Are Total and Individual Dietary Lignans Related to Cardiovascular Disease and Its Risk Factors in Postmenopausal Women? A Nationwide Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
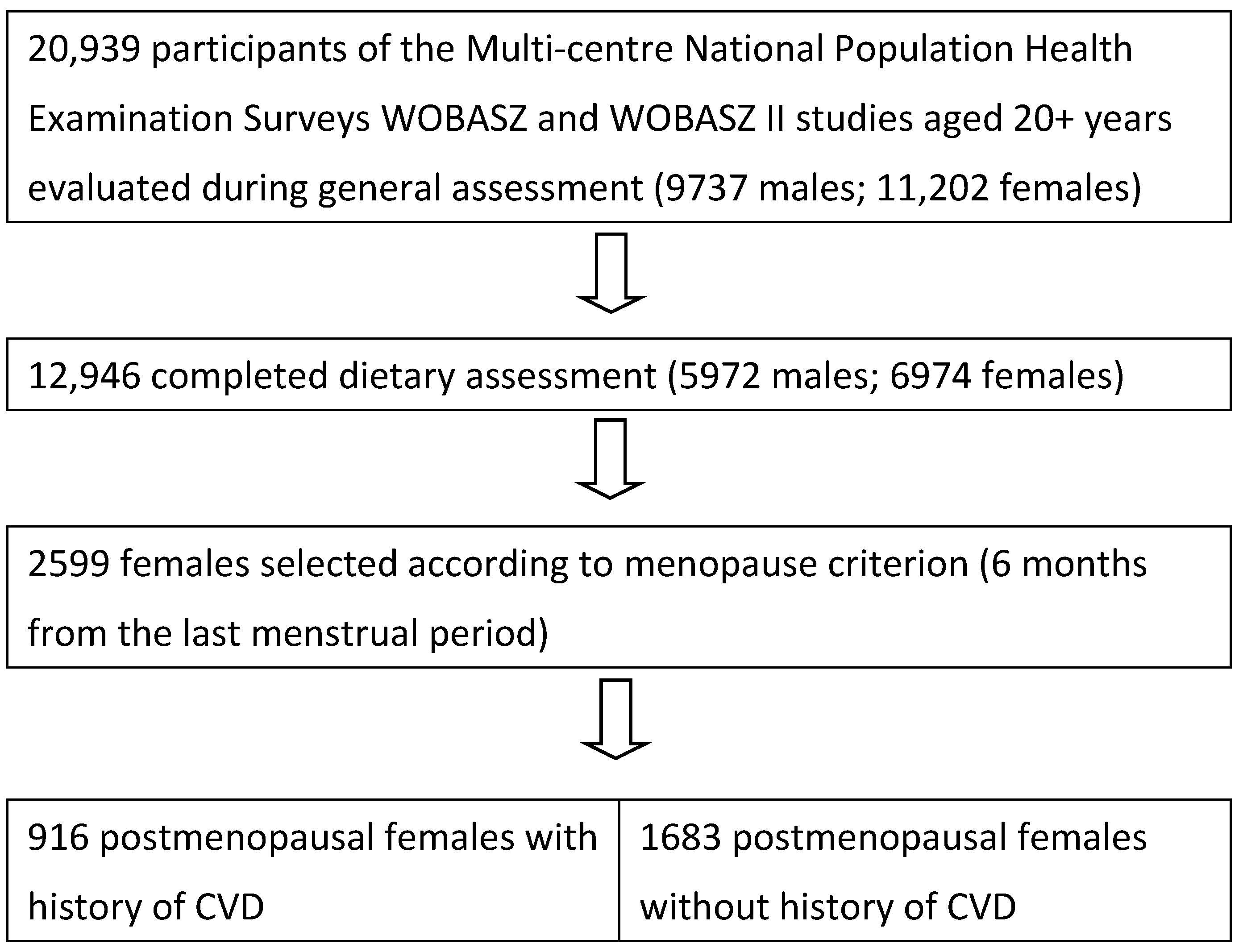
2.1. Participants
2.2. Data Collection
2.3. Dietary Assessment
2.4. Estimation of Total and Individual Lignan Intakes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Witkowska, A.M.; Zujko, M.E.; Waśkiewicz, A.; Terlikowska, K.M.; Piotrowski, W. Comparison of various databases for estimation of dietary polyphenol intake in the population of Polish adults. Nutrients 2015, 7, 9299–9308. [Google Scholar] [CrossRef] [PubMed]
- Tetens, I.; Turrini, A.; Tapanainen, H.; Christensen, T.; Lampe, J.W.; Fagt, S.; Håkansson, N.; Lundquist, A.; Hallund, J.; Valsta, L.M.; et al. Phytohealth WP1 working group. Dietary intake and main sources of plant lignans in five European countries. Food Nutr. Res. 2013, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, K. Antioxidant activity of secoisolariciresinol diglucoside-derived metabolites, secoisolariciresinol, enterodiol, and enterolactone. Int. J. Angiol. 2000, 9, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Kawaguchi, K.; Kiyama, R. Differential and directional estrogenic signaling pathways induced by enterolignans and their precursors. PLoS ONE 2017, 12, e0171390. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, R.C.G.; Peralta, R.M.; Haminiuk, C.W.I.; Maciel, G.M.; Bracht, A.; Ferreira, I.C.F.R. New phytochemicals as potential human anti-aging compounds: Reality, promise, and challenges. Crit. Rev. Food Sci. Nutr. 2018, 58, 942–957. [Google Scholar] [CrossRef] [PubMed]
- De Kat, A.C.; Dam, V.; Onland-Moret, N.C.; Eijkemans, M.J.; Broekmans, F.J.; van der Schouw, Y.T. Unraveling the associations of age and menopause with cardiovascular risk factors in a large population-based study. BMC Med. 2017, 15, 2. [Google Scholar] [CrossRef]
- Felmlee, M.A.; Woo, G.; Simko, E.; Krol, E.S.; Muir, A.D.; Alcorn, J. Effects of the flaxseed lignans secoisolariciresinol diglucoside and its aglycone on serum and hepatic lipids in hyperlipidaemic rats. Br. J. Nutr. 2009, 102, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M. Association between polyphenol intake and hypertension in adults and older adults: A population-based study in Brazil. PLoS ONE 2016, 11, e0165791. [Google Scholar] [CrossRef] [PubMed]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; de la Torre, R.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Inverse association between habitual polyphenol intake and incidence of cardiovascular events in the PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 639–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milder, I.E.; Feskens, E.J.; Arts, I.C.; Bueno-de-Mesquita, H.B.; Hollman, P.C.; Kromhout, D. Intakes of 4 dietary lignans and cause-specific and all-cause mortality in the Zutphen Elderly Study. Am. J. Clin. Nutr. 2006, 84, 400–405. [Google Scholar] [PubMed]
- Van der Schouw, Y.T.; Kreijkamp-Kaspers, S.; Peeters, P.H.; Keinan-Boker, L.; Rimm, E.B.; Grobbee, D.E. Prospective study on usual dietary phytoestrogen intake and cardiovascular disease risk in Western women. Circulation 2005, 111, 465–471. [Google Scholar] [CrossRef] [PubMed]
