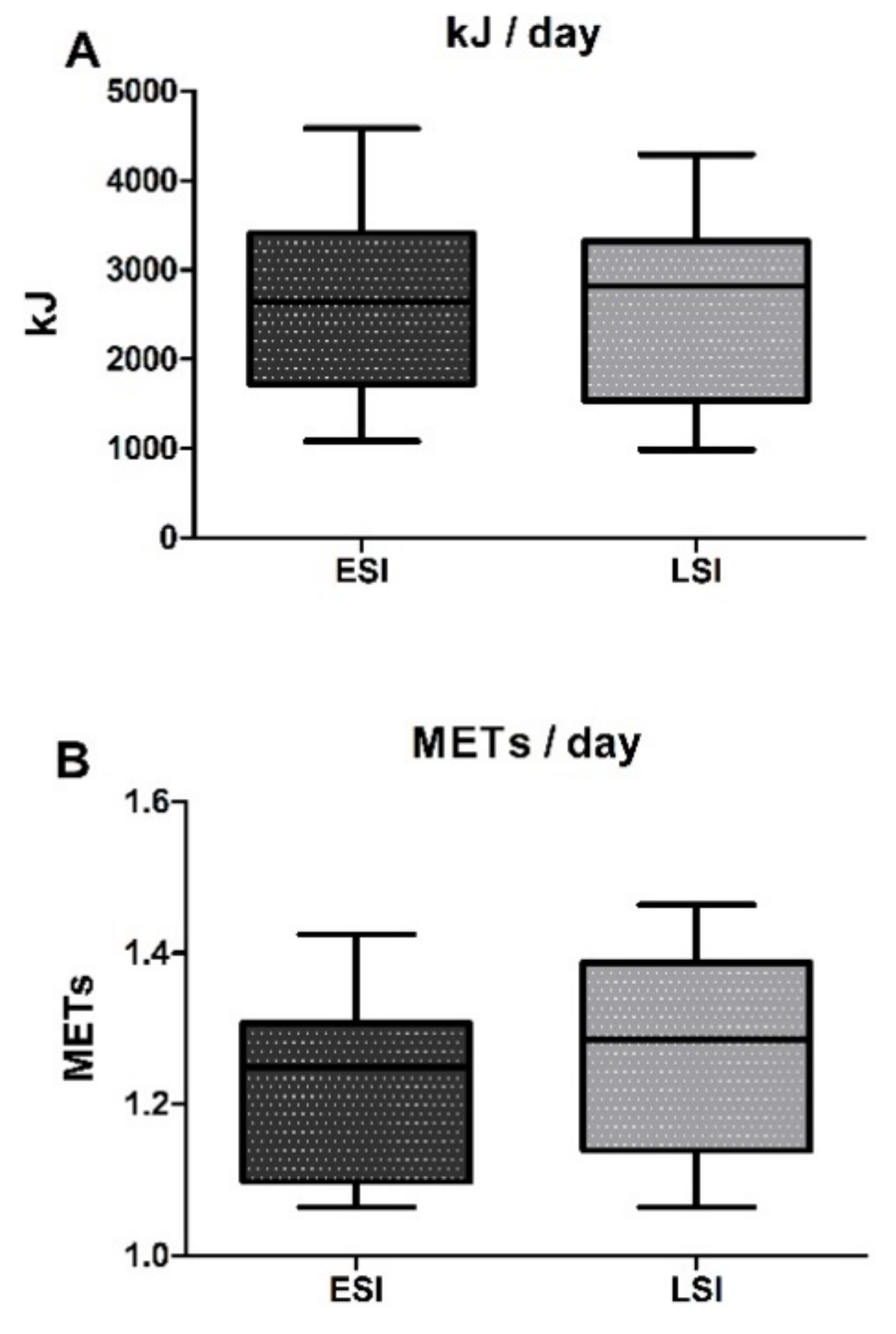
2.3. Physical Activity
2.4. Dietary Assessment
2.5. Systemic Inflammation
2.6. Statistical Analyses
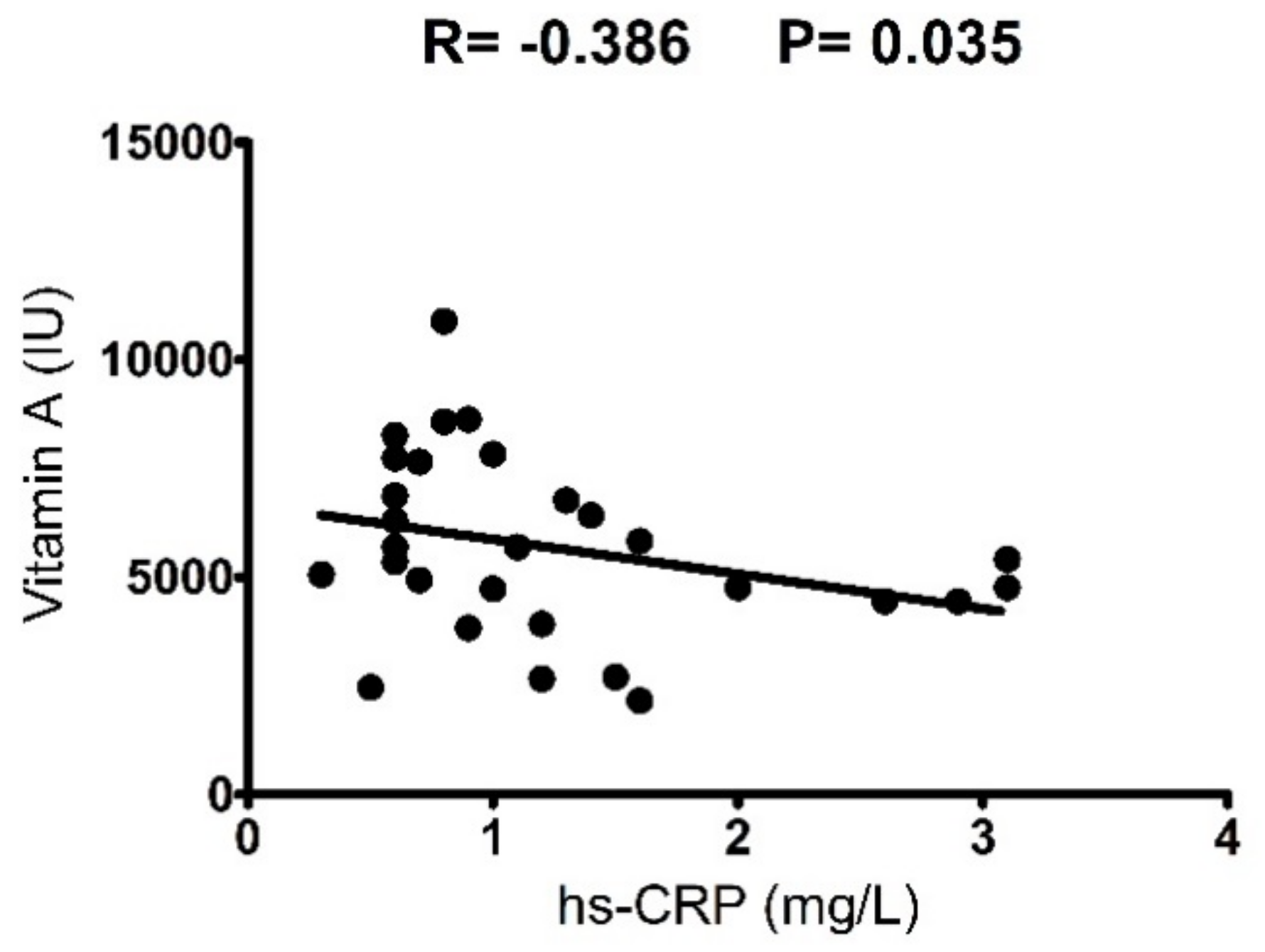
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Franceschi, C.; Bonafe, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C. Inflammaging as a Major Characteristic of Old People: Can It Be Prevented or Cured? Nutr. Rev. 2007, 65, S173–S176. [Google Scholar] [CrossRef] [PubMed]
- Calcada, D.; Vianello, D.; Giampieri, E.; Sala, C.; Castellani, G.; de Graaf, A.; Kremer, B.; van Ommen, B.; Feskens, E.; Santoro, A.; et al. The role of low-grade inflammation and metabolic flexibility in aging and nutritional modulation thereof: A systems biology approach. Mech. Ageing Dev. 2014, 136–137, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, R.E.; O’Mahony, M.S.; Savva, G.M.; Calver, B.L.; Woodhouse, K.W. Inflammation and frailty measures in older people. J. Cell. Mol. Med. 2009, 13, 3103–3109. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Vitale, G.; Capri, M.; Salvioli, S. Inflammaging and ‘Garb-aging’. Trends Endocrinol. Metab. 2016. [Google Scholar] [CrossRef] [PubMed]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Newman, A.B. Inflammatory markers in population studies of aging. Ageing Res. Rev. 2011, 10, 319–329. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Franceschi, C.; Monti, D.; Ginaldi, L. Inflamm-ageing and lifelong antigenic load as major determinants of ageing rate and longevity. FEBS Lett. 2005, 579, 2035–2039. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A.; et al. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef]
- Michaud, M.; Balardy, L.; Moulis, G.; Gaudin, C.; Peyrot, C.; Vellas, B.; Cesari, M.; Nourhashemi, F. Proinflammatory cytokines, aging, and age-related diseases. J. Am. Med. Dir. Assoc. 2013, 14, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Payette, H.; Roubenoff, R.; Jacques, P.F.; Dinarello, C.A.; Wilson, P.W.; Abad, L.W.; Harris, T. Insulin-like growth factor-1 and interleukin 6 predict sarcopenia in very old community-living men and women: The Framingham Heart Study. J. Am. Geriatr. Soc. 2003, 51, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [PubMed]
- Cevenini, E.; Monti, D.; Franceschi, C. Inflamm-ageing. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 14–20. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Hammar, M.; Ostgren, C.J. Healthy aging and age-adjusted nutrition and physical fitness. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Bueno, D.R.; Marucci, M.F.N.; Rosa, C.; Fernandes, R.A.; de Oliveira Duarte, Y.A.; Lebao, M.L. Objectively Measured Physical Activity and Healthcare Expenditures Related to Arterial Hypertension and Diabetes Mellitus in Older Adults: SABE Study. J. Aging Phys. Act. 2017, 25, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Huang, L.; Hardy, R.; Crainiceanu, A.; Harris, T.; Schrack, J.A.; Crainiceanu, C.; Kuh, D. Obesity History and Daily Patterns of Physical Activity at Age 60–64 Years: Findings from the MRC National Survey of Health and Development. J. Gerontol. Ser A Biol. Sci. Med. Sci. 2017, 72, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Huisingh-Scheetz, M.; Wroblewski, K.; Kocherginsky, M.; Huang, E.; William, D.; Waite, L.; Schumm, L.P. Physical Activity and Frailty among Older Adults in the U.S. Based on Hourly Accelerometry Data. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Buchner, D.M.; Rillamas-Sun, E.; Di, C.; LaMonte, M.J.; Marshall, S.W.; Hunt, J.; Zhang, Y.; Rosenberg, D.E.; Lee, I.M.; Evenson, K.R.; et al. Accelerometer-Measured Moderate to Vigorous Physical Activity and Incidence Rates of Falls in Older Women. J. Am. Geriatr. Soc. 2017, 65, 2480–2487. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R. Keeping older muscle “young” through dietary protein and physical activity. Adv. Nutr. 2014, 5, 599S–607S. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Mandrichenko, O.; Helbostadt, J.L.; Skelton, D.A. Associations between objectively-measured sedentary behaviour and physical activity with bone mineral density in adults and older adults, the NHANES study. Bone 2014, 64, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Abellan van Kan, G.; Vellas, B. Healthy brain aging: Role of exercise and physical activity. Clin. Geriatr. Med. 2010, 26, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Iwasa, H.; Kumagai, S.; Suzuki, T.; Awata, S.; Yoshida, H. Longitudinal association between habitual physical activity and depressive symptoms in older people. Psychiatry Clin. Neurosci. 2015, 69, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Lavoie, K.L.; Bacon, S.L. Taking up physical activity in later life and healthy ageing: The English longitudinal study of ageing. Br. J. Sports Med. 2014, 48, 239–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, R.A.; Guralnik, J.M.; King, A.C.; Pahor, M.; McDermott, M.M.; Tudor-Locke, C.; Manini, T.M.; Glynn, N.W.; Marsh, A.P.; Axtell, R.S.; et al. Dose of physical activity, physical functioning and disability risk in mobility-limited older adults: Results from the LIFE study randomized trial. PLoS ONE 2017, 12, e0182155. [Google Scholar] [CrossRef] [PubMed]
- Abramson, J.L.; Vaccarino, V. Relationship between physical activity and inflammation among apparently healthy middle-aged and older US adults. Arch. Intern. Med. 2002, 162, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Colbert, L.H.; Visser, M.; Simonsick, E.M.; Tracy, R.P.; Newman, A.B.; Kritchevsky, S.B.; Pahor, M.; Taaffe, D.R.; Brach, J.; Rubin, S.; et al. Physical activity, exercise, and inflammatory markers in older adults: Findings from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2004, 52, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Bartali, B.; Ordovas, J.M.; Corsi, A.M.; Lauretani, F.; Ferrucci, L. Association between physical activity, physical performance, and inflammatory biomarkers in an elderly population: The InCHIANTI study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 760–767. [Google Scholar] [CrossRef]