- De Kleijn, M.J.; van der Schouw, Y.T.; Wilson, P.W.; Grobbee, D.E.; Jacques, P.F. Dietary intake of phytoestrogens is associated with a favorable metabolic cardiovascular risk profile in postmenopausal U.S. women: The Framingham study. J. Nutr. 2002, 132, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, N.; Valtueña, S.; Ardigò, D.; Brighenti, F.; Franzini, L.; Del Rio, D.; Scazzina, F.; Piatti, P.M.; Zavaroni, I. Intake of the plant lignans matairesinol, secoisolariciresinol, pinoresinol, and lariciresinol in relation to vascular inflammation and endothelial dysfunction in middle age-elderly men and post-menopausal women living in Northern Italy. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Broda, G.; Rywik, S. Multicenter national Polish population health status tests—WOBASZ project with defined problems and treatment goals. Kardiol. Pol. 2005, 63 (Suppl. 4), 601–604. (In Polish) [Google Scholar]
- Rywik, S.; Kupść, W.; Piotrowski, W.; Broda, G.; Piwoński, J.; Kurjata, P.; Waśkiewicz, A.; Gaździk, D. Multicenter national Polish population health status tests—WOBASZ project. Establishment of methods and logistics. Kardiol. Pol. 2005, 63 (Suppl. 4), 605–613. (In Polish) [Google Scholar]
- Drygas, W.; Niklas, A.A.; Piwońska, A.; Piotrowski, W.; Flotyńska, A.; Kwaśniewska, M.; Nadrowski, P.; Puch-Walczak, A.; Szafraniec, K.; Bielecki, W.; et al. Multi-center National Population Health Examination Survey (WOBASZ II study): Assumptions, methods and implementation. Kardiol. Pol. 2015. [Google Scholar] [CrossRef]
- Mendis, S.; Puska, P.; Norrving, B. (Eds.) Global Atlas on Cardiovascular Disease Prevention and Control, 1st ed.; World Health Organization in Collaboration with the World Heart Federation; The World Stroke Organization: Geneva, Switzerland, 2011; pp. 2–7. [Google Scholar]
- Witkowska, A.M.; Waśkiewicz, A.; Zujko, M.E.; Szcześniewska, D.; Pająk, A.; Stepaniak, U.; Drygas, W. Dietary polyphenol intake, but not the dietary total antioxidant capacity, is inversely related to cardiovascular disease in postmenopausal Polish women: Results of WOBASZ and WOBASZ II Studies. Oxid. Med. Cell. Longev. 2017, 2017, 5982809. [Google Scholar] [CrossRef] [PubMed]
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. Food Composition Tables; PZWL: Warsaw, Poland, 2005. [Google Scholar]
- Milder, I.E.; Arts, I.C.; van de Putte, B.; Venema, D.P.; Hollman, P.C. Lignan contents of Dutch plant foods: A database including lariciresinol, pinoresinol, secoisolariciresinol and matairesinol. Br. J. Nutr. 2005, 93, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Kuhnle, G.G.C.; Dell’Aquila, C.; Aspinall, S.M.; Runswick, S.A.; Mulligan, A.A.; Bingham, S.A. Phytoestrogen content of beverages, nuts, seeds, and oils. J. Agric. Food Chem. 2008, 56, 7311–7315. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.U.; Boucher, B.A.; Liu, Z.; Cotterchio, M.; Kreiger, N. Phytoestrogen content of foods consumed in Canada, including isoflavones, lignans, and coumestan. Nutr. Cancer 2006, 54, 184–201. [Google Scholar] [CrossRef] [PubMed]
- Neill, A.S.; Ibiebele, T.I.; Lahmann, P.H.; Hughes, M.C.; Nagle, C.M.; Webb, P.M.; Australian Ovarian Cancer Study Group; Australian National Endometrial Cancer Study Group. Dietary phyto-oestrogens and the risk of ovarian and endometrial cancers: Findings from two Australian case-control studies. Br. J. Nutr. 2014, 111, 1430–1440. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Wang, S.; Zhou, M.; Yu, W.; Zhang, Y.; He, X. Phytoestrogens and risk of prostate cancer: A meta-analysis of observational studies. World, J. Surg. Oncol. 2015, 13, 231. [Google Scholar] [CrossRef] [PubMed]