- Fischer, C.P.; Berntsen, A.; Perstrup, L.B.; Eskildsen, P.; Pedersen, B.K. Plasma levels of interleukin-6 and C-reactive protein are associated with physical inactivity independent of obesity. Scand. J. Med. Sci. Sports 2007, 17, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Molloy, G.J.; de Oliveira, C.; Demakakos, P. Leisure time physical activity, risk of depressive symptoms, and inflammatory mediators: The English Longitudinal Study of Ageing. Psychoneuroendocrinology 2009, 34, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Jankord, R.; Jemiolo, B. Influence of physical activity on serum IL-6 and IL-10 levels in healthy older men. Med. Sci. Sports Exerc. 2004, 36, 960–964. [Google Scholar] [CrossRef] [PubMed]
- Moy, M.L.; Teylan, M.; Weston, N.A.; Gagnon, D.R.; Danilack, V.A.; Garshick, E. Daily step count is associated with plasma C-reactive protein and IL-6 in a US cohort with COPD. Chest 2014, 145, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, B.J.; Beavers, D.P.; Mihalko, S.L.; Miller, G.D.; Loeser, R.F.; Messier, S.P. Relationship of Objectively-Measured Habitual Physical Activity to Chronic Inflammation and Fatigue in Middle-Aged and Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Reuben, D.B.; Judd-Hamilton, L.; Harris, T.B.; Seeman, T.E. The associations between physical activity and inflammatory markers in high-functioning older persons: MacArthur Studies of Successful Aging. J. Am. Geriatr. Soc. 2003, 51, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Taaffe, D.R.; Harris, T.B.; Ferrucci, L.; Rowe, J.; Seeman, T.E. Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur studies of successful aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M709–M715. [Google Scholar] [CrossRef]
- Valentine, R.J.; Woods, J.A.; McAuley, E.; Dantzer, R.; Evans, E.M. The associations of adiposity, physical activity and inflammation with fatigue in older adults. Brain Behav. Immun. 2011, 25, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Wahlin-Larsson, B.; Carnac, G.; Kadi, F. The influence of systemic inflammation on skeletal muscle in physically active elderly women. Age 2014, 36, 9718. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Lowe, G.D.; Whincup, P.H.; Rumley, A.; Walker, M.; Lennon, L. Physical activity and hemostatic and inflammatory variables in elderly men. Circulation 2002, 105, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Tir, A.M.D.; Labor, M.; Plavec, D. The effects of physical activity on chronic subclinical systemic inflammation. Arch. Ind. Hyg. Toxicol. 2017, 68, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.J.; Zourdos, M.C.; Jo, E.; Ormsbee, M.J. Influence of physical activity and nutrition on obesity-related immune function. Sci. World J. 2013, 2013, 752071. [Google Scholar] [CrossRef] [PubMed]