- McCann, S.E.; Hootman, K.C.; Weaver, A.M.; Thompson, L.U.; Morrison, C.; Hwang, H.; Edge, S.B.; Ambrosone, C.B.; Horvath, P.J.; Kulkarni, S.A. Dietary intakes of total and specific lignans are associated with clinical breast tumor characteristics. J. Nutr. 2012, 142, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Velentzis, L.S.; Cantwell, M.M.; Cardwell, C.; Keshtgar, M.R.; Leathem, A.J.; Woodside, J.V. Lignans and breast cancer risk in pre- and post-menopausal women: Meta-analyses of observational studies. Br. J. Cancer 2009, 100, 1492–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Q.; Wedick, N.M.; Pan, A.; Townsend, M.K.; Cassidy, A.; Franke, A.A.; Rimm, E.B.; Hu, F.B.; van Dam, R.M. Gut microbiota metabolites of dietary lignans and risk of type 2 diabetes: A prospective investigation in two cohorts of U.S. women. Diabetes Care 2014, 37, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Yngve, A.; Lagergren, J.; Lu, Y. A dietary pattern rich in lignans, quercetin and resveratrol decreases the risk of oesophageal cancer. Br. J. Nutr. 2014, 112, 2002–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaineddin, A.K.; Buck, K.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Linseisen, J.; Chang-Claude, J. The association between dietary lignans, phytoestrogen-rich foods, and fiber intake and postmenopausal breast cancer risk: A German case-control study. Nutr. Cancer 2012, 64, 652–665. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Forouhi, N.G.; Sharp, S.J.; González, C.A.; Buijsse, B.; Guevara, M.; van der Schouw, Y.T.; Amiano, P.; Boeing, H.; Bredsdorff, L.; et al. The association between dietary flavonoid and lignan intakes and incident type 2 diabetes in European populations: The EPIC-InterAct study. Diabetes Care 2013, 36, 3961–3970. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Micek, A.; Kozela, M.; Stefler, D.; Bobak, M.; Pajak, A. Dietary polyphenol intake and risk of type 2 diabetes in the Polish arm of the Health, Alcohol and Psychosocial factors in Eastern Europe (HAPIEE) study. Br. J. Nutr. 2017, 118, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Wallström, P.; Drake, I.; Sonestedt, E.; Gullberg, B.; Bjartell, A.; Olsson, H.; Adlercreutz, H.; Tikkanen, M.J.; Wirfält, E. Plasma enterolactone and risk of prostate cancer in middle-aged Swedish men. Eur. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nooyens, A.C.; Milder, I.E.; van Gelder, B.M.; Bueno-de-Mesquita, H.B.; van Boxtel, M.P.; Verschuren, W.M. Diet and cognitive decline at middle age: The role of antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Knaze, V.; Luján-Barroso, L.; Kuhnle, G.G.; Mulligan, A.A.; Touillaud, M.; Slimani, N.; Romieu, I.; Powell, N.; Tumino, R.; et al. Dietary intakes and food sources of phytoestrogens in the European Prospective Investigation into Cancer and Nutrition (EPIC) 24-h dietary recall cohort. Eur. J. Clin. Nutr. 2012, 66, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Van der Schouw, Y.T.; Sampson, L.; Willett, W.C.; Rimm, E.B. The usual intake of lignans but not that of isoflavones may be related to cardiovascular risk factors in U.S. men. J. Nutr. 2005, 135, 260–266. [Google Scholar] [CrossRef] [PubMed]
- De Kleijn, M.J.; van der Schouw, Y.T.; Wilson, P.W.; Adlercreutz, H.; Mazur, W.; Grobbee, D.E.; Jacques, P.F. Intake of dietary phytoestrogens is low in postmenopausal women in the United States: The Framingham study. J. Nutr. 2001, 131, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Wolk, A.; Bergstrom, R.; Hunter, D.; Willett, W.; Ljung, H.; Holmberg, L.; Bruce, A.; Adami, H.O. A prospective study of association of monounsaturated fat and other types of fat with risk of breast cancer. Arch. Intern. Med. 1998, 158, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Milder, I.E.; Feskens, E.J.; Arts, I.C.; de Mesquita, H.B.; Hollman, P.C.; Kromhout, D. Intake of the plant lignans secoisolariciresinol, matairesinol, lariciresinol, and pinoresinol in Dutch men and women. J. Nutr. 2005, 135, 1202–1207. [Google Scholar] [CrossRef] [PubMed]