- Panickar, K.S.; Jewell, D.E. The beneficial role of anti-inflammatory dietary ingredients in attenuating markers of chronic low-grade inflammation in aging. Horm. Mol. Biol. Clin. Investig. 2015, 23, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Wintergerst, E.S.; Maggini, S.; Hornig, D.H. Contribution of selected vitamins and trace elements to immune function. Ann. Nutr. Metab. 2007, 51, 301–323. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.S.; Rudkowska, I. Dairy nutrients and their effect on inflammatory profile in molecular studies. Mol. Nutr. Food Res. 2015, 59, 1249–1263. [Google Scholar] [CrossRef] [PubMed]
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nat. Rev. Immunol. 2011, 11, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Lordan, R.; Tsoupras, A.; Zabetakis, I. Phospholipids of Animal and Marine Origin: Structure, Function, and Anti-Inflammatory Properties. Molecules 2017, 22. [Google Scholar] [CrossRef]
- Draganidis, D.; Karagounis, L.G.; Athanailidis, I.; Chatzinikolaou, A.; Jamurtas, A.Z.; Fatouros, I.G. Inflammaging and Skeletal Muscle: Can Protein Intake Make a Difference? J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M.; Koster, A.; Schols, J.M.; Meijers, J.M.; Halfens, R.J.; Gudnason, V.; Eiriksdottir, G.; Siggeirsdottir, K.; Sigurdsson, S.; Jonsson, P.V.; et al. Physical activity and incidence of sarcopenia: The population-based AGES-Reykjavik Study. Age Ageing 2016, 45, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Labonte, M.E.; Cyr, A.; Abdullah, M.M.; Lepine, M.C.; Vohl, M.C.; Jones, P.; Couture, P.; Lamarche, B. Dairy product consumption has no impact on biomarkers of inflammation among men and women with low-grade systemic inflammation. J. Nutr. 2014, 144, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Douroudos, I.; Panagoutsos, S.; Pasadakis, P.; Nikolaidis, M.G.; Chatzinikolaou, A.; Sovatzidis, A.; Michailidis, Y.; Jamurtas, A.Z.; Mandalidis, D.; et al. Effects of L-carnitine on oxidative stress responses in patients with renal disease. Med. Sci. Sports Exerc. 2010, 42, 1809–1818. [Google Scholar] [CrossRef] [PubMed]
- Draganidis, D.; Chondrogianni, N.; Chatzinikolaou, A.; Terzis, G.; Karagounis, L.G.; Sovatzidis, A.; Avloniti, A.; Lefaki, M.; Protopapa, M.; Deli, C.K.; et al. Protein ingestion preserves proteasome activity during intense aseptic inflammation and facilitates skeletal muscle recovery in humans. Br. J. Nutr. 2017, 118, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry analysis of physical activity and sedentary behavior in older adults: A systematic review and data analysis. Eur. Rev. Aging Phys. Act. 2014, 11, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Ward, S.C.; Schnelle, J.F.; Buchowski, M.S. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med. Sci. Sports Exerc. 2012, 44, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Keadle, S.K.; Shiroma, E.J.; Freedson, P.S.; Lee, I.M. Impact of accelerometer data processing decisions on the sample size, wear time and physical activity level of a large cohort study. BMC Public Health 2014, 14, 1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. Available online: http://apps.who.int/iris/handle/10665/42330 (accessed on 4 May 2018).
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). Protein and Amino Acid Requirements in Human Nutrition. Available online: http://apps.who.int/iris/bitstream/handle/10665/43411/WHO_TRS_935_eng.pdf?sequence=1 (accessed on 4 May 2018).
- Morrisette-Thomas, V.; Cohen, A.A.; Fulop, T.; Riesco, E.; Legault, V.; Li, Q.; Milot, E.; Dusseault-Belanger, F.; Ferrucci, L. Inflamm-aging does not simply reflect increases in pro-inflammatory markers. Mech. Ageing Dev. 2014, 139, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Keadle, S.K.; Shiroma, E.J.; Kamada, M.; Matthews, C.E.; Harris, T.B.; Lee, I.M. Reproducibility of Accelerometer-Assessed Physical Activity and Sedentary Time. Am. J. Prev. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, M.A.; Leggate, M.; Viana, J.L.; King, J.A. The effect of physical activity on mediators of inflammation. Diabetes Obes. Metab. 2013, 15 (Suppl. 3), 51–60. [Google Scholar] [CrossRef] [PubMed]
- Sabiston, C.M.; Castonguay, A.; Low, N.C.; Barnett, T.; Mathieu, M.E.; O’Loughlin, J.; Lambert, M. Vigorous physical activity and low-grade systemic inflammation in adolescent boys and girls. Int. J. Pediatr. Obes. 2010, 5, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Capri, M.; Monti, D.; Giunta, S.; Olivieri, F.; Sevini, F.; Panourgia, M.P.; Invidia, L.; Celani, L.; Scurti, M.; et al. Inflammaging and anti-inflammaging: A systemic perspective on aging and longevity emerged from studies in humans. Mech. Ageing Dev. 2007, 128, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Kim, H.J.; Kim, J.W.; Yu, B.P. The inflammation hypothesis of aging: Molecular modulation by calorie restriction. Ann. N. Y. Acad. Sci. 2001, 928, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Baylis, D.; Bartlett, D.B.; Patel, H.P.; Roberts, H.C. Understanding how we age: Insights into inflammaging. Longev. Healthspan 2013, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Jamurtas, A.Z.; Villiotou, V.; Pouliopoulou, S.; Fotinakis, P.; Taxildaris, K.; Deliconstantinos, G. Oxidative stress responses in older men during endurance training and detraining. Med. Sci. Sports Exerc. 