- Penalvo, J.L.; Haajanen, K.M.; Botting, N.; Adlercreutz, H. Quantification of lignans in food using isotope dilution gas chromatography/mass spectrometry. J. Agric. Food Chem. 2005, 53, 9342–9347. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Bergante, S.; Satriano, A.; Pluchinotta, F.R.; Marranzano, M. Dietary phytoestrogen intake is inversely associated with hypertension in a cohort of adults living in the Mediterranean area. Molecules 2018, 23, 368. [Google Scholar] [CrossRef] [PubMed]
- McGill, C.R.; Kurilich, A.C.; Davignon, J. The role of potatoes and potato components in cardiometabolic health: A review. Ann. Med. 2013, 45, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Kapusta-Duch, J.; Kopeć, A.; Piatkowska, E.; Borczak, B.; Leszczyńska, T. The beneficial effects of Brassica vegetables on human health. Roczniki Państwowego Zakładu Higieny 2012, 63, 389–395. [Google Scholar] [PubMed]
- Sesso, H.D.; Gaziano, J.M.; Liu, S.; Buring, J.E. Flavonoid intake and the risk of cardiovascular disease in women. Am. J. Clin. Nutr. 2003, 77, 1400–1408. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Women Diagnosed with CVD n = 916 | Women without CVD n = 1683 | ||||
|---|---|---|---|---|---|
| Characteristics | Mean ± SD | Median (25–75 Percentile) | Mean ± SD | Median (25–75 Percentile) | p |
| Age (years) | 65.48 + 9.21 | 65.00 (58.00–72.00) | 60.98 + 8.41 | 60.00 (55.00–66.00) | <0.0001 |
| Fasting glucose (mmol/L) | 5.7 ± 1.9 | 5.14 (4.72–5.80) | 5.5 ± 1.6 | 5.19 (4.72–5.77) | 0.531 |
| Total cholesterol (mmol/L) | 5.4 ± 1.2 | 5.43 (4.64–6.20) | 5.8 ± 1.3 | 5.76 (5.06–6.53) | <0.0001 |
| Energy from food (kcal/day) | 1517 ± 580 | 1438 (1130–1831) | 1653 ± 628 | 1587 (1220–1976) | <0.0001 |
| Intake of vegetables (g/day) | 215 ± 156 | 189 (104–299) | 214 ± 155 | 187 (100–302) | 0.850 |
| Intake of fruits (g/day) | 214 ± 226 | 150 (25–300) | 217 ± 227 | 150 (10–320) | 0.989 |
| Intake of tea (g/day) | 361 ± 252 | 400 (200–500) | 348 ± 251 | 300 (200–500) | 0.180 |
| Intake of coffee (g/day) | 130 ± 166 | 0 (0–250) | 175 ± 172 | 200 (0–250) | <0.0001 |
| Intake of alcohol (pure ethanol g/day) | 0.69± 2.67 | 0.15 (0–0.50) | 0.99 ± 2.86 | 0.25 (0–0.80) | <0.0001 |
| % | % | ||||
| Family history of CVD (%) | 39.4 | 36.1 | 0.098 | ||
| Diseases (%) | |||||
| Hypertension | 73.1 | 57.3 | <0.0001 | ||
| Myocardial infarction | 12.6 | 0 | <0.0001 | ||
| Stroke | 7.9 | 0 | <0.0001 | ||
| Diabetes | 19.8 | 13.4 | <0.0001 | ||
| Hypercholesterolemia (%) | 79.7 | 84.1 | 0.0056 | ||
| BMI [kg/m2] (%) | <0.0001 | ||||
| Underweight (BMI < 18.5) | 0.3 | 0.7 | |||
| Normal (BMI 18.5–24.99) | 20.2 | 27.8 | |||
| Overweight (BMI 25–29.99) | 35.2 | 39.3 | |||
| Obesity (BMI > 30) | 44.3 | 32.2 | |||
| Central obesity (%) | 88.3 | 82.8 | <0.0001 | ||
| Smoking status (%) | <0.0001 | ||||
| Current smokers | 12.5 | 20.9 | |||
| Past smokers | 18.6 | 17.7 | |||
| Never smokers | 68.9 | 61.4 | |||
| Leisure-time physical activity (%) | 0.107 | ||||
| Low level | 52.1 | 47.8 | |||
| Middle level | 16.5 | 18.4 | |||
| High level | 31.3 | 33.8 | |||
| Level of education (%) | 0.009 | ||||
| Under middle | 61.0 | 55.2 | |||
| Middle | 31.9 | 35.4 | |||
| High | 7.1 | 9.5 | |||
| Menopause hormone therapy (%) | 3.8 | 4.9 | 0.178 | ||
| Food Categories | Women with CVD n = 916 | Women without CVD n = 1683 | p Value | |
|---|---|---|---|---|