2004, 36, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Bori, Z.; Koltai, E.; Fatouros, I.G.; Jamurtas, A.Z.; Douroudos, I.I.; Terzis, G.; Nikolaidis, M.G.; Chatzinikolaou, A.; Sovatzidis, A.; et al. Age-dependent changes in 8-oxoguanine-DNA glycosylase activity are modulated by adaptive responses to physical exercise in human skeletal muscle. Free Radic. Biol. Med. 2011, 51, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Calvani, R.; Marini, F.; Cesari, M.; Buford, T.W.; Manini, T.M.; Pahor, M.; Leeuwenburgh, C.; Bernabei, R.; Landi, F.; Marzetti, E. Systemic inflammation, body composition, and physical performance in old community-dwellers. J. Cachexia Sarcopenia Muscle 2016. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.; Pahor, M.; Lauretani, F.; Corsi, A.M.; Rhys Williams, G.; Guralnik, J.M.; Ferrucci, L. Inflammatory markers and physical performance in older persons: The InCHIANTI study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 242–248. [Google Scholar] [CrossRef]
- Zhou, L.M.; Xu, J.Y.; Rao, C.P.; Han, S.; Wan, Z.; Qin, L.Q. Effect of whey supplementation on circulating C-reactive protein: A meta-analysis of randomized controlled trials. Nutrients 2015, 7, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.J.; Rasmussen, B.B. Leucine-enriched nutrients and the regulation of mammalian target of rapamycin signalling and human skeletal muscle protein synthesis. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.R.; Jefferson, L.S. Signaling pathways and molecular mechanisms through which branched-chain amino acids mediate translational control of protein synthesis. J. Nutr. 2006, 136, 227s–231s. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Fritsche, K.L. The science of fatty acids and inflammation. Adv. Nutr. 2015, 6, 293S–301S. [Google Scholar] [CrossRef] [PubMed]
- Bleau, C.; Karelis, A.D.; St-Pierre, D.H.; Lamontagne, L. Crosstalk between intestinal microbiota, adipose tissue and skeletal muscle as an early event in systemic low-grade inflammation and the development of obesity and diabetes. Diabetes Metab. Res. Rev. 2015, 31, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Lordan, R.; Tsoupras, A.; Mitra, B.; Zabetakis, I. Dairy Fats and Cardiovascular Disease: Do We Really Need to be Concerned? Foods 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Garcia, O.P. Effect of vitamin A deficiency on the immune response in obesity. Proc. Nutr. Soc. 2012, 71, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin C status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.; Mo, H.; Wang, S.; Zu, Y.; Elfakhani, M.; Rios, S.R.; Chyu, M.C.; Yang, R.S.; Shen, C.L. Potential roles of vitamin E in age-related changes in skeletal muscle health. Nutr. Res. 2018, 49, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Dore, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health relevance of the modification of low grade inflammation in ageing (inflammageing) and the role of nutrition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | LSI (n = 17) | ESI (n = 17) |
|---|---|---|
| Age (years) | 68.2 ± 2.6 | 68.7 ± 3.0 |
| Body Height (m) | 1.71 ± 0.07 | 1.73 ± 0.04 |