| Beverages | μg/day (mean ± SD) | 152.5 ± 92 | 152.9 ± 92 | 0.7711 |
| Contribution to LIG (%) | 13.49 | 13.96 | ||
| Major sources (% contribution) * | tea (11.76), coffee (1.17), fruit juices (0.44) | tea (11.72), coffee (1.63), fruit juices (0.44) | ||
| Cereals | μg/day (mean ± SD) | 105.8 ± 112 | 103.9 ± 112 | 0.5003 |
| Contribution to LIG (%) | 9.36 | 9.49 | ||
| Major sources (% contribution) * | rye bread (3.82), wheat bread (1.46), mixed bread (1.34) | rye bread (3.66), pastry (3.15), mixed bread (1.77) | ||
| Fruit | μg/day (mean ± SD) | 115.9 ± 254 | 109.6 ± 217 | 0.5386 |
| Contribution to LIG (%) | 10.25 | 10.01 | ||
| Major sources (% contribution) * | strawberries (2.17), pears (1.75), peaches (1.54), plums (1.42) | strawberries (2.28), pears (2.22), plums (1.21), peaches (1.00) | ||
| Vegetables | μg/day (mean ± SD) | 416.7 ± 524 | 420.1 ± 538 | 0.8185 |
| Contribution to LIG (%) | 36.85 | 38.36 | ||
| Major sources (% contribution) * | cabbage (15.70), potato (7.18), legumes (5.32), carrot (2.13) | cabbage (14.66), potato (8.14), legumes (4.19), broccoli and cauliflower (3.98), carrot (1.90) | ||
| Nuts and seeds | μg/day (mean ± SD) | 309.2 ± 4316 | 252.8 ± 4728 | 0.5505 |
| Contribution to LIG (%) | 27.35 | 23.08 | ||
| Major sources (% contribution) * | flaxseed (26.94), sunflower seeds (0.26), walnuts (0.07) | flaxseed (21.63), sesame (0.86), sunflower seeds (0.44) | ||
| Vegetable fats | μg/day (mean ± SD) | 14.6 ± 18.4 | 16.7 ± 19.7 | 0.0057 |
| Contribution to LIG (%) | 1.29 | 1.52 | ||
| Major sources (% contribution) * | canola oil (0.66), soft margarine (80% fat) (0.26), sunflower oil (0.22) | canola oil (0.84), soft margarine (80% fat) (0.31), sunflower oil (0.21) | ||
| Other food categories | μg/day (mean ± SD) | 16 ± 113 | 39 ± 460 | 0.0029 |
| Contribution to LIG (%) | 1.42 | 3.56 | ||
| Major sources (% contribution) * | confectionery (1.20), cocoa products (0.11) | confectionery (3.31), cocoa products (0.17) | ||
| Total lignan intake | μg/day (mean ± SD) | 1130.7 ± 4844 | 1095.1 ± 4352.7 | 0.9251 |
| Contribution to LIG (%) | 100 | 100 | ||
| Major sources (% contribution) * | flaxseed (26.94), cabbage (15.70), tea (11.76), potato (7.18), legumes (5.32), rye bread (3.82) | flaxseed (21.63), cabbage (14.66), tea (11.72), potato (8.14), legumes (4.19), broccoli and cauliflower (3.98) | ||
| Food Categories | Women with CVD n = 916 | Women without CVD n = 1683 | p Value | |
|---|---|---|---|---|
| Beverages | μg/day (mean ± SD) | 122.3 ± 74.0 | 122.7 ± 74.0 | 0.7405 |
| Contribution to SECO (%) | 21.57 | 25.0 | ||
| Major sources (% contribution) * | tea (19.10), coffee (1.97), fruit juices (0.36) | tea (21.27), coffee (3.10), fruit juices (0.42) | ||
| Cereals | μg/day (mean ± SD) | 50.3 ± 68.6 | 48.8 ± 71.2 | 0.5669 |
| Contribution to SECO (%) | 8.87 | 9.94 | ||
| Major sources (% contribution) * | rye bread (5.78), wheat bread (1.21), mixed bread (0.67) | rye bread (6.19), wheat bread (1.43), mixed bread (0.97) | ||
| Fruit | μg/day (mean ± SD) | 21.4 ± 42.2 | 19.7 ± 36.5 | 0.3650 |
| Contribution to SECO (%) | 3.77 | 4.01 | ||
| Major sources (% contribution) * | plums (0.94), strawberries (0.46), peaches (0.43) | plums (0.90), strawberries (0.54), apples (0.43) | ||
| Vegetables | μg/day (mean ± SD) | 71.3 ± 141.6 | 62.1 ± 113.8 | 0.5046 |
| Contribution to SECO (%) | 12.57 | 12.65 | ||
| Major sources (% contribution) * | legumes (5.41), carrot (2.57), cabbage (1.35) | legumes (4.03), carrot (2.59), cabbage (1.75) | ||
| Nuts and seeds | μg/day (mean ± SD) | 296.4 ± 4183 | 230.9 ± 4567 | 0.5499 |
| Contribution to SECO (%) | 52.27 | 47.05 | ||
| Major sources (% contribution) * | flaxseed (52.07), walnuts (0.13), sunflower seeds (0.05) | flaxseed (46.78), walnuts (0.13), sunflower seeds (0.09) | ||
| Vegetable fats | μg/day (mean ± SD) | 2.73 ± 4.74 | 3.19 ± 5.13 | 0.0113 |
| Contribution to SECO (%) | 0.48 | 0.65 | ||
| Major sources (% contribution) * | canola oil (0.36), sunflower oil (0.12) | canola oil (0.52), sunflower oil (0.13) | ||
| Other food categories | μg/day (mean ± SD) | 5.4 ± 10.8 | 6.6 ± 11.4 | 0.0067 |
| Contribution to SECO (%) | 0.95 | 1.34 | ||
| Major sources (% contribution) * | confectionery (0.39), cocoa products (0.01) | confectionery (0.56), cocoa products (0.02) | ||
| Total secoisolariciresinol | μg/day (mean ± SD) | 567.1 ± 4185 | 490.8 ± 4570 | 0.7464 |
| Contribution to SECO (%) | 100 | 100 | ||
| Major sources (% contribution) * | flaxseed (52.07), tea (19.10), rye bread (5.78), legumes (5.41) | flaxseed (46.78), tea (21.27), rye bread (6.19), legumes (4.03) | ||
| Food Categories | Women with CVD n = 916 | Women without CVD n = 1683 | p Value | |
|---|---|---|---|---|
| Beverages | μg/day (mean ± SD) | 16.1 ± 11.3 | 15.7 ± 11.6 | 0.5580 |
| Contribution to PINO (%) | 5.93 | 5.49 | ||
| Major sources (% contribution) * | tea (5.30), fruit juices (0.38), beer (0.12), coffee (0.10) | tea (4.86), fruit juices (0.33), beer (0.13), coffee (0.12) | ||
| Cereals | μg/day (mean ± SD) | 20.4 ± 20.2 | 21.7 ± 24.8 | 0.0901 |
| Contribution to PINO (%) | 7.51 | 7.59 | ||
| Major sources (% contribution) * | mixed bread (1.96), wheat bread (1.41), breakfast cereals (1.38), | mixed bread (2.32), breakfast cereals (1.58), wheat bread (1.22) | ||
| Fruit | μg/day (mean ± SD) | 46.7 ± 129.5 | 40.7 ± 104.2 | 0.3223 |
| Contribution to PINO (%) | 17.20 | 14.23 | ||
| Major sources (% contribution) * | strawberries (4.71), peaches (3.98), plums (3.26) | strawberries (4.55), plums (2.57), peaches (2.40) | ||
| Vegetables | μg/day (mean ± SD) | 165.6 ± 312.5 | 160.7 ± 304.9 | 0.3921 |
| Contribution to PINO (%) | 60.99 | 56.19 | ||
| Major sources (% contribution) * | cabbage (43.17), potato (7.40), legumes (4.09) | cabbage (36.19), potato (7.69), legumes (3.95) | ||
| Nuts and seeds | μg/day (mean ± SD) | 3.67 ± 47.2 | 10.2 ± 257.4 | 0.5429 |
| Contribution to PINO (%) | 1.35 | 3.57 | ||
| Major sources (% contribution) * | flaxseed (1.22), sunflower seeds (0.11), pumpkin seeds (0.02) | flaxseed (0.90), sesame (2.45) sunflower seeds (0.16) | ||
| Vegetable fats | μg/day (mean ± SD) | 11.3 ± 13.4 | 12.9 ± 14.3 | 0.0062 |
| Contribution to PINO (%) | 4.16 | 4.51 | ||
| Major sources (% contribution) * | canola oil (1.89), soft margarine (80% fat) (1.03), sunflower oil (0.62), soft margarine (60% fat) (0.40) | canola oil (2.21), soft margarine (80% fat) (1.13), sunflower oil (0.57), soft margarine (60% fat) (0.33) | ||
| Other food categories | μg/day (mean ± SD) | 19.03 ± 83.8 | 37.0 ± 344.9 | 0.0249 |
| Contribution to PINO (%) | 7.02 | 12.93 | ||
| Major sources (% contribution) * | confectionery (2.14), cocoa products (0.24), | confectionery (7.55), cocoa products (0.32), | ||
| Total pinoresinol | μg/day (mean ± SD) | 271.5 ± 356.1 | 286.0 ± 548.0 | 0.4899 |
| Contribution to PINO (%) | 100 | 100 | ||
| cabbage (43.17), potato (7.40), tea (5.30) | cabbage (36.19), potato (7.69), confectionery (7.55) | |||
| Food Categories | Women with CVD n = 916 | Women without CVD n = 1683 | p Value | |
|---|---|---|---|---|
| Beverages | μg/day (mean ± SD) | 3.45 ± 5.72 | 3.86 ± 6.14 | 0.0001 |
| Contribution to LARI (%) | 1.35 | 1.35 | ||