| Body Weight (kg) | 82.3 ± 8.5 | 85.2 ± 7.5 |
| BMI (kg/m2) | 27.3 ± 3.1 | 27.9 ± 2.5 |
| Fat Mass (kg) | 24.1 ± 7.0 | 26.3 ± 4.1 |
| Fat (%) | 29.5 ± 6.6 | 31.8 ± 2.1 |
| Fat-Free Mass (kg) | 56.3 ± 4.6 | 58.4 ± 5.2 |
| Lean Body Mass (kg) | 53.3 ± 4.5 | 55.3 ± 5.1 |
| ALM (kg) | 23.2 ± 2.4 | 24.4 ± 2.1 |
| SMI (kg/m2) | 8.12 ± 0.7 | 8.13 ± 0.6 |
| Grip Strength (kg) | 34.3 ± 5.5 | 36.7 ± 6.6 |
| SPPB (score) | 11.9 ± 0.2 | 11.2 ± 1.0 1 |
| Sarcopenia Status | Non-Sarcopenic | Non-Sarcopenic |
| hs-CRP (mg/L) | 0.7 ± 0.2 | 2.1 ± 0.8 2 |
| Parameter | LSI (n = 17) | ESI (n = 17) | p Value | χ2 |
|---|---|---|---|---|
| Total Energy (kJ/day) | 6952.9 ± 1241.8 | 6797.8 ± 1136.8 | 0.771 | 0.085 |
| Protein | ||||
| g/day | 63.8 ± 20.3 | 66.9 ± 14.6 | 0.183 | 1.770 |
| g/kg BM/day | 0.8 ± 0.3 | 0.8 ± 0.2 | 0.817 | 0.054 |
| % of total calories | 15 ± 2.7 | 16 ± 3.0 | ||
| Leucine (g/day) | 4.89 ± 1.7 | 5.13 ± 1.2 | 0.430 | 0.624 |
| BCAAs (g/day) | 11.38 ± 3.6 | 11.53 ± 2.4 | 0.533 | 0.389 |
| Carbohydrates | ||||
| g/day | 156.2 ± 37.6 | 154.9 ± 52.7 | 0.901 | 0.016 |
| % of total calories | 37.7 ± 6.9 | 37.5 ± 8.4 | ||
| Fat | ||||
| g/day | 79.3 ± 12.5 | 73.7 ± 17.0 | 0.318 | 0.996 |
| % of total calories | 42.0 ± 4.0 | 41.7 ± 7.1 | ||
| PUFA (g/day) | 10.1 ± 2.4 | 8.9 ± 2.6 | 0.275 | 1.191 |
| MUFA (g/day) | 43.7 ± 10.8 | 37.9 ± 10.9 | 0.359 | 0.840 |
| Vitamin A (IU/day) | 6590.7 ± 2219.6 | 4701.8 ± 1552.6 1 | 0.018 | 5.616 |
| Vitamin C (mg/day) | 120.0 ± 55.5 | 77.3 ± 39.1 1 | 0.020 | 5.421 |
| Vitamin E (mg/day) | 10.0 ± 2.9 | 7.5 ± 3.0 1 | 0.034 | 4.496 |
| Selenium (μg/day) | 93.2 ± 29.8 | 96.1 ± 29.7 | 0.589 | 0.292 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Draganidis, D.; Jamurtas, A.Z.; Stampoulis, T.; Laschou, V.C.; Deli, C.K.; Georgakouli, K.; Papanikolaou, K.; Chatzinikolaou, A.; Michalopoulou, M.; Papadopoulos, C.; et al. Disparate Habitual Physical Activity and Dietary Intake Profiles of Elderly Men with Low and Elevated Systemic Inflammation. Nutrients 2018, 10, 566. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050566
Draganidis D, Jamurtas AZ, Stampoulis T, Laschou VC, Deli CK, Georgakouli K, Papanikolaou K, Chatzinikolaou A, Michalopoulou M, Papadopoulos C, et al. Disparate Habitual Physical Activity and Dietary Intake Profiles of Elderly Men with Low and Elevated Systemic Inflammation. Nutrients. 2018; 10(5):566. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050566
Chicago/Turabian StyleDraganidis, Dimitrios, Athanasios Z. Jamurtas, Theodoros Stampoulis, Vasiliki C. Laschou, Chariklia K. Deli, Kalliopi Georgakouli, Konstantinos Papanikolaou, Athanasios Chatzinikolaou, Maria Michalopoulou, Constantinos Papadopoulos, and et al. 2018. "Disparate Habitual Physical Activity and Dietary Intake Profiles of Elderly Men with Low and Elevated Systemic Inflammation" Nutrients 10, no. 5: 566. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10050566