| Major sources (% contribution) * | fruit juices (0.53), coffee (0.46), tea (0.28) | coffee (0.55), fruit juices (0.44), tea (0.24) | ||
| Cereals | μg/day (mean ± SD) | 27.6 ± 44.4 | 25.9 ± 36.2 | 0.1919 |
| Contribution to LARI (%) | 10.78 | 9.06 | ||
| Major sources (% contribution) * | groats and grains (3.85), mixed bread (3.85) | mixed bread (3.45), pastry (3.45) | ||
| Fruit | μg/day (mean ± SD) | 45.8 ± 111.4 | 47.5 ± 106.6 | 0.5872 |
| Contribution to LARI (%) | 17.88 | 16.22 | ||
| Major sources (% contribution) * | pear (7.69), strawberries (3.85), citrus fruits (3.85) | pear (6.90), strawberries (3.45), citrus fruits (3.45) | ||
| Vegetables | μg/day (mean ± SD) | 168.1 ± 170.6 | 189.5 ± 241.7 | 0.1081 |
| Contribution to LARI (%) | 65.64 | 66.31 | ||
| Major sources (% contribution) * | potato (23.08), cabbage (19.23), broccoli and cauliflower (3.85), tomato (3.85), carrot (3.85) | potato (20.69), cabbage (17.24), broccoli and cauliflower (10.34), tomato (3.45), carrot (3.45) | ||
| Nuts and seeds | μg/day (mean ± SD) | 5.39 ± 58.1 | 7.60 ± 105.7 | 0.5453 |
| Contribution to LARI (%) | 2.10 | 2.66 | ||
| Major sources (% contribution) * | flaxseed (1.50), sunflower seeds (0.47), pumpkin seeds (0.1), walnuts (0.02) | flaxseed (1.05), sesame (0.76), sunflower seeds (0.68) | ||
| Vegetable fats | μg/day (mean ± SD) | 0.567 ± 0.671 | 0.644 ± 0.716 | 0.0062 |
| Contribution to LARI (%) | 0.22 | 0.23 | ||
| Major sources (% contribution) * | canola oil (0.10), soft margarine (80% fat) (0.05), sunflower oil (0.03) | canola oil (0.11), soft margarine (80% fat) (0.06), sunflower oil (0.03) | ||
| Other food categories | μg/day (mean ± SD) | 5.76 ± 26.2 | 11.44 ± 106.1 | 0.0263 |
| Contribution to LARI (%) | 2.25 | 4.00 | ||
| Major sources (% contribution) * | confectionery (1.75), cocoa products (0.22) | confectionery (3.53), cocoa products (0.29) | ||
| Total lariciresinol | μg/day (mean ± SD) | 256.1 ± 222.4 | 285.8 ± 320.5 | 0.0614 |
| Contribution to LARI (%) | 100 | 100 | ||
| Major sources (% contribution) * | potato (23.08), cabbage (19.23), pear (7.69) | potato (20.69), cabbage (17.24), broccoli and cauliflower (10.34) | ||
| Food Categories | Women with CVD n = 916 | Women without CVD n = 1683 | p Value | |
|---|---|---|---|---|
| Beverages | μg/day (mean ± SD) | 10.7 ± 6.8 | 10.6 ± 6.7 | 0.8108 |
| Contribution to MAT (%) | 29.72 | 32.62 | ||
| Major sources (% contribution) * | tea (26.56), fruit juices (1.57), coffee (1.44) | tea (28.37), coffee (2.16), fruit juices (1.70) | ||
| Cereals | μg/day (mean ± SD) | 7.56 ± 10.3 | 7.43 ± 11.1 | 0.3583 |
| Contribution to MAT (%) | 21.00 | 22.86 | ||
| Major sources (% contribution) * | rye bread (13.06), wheat bread (2.89), breakfast cereals (2.63) | rye bread (13.42), wheat bread (3.26), breakfast cereals (3.00) | ||
| Fruit | μg/day (mean ± SD) | 1.92 ± 7.9 | 1.69 ± 5.7 | 0.2993 |
| Contribution to MAT (%) | 5.33 | 5.20 | ||
| Major sources (% contribution) * | grapes (1.93), citrus fruits (1.44), dried fruits (1.20) | citrus fruits (1.80), grapes (1.74), dried fruits (0.8) | ||
| Vegetables | μg/day (mean ± SD) | 11.7 ± 184.6 | 7.84 ± 99.9 | 0.7974 |
| Contribution to MAT (%) | 32.50 | 24.12 | ||
| Major sources (% contribution) * | legumes (23.03), potato (4.28), parsnips (2.72) | legumes (13.60), potato (5.20), parsnips (2.74) | ||
| Nuts and seeds | μg/day (mean ± SD) | 3.69 ± 37.2 | 4.12 ± 45.5 | 0.5510 |
| Contribution to MAT (%) | 10.25 | 12.68 | ||
| Major sources (% contribution) * | flaxseed (6.11), sunflower seeds (3.36), pumpkin seeds (0.71), walnuts (0.06) | sunflower seeds (5.97), flaxseed (5.26), pumpkin seed (0.86), sesame (0.52) | ||
| Vegetable fats | μg/day (mean ± SD) | 0.0085 ± 0.010 | 0.0098 ± 0.011 | 0.0054 |
| Contribution to MAT (%) | 0.02 | 0.03 | ||
| Major sources (% contribution) * | canola oil (0.01), soft margarine (80% fat) (0.01) | canola oil (0.01), soft margarine (80% fat) (0.01) | ||
| Other food categories | μg/day (mean ± SD) | 0.43 ± 2.10 | 0.82 ± 8.26 | 0.0033 |
| Contribution to MAT (%) | 1.20 | 2.52 | ||
| Major sources (% contribution) * | confectionery | confectionery | ||
| Total matairesinol | μg/day (mean ± SD) | 36.0 ± 190 | 32.5 ± 111 | 0.5174 |
| Contribution to MAT (%) | 100 | 100 | ||
| Major sources (% contribution) * | tea (26.56), legumes (23.03), rye bread (13.06) | tea (28.37), legumes (13.60), rye bread (13.06) | ||
| Variables | CVD 1 OR (95% CI) | Hypercholeste-Rolemia 2 OR (95% CI) | Hypertension 3 OR (95% CI) | Central Obesity 4 OR (95% CI) | |
|---|---|---|---|---|---|
| Total lignans (μg/day) | Model 1 | 1.002 (0.984; 1.020) p = 0.8380 | 0.989 (0.972; 1.006) p = 0.2117 | 0.991 (0.971; 1.011) p = 0.3522 | 0.981 (0.960; 1.003) p = 0.0927 |
| Model 2 | 1.003 (0.986; 1.021) p = 0.7594 | 0.989 (0.972; 1.007) p = 0.2277 | 0.991 (0.972; 1.011) p = 0.3923 | 0.982 (0.961; 1.003) p = 0.0975 | |
| Secoisolariciresinol (μg/day) | Model 1 | 1.003 (0.985; 1.022) 0.7145 | 0.991 (0.972; 1.009) p = 0.3277 | 0.993 (0.973; 1.013) p = 0.4939 | 0.978 (0.954; 1.002) p = 0.0739 |
| Model 2 | 1.003 (0.985; 1.022) 0.7136 | 0.991 (0.972; 1.009) p = 0.3229 | 0.993 (0.973; 1.013) p = 0.5003 | 0.977 (0.953; 1.002) p = 0.0742 | |
| Pinoresinol (μg/day) | Model 1 | 0.944 (0.782; 1.139) p = 0.5457 | 0.836 (0.695; 1.005) p = 0.0565 | 0.842 (0.697; 1.016) p = 0.0734 | 1.126 (0.881; 1.455) p = 0.3665 |
| Model 2 | 0.987 (0.821; 1.187) p = 0.8927 | 0.853 (0.708; 1.028) p = 0.0958 | 0.868 (0.720; 1.047) p = 0.1382 | 1.160 (0.886; 1.520) p = 0.2807 | |
| Lariciresinol (μg/day) | Model 1 | 0.717 (0.507; 1.014) p = 0.0597 | 0.656 (0.468; 0.921) p = 0.0148 | 0.694 (0.505; 0.952) p = 0.0236 | 1.048 (0.713; 1.539) p = 0.8128 |
| Model 2 | 0.815 (0.575; 1.154) p = 0.2487 | 0.693 (0.488; 0.985) p = 0.0410 | 0.744 (0.539; 1.029) p = 0.0736 | 1.109 (0.741; 1.659) p = 0.6146 | |
| Matairesinol (μg/day) | Model 1 | 1.347 (0.776; 2.338) p = 0.2902 | 1.082 (0.459; 2.552) p = 0.8576 | 1.290 (0.692; 2.405) p = 0.4228 | 1.128 (0.451; 2.817) p = 0.7968 |
| Model 2 | 1.415 (0.811; 2.469) p = 0.2214 | 1.133 (0.463; 2.777) p = 0.7842 | 1.347 (0.708; 2.564) p = 0.3645 | 1.166 (0.455; 2.989) p = 0.7489 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Witkowska, A.M.; Waśkiewicz, A.; Zujko, M.E.; Szcześniewska, D.; Stepaniak, U.; Pająk, A.; Drygas, W. Are Total and Individual Dietary Lignans Related to Cardiovascular Disease and Its Risk Factors in Postmenopausal Women? A Nationwide Study. Nutrients 2018, 10, 865. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070865
Witkowska AM, Waśkiewicz A, Zujko ME, Szcześniewska D, Stepaniak U, Pająk A, Drygas W. Are Total and Individual Dietary Lignans Related to Cardiovascular Disease and Its Risk Factors in Postmenopausal Women? A Nationwide Study. Nutrients. 2018; 10(7):865. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070865
Chicago/Turabian StyleWitkowska, Anna Maria, Anna Waśkiewicz, Małgorzata Elżbieta Zujko, Danuta Szcześniewska, Urszula Stepaniak, Andrzej Pająk, and Wojciech Drygas. 2018. "Are Total and Individual Dietary Lignans Related to Cardiovascular Disease and Its Risk Factors in Postmenopausal Women? A Nationwide Study" Nutrients 10, no. 7: 865. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10070865